Embed Size (px)
Citation preview

www.biomedcentral.com/bmcpregnancychildbirth
BMCPregnancy and Childbirth
Summary of contentsThe 3.2 million stillbirths that occur worldwide each year are largely absent from global data tracking, policy dialogue and pro-grammes. Limitations of global stillbirth data and a lack of consensus surrounding priority interventions render stillbirths invisible inpolicy and programmes. This supplement provides an in-depth analysis of the burden and evidence base for potential interventionsto avert stillbirths. Lead investigators from the Aga Khan University (Karachi, Pakistan), supported by colleagues from Johns HopkinsUniversity (Baltimore, USA) and Saving Newborn Lives (South Africa), reviewed evidence for impact of interventions to prevent still-births and strategies for delivering them.
Paper 1 (www.biomedcentral.com/1471-2393/9/S1/S2) describes risk factors for and causes of stillbirth, challenges in measuringthe global burden of stillbirths including a lack of cause-specific data, social factors that keep stillbirths hidden, and the lack of afeasible, internationally comparable classification system for stillbirth. The paper concludes by outlining the methodology and frame-work for this comprehensive global assessment of evidence for intervention impact and health systems strategies to deliver inter-ventions to reduce the global burden of stillbirths.
Poor nutritional status, inadequate antenatal care and social behaviours before and during pregnancy increase stillbirth risk in manyresource-poor settings. Paper 2 (www.biomedcentral.com/1471-2393/9/S1/S3) reviews twelve interventions for behavioural andsocially mediated risk factors, including exposures to harm from female genital mutilation, tobacco use, and indoor air pollution; ante-natal care; and maternal nutritional supplementation.
Maternal infections including syphilis and malaria, and maternal conditions including hypertensive disorders, are known risk factorsfor stillbirth. Paper 3 (www.biomedcentral.com/1471-2393/9/S1/S4) reviews evidence for impact on stillbirths of 16 clinical inter-ventions during pregnancy, including interventions to address chronic and pregnancy-induced hypertension and prevention of pre-eclampsia; auto-immune and coagulation disorders; obstetric intrahepatic cholestasis; cervical incompetence; and infections includ-ing helminthiases, bacteriuria, periodontal disease, syphilis, and malaria.
Screening and monitoring technologies can identify high-risk pregnancies and monitor fetal well-being, and appropriate subsequentmanagement of the maternal and fetal risk factors and complications identified could prevent stillbirths. Paper 4 (www.biomedcen-tral.com/1471-2393/9/S1/S5) examines the evidence for impact on stillbirth of 14 screening and monitoring interventions in preg-nancy, including fetal movement monitoring, ultrasound and Doppler studies, diabetes screening and management; advanced fetalsurveillance techniques including non-stress testing, amniotic fluid assessment, and biophysical profile; and monitoring of labourusing the partograph or intrapartum cardiotocography.
Most intrapartum stillbirths occur in low- and middle-income countries and are associated with absent, inadequate, or delayedobstetric care. Because quality obstetric care could prevent intrapartum stillbirths, Paper 5 (www.biomedcentral.com/1471-2393/9/S1/S6) assesses the evidence for impact of eight interventions delivered antepartally or during labour, including operativedelivery, emergency obstetric care, induction of labour, treatment of pre-eclampsia and eclampsia, maternal hyperoxygenation, andamnioinfusion.
The final paper in the series, Paper 6 (www.biomedcentral.com/1471-2393/9/S1/S7), assesses the evidence for strategies to deliv-er evidence-based interventions within health systems, particularly in low-/middle-income countries where 98% of the world’s still-births occur. Innovative community and health systems strategies are evaluated, including community loan schemes and maternitywaiting homes to minimise cost and distance barriers; training (including task-shifting and drills) for different cadres of health work-ers to improve quality of antenatal and intrapartum care; and perinatal audit systems to identify deficiencies in care. Findings are syn-thesized across the series of papers and used to formulate programme and policy recommendations for optimal delivery of evidence-based interventions to prevent stillbirths at all levels of the health system and across the continuum of care. Further analysis of inter-ventions and delivery strategies is continuing in collaboration with the Global Alliance for Prevention of Prematurity andStillbirths (GAPPS).
