Embed Size (px)
Citation preview

R E V I E W S E R I E S ndash S T A T E O F T H E A R T M E D I C A L M A S T E R C L A S S
AcromegalyR Dineen1 PM Stewart2 and M Sherlock1
From the 1Department of Endocrinology Adelaide and Meath Hospitals Incorporating the National ChildrenrsquosHospital Tallaght Dublin and Trinity College Dublin Ireland and 2Department of Endocrinology University ofLeeds Leeds UK
Address correspondence to M Sherlock Department of Endocrinology Adelaide and Meath Hospitals Incorporating the National Childrenrsquos Hospital andTrinity College Dublin Tallaght Dublin 24 Ireland email sherlomatcdie
Summary
Acromegaly is a rare chronic progressive disease characterized by an excess secretion of growth hormone (GH) andincreased circulating insulin-like growth factor 1 (IGF-1) concentrations It is caused by a pituitary adenoma in the vast ma-jority of cases The clinical diagnosis based on symptoms related to GH excess is often delayed due to the insidious natureof the disease Consequently patients often have established systemic complications at diagnosis with increased morbidityand premature mortality Serum IGF-1 measurement is recommended as the initial screen for patients with suspected acro-megaly The gold standard diagnostic test remains the oral glucose tolerance test with concomitant GH measurementTherapy for acromegaly is targeted at decreasing GH and IGF-1 levels ameliorating patientsrsquo symptoms and decreasing anylocal compressive effects of the pituitary adenoma The therapeutic options for acromegaly include surgery medical thera-pies (such as dopamine agonists somatostatin receptor agonists and the GH receptor antagonist pegvisomant) and radio-therapy A multidisciplinary approach is recommended with often a requirement for combined treatment modalities Withdisease control associated morbidity and mortality can be reduced The recently published evidence-based guidelines bythe Endocrine society addressed important clinical issues regarding the evaluation and management of acromegaly This re-view discusses advances in our understanding of the pathophysiology of acromegaly diagnosis of various forms of the dis-ease and focuses on current treatment modalities and on future pharmacological therapies for patients with acromegaly
Background
Acromegaly is a slowly progressive disease caused by chronichypersecretion of growth hormone (GH) and excess circulatinginsulin-like growth factor-1 (IGF-1) The etiology of acromegaly isalmost invariably an underlying GH-secreting pituitary adenomaRarely it is due to a hypothalamic tumor secreting GHRH or ec-topic growth hormone releasing hormone (GHRH) secretion orvery rarely GH from an ectopic source1 Acromegaly is rare withan estimated prevalence of 36ndash60 cases per million with an an-nual incidence of 3ndash4 per million2
Pathophysiology
Pituitary tumors are monoclonal adenomas that account for10 of primary intracranial neoplasms3 GH is synthesizedand stored in somatotroph cells which account for gt50 ofpituitary hormone secreting cells4 GH production and secre-tion is regulated by hypothalamic GH-releasing hormoneghrelin and somatostatin IGF-1 inhibits GH secretion by bothdirect effect on the somatrophs and indirectly through stimu-lation of somatostatin that inhibits GH secretion GH is se-creted in sporadic pulses with minimal basal secretion
Received 19 November 2015
VC The Author 2016 Published by Oxford University Press on behalf of the Association of PhysiciansAll rights reserved For Permissions please email journalspermissionsoupcom
411
QJM An International Journal of Medicine 2017 411ndash420
doi 101093qjmedhcw004Advance Access Publication Date 12 February 2016Review
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
determined by sex age neurotransmitters exercise andstress
GH action is achieved via its interaction with a single-chaintransmembrane glycoprotein receptor (GHR) The GH moleculeinteracts with a preformed dimer of identical GHR pairs causinginternalization of the receptor to initiate signaling As a conse-quence two Janus tyrosine kinase 2 molecules undergoautophosphorylation and in turn phosphorylate the GHR cyto-plasmic domain This activates intracellular proteins involvedin signal transduction and transcription (STAT)5
The gene encoding the GHR is ubiquitously expressed par-ticularly in liver fat and muscle GH activation of the intracellu-lar molecule STAT5b induces transcription of IGF-1 SystemicIGF-1 is synthesized primarily in the liver but also in extrahep-tatic tissues including bone muscle and kidney and in the pitu-itary gland itself IGF-1 circulates in serum bound to IGF-1binding protein (IGFBP-3) or IGFBP-5 and acid-labile subunit ina 150-kD complex Less than 1 of total serum IGF-1 circulatesas a free hormone The IGF-1 cellular effects are mediated bythe IGF-1 receptor (IGF-1R) a heterotetrameric protein structur-ally similar to the insulin receptor IGF-1 acts to mediate tissuegrowth or locally synthesized IGF-1 acts in a paracrine mannerto regulate local GH target tissue growth 6
Several candidate genes that could account for the somato-troph clonal expansion have been examined in animal modelsThese include the retinoblastoma tumor suppression gene andp27 Disruption of the MENIN gene results in multiple endo-crine neoplasia type I Ras mutations have been reported to acti-vate GH secretion in experimental animal models as havemutations of a pituitary tumor-transforming gene Mutations inthe tumor suppressor gene arylhydrocarbon receptor interact-ing protein (AIP) are prevalent in young-onset GH excess pa-tients and familial isolated and young-onset pituitaryadenomas In a longitudinal international collaborative studyKorbonits et al7 identified AIP mutations in 467 of patientswith gigantism in their cohort of 216 patients Two histologicalsubtypes of GH-secreting pituitary adenoma have been identi-fied based on the pattern of cytoplasmic cytokeratin Sparselygranulate cytokeratin at histology suggest more invasive le-sions These lesions are more common in younger patients andare less response to somatostatin receptor ligand therapy8
Clinical features
First observed by Verga in 1864 acromegaly is characterized bydisproportionate skeletal tissue and organ growth At diagno-sis patients may exhibit a spectrum of clinical signs includingskeletal and acral overgrowth and soft tissue enlargement withfrontal bossing mandibular prognathism jaw malocclusionand overbite skin thickening and increased ring and shoe size(Table 1) Other features include hyperhidrosis paresthesiagoiter arthritis kyphoscoliosis headaches visual field deficitscolon polyps sleep apnea and daytime somnolence reproduct-ive disorders and cardiovascular disease9 It should be high-lighted that there is a large spectrum of clinical featuresassociated with acromegaly and patients may have a spectrumof mild to severe clinical phenotype therefore a high index ofsuspicion is required
Morbidity
Acromegaly often evades diagnosis until in its clinically obviouslater stages often resulting in a delay of 5ndash10 years after ap-proximate symptom onset10 Patients often present with
significant co-morbidities including hypertension diabetesmellitus and sleep apnea
