Embed Size (px)
Citation preview
OCCASIONAL SURVEY
Contemporary adrenal scintigraphy
Milton D. Gross & Anca Avram & Lorraine M. Fig &
Domenico Rubello
Received: 15 June 2006 /Accepted: 8 August 2006 / Published online: 25 November 2006# Springer-Verlag 2006
AbstractIntroduction High-resolution computed tomography (CT)and magnetic resonance (MR) imaging have replacedscintigraphy as primary imaging modalities for the evalu-ation of adrenal diseases.Discussion Thin-slice CT, CT contrast washout studies andMR pulse sequences specifically designed to identifyadrenal lipid content have radically changed the approachto anatomic imaging and provide unique insight into thephysical characteristics of the adrenals. With a confirmedbiochemical diagnosis, further evaluation is often unneces-sary, especially in diagnostic localization of diseases of theadrenal cortex. However, despite the exquisite detailafforded by anatomy-based imaging, there are not infre-quently clinical situations in which the functional insightprovided by scintigraphy is crucial to identify adrenaldysfunction and to assist in localization of adrenocorticaland adrenomedullary disease. The introduction of hybridPET/CT and SPECT/CT, modalities that directly integrateanatomic and functional information, redefine the radio-tracer principle in the larger context of high-resolution
anatomic imaging. Instead of becoming obsolete, scintigra-phy is an element of a device that combines it with CT orMR to allow a direct correlation between function andanatomy, whereby the combination creates a more powerfuldiagnostic tool than the separate component modalities.
Keywords Scintigraphy . Adrenal . Adrenocortical .
Adrenomedullary . Radiopharmaceutical
Introduction
Contemporary adrenal imaging relies heavily upon com-puted tomography (CT) as the primary modality of adrenallocalization. The availability of CT in clinical practicemakes it ideal for evaluating adrenal gland morphology [1].Magnetic resonance (MR) also provides high-resolutionimaging and tissue characterization [1]. It, too, has beenused to diagnostic advantage in the evaluation of theadrenal cortex and medulla. Other modalities, such asadrenal vein hormone sampling, have value in selectedcases in which neither anatomic nor functional imaging candiscern the site(s) of adrenal hormonal hypersecretion.However, even with the availability of high-resolutionimaging techniques, adrenal scintigraphy continues toprovide useful information in depicting and staging neo-plasms and differential function of the adrenals (Table 1) [2].
Scintigraphic studies of the adrenal glands take advan-tage of radiopharmaceuticals with specific affinity forunique functional characteristics of the adrenal cortex andadrenal medulla [3–5]. Radiopharmaceuticals designed foradrenal imaging enter hormone biosynthetic pathways asprecursors, as compounds that mimic hormones or asligands that possess affinity for specific tissue receptors.Taking advantage of these unique endocrine tissue charac-
Eur J Nucl Med Mol Imaging (2007) 34:547–557DOI 10.1007/s00259-006-0265-5
M. D. Gross :A. Avram : L. M. FigDepartment of Radiology, Division of Nuclear Medicine,University of Michigan,Ann Arbor, MI, USA
M. D. Gross (*) : L. M. FigNuclear Medicine Service (115),Department of Veterans Affairs Health System,2215 Fuller Rd,Ann Arbor, MI 48105, USAe-mail: [email protected]
D. RubelloNuclear Medicine Service-PET Unit, S. Maria della MisericordiaRovigo Hospital, Istituto Oncologico Veneto (IOV),Rovigo, Italy

teristics, specific radiopharmaceuticals can be used not onlyto measure the process of accumulation, but to depict targettissue endocrine function. In this manner, scintigraphycontinues to play a role in the diagnosis and staging ofmalignant adrenal neoplasms, this role having evolved withthe availability of PET and SPECT/CT [6–8].
In this paper we shall review recent developments in thefield of adrenal scintigraphy that demonstrate again theimportance of an approach that integrates the functional andanatomic evaluation of adrenal disease.
Physiologic basis of functional adrenal imaging
The adrenal gland consists of two embryologically, morpho-logically and functionally distinct divisions, the adrenalcortex arising from mesoderm forming an outer zonaglomerulosa producing mineralocorticoids (aldosterone) anda deeper zona fasciculata and reticularis producing glucocor-ticoids and weak androgens, and the adrenal medulla, arisingfrom the neural crest, which secretes catecholamines.
Adrenal cortex
Steroid hormone biosynthesis begins with circulating low-density lipoprotein (LDL)-derived cholesterol, and it is thispathway that has been exploited with tracers that mimiccholesterol substrate, radiolabeled LDL or inhibitors ofenzymes responsible for steroid hormone production. The
radiocholesterol analogues labeled with 131I or 75Se 6β-nor-cholesterols are rapidly incorporated into LDL and accu-mulated by adrenocortical steroid hormone-producing cellsvia a specific, receptor-mediated process. Within adreno-cortical cells these radiocholesterols are esterified, but donot undergo further metabolism [9]. The adrenocorticalLDL receptor is under the control of pituitary adrenocor-ticotrophic hormone (ACTH) in the zona fasciculata andreticularis and the renin-angiotensin system in the zonaglomerulosa, and the accumulation of radiocholesterolanalogs can be quantitatively related to steroid hormoneoutput from the functional zones of the adrenal [9, 10].Imaging protocols have been devised to take advantage ofthese mechanisms of control to accentuate abnormalfunction for improved diagnostic performance. Alternativeapproaches to adrenocortical scintigraphy are radiolabeledLDL and inhibitors of intermediary enzymes that partici-pate in steroid biosynthesis. The recent introduction of 11C-metomidate (MTO), a compound that binds selectively to11β-hydroxylase (an enzyme essential in the biosynthesisof cortisol and aldosterone) and is regulated by ACTH, hasbeen shown to depict adrenocortical neoplasms using PET[11–13] (Table 2).
Adrenal medulla
The adrenal medulla synthesizes catecholamines (norepi-nephrine and epinephrine) and stores them in membrane-bound vesicles. Control of catecholamine secretion is via
Table 1 Clinical utility of ad-renal scintigraphy
Modified and used withpermission from [2]: GrossMD, Rubello D, Shapiro B.Is there a future for adrenalscintigraphy? Nucl MedCommun 2002;23:197–202NP-59131 I-6β-iodomethyl-norcholesterol, SMC75 Se-selenomethyl-norcholesterol,FDG18 F-fluorodeoxyglucose,MTO11 C-metomidate,MIBG131 I (123 I)-metaiodobenzylguanidine,OCT123 I, 111 In-octreotideand analogs, EPI11 C-epineph-rine, HED11 C-hydroxyephe-drine, DA18
F-dopamine, DOPA18
F-dihydroxyphenylalanine
Uses of adrenal scintigraphy
AdrenocorticalDistinguishing unilateral from bilateral adrenocortical diseaseAutonomous asymmetric, bilateral adrenal hyperplasia in hypercortisolism (NP-59, SMC)Subtle bilateral adrenal hyperplasia in primary aldosteronism (NP-59, SMC)Identifying the adrenal contribution to hyperandrogenism (NP-59)Depicting adrenal cortical functionIdentifying function in benign vs space-occupying/malignant or metastatic unilateral and bilateralincidentally discovered adrenal masses (NP-59, SMC, FDG, MTO)Identifying function in adrenocortical reimplants after bilateral adrenalectomy (NP-59, SMC)Identifying adrenocortical function after intra-arterial alcohol infusion for ablation (NP-59, SMC)Preoperative identification of suppression of normal contralateral adrenal function (NP-59, SMC)Prediction of incidentally discovered masses with potential to progress to autonomous adrenal function(NP-59, SMC)
AdrenomedullaryDepicting sources of hypercatecholaminemiaIntra-adrenal/extra-adrenal/metastatic/familial pheochromocytomas (MIBG, OCT, FDG, EPI, HED, DA,DOPA)
Other neuroendocrine neoplasmsNeuroblastoma, non-hypersecretory pheochromocytoma/paragangliomas (MIBG, OCT, FDG, EPI, HED,DA, DOPA)
548 Eur J Nucl Med Mol Imaging (2007) 34:547–557
neural or humoral (e.g., angiotensin, serotonin, histamine)stimulation. Catecholamines are released from the vesiclesby exocytosis and diffuse into the circulation, while in theadrenal medulla, catecholamines are subject to reuptakeinto secretory vesicles by a specific, energy-dependent,uptake mechanism (type I). Circulating catecholamines areinactivated by a type II uptake mechanism in extra-adrenaltissues and are rapidly metabolized to metanephrines.