stillbirth prelims.qxp 30/04/2009 15:31 Page 5

Volume 9 Supplement 1May 2009
www.biomedcentral.com/bmcpregnancychildbirth
BMCPregnancy and Childbirth
Contents
Commentary: reducing the world’s stillbirths Robert L Goldenberg, Elizabeth M McClure, José M Belizán
www.biomedcentral.com/1471-2393/9/S1/S1
Paper 13.2 million stillbirths: epidemiology and overview of the evidence review Joy E Lawn, Mohammad Yawar Yakoob, Rachel A Haws, Tanya Soomro, Gary L Darmstadt, Zulfiqar A Bhutta
www.biomedcentral.com/1471-2393/9/S1/S2
Paper 2Reducing stillbirths: behavioural and nutritional interventions before and during pregnancy Mohammad Yawar Yakoob, Esme V Menezes, Tanya Soomro, Rachel A Haws, Gary L Darmstadt, Zulfiqar A Bhutta
www.biomedcentral.com/1471-2393/9/S1/S3
Paper 3Reducing stillbirths: prevention and management of medical disorders and infections during pregnancy Esme V Menezes, Mohammad Yawar Yakoob, Tanya Soomro, Rachel A Haws, Gary L Darmstadt, Zulfiqar A Bhutta
www.biomedcentral.com/1471-2393/9/S1/S4
Paper 4Reducing stillbirths: screening and monitoring during pregnancy and labourRachel A Haws, Mohammad Yawar Yakoob, Tanya Soomro, Esme V Menezes, Gary L Darmstadt, Zulfiqar A Bhutta
www.biomedcentral.com/1471-2393/9/S1/S5
Paper 5Reducing stillbirths: interventions during labourGary L Darmstadt, Mohammad Yawar Yakoob, Rachel A Haws, Esme V. Menezes, Tanya Soomro, Zulfiqar A Bhutta
www.biomedcentral.com/1471-2393/9/S1/S6
Paper 6Delivering interventions to reduce the global burden of stillbirths: improving service supply and community demandZulfiqar A Bhutta, Gary L Darmstadt, Rachel A Haws, Mohammad Yawar Yakoob, Joy E Lawn
www.biomedcentral.com/1471-2393/9/S1/S7
stillbirth prelims.qxp 30/04/2009 15:31 Page 3

Stillbirths – the global picture and evidence-based solutions
An Executive Summary for the BMC Pregnancy and Childbirth Supplement
Photo credit: Save the Children/Jeff Holt

The BMC Pregnancy and Childbirth Supplement, “Stillbirths – the global picture and evidence-based solutions” provides a detailed assessment of the 3.2 million stillbirths that occur worldwide each year, which are largely absent from global data tracking, policy dialogue and programmes. Stillbirths are a major burden in both high-income and low- and middle-income countries, but have received low priority in both settings. However, stillbirth rates are particularly high and attention is most lacking in policy and programmes in low-income countries. This supplement contains six papers [1-6] and one commentary that provide an in-depth analysis of the burden and evidence base for interventions to avert stillbirths. Lead investigators from Aga Khan University (Karachi, Pakistan), supported by colleagues from Johns Hopkins University (Baltimore, USA) and Saving Newborn Lives/Save the Children (Cape Town, South Africa), reviewed the evidence for impact of interventions to prevent stillbirths and strategies for delivering effective interventions in low- and middle-income settings.
The aim of the Supplement was to provide a comprehensive, global review of available information on stillbirths, with main objectives to:1) elucidate the epidemiology and major risk factors for stillbirths [1];2) evaluate potential interventions and strategies to deliver these interventions, categorising their level of evidence and highlighting key implementation, monitoring and research gaps [2-6]; and 3) place the available evidence for interventions in a health systems context to guide programme implementation [6].
KEY MESSAGES1. Stillbirths are invisible in policy and programmes, yet constitute an enormous burden of
deaths, and disproportionately affect the poor. • 3.2 million deaths: 2.2 million antepartum stillbirths and 1.0 million intrapartum
stillbirths • 98% of the world’s stillbirths occur in low- and middle-income countries
2. We reviewed the evidence for interventions to be implemented at all levels of the health system, along the continuum of care from pre-pregnancy through labour, including interventions:
• Before and during pregnancy, especially those that are feasible in family and community settings
• For screening and monitoring during pregnancy and labour• During labour (i.e. intrapartum)
3. Many interventions of benefi t for preventing stillbirths can be delivered effectively through or alongside existing maternal, newborn and child health (MNCH) programmes.