Arterial hypertension is reported to affect up to 40 of pa-tients with acromegaly Experimental and clinical studies haveshown that both GH and IGF-1 exert direct effects on myocardialgrowth and function The key feature of acromegaly cardiomy-opathy is concentric biventricular hypertrophy Hypertrophy in-volves proliferation of the myocardial fibrous tissue whichresults in interstitial remodeling and subsequent impaired ven-tricular relaxation and diastolic dysfunction The cardiomyop-athy of acromegaly is further aggravated by hypertension andglucose abnormalities
Valvular heart disease and arrhythmias are more frequentlyobserved in patients with acromegaly with up to 40 of pa-tients suffering from conduction disorders Colao et al6 demon-strated a high prevalence of both mitral and aortic valvedysfunction in patients with active acromegaly If the disease isuncontrolled then diastolic and ultimately systolic heart failurecan develop
Impaired glucose tolerance and diabetes mellitus are fre-quently associated with acromegaly as GH excess promotesinsulin resistance in the liver and the periphery Hyperinsuli-naemia and increased gluconeogenesis are observed in patients
Table 1 Clinical features of acromegaly
Direct tumoreffects
Visual field deficit
Cranial nerve palsyHeadacheHypopituitarism
Soft tissue andskin changes
Increased skin thickness and soft tissuehyperplasia
HyperhidrosisSkin tags and acanthosis nigricans
Bone and jointfeatures
Somatic effects (Acral enlargement prognathismfrontal bossing)
ArthropathyosteoarthritisCarpal tunnel syndromeOsteopenia vertebral fracturesProximal myopathyHearing loss
Cardiovascularfeatures
Biventricular hypertrophy
Increased interventricular septum thickness (ec-centric hypertrophy)
Diastolic dysfunction at rest andor systolic dys-function on effort
Diastolic heart failureArrthymiasHypertensionEndothelial dysfunction and increased carotid IMT
Metabolicfeatures
Impaired fasting glucose
Impaired glucose toleranceDiabetes mellitusInsulin resistanceReduced total cholesterol and increased
triglyceridesIncreased nitrogen retention
Respiratoryfeatures
Upper airway obstruction
MacroglossiaSleep apnea
412 | QJM An International Journal of Medicine 2017 Vol 110 No 7
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
with acromegaly11 The exact prevalence of overt diabetes mel-litus in acromegaly is unknown but ranges from 19 to as highas 5212 The differing prevalence rates are likely due to the het-erogeneity of the case series in addition to the impact of revisedaccepted criteria for the diagnosis and classification of diabetesmellitus
Respiratory disorders can develop in patients with acromeg-aly as a result of anatomical changes affecting craniofacialbone and soft tissues as well as alterations in activity of re-spiratory muscles Sleep apnea can affect up to 60 of patientsmost often due macroglossia and anatomical narrowing of theupper airways Central sleep apnea has been observed in a mi-nority of cases13
Arthropathy affects 75 of patients with acromegaly and isthe leading cause of morbidity and functional disability forthese patients14 Pain is the most common symptom usuallyexacerbated by activity Carpal tunnel syndrome is present inup to 64 of patients at presentation15 With disease progres-sion the bone undergoes accelerated turnover and the articularcartilage thins with narrowing of joint spaces similar to fea-tures of osteoarthiritis A recent meta-analysis observed ahigher bone formation but with a greater frequency of vertebralfractures compared with controls16
In recent years particular focus has been placed on colorec-tal cancer (CRC) to a lesser extent on breast prostate and thy-roid cancer rates in patients with acromegaly The pooled oddratios are increased for benign neoplasia (248 for colonic aden-omas and 3557 for hyperplastic polyps) in addition to coloncancer (204ndash4351)17 Orme et al investigated the incidence andmortality for cancer in a cohort of 1239 patients They excludedall malignancies pre-diagnosed to the diagnosis of acromegalyand used reliable national cancer registers for cross-examin-ation The overall cancer incidence was lower in the acromegalypatients than in the normal population (79 vs 109 malignanciesrespectively) However the SIRs revealed a small increase incolon cancers in acromegaly patients (SIR 168) and the deathrate from colon cancer outnumbered that recorded in the nor-mal population (13 observed deaths vs 5 expected) The occur-rence of cancer was unrelated to either disease duration or ageat diagnosis but the standard mortality rate associated withcancer was higher with post-treatment levels of GHgt10 lgl18
More recent results from the German Acromegaly Registry for446 patients (6656 person-years from diagnosis) did not showany evidence for a higher incidence of cancer (SIR 075 95CI055ndash10) most notably CRC or breast cancer19
Mortality
It is well reported in the literature that untreated acromegaly isassociated with reduced life expectancy Analysis of the deter-minants of mortality indicate that 60 die from cardiovascu-lar disease 25 from respiratory disease and 15 frommalignancies With advances in the medical therapy surgicaltechniques and localized stereotactic radiotherapy overall mor-tality rates in acromegaly have improved Although mortality inacromegalic patients remains elevated compared with the gen-eral population in several studies the mortality increase is gen-erally less than 2-fold compared with the 2- to 3-fold mortalityrates seen in earlier series20
There is compelling evidence to support that the last avail-able follow-up GH value is the most predictive survival indexBates et al21 reported that in a cohort of 79 patients with acro-megaly the Standardised Mortality ratio (SMR) fell from 26 to20 if treatment reduced GH levels to under 10 mUl (5 lgl) Even
more significant was the fact that mortality was reduced to nor-mal if post-treatment GH levels of lt5 mUl (25 lgl) wereachieved21 In the West Midlands Acromegaly Study compari-son of crude death rates per 1000 population suggested that aGH of 2 lgl may be a more appropriate treatment target with astep-up in the death rate once GH exceeded 2 lgl22 The FinnishNationwide Survey of Mortality in Acromegaly reported similarfindings In a cohort of 334 acromegalic patients with 56 deathsexcess mortality was seen in those with post-treatment GH lev-els gt25 lgl (SMR 163 (11ndash235) Plt 0001)23
In a recent meta-analysis Holdaway et al focused on the re-lationship between biochemical measurements and mortalityduring follow-up after treatment for acromegaly24 Mortalitywas close to the expected level when last available GH wasunder 25 lgl (SMR 11 95 CI 09ndash14) but was significantlyelevated in those with last available GH above 25 lgl (SMR 1995 CI 15ndash24)
Therefore the biochemical aim of treatment in acromegalyshould be reduction of GH values to lt25 lgl and possibly evenlower to lt1 lgl although care must be taken that this is not atthe expense of inducing GH deficiency and hypopituitarismwhich in itself is associated with an adverse outcome20