Metaiodobenzylguanidine (MIBG), a guanethidine ana-log structurally similar to norepinephrine (NE), is accumu-lated in the adrenal medulla by the type I uptakemechanism and is accumulated in the catecholaminestorage vesicles, providing the rational for its use as atracer for imaging sympathomimetic tissues [14–16].
Somatostatin receptors are widely distributed and arefound in many neoplasms of the neural crest, and a growingnumber of somatostatin receptor imaging agents havedemonstrated success in depicting neoplasms of adrenalmedulla origin. Pentetreotide, a long-acting somatostatinantagonist, has been labeled with a variety of radioisotopes(e.g., 111In, 123I) and has been used to image pheochro-mocytomas and related neoplasms [17–19]. Like 131I- and125I-MIBG, somatostatin analogs labeled with alpha- andbeta-emitters have been offered as alternatives or adjunctsto conventional chemotherapy for the treatment of me-tastatic pheochromocytomas, and beta-emitting analogslabeled with Y and Lu have been used in early clinicaltrials [20] (Table 3).
There is a growing list of positron-emitting radio-pharmaceuticals that target catecholamine synthesis orreuptake pathways to include: 11C-epinephrine, 11C-hydroxyepinephrine, 18F-fluorodopamine and 18F-fluorodi-hydroxyphenylalanine. Taking advantage of the unique
characteristics of adrenal medulla physiology, these agentshave been demonstrated to have high sensitivity andspecificity for localization of pheochromocytomas [17,21]. 18F-fluoro-2-deoxy-D-glucose (18F-FDG), a non-spe-cific tumor imaging agent, has been used to depict andstage a broad spectrum of neoplasms, including primaryand metastatic adrenal tumors, with high sensitivity andspecificity [22, 23].
Functional imaging of the adrenal cortex
Cushing syndrome
The availability of sensitive ACTH assays and the routineuse of anatomic imaging techniques for detection ofpituitary adenomas and other ACTH-secreting tumors havereduced the need for scintigraphy in the diagnosis ofACTH-dependent Cushing syndrome. Anatomic imagingin ACTH-dependent Cushing syndrome may show normaladrenals (in approximately 30% of cases) or diffusebilateral enlargement (in approximately 70% of cases),and the mean width of the adrenal limbs is positivelycorrelated with circulating cortisol and ACTH levels [24].Iodocholesterol scintigraphy has, however, been used foridentification of adrenal remnants in patients with persistentcortisol excess after bilateral adrenalectomy [5].
Primary adrenal disease causing ACTH-independentCushing syndrome is most often the result of an adrenaladenoma, or uncommonly a hypersecreting, adrenal carci-noma or bilateral cortical nodular hyperplasia. Scintigraphydepicts each of these with a distinctive pattern. Adrenaladenomas display unilateral activity on scintigraphy as a
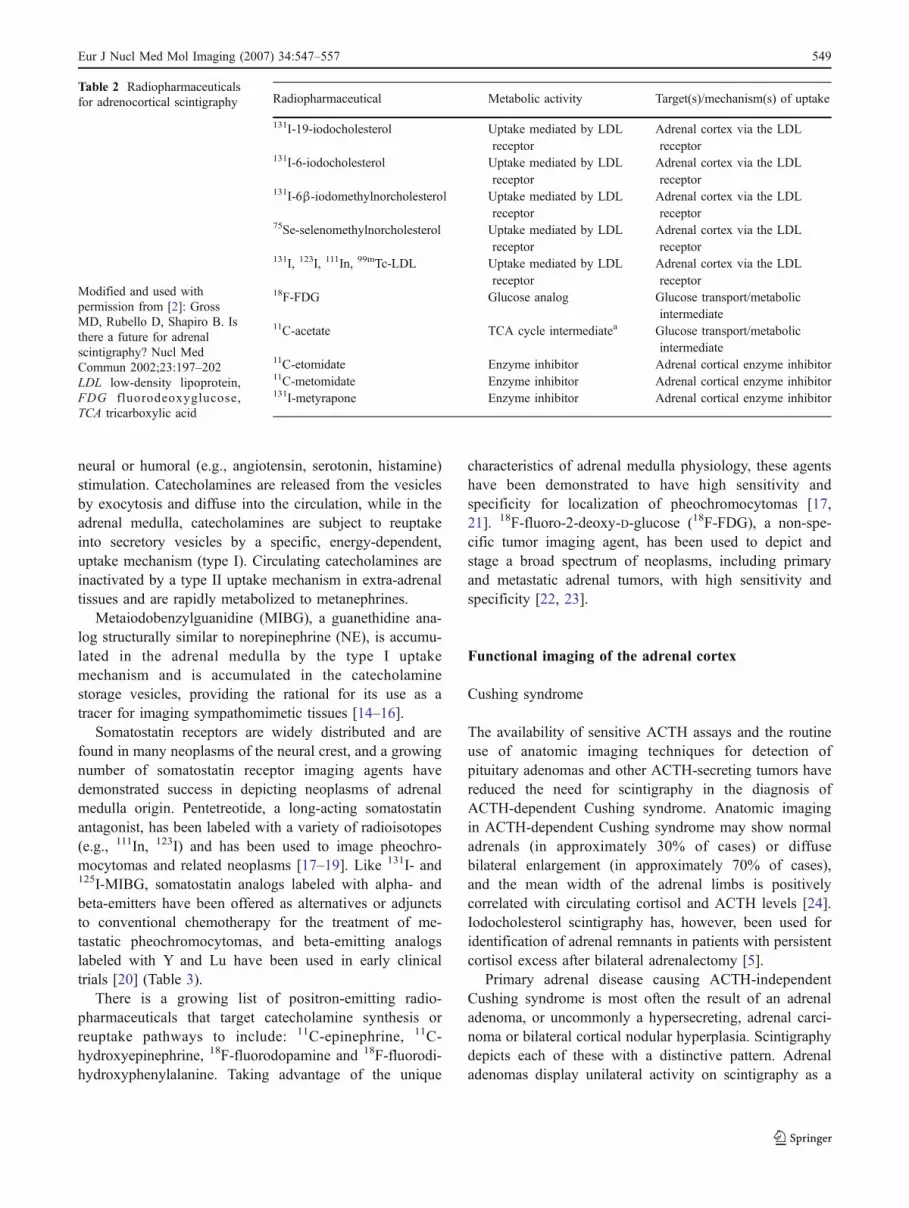
Table 2 Radiopharmaceuticalsfor adrenocortical scintigraphy
Modified and used withpermission from [2]: GrossMD, Rubello D, Shapiro B. Isthere a future for adrenalscintigraphy? Nucl MedCommun 2002;23:197–202LDL low-density lipoprotein,FDG fluorodeoxyglucose,TCA tricarboxylic acid
Radiopharmaceutical Metabolic activity Target(s)/mechanism(s) of uptake
131I-19-iodocholesterol Uptake mediated by LDLreceptor
Adrenal cortex via the LDLreceptor
131I-6-iodocholesterol Uptake mediated by LDLreceptor
Adrenal cortex via the LDLreceptor
131I-6β-iodomethylnorcholesterol Uptake mediated by LDLreceptor
Adrenal cortex via the LDLreceptor
75Se-selenomethylnorcholesterol Uptake mediated by LDLreceptor
Adrenal cortex via the LDLreceptor
131I, 123I, 111In, 99mTc-LDL Uptake mediated by LDLreceptor
Adrenal cortex via the LDLreceptor
18F-FDG Glucose analog Glucose transport/metabolicintermediate
11C-acetate TCA cycle intermediatea Glucose transport/metabolicintermediate
11C-etomidate Enzyme inhibitor Adrenal cortical enzyme inhibitor11C-metomidate Enzyme inhibitor Adrenal cortical enzyme inhibitor131I-metyrapone Enzyme inhibitor Adrenal cortical enzyme inhibitor
Eur J Nucl Med Mol Imaging (2007) 34:547–557 549