4. Recommended implementation and research actions include to:• Improve rates of skilled birth attendance and access to emergency obstetric care• Identify and address maternal infections, especially syphilis and malaria in endemic areas• Promote quality antenatal care and referral systems as a platform for improving
coverage of evidence-based interventions• Systematically map and address stillbirth research gaps
Photo credits: Save the Children/Ahmed El-Nemr; Save the Children/Chris Taylor; Save the Children/Jonathan Hubschman
2

INVISIBILITY OF STILLBIRTHS [Paper 1]
More than 3.2 million stillbirths occur globally each year, yet stillbirths are largely invisible in global health indicators, policies, and programmes [7]. This mismatch of burden to action is due to a number of factors that keep stillbirths hidden, notably a lack of data and a lack of consensus on priority interventions, but also social taboos that reduce the visibility and global count of stillbirths. Inconsistent defi nitions cause additional confusion and hamper the recognition of stillbirths as a public health concern (panel 1).
Whilst there are estimates of the numbers of stillbirths and the size of the burden relative to other time periods in the life cycle (Figure 1), there have been no systematic global analyses and estimates of the causes of stillbirths. A systematic estimate based on 194 countries, using data from 2005, suggested that a total of 1.02 million intrapartum stillbirths due to all causes occur globally per annum [8], emphasising the importance of interventions during childbirth.
There are at least 35 classifi cation systems for stillbirths, and most are complex and primarily focused on data available only in high-income countries. This is a major challenge to developing national and global estimates for causes of stillbirth. This Supplement proposes a programmatic classifi cation that is feasible and comparable across settings.
METHODS AND SEARCHES [Paper 1]
A systematic review was undertaken of all available evidence for the impact of interventions on stillbirths. Searches included electronic reference libraries of indexed (PubMed/MEDLINE, POPLINE, LILACS, and WHO regional databases) and non-indexed medical journals, as well as published analytical reviews and meta-analyses (Cochrane Reference Libraries). Manual reviews were conducted to incorporate relevant grey literature, including theses, monographs, and project documentation. Studies were included if they (1) detailed an intervention that could reduce stillbirth incidence through a biologically plausible pathway, and (2) reported stillbirth rate, fetal death rate, perinatal mortality rate, or data allowing calculation of such a rate as an outcome measure.
Altogether, over 97,000 paper titles and nearly 12,800 abstracts were screened, and over 1000 reviews and studies on interventions to avert stillbirths or perinatal deaths were reviewed in detail using SIGN and GRADE criteria. The evidence of benefi t for each intervention was synthesised within the following categories: clear evidence (recommended for inclusion and scaling up in programmes), some evidence (can include in programmes but further research is recommended), uncertain evidence (more research is needed before including in programmes), or no/negative evidence (not recommended for inclusion in programmes). The evidence was then separated into 1) specifi c interventions, and 2) strategies to improve service delivery and community demand.
PANEL 1 - DEFINITIONS [1]
Fetal death: According to International Classifi cation of Disease, revision 10 (ICD 10), an early fetal death is death of a fetus weighing at least 500 g (or if birthweight is unavailable then after 22 weeks gestation, or with a crown-heel length of 25 cm or more). A late fetal death is defi ned as death of a fetus weighing at least 1000 g (or a gestational age of 28 completed weeks or a crown heel length of 35 cm or more). Late fetal deaths are recommended by the World Health Organization as the measure for international comparison.Stillbirths: Stillbirth is the colloquial term commonly used for fetal death, and is the term used in this series to refer to both early and late fetal deaths.Stillbirth rate: As the data used here is for international comparison, all stillbirth rate data refer to late fetal deaths i.e. the number of babies born dead after 28 weeks of gestation per 1,000 total births. Perinatal period: This time interval includes some portion of late pregnancy and some or all of the fi rst month of life. It has been used to refer to at least 10 different time periods depending on the time period cut-offs used. The term “perinatal” is also used to refer to some, but not all, causes of neonatal death in the ICD-10. Hence, the term often causes confusion. We use perinatal deaths to include stillbirths after 28 weeks gestational age and early neonatal deaths in the fi rst 7 days of life. In general, however, we have specifi ed the outcome (stillbirth, or neonatal death) or the cause of death where the data have allowed this distinction.