The introduction of GH antagonists as medical treatment foracromegaly necessitates the use of IGF-I in the biochemicalmonitoring of patients treated with these agents Holdaway et alfound that those with normal IGF-1 had mortality close to theexpected values for the general population (SMR 11 95 CI 09ndash14) whereas the SMR for those with elevated IGF-1 at last fol-low-up remained significantly increased (SMR 25 95 CI 16ndash40) However it should be noted that two of the largest studiesin the meta-analysis comprising a total of 151 deaths in 753 pa-tients have failed to demonstrate any relationship betweenpost-treatment IGF-1 levels and mortality(Relative Risk 12 95CI 071ndash202 Pfrac14 05 and RR 046 95 CI 017ndash126 Pfrac14 013) sug-gesting that last available serum IGF-I may not be as reliable amarker of mortality in acromegaly as last available GH
There are also methodological problems with using the lastavailable GHIGF-I in the analysis for mortality because thisvalue is inherently biased and does not take into account priorGHIGF-1 levels Many studies were also performed using olderassays that may not be used in clinical practice today howeverit may take many years to get meaningful data on survival usingnewer more sensitive assays and these older studies have to beinterpreted with this in mind
In the West Midlands study compared with the generalpopulation the use of external radiotherapy was associatedwith increased mortality with an SMR of 158 (95 CI 122ndash204Pfrac14 0005) and when assessed on internal analysis within theacromegaly cohort resulted in an RR of 167 (95 CI 11ndash256Pfrac14 002) In the Finnish survey mortality was also increased inpatients who had been treated with radiotherapy [SMR 169(95 CI 105ndash 258) Plt 0001] In the Spanish acromegaly regis-try patients who died had a twice greater probability of havingbeen treated with radiotherapy than those who had survived(hazard ratio 229 95 CI 103ndash508 Pfrac14 0026)
Although hypopituitarism is associated with increased mor-tality first identified by Rosen and Bengtsson25 there is littledata on the role of hypopituitarism in patients with acromegalyIn the West Midlands study there was a trend (Pfrac14 007) towardreduced survival in patients with acromegaly who had a greaternumber of deficient hypothalamo-pituitary axes compared withthose without evidence of hypopituitarism Sherlock et alshowed that neither TSH deficiency nor gonadotropin defi-ciency was associated with increased mortality in acromegaly
R Dineen et al | 413
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
on internal analysis (gonadotropin deficiency was associatedwith increased SMR compared with the general population)however adrenocorticotrophic hormone (ACTH) deficiency wasassociated with increased mortality [RR 17 (95 CI 12ndash25)Pfrac14 0004] The cause of death was predominantly cardiovascu-lar and higher doses of hydrocortisone therapy were associatedwith increased mortality20
Other variables found to influence outcome included hyper-tension duration of the disorder before treatment and ageHypertension and glucose intolerance are important contribu-tory factors to the vascular morbidity associated with acromeg-aly However there are few published reports on their impacton mortality in acromegaly and how this correlates with GHand IGF-I levels Hypertension is considered one of the mostrelevant negative prognostic factors for mortality inacromegaly
Diagnosis
The diagnosis of acromegaly is based upon a combination ofclinical examination and biochemical demonstration of dysre-gulated autonomous GH secretion as well as elevated IGF-1 lev-els Serum GH concentrations are typically elevated but levelsmay fluctuate widely Measuring serum IGF-1 in a patient withclinically suspected acromegaly should be the initial test26 It isalso recommended to test patients without the typical clinicalappearance but who have associated comorbidities sleepapnea type 2 diabetes disabling arthritis carpal tunnel syn-drome hyperhidrosis and hypertension A normal IGF-1 level(using age- and sex-matched reference ranges) effectively ex-cludes the diagnosis of acromegaly False positives may occur inpregnancy patients taking estrogen therapy and late-stage ado-lescence Multiple factors can make the biochemical interpret-ation of IGF-1 level challenging including the presence ofcertain pathological conditions such as hepatic and renal fail-ure malnutrition hypothyroidism and uncontrolledhyperglycemia
Failure of normal suppression of serum GH following astandard 75 g-oral glucose load remains the gold-standard diag-nostic test and should be used to confirm the diagnosis in allcases with high or equivocal IGF-1 or in the presence of condi-tions interfering with the measurement where clinical suspi-cion is high27
The use of higher sensitivity immunofluorometric chemilu-minescent and immunoradiometric assays has been associatedwith significantly lower nadir GH during oral glucose tolerancetest (OGTT) in healthy controls than was previously thought(ranging from 0029ndash025 mgl) with a gender difference notedin some studies 27
As ultrasensitive immunoassays are not uniformly availableworldwide current guidelines suggest a cutoff for nadir GH afterOGTTlt 1 lgl acceptable for exclusion of the diagnosis26 Itshould be highlighted that this could result in inaccurate exclu-sion of mild active disease A further challenge in diagnosis isthe presence of discordant serum GH and IGF-1 levels ElevatedIGF-1 with normal GH may reflect early disease and should war-rant further investigation (including imaging) to clarify thediagnosis28
Current guidelines recommend contrast-enhanced pituitaryMRI as the first line imaging modality after biochemical con-firmation of acromegaly If MRI is contraindicated or unavail-able then pituitary computed tomography should be performedAt diagnosis macroadenomas are detected in 73 of patients2
Visual field testing is recommended in all patients with con-firmed pituitary tumors As onset is often insidious patients maynot be aware of any alteration in their vision and a baseline as-sessment facilitates accurate interpretation of further testing if adeterioration is reported by the patient or in response to therapy
Assessment of the integrity of the other pituitary hormonesby the combination of basal and appropriate dynamic testing isrecommended Hyperprolactinemia from tumor co-secretionoccurs in up to a third of patients and can contribute to hypo-gonadism but may also occur a result of lsquostalk effectrsquo due totumor compression of the pituitary stalk interrupting the deliv-ery of inhibitory dopamine to the pituitary29 Evaluating all pa-tients with acromegaly for associated co-morbidities isrecommended at diagnosis (Table 2) in addition to longitudinalmonitoring during follow-up26
Treatment
Treatment goals in acromegaly include symptom relief tumorcontrol with maintenance of pituitary function biochemicalnormalization of GHIGF-1 and reversal of the excess morbidityand mortality associated with the disorder Current modalitiesof treatment available include surgery medical therapy andradiotherapy Treatment is complex and frequently more thanone modality is required to achieve treatment goals The deci-sion to treat and the therapeutic intervention used is based on anumber of factors which need to be weighed and tailored care-fully for each patient in a multidisciplinary setting