result of suppression of ACTH and tracer accumulation inthe contralateral, normal adrenal cortex [9, 25]. Bilateralcortical nodular hyperplasia, on the other hand, demon-strates bilateral uptake that is often asymmetric, reflectingthe nodular process whereby large nodules are usuallypresent in one gland with smaller nodules in the other.Functioning (hypersecreting) adrenocortical carcinomasusually do not image as a result of insufficient traceraccumulation by the tumor despite obvious Cushingsyndrome with suppression of ACTH and contralateraladrenal accumulation of radiocholesterol [7, 9, 10]. Thedegree of cellular differentiation appears to play a role inthe scintigraphic imaging of adrenal carcinoma, and thereare reports of well-differentiated tumors that have imagedwith NP-59 [26]. The clinical value of scintigraphy inACTH-independent Cushing syndrome is to distinguishunilateral adenoma from bilateral cortical nodular hyper-plasia, a distinction that may not be apparent biochemicallyor on high-resolution anatomic imaging; in this application,iodocholesterol scintigraphy has been shown to demon-strate high sensitivity and accuracy [26].
An alternative approach to adrenocortical imaging withradiocholesterol is PET with 11C-MTO [11–13, 27]. Recent
studies demonstrate that 11C-MTO can be used to distin-guish adrenocortical neoplasms (including non-secretingand hypersecretory cortical adenomas, cortical carcinoma,and macronodular hyperplasia) from non-adrenocorticaltumors (benign and malignant pheochromocytoma andmetastasis to the adrenal) with high specificity (89%) andsensitivity (96%) [28]. On the other hand, 11C-MTO PETdoes not distinguish benign adrenal neoplasms fromadrenocortical carcinoma [12, 27, 28]. It is interesting,however, that maximal SUVs in hypersecreting adrenaladenomas and an adrenocortical carcinoma were found tobe greater than in the contralateral, normal adrenal cortex,indicating relative “suppression” of contralateral adrenal11β-hydroxylase activity [12]. This is an expected conse-quence of uncontrolled unilateral hyperfunction uponpituitary ACTH, a condition that mimics the suppressionof radiocholesterol uptake by the normal contralateral,adrenal cortex in hypersecreting adrenal adenomas inACTH-independent Cushing syndrome [12]. A furtheralternative approach is to use 18F-FDG, which has beenreported to depict both primary and metastatic adrenocor-tical carcinomas and some adrenocortical adenomas andbilateral adrenal hyperplasia [13, 24, 29–32].
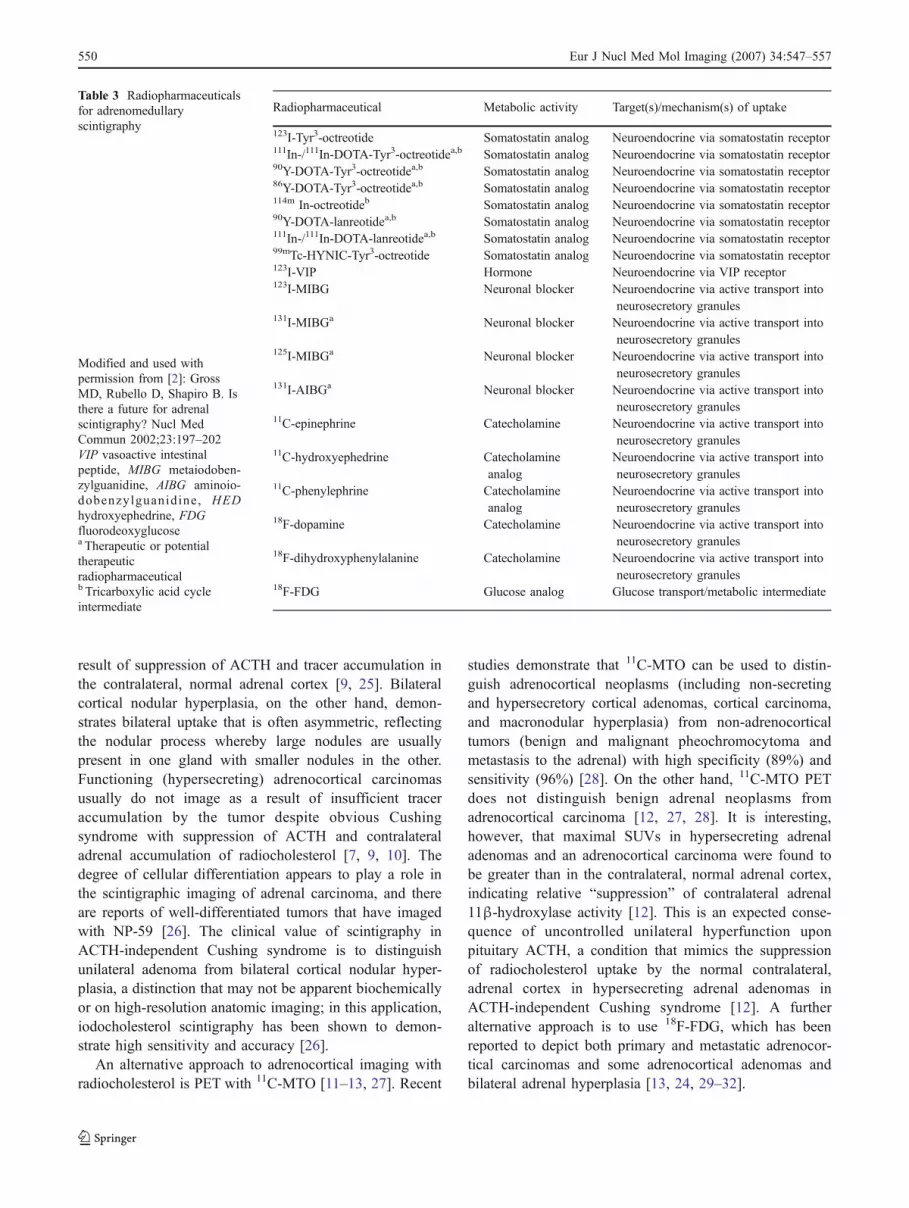
Table 3 Radiopharmaceuticalsfor adrenomedullaryscintigraphy
Modified and used withpermission from [2]: GrossMD, Rubello D, Shapiro B. Isthere a future for adrenalscintigraphy? Nucl MedCommun 2002;23:197–202VIP vasoactive intestinalpeptide, MIBG metaiodoben-zylguanidine, AIBG aminoio-dobenzylguanidine, HEDhydroxyephedrine, FDGfluorodeoxyglucosea Therapeutic or potentialtherapeuticradiopharmaceuticalb Tricarboxylic acid cycleintermediate
Radiopharmaceutical Metabolic activity Target(s)/mechanism(s) of uptake
123I-Tyr3-octreotide Somatostatin analog Neuroendocrine via somatostatin receptor111In-/111In-DOTA-Tyr3-octreotidea,b Somatostatin analog Neuroendocrine via somatostatin receptor90Y-DOTA-Tyr3-octreotidea,b Somatostatin analog Neuroendocrine via somatostatin receptor86Y-DOTA-Tyr3-octreotidea,b Somatostatin analog Neuroendocrine via somatostatin receptor114m In-octreotideb Somatostatin analog Neuroendocrine via somatostatin receptor90Y-DOTA-lanreotidea,b Somatostatin analog Neuroendocrine via somatostatin receptor111In-/111In-DOTA-lanreotidea,b Somatostatin analog Neuroendocrine via somatostatin receptor99mTc-HYNIC-Tyr3-octreotide Somatostatin analog Neuroendocrine via somatostatin receptor123I-VIP Hormone Neuroendocrine via VIP receptor123I-MIBG Neuronal blocker Neuroendocrine via active transport into
neurosecretory granules131I-MIBGa Neuronal blocker Neuroendocrine via active transport into
neurosecretory granules125I-MIBGa Neuronal blocker Neuroendocrine via active transport into
neurosecretory granules131I-AIBGa Neuronal blocker Neuroendocrine via active transport into
neurosecretory granules11C-epinephrine Catecholamine Neuroendocrine via active transport into
neurosecretory granules11C-hydroxyephedrine Catecholamine
analogNeuroendocrine via active transport intoneurosecretory granules
11C-phenylephrine Catecholamineanalog
Neuroendocrine via active transport intoneurosecretory granules
18F-dopamine Catecholamine Neuroendocrine via active transport intoneurosecretory granules