FIGURE 1: Stillbirths – the mortality burden compared to other linked global mortality burdens
2.6
3.2
2.63
3.2
3.8
0
1
2
3
4
5
STLLBIRTHS (from
28 weeks
gestation)
NEONATAL
DEATHS ( 0 - 28
days)
POSTNEONATAL
INFANT DEATHS
(28 - 364.9 days)
CHILD DEATHS
AGED 1 TO 4.99
YEARS
ADULT DEATHS
DUE TO AIDS
Intrapartum related deaths Antepartum
3.8
Intrapartum-related deaths Antepartum
STILLBIRTHS (from 28 weeks
gestation)
0
1
2
3
4
5
3.2
NEONATAL DEATHS
(0 - 28 days)
POSTNEONATAL INFANT DEATHS (28 - 364.9 days)
CHILD DEATHS
AGED 1 TO 4.99 YEARS
ADULT DEATHS
DUE TO AIDS
3.8
2.6
3.2
2.63
DEA
TH
S (M
ILLI
ON
S)
3

RESULTS [Papers 2-6]
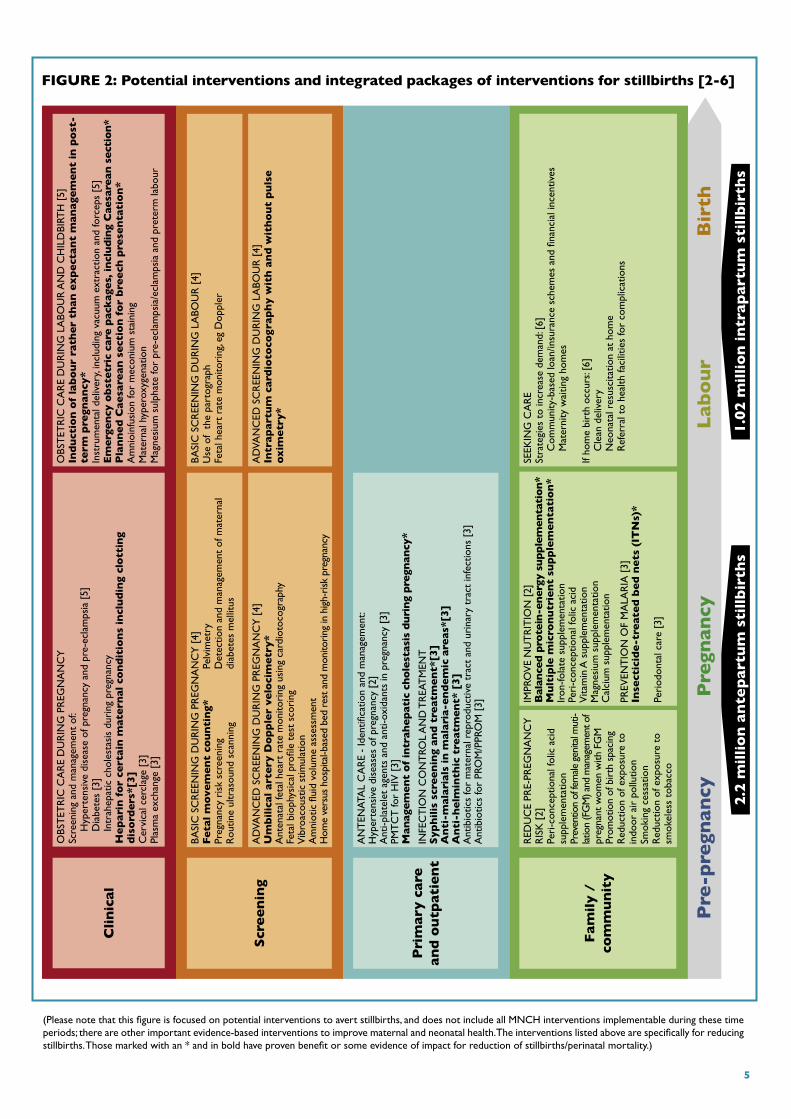
The Supplement systematically evaluated a total of 62 different maternal interventions for prevention of stillbirths. These interventions included general supportive measures to improve environmental and social conditions, as well as interventions that address maternal nutrition, infections, and other conditions during pregnancy and childbirth. The selection of these specific interventions was based on biological plausibility and possibility of inclusion as a component in antenatal and intrapartum health care programmes. Figure 2 displays these interventions along the continuum of care from pre-pregnancy through labour.