The definition of biochemical remission is difficult due tovariability in the assay and reference ranges used It is crucialthat the same GH and IGF-1 assay is maintained in the same pa-tient throughout their management While it remains contro-versial the current recommended biochemical target is arandom GHlt 1 lgl26 The decline in IGF-1 is more delayed com-pared with GH likely due to differential half-life of IGF-bindingproteins IGF-1 levels measured at 12 weeks after surgery are avalid reflection of surgical remission If the IGF-1 level hasdeclined but is still not normal measurement of a repeat IGF-1level is warranted due to variability in the IGF-1 assay
A normal IGF-1 value and undetectable GH value are suffi-cient for indicating surgical remission However if the GH is de-tectable (ie gt04 lgL) measurement of GH after a glucose loadmay yield important information The mean value of severalsamples taken a few hours apart throughout the day can also beused (GH day curve (GHDC)) as it is significantly correlated withthe GH nadir during OGTT and with the IGF-1 level30 While theideal endocrine outcome of any therapy in acromegaly is a nor-mal IGF-1 value and undetectable GH value levels that are asso-ciated with a normalization of mortality (as discussed in thesection above relating to mortality) are acceptable
Surgery
Transphenoidal surgery by an experienced pituitary surgeon isthe initial treatment of choice recommended for the majority ofpatients26 Ninety percent of patients who undergo pituitary sur-gery are treated using the transphenoidal approach craniotomy israrely performed The development of endoscopic and microsurgi-cal transphenoidal surgery offers further advantages over the con-ventional techniques including the possibility of superior tumorclearance in previously difficult to access areas less surgical mor-bidity fewer complications and reduced postoperative pain31
The main postoperative complaints relate to the transphe-noidal approach including nasal congestion sinusitis and
414 | QJM An International Journal of Medicine 2017 Vol 110 No 7
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
epistaxis More serious complications include hemorrhage CSFleakage and risk of meningitis stroke visual impairment vas-cular injury transient diabetes insipidus (DI) (typically occur-ring as a result of intraoperative manipulation of the pituitarystalk) and hypopituitarism32 Despite significant co-morbiditiesin patients with acromegaly surgical mortality rates of lt05can be anticipated33
Several factors are associated with reduced surgical successrates including large tumor size extrasellar extension andhigher preoperative GH levels34 Recurrence rates peak in years1ndash5 postoperatively with reported recurrence rates of up to 8with recurrence rates being lower in microadenomas comparedwith macroadenomas35 A normal IGF value and undetectableGH value are sufficient for indicating surgical remission
The Acromegaly group consensus guidelines suggest that ina patient with persistent disease after surgery repeat surgerymay be an option if the tumor is accessible26 The decision toinitiate somatostatin therapy prior surgery remains controver-sial In a prospective study of 30 patients with newly diagnosedacromegaly reductions in GH and IGF-1 concentrations andtumor volume were observed following 24 weeks of preopera-tive lanreotide autogel therapy36 Further studies do not reportany difference in the long-term results37 Due to the lack ofrandomized controlled studies the Acromegaly group consen-sus recommend against the routine use of preoperative somato-statin therapy In certain circumstances particularly forpatients with severe soft tissue growth complicating anestheticrisk or with significant comorbidities that may be improved bypreoperative therapy pretreatment with somatostatin receptorligands (SRL) may be considered38
Surgical debulking may be considered in patients with lowpredictive surgical cure rate at diagnosis to improve the chanceof achieving target GHIGF-1 levels with subsequent medicaltherapy Pretreatment disease burden is inversely correlatedto somatostatin analogue responsiveness39 In addition tobiochemical testing of remission as outlined above a contrast-enhanced MRI is recommended at least 12 weeks postopera-tively to visualize residual tumor This provides a baseline forfuture surveillance Formal visual field testing should also beperformed for patients with pre-operative visual deficits
Successful surgery by an experience neurosurgeon in a spe-cialized pituitary center can result in immediate biochemical
remission elimination of direct mass effects in addition to pro-viding tissue for immunohistochemical analysis Hence surgeryremains the primary therapeutic intervention in most patientswith acromegaly26
Medical treatment
Medical therapy has an important role as an adjunctive treat-ment option for persistent disease following non-curative sur-gery and also as first line therapy where surgery is not a feasibletherapeutic option Consensus guidelines outline the recom-mended role of medical therapy in the treatment of patientswith acromegaly There are a number of options for medicaltherapy in acromegaly including somatostatin receptor ligandsGH receptor antagonists and dopamine agonists
Somatostatin receptor ligands
Somatostatin is distributed throughout the nervous system andexerts neural control over many physiological functions includ-ing the inhibition of GH release It exists in two biologically ac-tive molecular forms somatostatin-14 and somatostatin -28with a short half-life of 2-3 min Its action is mediated throughG-protein coupled cell-surface receptors identified in a varietyof tissues including the pituitary Both bioactive forms havehigh binding affinity toward all five identified receptor sub-types SSR1-SSR540 GH-secreting pituitary adenomas expresspredominantly SSR2 and SSR5 First generation somatostatinanalogs octreotide and lanreotide show high affinity binding toSSR2 and to a lesser extent to SSR541
Currently three long-acting SRL formulations are availableoctreotide LAR Lanreotide depotautogel and pasireotide Rapidacting subcutaneous octreotide is also available and is adminis-tered two-three times daily The long-acting octreotide LAR isadministered intramuscularly every 4ndash6 weeks The approvedstarting octreotide LAR dose is 20 mg monthly with dose titra-tion every 3ndash6 months to a maximum dose of 40 mg monthlyLanreotide is available in a microsphere formulation (depot) in-jected intramuscularly every 7ndash14 days and an aqueous solution(Autogel) administered by deep subcutaneous injection every 4ndash6 weeks For lanreotide autogeldepot the approved starting
Table 2 Assessment of acromegaly complications at diagnosis and during long-term monitoring
At diagnosis During long-term follow-up
BP measurement Every 6 months or when change of treatment (if hypertensive)Echocardiography AnnuallyECG AnnuallyEpworth scale or sleep study AnnuallyECHO Doppler of peripheral arterial and venous
systemAnnually particularly in gigantism
OGTT Fasting blood glucose every 6 months (particularly in uncontrolled disease andduring SRL therapy) HbA1c every 6 months if diabetes present
Total testosterone SHBG and prolactin (males) Annually (free testosterone when doubts in interpretation of total testosterone)LH FSH17b-estradiol and prolactin (females) AnnuallyAcroQol AnnuallyDEXA Every 2 years if patient with osteopeniaosteoporosisThoracic and lumbar spine Xray Every 2ndash3 years if osteoporosis risk factors kyphosis or symptomsColonoscopy Every 10 years (more frequently if IGF-1 remains persistently elevated or if abnormal