18F-dihydroxyphenylalanine Catecholamine Neuroendocrine via active transport intoneurosecretory granules
18F-FDG Glucose analog Glucose transport/metabolic intermediate
550 Eur J Nucl Med Mol Imaging (2007) 34:547–557

Primary aldosteronism
Hypersecretion of aldosterone from either an adrenaladenoma or bilateral adrenal hyperplasia characterizes thesyndrome of primary aldosteronism. Excessive aldosteronesecretion suppresses plasma renin activity and results inhypertension, hypokalemia and elevated plasma and urinaryaldosterone levels.
As a result of different secretory rates of the inner andthe outer adrenal cortex, suppression of the ACTH-dependent component of radiocholesterol uptake of theinner cortex with dexamethasone facilitates imaging andimproves the diagnostic efficacy of iodocholesterol scintig-raphy in evaluating the outer cortex in primary aldosteron-ism. Bilateral adrenal hyperplasia can be distinguished fromunilateral adrenal adenoma and normal adrenal functionbased upon the pattern of imaging, i.e., unilateral vsbilateral, and the timing of adrenal visualization [9](Fig. 1). With attention to details of concurrent medicationsthat might interfere with adrenal function and subsequentiodocholesterol accumulation, studies performed underdexamethasone suppression demonstrate high sensitivityand specificity in primary aldosteronism [9]. Imagingprotocols and interpretative algorithms using iodocholes-terol do, however, require prolonged intervals after injec-tion, and sometimes multiple imaging sessions.
The utility of PET with 11C-MTO has been reported infive patients with primary aldosteronism due to adrenaladenoma. SUVs in the abnormal adrenals ranged from 15.7to 22.0, although the ratio of maximal SUV of the
hyperfunctioning gland to that of the contralateral normalgland was 1.2 with a range of 0.9–1.7. This reflects the lackof suppression of 11β-hydroxylase activity and contrastswith the higher adenoma/normal adrenal SUV ratios thatfavor Cushing’s adenoma and hypersecreting adrenocorticalcarcinoma [13].
Incidentally discovered adrenal masses (adrenalincidentaloma)
The routine use of high-resolution imaging techniques(ultrasound, CT, and MR imaging) for evaluation ofabdominal symptoms has led to the identification of manyunsuspected adrenal lesions (incidentalomas) [22]. Multiplestudies have shown that adrenal adenomas are common (2–9%) in the general population. In the absence of a knownmalignancy, 70–94% of adrenal incidentalomas are non-hypersecreting, benign adenomas, while in the setting of aknown extra-adrenal malignancy, 50% are adrenal metasta-ses from carcinomas of the lung, breast, stomach, ovary, orkidney or from leukemia, lymphoma, or melanoma [33].Other common adrenal masses are adrenal cysts (4–22%),myelolipoma (7–15%), and pheochromocytoma (0–11%)[34].
Regardless of the potential etiology, a biochemicalevaluation sufficient to exclude a hypersecreting adrenalmass is mandatory. Although the extent of the biochemicalevaluation remains a topic of disagreement, at a minimum itshould include a representative functional analysis of allzones of the adrenal cortex and medulla.
Fig. 1 NP-59 SPECT/CT in a 65-year-old man with primary hyper-aldosteronism (Conn’s syndrome). A 0.8-cm left adrenal nodule isseen on a diagnostic CT scan (left). The scintigraphic images (middle)
demonstrate bilateral tracer activity (arrows) corresponding to theadrenal glands in an imaging pattern consistent with bilateralhyperplasia. The fused images are shown on the right
Eur J Nucl Med Mol Imaging (2007) 34:547–557 551
Computed tomography and MR imaging usually providekey anatomic clues in the characterization of incidentallydiscovered adrenal masses. Unenhanced CT density mea-surements of <10 Hounsfield units (HU) define a “lipid-rich” adenoma with a sensitivity of 71% and a specificity of98% [35]. In the case of an inhomogeneous mass or a CTdensity ≥10 HU, contrast-enhanced CT depicts adenomasas masses that demonstrate enhanced washout of contrast ascompared with adrenal metastases [36–38]. Attenuationvalues less than 30–40 HU at 15 min after contrastadministration are invariably indicative of adenomas [39].Further, a 60% percentage washout at 15 min has asensitivity of 88% and a specificity of 96% for thediagnosis of adenoma [39].