The intervention evaluations were separated into six papers as follows: epidemiology, global burden and risk factors for stillbirths [1]; behavioural and nutritional interventions before and during pregnancy [2]; interventions during pregnancy for management and prevention of medical disorders and infections [3]; interventions for screening and monitoring [4]; interventions during labour [5]; and strategies to improve service delivery and community demand [6].
Based on analysis of the evidence for impact of the different peri-conceptional, antenatal, and intrapartum maternal interventions on prevention of stillbirths, the interventions were categorised into levels according to the strength and quality of evidence, and therefore, the level of confidence in recommending interventions for wide-scale delivery in programmes. Five interventions with proven benefit in reducing stillbirths were identified, while another nine interventions had some evidence of impact (Table 1).
Strategies to deliver these interventions, including overcoming barriers to accessing care, task-shifting to other cadres of community health workers, and quality improvement strategies including obstetric drills and perinatal audit, were also evaluated. Evidence clearly supported financial incentives to improve access to emergency obstetric care and—in settings where adequate skilled personnel cannot be trained in the short term—training traditional birth attendants in clean delivery, while building linkages with health systems for referrals. Other delivery strategies had some evidence of impact but require further operational research, including training cadres of community health workers, training professional midwives in antenatal and intrapartum care, training in neonatal resuscitation for physicians and other health workers, and home birth with skilled attendance (versus hospital birth). Some evidence suggests that perinatal audit can improve care quality and subsequent perinatal outcomes, but data were unavailable to assess the impact on stillbirths of promising quality improvement strategies such as obstetric drills for Caesarean section and shoulder dystocia.
Table 1: Interventions with proven benefit or some evidence in reducing stillbirths
Interventions with proven benefit in reducing stillbirths
• Syphilis screening and treatment• Use of insecticide-treated bednets in malaria-endemic areas during pregnancy• Administration of heparin for certain maternal conditions including auto-immune
and clotting disorders• Emergency obstetric care• Planned Caesarean section for breech delivery
Interventions with some evidence of impact
• Multiple micronutrient supplementation during pregnancy• Balanced protein-energy supplementation during pregnancy• Management of intrahepatic cholestasis during pregnancy• Anti-helminthic treatment• Anti-malarials in malaria-endemic areas• Fetal movement counting for high-risk pregnancies• Umbilical artery Doppler velocimetry for high-risk pregnancies• Intrapartum cardiotocography with or without pulse oximetry• Elective induction of labour in post-term pregnancy.
4
Cli
nic
al
Scr
ee
nin
g
Pri
mary
care
an
d o
utp
atie
nt
Fam
ily /
co
mm
un
ity
OBS
TET
RIC
CA
RE
DU
RIN
G P
REG
NA
NC
YSc
reen
ing
and
man
agem
ent
of:
Hyp
erte
nsiv
e di
seas
e of
pre
gnan
cy a
nd p
re-e
clam
psia
[5]
Dia
bete
s [3
] In
trah
epat
ic c
hole
stas
is d
urin
g pr
egna
ncy
He
pari
n f
or
cert
ain
mat
ern
al c
on
dit
ion
s in
clu
din
g cl
ott
ing
dis
ord
ers
*[3]
Cer
vica
l cer
clag
e [3
]Pl
asm
a ex
chan
ge [
3]
AN
TEN
ATA
L C
AR
E -
Iden
tifica
tion
and
man
agem
ent:
Hyp