colonoscopy or family history of chronic cancer)Genetic screening for markers of familial acromeg-
aly (if suspicion)
R Dineen et al | 415
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
dose is 90 mg monthly with a maximum dose up to 120 mgmonthly26
A large body of evidence supports the efficacy of long -actingSRL therapy In a critical analysis of the largest studies octreo-tide LAR reduced GH tolt25 lgl and normalized the IGF-1 levelsin 66 and 63 respectively42 Similar targets were achievedwith lanreotide-SR in 52 and 47 of cases respectively An ear-lier meta-analysis by Freda et al43 reported the overall chance ofIGF-1 normalization was 67 with octreotide and 47 with lan-reotide SR The higher efficacy reported with octreotide may beaccounted by pre-selection of responsive cases (patients whoshowed response to short acting octreotide only being recruitedto studies) inclusion of both primary and secondary therapycases and small case series An inherent challenge to meta-analyses in such a complex condition is the lack of standardiza-tion of GH and IGF-1 assays making comparison of absolutevalues between studies impossible
Smaller tumors lower baseline GH and IGF-1 levels44 highSSR2 and SSR5 expression45 and those previously treated withsurgery are associated with a better response to SRL treatmentRoutine performance of somatostatin receptor scintigraphy oran acute GH response to a subcutaneous octreotide injection asa determinant of SRL response are not recommended26
Somatostatin receptor ligands also have proven efficacy intumor volume reduction This has been extensively reviewedrecently by Colao et al46 Tumor reduction may be mediated bydirect anti-proliferative effects via activation of somatostatinreceptors or indirectly through angiogenesis inhibitionSathyapalan et al47 showed a significant reduction in the func-tional vascularity of pituitary tumors in a small study of five pa-tients after 24 weeks of octreotide therapy
Published meta-analysis revealed that octreotide LAR andlanreotide formulation induce tumor shrinkage in 660 and328 of cases respectively4849 Tumor reduction is progressivewith prolonged treatment and decreased IGF-1 levels may beits best predictor followed by age and degree of GH decrease
A recent detailed review of published studies evaluatingsomatostatin analogues as first line therapy showed that 6-24months of octreotide LAR therapy achievedgt20-30 tumor vol-ume reduction in 73-85 of patients Unlike surgery primarymedical therapy cannot cure acromegaly Based on a recentmeta-analysis of available studies primary SRL therapy is asso-ciated with a lower remission rates compared to initial surgery(45 vs 67)49 However the accuracy of these remission ratesis questionable given the non-comparable nature and the het-erogeneity of studies included Primary SRL therapy can beoffered before surgery in patients with contraindications incases with unresectable tumor or with severe comorbidities26
During SRL treatment the most frequent side effects includeabdominal discomfort flatulence cramps and diarrheaGallbladder sludge or gallstones occur in 25 of subjects butare usually asymptomatic SRL treatment was initially thoughtto aggravate the increased risk of glucose intolerance in thesepatients but the overall effect on glucose metabolism is not clin-ically significant50
Pasireotide is a multireceptor-targeted somatostatin recep-tor ligand which has higher functional activity than octreotideon SSR subtypes except type 4 but in particular SSR551 In alarge phase III randomized trial in patients with acromegalywho were naive to medical therapy pasireotide LAR and octreo-tide LAR have a similar effect of tumor reduction despite thefact that pasireotide was superior to octreotide in providing bio-chemical control After 12 months of treatment 81 of pasireo-tide patients had20 reduction in tumor volume compared
with 77 of octreotide LAR patients52 Pasireotide has similarrates of gastrointestinal side effects to other SRLs however therates of hyperglycemia are significantly higher (occurring in 31ndash57 of patients)
Pegvisomant
Pegvisomant is a pegylated recombinant analog of human GHincorporating nine amino acid mutations Pegylation extendsthe half-life by reducing renal clearance53 The mutations resultin increased affinity to the GH receptor in addition to blockingthe second binding site on the receptor preventing GHR dimer-ization and signal transduction GH hypersecretion persists asit does not target the GH secreting tumor at the level of the pitu-itary hence GH measurements cannot be used to monitor dis-ease activity and IGF-1 becomes the sole marker to monitorbiochemical response during therapy
Pegvisomant has been shown to be highly effective in pro-viding biochemical control of acromegaly in multiple studies Ina 12-week double-blind placebo controlled study Trainer et al54
randomly assigned patients to receive placebo 10 15 or 20 mgof pegvisomant Normalization of IGF-1 (using age and sex-matched reference ranges) was achieved in 10 54 81 and89 respectively Symptom control was also observed The effi-cacy of pegvisomant over a longer period was subsequentlystudied Van der Lely et al55 reported 97 of patients achievingnormal IGF-1 levels in patients receiving therapy for 12 monthsor more (Figure 1) Dose reduction was required in 1190 pa-tients as IGF-1 levels dropped below normal reference range forage and sex
As mentioned above pegvisomant does not exert a centraleffect on pituitary GH secretion hence fears exist over the pos-sibility of increased tumor growth The German PegvisomantObservational Study is a multicenter surveillance study com-menced in 2004 to assess the efficacy and safety of pegvisomanttherapy in patients with acromegaly56 Neuroradiological moni-toring of tumor extension is performed with MRI imagingBuchfelder et al studied 3 years of follow-up data of 307 pa-tients Tumor progression was reported in between 2 and3 ofpatients treated an increase not outside the expected rate inpatients not treated with pegvisomant
Pegvisomant is administered as daily subcutaneous injec-tion It is generally well tolerated with adverse effects reportedinlt10 of patients These may include injection site reactionswith reversible lipohypertrophy and deranged liver functiontests (attributable to the polyethylene glycol pegylated vehicle)
The predominant limiting factor for use of this agent in clin-ical practice remains its considerable cost It is most often usedas a second line agent in cases resistant or intolerant to SRLtherapy or in combination with SRLrsquos in partially resistantcases It is also a potential treatment option in acromegaly pa-tients with difficult to control diabetes mellitus due to its favor-able effect on glycemic control
Dopamine agonists
Dopamine agonists bind to the D2 dopamine receptors in the pi-tuitary gland and suppress prolactin and GH secretion The useof bromocriptine a first-generation dopamine agonist is lim-ited by its side effect profile including GI symptoms lethargyand orthostatic hypotension It also compares poorly with som-atostatin receptor ligands in terms of efficacy with normaliza-tion of GHIGF-1 reported in only 10 of patients57