Chemical shift MR imaging can also be used todifferentiate adrenal adenomas from metastases. Anylipid-containing tissue demonstrates signal loss from fatand water on opposed-phase compared with in-phaseimages. Visual analysis of in-phase and opposed-phaseimages for the detection of lipid within adrenal masses hasa sensitivity of 78% and a specificity of 87% for adrenaladenoma [40].
While CT and MR techniques provide importantanatomic and structural detail, functional adrenal imagingusing iodocholesterol, MIBG, or FDG offers high sensitiv-ity and specificity for the characterization of incidentaladrenal lesions.
Iodocholesterol scintigraphy has been used to depictadrenal adenomas and to distinguish them from non-adenomas, including primary adrenal cancer, adrenalmetastases, cysts, hematoma/hemorrhage, lipoma, myeloli-poma, and pseudoadrenal masses [34]. In a manner akin tothat used to distinguish functioning from non-functioningthyroid nodules, three distinct scintigraphic patterns ofimaging in incidentalomas have been described. A concor-dant pattern of uptake (uptake greater on the side of themass seen on CT) is the result of a benign adrenal adenoma[34]. The contralateral adrenal gland may demonstratevariable tracer accumulation in relation to the amount ofsuppression caused by the adrenal mass. A discordantpattern of uptake with absent or decreased iodocholesteroluptake on the side of the adrenal mass depicted on CT isinvariably due to destructive or malignant processes. Anormal pattern of uptake is seen in pseudoadrenal masses.Lesions that are <1 to 2 cm may yield a non-lateralizingpattern owing to the limited spatial resolution of planarscintigraphy [34]. The increased resolution and directanatomic localization offered by SPECT/CT may be usefulin identifying small adrenal lesions [8].
Because NP-59, MIBG, and FDG target differentphysiologic processes, they can be used selectively in theevaluation of non-hypersecretory masses to identify differ-ent types of adrenal tumors [41, 42]. Employing various
radiotracers in the evaluation of incidentally discoveredadrenal masses, Maurea et al. demonstrated that inadenoma, iodocholesterol imaging has a positive predictivevalue of 89% and a negative predictive of 100% [41]. Thepositive and negative predictive values of MIBG forconfirming an adrenal mass as neuroendocrine were 83%and 100%, respectively. In the same study, FDG differen-tiated benign from malignant adrenal lesions with 100%sensitivity and specificity. On the basis of these data it hasbeen proposed that functional imaging should start withiodocholesterol scintigraphy in patients without a history ofcancer, because benign adenomas are the most commonincidentally discovered adrenal masses. In the case ofnormal iodocholesterol imaging, MIBG should be used toidentify non-hypersecreting pheochromocytoma, andshould MIBG be negative, an FDG study should follow.In patients with a prior history of malignancy, FDG shouldbe the initial study of choice, followed by the sequence ofiodocholesterol and MIBG imaging [41].
In a comparative study of MRI and radionuclidetechniques (iodocholesterol, MIBG, and FDG) for thecharacterization of non-hypersecreting unilateral adrenallesions in 30 patients, with 22 benign and eight malignantlesions, qualitative MR evaluation showed T2 signalhyperintensity in 46% of adenomas and 100% of pheo-chromocytomas, and chemical-shift MR imaging wassuccessful in distinguishing 100% of adenomas. Gadolin-ium enhancement was seen in 100% of pheochromocyto-mas and in 63% of malignant adrenal tumors [42]. Notunexpectedly, radionuclide studies showed increased iodo-cholesterol uptake in adenomas, significant MIBG accu-mulation in pheochromocytomas, and focal FDG activity inmalignant adrenal lesions [42].
Like in other non-adrenal neoplasms, FDG PET can beused to differentiate malignant from benign adrenal lesionsand metastases to the adrenals (Figs. 2, 3). In a study byYun et al. in 50 patients with known or suspectedmalignancy, FDG PET had a sensitivity of 100%, aspecificity of 94%, and an accuracy of 96% for character-ization of adrenal lesions [17]. By altering the interpretativecriteria to include lesions with FDG uptake equal to orgreater than the liver, specificity of FDG PET for detectingmalignant adrenal lesions improved, without decreasingsensitivity. In another study, by Metser et al., FDG PET/CTwas used to characterize the adrenal masses in 150 patients[23]. With a cutoff SUV of 3.1, PET alone had a sensitivityof 98.5% and a specificity of 92%; the addition of CT toPET resulted in an increase in specificity to 98% and at acutoff SUV of 3.1 all lesions were correctly identified asbenign or malignant.
In a comparative study, 11C-MTO PET and 18F-FDGPET were used in 21 patients with incidentally discoveredhypersecretory and non-hypersecretory masses including
552 Eur J Nucl Med Mol Imaging (2007) 34:547–557
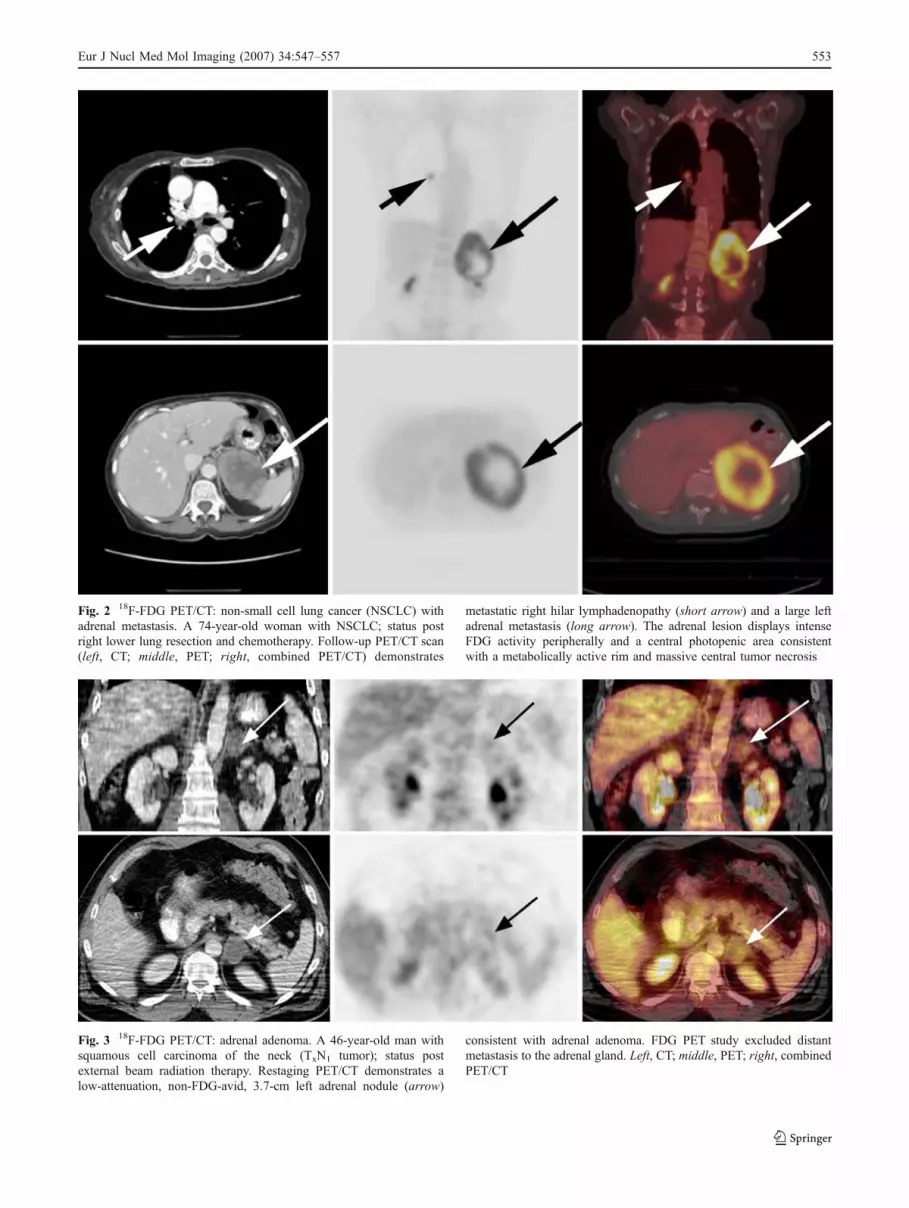
Fig. 2 18F-FDG PET/CT: non-small cell lung cancer (NSCLC) withadrenal metastasis. A 74-year-old woman with NSCLC; status postright lower lung resection and chemotherapy. Follow-up PET/CT scan(left, CT; middle, PET; right, combined PET/CT) demonstrates