erte
nsiv
e di
seas
es o
f pre
gnan
cy [
2]A
nti-p
late
let
agen
ts a
nd a
nti-o
xida
nts
in p
regn
ancy
[3]
PMT
CT
for
HIV
[3]
Man
agem
en
t o
f in
trah
ep
atic
ch
ole
stas
is d
uri
ng
pre
gnan
cy*
INFE
CT
ION
CO
NT
ROL
AN
D T
REA
TM
ENT
Syp
hil
is s
cre
en
ing
an
d t
reat
me
nt*
[3]
An
ti-m
alari
als
in m
alari
a-e
nd
em
ic a
reas
*[3
]A
nti
-he
lmin
thic
tre
atm
en
t* [
3]
Ant
ibio
tics
for
mat
erna
l rep
rodu
ctiv
e tr
act
and
urin
ary
trac
t in
fect
ions
[3]
Ant
ibio
tics
for
PRO
M/P
PRO
M [
3]
RED
UC
E PR
E-PR
EGN
AN
CY
R
ISK
[2]
Peri
-con
cept
iona
l fol
ic a
cid
supp
lem
enta
tion
Prev
entio
n of
fem
ale g
enita
l mut
i-lat
ion
(FG
M) a
nd m
anag
emen
t of
preg
nant
wom
en w
ith F
GM
Prom
otio
n of
bir
th s
paci
ng
Red
uctio
n of
exp
osur
e to
in
door
air
pol
lutio
n
Smok
ing
cess
atio
n R
educ
tion
of e
xpos
ure
to
smok
eles
s to
bacc
o
OBS
TET
RIC
CA
RE
DU
RIN
G L
ABO
UR
AN
D C
HIL
DBI
RTH
[5]
Ind
uct
ion
of
lab
ou
r ra
the
r th
an
ex
pe
ctan
t m
an
age
me
nt
in p
ost
-te
rm p
regn
an
cy*
Inst
rum
enta
l del
iver
y, in
clud
ing
vacu
um e
xtra
ctio
n an
d fo
rcep
s [5
] E
merg
en
cy o
bst
etr
ic c
are p
ack
ages,
in
clu
din
g C
aesa
rean
sect
ion
*P
lan
ne
d C
aesa
rean
se
ctio
n f
or
bre
ech
pre
sen
tati
on
* A
mni
oinf
usio
n fo
r m
econ
ium
sta
inin
gM
ater
nal h
yper
oxyg
enat
ion
Mag
nesi
um s
ulph
ate
for
pre-
ecla
mps
ia/e
clam
psia
and
pre
term
labo
ur
BA
SIC
SC
REE
NIN
G D
UR
ING
PR
EGN
AN
CY
[4]
Fe
tal
mo
vem
en
t co
un
tin
g*Pr
egna
ncy
risk
scr
eeni
ng
R
outin
e ul
tras
ound
sca
nnin
g
BA
SIC
SC
REE
NIN
G D
UR
ING
LA
BOU
R [
4]U
se o
f th
e pa
rtog
raph
Feta
l hea
rt r
ate
mon
itori
ng, e
g D
oppl
er
IMPR
OV
E N
UT
RIT
ION
[2]
Bal
ance
d p
rote
in-e
ner
gy s
up
ple
men
tati
on
*M
ult
iple
mic
ron
utr
ien
t su
pp
lem
en
tati
on
*Ir
on-fo
late
sup
plem
enta
tion
Peri
-con
cept
iona
l fol
ic a
cid
Vita
min
A s
uppl
emen
tatio
nM
agne
sium
sup
plem
enta
tion
Cal
cium
sup
plem
enta
tion
PREV
ENT
ION
OF
MA
LAR
IA [
3]In
sect
icid
e-t
reat
ed
be
d n
ets
(IT
Ns)
*
Peri
odon
tal c
are
[3]
SEEK
ING
CA
RE
Stra
tegi
es t
o in
crea
se d
eman
d: [
6]C
omm
unity
-bas
ed lo
an/in
sura
nce
sche
mes
and
fina
ncia
l inc
entiv
esM
ater
nity
wai
ting
hom
es
If ho
me
birt
h oc
curs
: [6]
Cle
an d
eliv
ery
Neo
nata
l res
usci
tatio
n at
hom
eR
efer
ral t
o he
alth
faci
litie
s fo
r co
mpl
icat
ions
Pre
-pre
gnan
cyP
regn
an
cyB
irth
Lab
ou
r
Pelv
imet
ryD
etec
tion
and
man
agem
ent
of m
ater
nal
diab
etes
mel
litus
AD
VAN
CED
SC
REE
NIN
G D
UR
ING
PR
EGN
AN
CY
[4]
Um
bil
ical
art
ery
Do
pp
ler
velo
cim
etr
y*
Ant
enat
al fe
tal h
eart
rat
e m
onito
ring
usi
ng c
ardi
otoc
ogra
phy
Feta
l bio
phys
ical
pro
file
test
sco
ring
Vib
roac
oust
ic s
timul
atio
nA
mni
otic
flui
d vo
lum
e as
sess
men
tH
ome
vers
us h
ospi
tal-b
ased
bed
res
t and
mon
itori
ng in
hig
h-ri
sk p
regn
ancy
AD
VAN
CED
SC
REE
NIN
G D
UR
ING
LA
BOU
R [
4]In
trap
art
um
card
ioto
cog
rap
hy w
ith
an
d w
ith
ou
t p
uls
e
ox
ime
try*
2.2
mil
lio
n a
nte
part
um
sti
llb
irth
s1.0
2 m
illi
on
in
trap
art
um
sti
llb
irth
s
FIGURE 2: Potential interventions and integrated packages of interventions for stillbirths [2-6]
(Please note that this figure is focused on potential interventions to avert stillbirths, and does not include all MNCH interventions implementable during these time periods; there are other important evidence-based interventions to improve maternal and neonatal health. The interventions listed above are specifically for reducing stillbirths. Those marked with an * and in bold have proven benefit or some evidence of impact for reduction of stillbirths/perinatal mortality.)