416 | QJM An International Journal of Medicine 2017 Vol 110 No 7
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
Cabergoline an ergot derivative dopamine agonist has beenused for decades in the treatment of hyperprolactinaemia andParkinsonrsquos disease Cabergoline is better tolerated and more ef-fective than bromocriptine however its use was superseded bythe development of SRL therapy showing higher efficacy rates
Clinical trials of cabergoline in acromegaly are small non-randomized and report variable results In a recent systematicreview of 10 trials with a total of 150 acromegaly patients con-trol of acromegaly was achieved in 34 of patients who receivedcabergoline therapy alone and 52 when added to SRL therapyin patients with suboptimal control58 Consequently currentguidelines recommend the use of cabergoline in patients withinadequate response to other medical treatment with highestbenefit expected in cases with modest persistent hormonal ele-vations26 Conflicting data exists as to whether the co-secretionof prolactin is predictive of response to dopamine agonist ther-apy Some studies conclude that tumors that co-secrete prolac-tin and GH have a greater response to dopamine agonisttherapy than those than solely secrete GH whereas othersshow no effect There remains little data available regardingtumor shrinkage in patients with acromegaly who are receivingdopamine agonist therapy59 Jaffe et al57 reported combined re-sults from a number of studies which revealed that 29 of pa-tients had some tumor shrinkage on dopamine agonist therapyand the majority of patients who had tumor shrinkage werealso hyperprolactinemic It is difficult to interpret these findinggiven the small number and heterogeneous characteristics ofthe patients included
The most frequent adverse effects of dopamine agonist ther-apy are nausea constipation headache mood disturbancenasal stuffiness and dizziness Cardiac valve abnormalitieswere described with high doses of cabergoline used inParkinsonrsquos disease but not with current recommended dosageused for patients with acromegaly60
DopastatinBIM-23A760 is a chimeric molecule hasbeen shown in vitro to have high affinity for both somatosta-tin receptor subtypes- 2 and 5 in addition to dopamine 2 recep-tor61 With increasing knowledge of the importance of SSR5 inregulation of GH in GH-secreting adenomas dopastatin isundergoing further development in clinical studies to deter-mine if there is a role for these compounds in the treatment ofacromegaly
Radiotherapy
Radiation therapy is used as adjuvant treatment in the settingof persistent disease despite surgery andor medical treatmentor if medical therapy is unavailable unsuccessful or not toler-ated Radiotherapy has been shown to be effective in loweringserum GH levels36 but conflicting results have been reported re-garding the normalization of IGF-1 levels62 Furthermore thedelay in therapeutic benefit and the high risk of developinghypopituitarism serve as arguments against the more routineuse of radiotherapy
Conventional radiotherapy has been used for gt30 years inthe adjunctive treatment of pituitary adenomas It is generallydelivered in fractionated doses 4ndash5 times per week so as to re-duce daily-fractionated dose The risk of adverse effects beingproportional to maximal dose per day63 Early studies of con-ventional radiotherapy reported high efficacy rate of 80ndash100however remission was defined as a GH level below 5-10 ngmlMore recent studies using revised biochemical remission tar-gets report a mean remission rate between 50 and 60 Jenkinset al64 assessed the effects of conventional pituitary irradiationin 884 patients of the UK National Acromegaly Register MeanGH levels declined from 135 to 53 ngml at 2 years after surgeryto 2 ngml by 10 years and a further decline to 11 ngml at 20years (Figure 2) Furthermore they observed a parallel fall in IGF-
Figure 1 Baseline and lowest values of individual serum insulin-like growth factor-1 concentrations achieved in 90 patients treated for 12 months or more with daily
pegvisomant (daggerPlt005 vs baseline DaggerPlt001 vs baseline) The shaded area represents the age-adjusted normal range for insulin-like growth factor-155
R Dineen et al | 417
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
1 levels with 63 of patients having a normal level by 10years64
Stereotactic radiotherapy offers improvement in immobil-ization imaging and treatment delivery from conventionaltechniques It can be delivered as a single fraction radiosurgeryusing a Gamma knife (a source of cobalt) or a linear acceleratoror a stereotactic conformal radiotherapy delivered as fractio-nated treatment using a linear accelerator There is no clear ad-vantage for either of the radiosurgical techniques in terms ofsparing normal tissue receiving high doses of radiation65 A crit-ical analysis of the literature reported variable rates of both bio-chemical and tumor response 17ndash82 and 37ndash100respectively66 The authors attributed the wide variability to theuse of different treatment schedules and definitions ofremission
Hypopituitarism is less frequent with radiosurgery than con-ventional radiotherapy At least 50 of patient treated with con-ventional radiotherapy will have acquired new anteriorpituitary hormonal deficits at 10 years67 In cohorts treatedsolely with stereotactic techniques rates of hypopituitarismvary between 0 and 2068 However it is likely that the candi-dates for stereotactic radiotherapy had smaller remnants of dis-ease and therefore less normal tissue irradiated
Annual hormonal testing is required due to the risk of latehypopituitarism26 Other complications following radiotherapyinclude the risk of second brain tumors stroke and rarely opticneuropathy cranial nerve deficits and radionecrosis a rare ad-verse effect of gamma knife radiotherapy69ndash71
Patients treated with conventional radiotherapy have beenreported to have increased mortality predominantly due tostroke independent of GHIGF-I levels and hypopituitarism20
Current guidelines recommend the use of stereotactic radio-therapy over conventional radiation therapy unless significantresidual tumor burden or the lesion is too close to the opticchiasm26
Conclusion
Prolonged exposure to elevated endogenous levels of GH andIGF-I results in a multisystem disease characterized by somaticovergrowth multiple co-morbidities and premature mortalityEarly detection prevents the development of irreversible com-plications of the disease including cardiomyopathy respiratory
dysfunction and arthropathy Despite the imprecision of assaysfor GH and IGF-I it is clear from epidemiologic studies that tightbiochemical control is essential to reduce morbidity controlsymptoms and improve mortality rates
Optimal implementation of current guidelines in routine clin-ical practice and maximal use of the medical treatment could im-prove the long-term control of patients with significant benefitsfor morbidity and mortality Another important aspect in thetreatment of patients with acromegaly is also the appropriate tar-geted treatment of co-morbidities associated with acromegaly