metastatic right hilar lymphadenopathy (short arrow) and a large leftadrenal metastasis (long arrow). The adrenal lesion displays intenseFDG activity peripherally and a central photopenic area consistentwith a metabolically active rim and massive central tumor necrosis
Fig. 3 18F-FDG PET/CT: adrenal adenoma. A 46-year-old man withsquamous cell carcinoma of the neck (TxN1 tumor); status postexternal beam radiation therapy. Restaging PET/CT demonstrates alow-attenuation, non-FDG-avid, 3.7-cm left adrenal nodule (arrow)
consistent with adrenal adenoma. FDG PET study excluded distantmetastasis to the adrenal gland. Left, CT; middle, PET; right, combinedPET/CT
Eur J Nucl Med Mol Imaging (2007) 34:547–557 553

adrenal cancer, pheochromocytoma, cyst, lipoma, lympho-ma, and adrenal metastases, 11C-MTO identified all lesionsof adrenocortical origin, with the highest SUVs in adreno-cortical carcinoma (SUVmedian 28), followed by hyper-secretory adrenal cortical adenomas (SUVmedian 12.7) andnon-secretory adenomas (SUVmedian 12.2); non-corticaltumors demonstrated a SUVmedian of 5.7.
18F-FDG showedincreased accumulation in pheochromocytomas and adre-nocortical carcinomas, but all non-hypersecreting and mosthypersecreting adenomas demonstrated minimal or noappreciable FDG accumulation [13]. Despite the potentialvalue of an adrenocortical-specific tracer, the very shorthalf-life of 11C-MTO restricts its use to those centres withthe capacity to synthesize the compound.
Functional adrenomedullary imaging
Pheochromocytoma
Tumors arising from adrenal medulla, pheochromocytomas,hypersecrete catecholamines and in their classic presenta-tion produce symptoms of hypertension with paroxysmalheadache, palpitations, and sweating. They may arise denovo as sporadic neoplasms, are often multiple and extra-adrenal, and can occur as part of heritable multipleendocrine neoplasia syndromes [1]. Not uncommonly theymay be clinically silent and discovered incidentally [1, 3].The presence of pheochromocytoma is established withbiochemical findings of elevated plasma or urine meta-nephrines or other catecholamines or catecholamine metab-olites. Approximately 90% of pheochromocytomas occurwithin the adrenal glands; tumors are often >2 cm indiameter and as a result, most pheochromocytomas arereadily detected on CT. The majority of pheochromocyto-mas have a CT unenhanced attenuation of >10 HU.Intravenous contrast-provoked hypertensive crises, previ-ously a source of concern, have not been seen with the useof non-ionic IV contrast agents, and contrast-enhanced CTin pheochromocytoma usually shows inhomogeneous en-hancement of a solid mass, the findings being similar tothose seen in adrenal metastasis or adrenal corticalcarcinoma [37].
MR imaging has assumed a prominent role in imagingpheochromocytoma owing to its ability to define anatomicdetail and tissue characterization. Most pheochromocytomasare hypointense on T1-weighted images and hyperintense onT2-weighted images. Although pheochromocytomas can becharacterized by their hyperintensity on T2-weightedimages, there is overlap with other neoplasms, e.g., adrenalcortical carcinomas, in up to 33% of cases [43].
Scintigraphy has played, and continues to play, animportant role in imaging pheochromocytoma. MIBG
scintigraphy (using 131I or 123I with SPECT) and PET using18F-fluorodopamine (18F-DA), 18F-dihydroxyphenylalanine(18F-DOPA), 11C-epinephrine, and 11C-hydroxyephedrinehave been demonstrated to image adrenomedullary neo-plasms [6, 7, 17, 23, 44].
Regardless of the radioisotope, the patterns of imagingwith these radiopharmaceuticals are essentially the same.Sporadic intra-adrenal pheochromocytomas are depicted asintense focal collections of radioactivity. MIBG scintigra-phy has been particularly useful in imaging metastases andin the localization of extra-adrenal pheochromocytomas(Fig. 4). These lesions are often not detected by CT or MRimaging owing to their small size and their close relation-ship to other structures [45]. MIBG scintigraphy has areported sensitivity of 87% and specificity of 99% for thedetection of pheochromocytomas [15]. Radiolabeledoctreotide has been successfully used to image pheochro-mocytomas and metastases with an efficacy that is less thanthat of MIBG for intra-adrenal pheochromocytoma butsomewhat better for extra-adrenal and metastatic pheochro-mocytoma [17, 19, 20]. Thenormal distribution of MIBGincludes the salivary glands, heart, liver, colon, bladder,and,in the case of 123I-MIBG, the normal adrenal medullain approximately 20% of patients(vs <5% with 131I-MIBG).Faint accumulation of 123I-MIBG can be seen in thenormalcontralateral adrenal in patients with pheochromocytoma,although it is usuallyless than or equal to that of othertissues (e.g., liver) [46]. Metaiodobenzylguanindine labeledwith 131I and 125I has been used to treat pheochromocyto-ma, and the possibility of high-dose radiation therapy totreat metastatic pheochromocytoma using alpha- and beta-emitting labeled octreotide analogs is under investigation[17, 20].