5

WHO CAN DO WHAT? [Paper 6]
Table 2: Possible delivery strategies for interventions with some or clear evidence of impact on stillbirths
Mass media (including so-cial market-
ing strategies, health days,
etc)
Facilitated community and advo-
cacy groups
TBAs Trained CHWs
(outreach workers)
Community-based
professional midwives
Other cadres of facility-
based health workers
Medical/nursing staff in first-level
facilities
Multiple micronutrient supplementation
+ + ¸ ¸ ¸ ¸
Balanced protein-energy supplementation
+ + ¸ ¸ ¸ ¸
Anti-malarials in pregnancy + + ¸ ¸ ¸ ¸ Insecticide-treated bed nets in pregnancy
+ ¸ ¸ ¸ ¸ ¸
Heparin in pregnancy for clotting disorders and antiphospholipid syndrome
¸
Anti-helminthic treatment in pregnancy
¸ ¸ ¸ ¸
Syphilis screening and treatment in pregnancy
+ ¸ ¸
Management of intrahepatic cholestasis in pregnancy
¸
Fetal movement counting (in high-risk pregnancy)
+ + ¸ ¸ ¸
Doppler monitoring (in high-risk pregnancy)
¸
Intrapartum cardiotocography (with access to Caesarean section)
¸
Amniotic fluid volume assessment in pregnancy
¸
Emergency obstetric care packages, including Caesarean section
+ + + + ¸ ¸
Elective induction of labour in post-term pregnancies
+ + ¸
Planned Caesarean section for term breech presentation*
+ ¸
Perinatal audit ¸ ¸ ¸
¸ Provision of intervention + Promotion of intervention
* Only advised in areas with ability to perform safe Caesarean section
PANEL 2 - Key programme recommendations to reduce stillbirths [Paper 6]
1. Community demand creation strategies and training of appropriate human resources for health promotion and preventive interventions
2. Antenatal care to deliver quality interventions and to screen for high risk pregnancies3. Recognition and prompt and appropriate management of maternal infections during pregnancy, such as syphilis and
malaria4. Skilled attendance at birth and emergency obstetric care availability (including Caesarean section)
6

PRIORITIES FOR REDUCING STILLBIRTHS [Paper 1 and 6]
Global data and policy priorities
• Tracking mortality reduction: Almost all (98%) of the world’s 3.2 million stillbirths occur in low- or middle-income countries, yet stillbirths are rarely mentioned by global decision makers or UN agencies. This is a missed opportunity for large-scale MNCH programmes to track signifi cant mortality benefi t. Stillbirths should be included in mortality tracking wherever child and/or maternal outcomes are being assessed in household surveys or in health system or research evaluations.
• Intrapartum priority: Given that 1 million stillbirths occur during the time of labour and that half of the world’s births are in facilities, improved obstetric care offers an immediate opportunity to reduce these deaths and the associated 904,000 neonatal deaths due to so-called ‘birth asphyxia’ that are intrapartum-related. However, many intrapartum stillbirths occur at home or on the way to a facility, so innovative approaches are required to address delays in accessing obstetric care.
• Effective antenatal care: Around 2.2 million stillbirths occur during the last trimester but before the onset of labour. Given that over 75% of pregnant women globally access antenatal care (72% in Africa and 68% in South Asia), there are many missed opportunities for effective interventions to be provided through antenatal care. Priority conditions to address include pregnancy-induced hypertension; antepartum haemorrhage; maternal infections such as syphilis and malaria; and obstetric risk conditions such as multiple pregnancy and abnormal lie.