Achievement of the criteria for cure during or after therapyis determined by assessing biochemical control targeting con-trolled levels of GH and normalization of IGF-I levels monitor-ing tumor size assessing residual pituitary function andmonitoring co-morbidities
New therapeutic molecules currently in trials will hopefullyoffer further benefit to those patients resistant to current thera-peutic modes for this chronic progressive disorder
Conflict of interest None declared
References1 Melmed S Braunstein GD Horvath E Ezrin C Kovacs K
Pathophysiology of acromegaly Endocr Rev 1983 4271ndash902 Mestron A Webb SM Astorga R Benito P Catala M
Gaztambide S et al Epidemiology clinical characteristicsoutcome morbidity and mortality in acromegaly based onthe Spanish Acromegaly Registry (Registro Espanol deAcromegalia REA) Eur J Endocrinol 2004 151439ndash46
3 Jagannathan J Dumont AS Prevedello DM Oskouian RJLopes B Jane JA Jr and Laws ER Jr Genetics of pituitary aden-omas current theories and future implications NeurosurgFocus 2005 19E4
4 Zhu X Lin CR Prefontaine CG Tollkuhn J Rosenfeld MGGenetic control of pituitary developement and hypopituitar-ism Curr Opin Genet Dev 2005 15332ndash40
5 Melmed S Acromegaly pathogenesis and treatment J ClinInvest 2009 1193189ndash202
6 Colao A Ferone D Marzullo P Lombardi G Systemic compli-cations of acromegaly epidemiology pathogenesis andmanagement Endocr Rev 2004 25102ndash52
7 Korbonits M Gadelha MR Roncaroli F Grossman AB Ellard SEvanson J et al Landscape of familial isolated and young-onset pituitary adenomas prospective diagnosis in AIP mu-tation carriers J Clin Endocrinol Metab 2015 100E1242ndash54
8 Larkin S Reddy R Karavitaki N Cudlip S Wass J Ansorge OGranulation pattern but not GSP or GHR mutation is associ-ated with clinical characteristics in somatostatin-naive pa-tients with somatotroph adenomas Eur J Endocrinol 2013168491ndash9
9 Molitch ME Clinical manifestations of acromegaly EndocrinolMetab Clin North Am 1992 21597ndash614
10Reid TJ Post KD Bruce JN Nabi KM Reyes-Vidal CM et alFeatures at diagnosis of 324 patients with acromegaly didnot change from 1981 to 2006 acromegaly remains under-recognized and under-diagnosed Clin Endocrinol 201072203ndash8
11Moslashller N Joslashrgensen JO Abildgard N Orskov L Schmitz OChristiansen JS Effects of growth hormone on glucose me-tabolism Horm Res 1991 36 (Suppl 1)32ndash5
12Dreval AV Trigolosova IV Misnikova IV Kovalyova YATishenina RS Barsukov IA et al Prevalence of diabetes melli-tus in patients with acromegaly Endocr Connect 2014 393ndash8
Figure 2 Percentage of all patients achieving a serum GH level lt25 ngml (bars)
and the mean GH level (line) in the years after pituitary irradiation64
418 | QJM An International Journal of Medicine 2017 Vol 110 No 7
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
13Roemmler J Gutt B Fischer R Vay S Wiesmeth ABidlingmaier M et al Elevated incidence of sleep apnoea inacromegaly-correlation to disease activity Sleep Breath 2012161247ndash53
14Killinger Z Payer J Lazurova I Imrich R Homerova Z KuzmaM et al Arthropathy in acromegaly Rheum Dis Clin North Am2010 36713ndash20
15Kameyama S Tanaka R Hasegawa A Tamura T Kuroki MSubclinical carpal tunnel syndrome in acromegaly NeurolMed Chir 1993 33547ndash51
16Mazziotti G Biagioli E Maffezzoni F Spinello M Serra VMaroldi R et al Bone turnover bone mineral density and frac-ture risk in acromegaly a meta-analysis J Clin EndocrinolMetab 2015 100384ndash94
17Renehan AG OrsquoConnell J OrsquoHalloran D Shanahan F PottenCS OrsquoDwyer ST et al Acromegaly and colorectal cancer acomprehensive review of epidemiology biological mechan-isms and clinical implications Horm Metab Res 200335712ndash25
18Orme S McNally RJ Cartwright RA Belchetz PE Mortality andcancer incidence in acromegaly a restrospective cohortstudy J Clin Endocrinol Metab 1998 832730ndash4
19Petroff D Teuroonjes A Grussendorf M Droste M Dimopoulou CStalla G et al The Incidence of cancer among acromegaly pa-tients results from the German Acromegaly Registry J ClinEndocrinol Metab 2015 1003894ndash902
20Sherlock M Ayuk J Tomlinson JW Toogood AA Aragon-Alonso A Sheppard MC et al Mortality in patients with pitu-itary disease Endocr Rev 2010 31301ndash42
21Bates AS Vanrsquot H Jones JM Clayton RN An audit of outcomeof treatment in acromegaly Q J Med 1993 86293ndash9
22Ayuk J Clayton RN Holder G Sheppard MC Stewart PMBates AS Growth hormone and pituitary radiotherapy butnot serum insulin-like growth factor-I concentrations pre-dict excess mortality in patients with acromegaly J ClinEndocrinol Metab 2004 891613ndash7
23Kauppinen-Meuroakelin R Sane T Reunanen A Veuroalimeuroaki MJNiskanen L Markkanen H et al A nationwide survey of mor-tality in acromegaly J Clin Endocrinol Metab 2005 904081ndash6
24Holdaway IM Bolland MJ Gamble GD A meta-analysis of theeffect of lowering serum levels of GH and IGF-I on mortalityin acromegaly Eur J Endocrinol 2008 15989ndash95
25Rosen T Bengtsson BA Premature mortality due to cardio-vascular disease in hypopituitarism Lancet 1990 336285ndash8
26Katznelson L Laws ER Jr Melmed S Molitch ME Murad MHUtz A et al Acromegaly an endocrine society clinical practiceguideline J Clin Endocrinol Metab 2014 993933ndash51
27Freda PU Post KD Powell JS Wardlaw SL Evaluation of dis-ease status with sensitive measures of growth hormone se-cretion in 60 postoperative patients with acromegaly J ClinEndocrinol Metab 1998 833808ndash16
28Dimaraki EV Jaffe CA DeMott-Friberg R Chandler WFBarkan AL Acromegaly with apparently normal GH secretionimplications for diagnosis and follow-up J Clin EndocrinolMetab 2002 873537ndash42
29Losa M Von Werder K Pathophysiology and clinical aspectsof the ectopic GH-releasing hormone syndrome ClinEndocrinol 1997 47123ndash35
30Dobrashian RD OrsquoHalloran DJ Hunt A Beardwell CG ShaletSM Relationships between insulin-like growth factor-1 levelsand growth hormone concentrations during diurnal profilesand following oral glucose in acromegaly Clin Endocrinol 199338589ndash93
31Frank G Pasquini E Farneti G Mazzatenta D Sciarretta VGrasso V et al The endoscopic versus the traditional ap-proach in pituitary surgery Neuroendocrinology 2006 83240ndash8
32Marquez Y Tuchman A Zada G Surgery and radiosurgery foracromegaly a review of indications operative techniquesoutcomes and complications Int J Endocrinol 2012 2012386ndash401
33Laws ER Vance ML Thapar K Pituitary surgery for the man-agement of acromegaly Horm Res 2000 5371ndash5
34Salaun C Foubert L Vialatou M Kujas M Turpin G Prognosticfactors of surgical cure of growth hormone secreting pituitary aden-omas Ann Medecine Interne 1999 150195ndash8
35Kreutzer J Vance ML Lopes MB Laws ER Jr Surgical manage-ment of GH-secreting pituitary adenomas an outcome studyusing modern remission criteria J Clin Endocrinol Metab 2001864072ndash7
36Annamalai AK Webb A Kandasamy N Elkhawad M Moir SKhan F et al A comprehensive study of clinical biochemicalradiological vascular cardiac and sleep parameters in anunselected cohort of patients with acromegaly undergoingpresurgical somatostatin receptor ligand therapy J ClinEndocrinol Metab 2013 981040ndash50
37Shen M Shou X Wang Y Zhang Z Wu J Mao Y et al Effect ofpresurgical long-acting octreotide treatment in acromegalypatients with invasive pituitary macroadenomas a prospect-ive randomized study Endocr J 2010 571035ndash44