Most pheochromocytomas are metabolically active andcan be imaged with 18F-FDG PET. Shulkin et al. identifiedpheochromocytomas with 18F-FDG in 22 of 29 patients. Inthis study pheochromocytomas that poorly concentratedMIBG were depicted with FDG, and all pheochro-mocytomas that failed to accumulate FDG were detectedwith MIBG—a finding that has been confirmed by others[23, 44]. Discordant results comparing FDG, MIBG, and18F-dopamine (DA) imaging were seen in five patients withmetastatic pheochromocytoma. Both 123I-MIBG and 18F-DAunderestimated the extent of disease when compared with
Fig. 4 123I-MIBG SPECT/CT: metastatic paraganglioma. A 52-year-old man with neurofibromatosis and paraganglioma (organ ofZuckerkandl); status post initial resection in 1998 and reinterventionin 2003 for abdominal recurrence, with persistent hypertension andelevated plasma metanephrine levels. Functional imaging demon-strates multiple MIBG-avid pulmonary nodules (arrows, a) consistentwith pulmonary metastases and large retroperitoneal soft tissue masses(arrows, b) consistent with abdominal recurrence in the sympatheticganglionic paravertebral chain (arrows). Left, CT; middle, PET; right,combined PET/CT
�
554 Eur J Nucl Med Mol Imaging (2007) 34:547–557

Eur J Nucl Med Mol Imaging (2007) 34:547–557 555

CT and MRI. 18F-FDG PET depicted lesions not detectedby 123I-MIBG or 18F-DA [18]. Hydroxyephedrine labeledwith 11C has been used to image pheochromocytomas withsuccess. Rapid and early imaging ∼10 min post injectionwas seen in nine of ten patients [47]. In a more recent studyby Trampal et al., 13 pheochromocytomas were depicted in12 patients (sensitivity 92%), with one false negativeand seven true negative studies (specificity 100%) [48].18F-fluorodopamine correctly identified 16 patients withmetastatic pheochromocytomas in which some metastaseswere not imaged with planar 131I-MIBG scans [49].
Present recommendations for depicting pheochromocy-tomas include consideration of the difficulty in predictingthe malignant potential. Thus, localization should includetwo different imaging modalities, anatomic imaging toassess structural detail (such as tumor size, invasion of therenal vein or inferior vena cava, and compression ofadjacent organs) and functional imaging to surveyfor metastases. The functional imaging test of choice is123I-MIBG (or 131I-MIBG if 123I-MIBG is not available).Should 123I-MIBG be non-localizing, PET using 18F-DA or18F-DOPA should be considered [21, 44, 49]. In the eventthat PET radiopharmaceuticals are negative, the tumor mayhave undergone dedifferentiation with loss of type 1 uptaketransporters and is probably malignant. In these instances,imaging with 18F-FDG or 111In-pentetreotide is recommen-ded to identify metastases, a not uncommon situation thathas a significant impact on subsequent therapy [7, 21, 44].
Conclusion
Anatomic imaging has assumed a preeminent role in theevaluation of adrenocortical and adrenomedullary disease.Subtle abnormalities of adrenal contour can be depicted,and for many adrenal diseases, the presence of biochemicalabnormalities and abnormal adrenal anatomy is sufficientevidence for definitive treatment. Despite this evolution inthe imaging and diagnostic approach, there are manyadrenal diseases in which high-resolution imaging, even inthe presence of biochemical evidence of disease, is notenough to assure a correct diagnosis. Functional imagingwith radiopharmaceuticals targeted to biosynthetic path-ways as substrates, enzyme inhibitors or receptor ligandsoffers unique insight into target tissues not available byother non-invasive imaging techniques. As a separatemodality, scintigraphy has demonstrable utility in theevaluation of bilateral cortical nodular, ACTH-independentCushing disease, hyperplasia in primary aldosteronism,some incidentally discovered adrenal masses, and the extentof disease and potential for malignancy in pheochromocy-toma. When combined with PET/CT or SPECT/CT,scintigraphy becomes a component of a much more
powerful modality with the ability to simultaneouslydisclose function and anatomy in adrenal diseases, con-ditions which have, in the past, been some of the mostchallenging diagnoses in medicine.
References
1. Gross MD, Korobkin M, Hussain H, et al. Adrenal gland imaging.In: Jameson JL, DeGroot LJ, editors. Endocrinology, 5th edn.Philadelphia: Saunders; 2005; p. 2425–53.
2. Gross MD, Rubello D, Shapiro B. Is there a future for adrenalscintigraphy? Nucl Med Commun 2002;23:197–202.
3. Gross MD, Shapiro B, Bui C, Shulkin B, Sisson J. Adrenalscintigraphy and metaiodobenzylguanidine therapy of neuro-endocrine tumors. In: Sandler MP, Coleman RE, Patton JA,Wackers FJT, Gottschalk A, editors. Diagnostic nuclear medicine,4th edn. Philadelphia: Lippincott Williams and Wilkins; 2003;p. 715–34.
4. Gross MD, Bui C, Shapiro B. Adrenocortical scintigraphy. In: EllPJ, Gambhir SS, editors. Nuclear medicine in clinical diagnosisand treatment, 3rd edn. Edinburgh: Churchill and Livingstone;2004; p. 45–52.
5. Avram A, Fig LM, Gross MD. Nuclear imaging of the adrenalgland. Semin Nucl Med 2006;36:212–27.
6. Eriksson B, Bergström M, Sundin A, Juhlin C, Örlefors H,Öberg K, et al. The role of PET in the localization ofneuroendocrine and adrenocortical tumors. Ann N Y Acad Sci2002;970:159–69.
7. Bombardieri E, Seregni E, Villano C, Chiti A, Bajetta E. Positionof nuclear medicine techniques in the diagnostic work-up ofneuroendocrine tumors. Q J Nucl Med 2004;48:150–63.
8. Kainberger F, Kurtaran A, Keinast O, Dobrozemsky G, Czerny C,Kletter K. Hybrid imaging for endocrine diseases: new perspec-tives. Weiner Klin Wochen 2003;115 (Suppl 2):87–90.
9. Gross MD, Valk TW, Thrall JH, Beierwaltes WH. The role ofpharmacologic manipulation in adrenal cortical scintigraphy.Semin Nucl Med 1981;11:128–48.
10. Gross MD, Shapiro, B. Scintigraphic studies in adrenal hyperten-sion. Semin Nucl Med 1990;19:122–43.
11. Pacak K, Eisenhofer G, Goldstein DS. Functional imaging ofendocrine tumors: role of positron emission tomography. EndocrRev 2004;25:568–80.
12. Minn H, Salonen A, Friberg J, Roivainen A, Viljanen T, LangsjoJ, et al. Imaging of adrenal incidentalomas with PET using 11C-metomidate and 18F-FDG. J Nucl Med 2004;45:972–9.
13. Zettinig G, Mitterhauser M, Wadsak W, Becherer A, Pirich C,Vierhapper H, et al. Positron emission tomography imaging ofadrenal masses: 18F-fluorodeoxyglucose and the 11β-hydroxylasetracer 11C-metomidate. Eur J Nucl Med Mol Imaging2004;31:1224–30.
14. Sisson JC, Frager MS, Valk TW, Gross MD, Swanson DP,Wieland DM, et al. Scintigraphic localization of pheochromocy-toma. N Engl J Med 1981;305:12–7.
15. Rubello D, Bui C, Casara D, Gross MD, Fig LM, Shapiro B.Functional scintigraphy of the adrenal gland. Eur J Endocrinol2002;147(1):13–28.
16. Gross MD, Shapiro B, Shreve P. Radionuclide imaging of theadrenal cortex. Q J Nucl Med 1999;43:224–32.
17. Ilias I, Pacak K. Anatomical and functional imaging of metastaticpheochromocytoma. Ann N Y Acad Sci 2004;1018:495–504.
18. Mamede M, Carrasquillo JA, Chen CC, Del Corral P, Whatley M,Ilias I, et al. Discordant localization of 2-[18F]-fluoro-2-deoxy-D-
556 Eur J Nucl Med Mol Imaging (2007) 34:547–557
glucose in 6-[18F]-fluorodopamine- and [123I]-metaiodobenzyl-guanidine-negative metastatic pheochromocytoma sites. Nucl MedCommun 2006;27(1):31–6.