National data and programme priorities
• In many high-income countries, stillbirth rates have not been declining at the expected rate. Improvements are possible with increased use of confi dential enquiry data and attention not only to implement evidence-based interventions well, but also to innovate to address key challenges.
• In middle-income countries, strengthening vital registration data for stillbirths and scaling up perinatal audit will give more data for priority setting and tracking of programme effectiveness.
• In low-income countries, urgent attention should be given to how to better measure stillbirth rates in existing large-scale household surveys (for example, the use of pregnancy history instead of birth history modules) and consideration of post-survey verbal autopsy to increase data on stillbirth cause of death.
• In all country programmes for maternal and neonatal health, when scaling up, specifi c attention should be paid to including high-impact interventions to reduce stillbirths and to tracking key indicators for quality of care such as intrapartum stillbirth rate.
• Research studies for maternal and neonatal health outcomes should consider measuring and reporting stillbirth outcomes.
Given the large annual burden of at least 3.2 million stillbirths and the opportunity to reduce this burden through existing MNCH programmes, the low policy and programme priority given to stillbirths may be unparalleled compared to any other need in global health today. Is this a simple oversight and lack of coherent communication of the data and the solutions? Or do stillbirths not count?
Photo credit: Save the Children/Jenny Matthews
7

The Series – Goldenberg RL, McClure EM, Belizán JM: Commentary: reducing the world’s stillbirths, 9(Suppl 1):S1.
1 Lawn JE, Yakoob MY, Haws RA, Soomro T, Darmstadt GL, Bhutta ZA: 3.2 million stillbirths Epidemiologyand overview of the evidence review. BMC Pregnancy and Childbirth 2009, 9(Suppl 1):S2.
2 Yakoob MY, Menezes EV, Soomro T, Haws RA, Darmstadt GL, Bhutta ZA: Reducing stillbirths: behavioural and nutritional interventions before and during pregnancy. BMC Pregnancy and Childbirth 2009, 9(Suppl 1):S3.
3 Menezes EV, Yakoob MY, Soomro T, Haws RA, Darmstadt GL, Bhutta ZA: Reducing stillbirths: prevention and management of medical disorders and infections during pregnancy. BMC Pregnancy and Childbirth 2009, 9(Suppl 1):S4.
4 Haws RA, Yakoob MY, Soomro T, Menezes EV, Darmstadt GL, Bhutta ZA: Reducing stillbirths: screening and monitoring during pregnancy and labour. BMC Pregnancy and Childbirth 2009, 9(Suppl 1):S5.
5 Darmstadt GL, Yakoob MY, Haws RA, Menezes EV, Soomro T, Bhutta ZA: Reducing stillbirths: interventions during labour. BMC Pregnancy and Childbirth 2009, 9(Suppl 1):S6.
6 Bhutta ZA, Darmstadt GL, Haws RA, Yakoob MY, Lawn JE: Delivering interventions to reduce the global burden of stillbirths: improving service supply and community demand. BMC Pregnancy and Childbirth 2009, 9(Suppl 1):S7.
All the papers can be accessed free of charge at http://www.biomedcentral.com/1471-2393/9?issue=S1
Additional references7 Stanton C, Lawn JE, Rahman H, Wilczynka-Ketende K, Hill K: Stillbirth rates: delivering estimates in
190 countries. Lancet 2006, 367: I487-I494.8 Lawn J, Shibuya K, Stein C: No cry at birth: global estimates of intrapartum stillbirths and
intrapartum-related neonatal deaths. Bulletin of World Health Organization 2005, 83(6): 409-417.
AcknowledgementsEditors of the series: Zulfi qar A. Bhutta, Gary L. Darmstadt, and Joy E. LawnCore group for Executive Summary (in alphabetical order): Zulfi qar A Bhutta, Gary L Darmstadt, Rachel A Haws, Mary Kinney, Joy E Lawn, and Mohammad Yawar YakoobDesign and layout: The Miracle Book, Cape TownPrinting: C2 Digital, Cape Town
Financial support: Funding for this publication was provided by Saving Newborn Lives/Save the Children USA through a grant from the Bill and Melinda Gates Foundation.
Photo credits: Save the Children/Ahmad El-Nemr, Save the Children/Thomas L. Kelly, Save the Children/Michael Bisceglie





