19. Van der Harst E, de Herder WW, Bruining HA, Bonjer HJ, deKrijger RR, Lamberts SW, et al. 123I-metaiodobenzylguanidineand 111In-octreotide uptake in benign and malignant pheochro-mocytomas. J Clin Endocrinol Metab 2001;86:685–93.
20. Shapiro B, Gross MD, Shulkin B. Radioisotope diagnosis andtherapy of malignant pheochromocytomas. Trends EndocrinolMetab 2001;12:469–75.
21. Eriksson B, Bergström M, Sundin A, Juhlin C, Örlefors H, ÖbergK, et al. The role of PET in the localization of neuroendocrine andadrenocortical tumors. Ann N Y Acad Sci 2002;970:159–69.
22. Yun M, Kim W, Alnafisi N, Lacorte L, Jang S, Alavi A. 18F-FDGPET in characterizing adrenal lesions detected on CT or MRI.J Nucl Med 2001;42:1795–9.
23. Metser U, Miller E, Lerman H, Lievshitz G, Avital S, Even-SapirE. 18F-FDG PET/CT in the evaluation of adrenal masses. J NuclMed 2006;47:32–7.
24. Sohaib SA, Hanson JA, Reznek RH, Trainer PJ, Monson JP,Grossman AB, et al. CT appearance of the adrenal glands inadrenocorticotrophic hormone-dependent Cushing syndrome. AmJ Roentgenol AJR 1999;172:997–1002.
25. Schteingart DE, Seabold JE, Gross MD, Swanson D. Iodocholes-terol adrenal tissue uptake and imaging in adrenal neoplasms. JClin Endocrinol Metab 1981;52:1156–62.
26. Fig LM, Ehrmann D, Gross MD, Shapiro B, Schteingart D, GlazerD. The localization of abnormal adrenal function in the ACTH-independent Cushing syndrome. Ann Intern Med 1988;109:547–53.
27. Khan TS, Sundin A, Juhlin C, Långström B, Bergström M,Eriksson B. 11C-metomidate imaging of adrenocortical cancer. EurJ Nucl Med Mol Imaging 2003;30:403–10.
28. Hennings J, Lindhe Ö, Bergström M, Långström B, Sundin A,Hellman P. [11C]metomidate positron emission tomography ofadrenocortical tumors in correlation with histopathological find-ings. J Clin Endocrinol Metab 2006;91:1410–4.
29. Tenenbaum F, Groussin L, Foehrenbach H, Tissier F, Gouya H,Berherat J, et al. 18F-fluorodeoxyglucose positron emissiontomography as a diagnostic tool for malignancy of adrenocorticaltumors? Preliminary results in 13 consecutive patients. Eur JEndocrinol 2004;150:789–92.
30. Fassnacht M, Kenn W, Allolio B. Adrenal tumors: how toestablish malignancy? J Endocrinol Invest 2004;27:387–99.
31. Rao SK, Caride VJ, Ponn R, Giakovis E, Lee SH. F-18fluorodeoxyglucose positron emission tomography-positive be-nign adrenal cortical adenoma: imaging features and pathologiccorrelation. Clin Nucl Med 2004;29(5):300–2.
32. Shimizu A, Oriuchi N, Tsushima Y. High [18F] 2-fluoro-2-deoxy-D-glucose (FDG) uptake of adrenocortical adenoma show-ing subclinical Cushing’s syndrome. Ann Nucl Med 2003;17(5):403–6.
33. Frilling A, Tecklenborg K, Weber F, Kühl H, Müller S, StamatisG, et al. Importance of adrenal incidentaloma in patients with ahistory of malignancy. Surgery 2004;136:1289–96.
34. Kloos RT, Gross MD, Francis IR. Incidentally discovered adrenalmasses. Endocr Rev 1995;16:460–84.
35. Boland GW, Lee MJ, Gazelle GS, Halpern EF, McNicholas MM,Mueller PR. Characterization of adrenal masses using unenhancedCT: an analysis of the CT literature. Am J Roentgenol AJR1998;171:201–4.
36. Szolar DH, Korobkin M, Reittner P, Berghold A, Bauernhofer T,Trummer H, et al. Adrenocortical carcinomas and adrenalpheochromocytomas: mass and enhancement loss evaluation atdelayed contrast-enhanced CT. Radiology 2005;234:479–85.
37. Al-Hawary MM, Francis IR, Korobkin M. Non-invasive evalua-tion of the incidentally detected indeterminate adrenal mass. BestPract Res Clin Endocrinol Metab 2005;19:277–92.
38. Sahdev A, Reznek RH. Imaging evaluation of the non-functioningindeterminate adrenal mass. Trends Endocrinol Metab2004;15:272–6.
39. Korobkin M, Brodeur FJ, Francis IR, Quint LE, Dunnick NR,Londy F. CT time-attenuation washout curves of adrenaladenomas and nonadenomas. Am J Roentgenol AJR 1998;170:747–52.
40. Outwater EK, Siegelman ES, Radecki PD, Piccoli CW, MitchellDG. Distinction between benign and malignant adrenal masses:value of T1-weighted chemical-shift MR imaging. A J RoentgenolAJR 1995;165:579–83.
41. Maurea S, Klain M, Mainolfi C, Ziviello M, Salvatore M. Thediagnostic role of radionuclide imaging in evaluation of patientswith nonhypersecreting adrenal masses. J Nucl Med 2004;42:884–92.
42. Maurea S, Caraco C, Klain M, Mainolfi M, Salvatore M. Imagingcharacterization of non-hypersecreting adrenal masses. Compari-son between MR and radionuclide techniques. Q J Nucl Med MolImaging 2004;48:188–97.
43. Francis IR, Korobkin M. Pheochromocytoma. Radiol Clin NorthAm 1996;34:1101–12.
44. Ilias I, Pacak K. Diagnosis and management of tumors of theadrenal medulla. Horm Metab Res 2005;37:717–21.
45. Shapiro B, Sisson J, Kalff V, Glowniak J, Satterlee W, Glazer G,et al. The location of middle mediastinal pheochromocytomas.J Thorac Cardiovasc Surg 1984;87:814–20.
46. Hay RV, Gross MD. Scintigraphic imaging of the adrenals andneuroectodermal tumors. In: Henkin RE, Bova D, Karesh SM,Dillehey GL, Wagner RH, Halama JR, Zimmer AM, editors.Nuclear medicine, 2nd edn. Philadelphia: Mosby; 2006; p. 820–44.
47. Ilias I, Shulkin B, Pacak K. New functional imaging modalitiesfor chromaffin tumors, neuroblastoma and ganglioneuromas.Trends Endocrinol Metab 2005;16:66–72.
48. Trampal C, Engler H, Juhlin C, Bergström M, Långström B.Pheochromocytomas: detection with 11C hydroxyephedrine PET.Radiology 2004;230:423–8.
49. Ilias I, Jorge JY, Carrasquillo JA, Chen CC, Eisenhofer G,Whatley M, et al. Superiority of 6-[18F]-fluorodopamine positronemission tomography versus [131I]-metaiodobenzylguanidine scin-tigraphy in the localization of metastatic pheochromocytoma.J Clin Endocrinol Metab 2003;88:4083–7.
Eur J Nucl Med Mol Imaging (2007) 34:547–557 557





