38Friedel ME Johnston D Singhal S Al Khalili K Farrell CJEvans JJ et al Airway management and perioperative con-cerns in acromegaly patients undergoing endoscopic trans-sphenoidal surgery for pituitary tumors Otolaryngol HeadNeck Surg 2013 149840ndash4
39Bhayana S Booth G Asa SL Kovacs Ezzat S The implicationof somatotroph adenoma phenotype to somatostatin analogresponsiveness in acromegaly J Clin Endocrinol Metab 2005906290ndash5
40Reisine T Bell GI Molecular biology of somatostatin recep-tors Endocr Rev 1995 16427ndash42
41Zatelli MC Piccin D Tagliati F et al Dopamine receptor sub-type 2 and somatostatin receptor subtype 5 expression influ-ences somatostatin analog effects on human somatotrophpituitary adenomas in vitro J Mol Endocrinol 2005 35333ndash41
42Murray RD Melmed S A critical analysis of clinically avail-able somatostatin analog formulations for therapy of acro-megaly J Clin Endocrinol Metab 2008 932957ndash68
43Freda PU Katznelson L Van der Lely A Reyes CM Zhao SRabinowitz D Long-acting somatostatin analog therapy ofacromegaly a meta-analysis J Clin Endocrinol Metab 2005904465ndash74
44Howlett TA Willis D Walker G Wass JA Trainer PJ Control ofgrowth hormone and IGF1 in patients with acromegaly in theUK responses to medical treatment with somatostatin ana-logues and dopamine agonists Clin Endocrinol 201379689ndash99
45Espinosa de los Monteros AL Carrasco C Albarran AAGadelha M Abreu A Mercado M The role of primary pharma-cological therapy in acromegaly Pituitary 2014 17 (Suppl1)S4ndashS10
46Colao AM Auriemma RS Pivonello R The effects of somato-statin analogue therapy on pituitary tumor volume in pa-tients with acromegaly Pituitary 2016 19210ndash21
47Sathyapalan T Lowry M Turnbull LW Rowland-Hill C AtkinSL Mechanism of action of octreotide in acromegalic tu-mours in vivo using dynamic contrast-enhanced magneticresonance imaging Pituitary 2007 10233ndash6
R Dineen et al | 419
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
48Giustina A Mazziotti G Torri V Spinello M Floriani IMelmed S Meta-analysis on the effects of octreotide ontumor mass in acromegaly PLoS One 2012 7e36411
49Abu Dabrh AM Mohammed K Asi N Farah WH Wang ZFarah MH et al Surgical interventions and medical treat-ments in treatment-naive patients with acromegaly system-atic review and meta-analysis J Clin Endocrinol Metab 2014994003ndash14
50Colao A Bronstein M Freda P Gu F Shen C-C Gadelha Met al Pasireotide versus octreotide in acromegaly a head-to-head superiority study J Clin Endocrinol Metab 2014 99791ndash9
51Schmid HA Schoeffter P Functional activity of the multili-gand analog SOM230 at human recombinant somatostatinreceptor subtypes supports its usefulness in neuroendocrinetumors Neuroendocrinology 2004 80 (Suppl 1)47ndash50
52Mazziotti G Floriani I Bonadonna S Torri V Chanson PGiustina A Effects of somatostatin analogs on glucosehomeostasis a metaanalysis of acromegaly studies J ClinEndocrinol Metab 2009 941500ndash8
53Higham CE Trainer PJ Growth hormone excess and the de-velopment of growth hormone receptor antagonists ExpPhysiol 2008 931157ndash69
54Trainer PJ Drake WM Katznelson L et al Treatment of acro-megaly with the growth hormone receptor antagonist pegvi-somant N Engl J Med 2000 3421171ndash7
55Van der Lely AJ Hutson RK Trainer PJ Besser GM Barkan ALKatznelson L et al Long-term treatment of acromegaly withpegvisomant a growth hormone receptor antagonist Lancet2001 3581754ndash9
56Buchfelder M Weigel D Droste M Mann K Saller B BrubachK et al Pituitary tumor size in acromegaly during pegvisom-ant treatment experience from MR re-evaluations of theGerman Pegvisomant Observational Study Eur J Endocrinol2009 16127ndash35
57 Jaffe CA Barkan AL Treatment of acromegaly with dopamineagonists Endocrinol Metab Clin North Am 1992 21713ndash35
58Sandret L Maison P Chanson P Place of cabergoline in acro-megaly a meta-analysis J Clin Endocrinol Metab 2011961327ndash35
59Sherlock M Woods C Sheppard C Medical therapy in acro-megaly Nat Rev Endocrinol 2011 7291ndash300
60Samson SL Ezzat S AACEACE disease state clinical reviewdopamine agonists for hyperprolactinemia and the risk ofcardiac valve disease Endocr Pract 2014 20608ndash16
61 Jaquet P Gunz G Saveanu A Dufour H Taylor J Dong J et alEfficacy of chimeric molecules directed towards multiplesomatostatin and dopamine receptors on inhibition of GHand prolactin secretion from GH-secreting pituitary aden-omas classified as partially responsive to somatostatin ana-log therapy Eur J Endocrinol 2005 153135ndash41
62Barkan AL Halasz I Dornfeld KJ Jaffe CA Friberg RDChandler WF et al Pituitary irradiation is ineffective in nor-malizing plasma insulin-like growth factor I in patients withacromegaly J Clin Endocrinol Metab 1997 823187ndash91
63Eastman RC Gorden P Glatstein E Roth J Radiation therapyof acromegaly Endocrinol Metab Clin North Am 199221693ndash712
64 Jenkins PJ Bates Carson MN Stewart PM Wass JAConventional pituitary irradiation is effective in loweringserum growth hormone and insulin-like growth factor-I inpatients with acromegaly J Clin Endocrinol Metab 2006911239ndash45
65Minniti G Gilbert DC Brada M Modern techniques for pituit-ary radiotherapy Rev Endocr Metab Disord 2008 10135ndash44
66Stapleton CJ Liu CY Weiss M The role of stereotactic radio-surgery in the multimodal management of growth hormone-secreting pituitary adenomas Neurosurg Focus 2010 29E11
67Biermasz NR van Dulken H Roelfsema F Long-term follow-up results of postoperative radiotherapy in 36 patients withacromegaly J Clin Endocrinol Metab 2000 852475ndash82
68Attanasio R Epaminonda P Motti E Giugni E Ventrella LCozzi R et al Gamma-knife radiosurgery in acromegaly a 4-year follow-up study J Clin Endocrinol Metab 2003 883105ndash12
69Minniti G Traish D Ashley S Gonsalves A Brada M Risk ofsecond brain tumor after conservative surgery and radiother-apy for pituitary adenoma update after an additional 10years J Clin Endocrinol Metab 2005 90800ndash4
70Brada M Burchell L Ashley S Traish D The incidence of cere-brovascular accidents in patients with pituitary adenoma IntJ Radiat Oncol Biol Phys 1999 45693ndash8
71Laws ER Sheehan JP Sheehan JM Jagnathan J Jane JA JrOskouian R Stereotactic radiosurgery for pituitary aden-omas a review of the literature J Neurooncol 2004 69257ndash72
420 | QJM An International Journal of Medicine 2017 Vol 110 No 7
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022

determined by sex age neurotransmitters exercise andstress
GH action is achieved via its interaction with a single-chaintransmembrane glycoprotein receptor (GHR) The GH moleculeinteracts with a preformed dimer of identical GHR pairs causinginternalization of the receptor to initiate signaling As a conse-quence two Janus tyrosine kinase 2 molecules undergoautophosphorylation and in turn phosphorylate the GHR cyto-plasmic domain This activates intracellular proteins involvedin signal transduction and transcription (STAT)5
The gene encoding the GHR is ubiquitously expressed par-ticularly in liver fat and muscle GH activation of the intracellu-lar molecule STAT5b induces transcription of IGF-1 SystemicIGF-1 is synthesized primarily in the liver but also in extrahep-tatic tissues including bone muscle and kidney and in the pitu-itary gland itself IGF-1 circulates in serum bound to IGF-1binding protein (IGFBP-3) or IGFBP-5 and acid-labile subunit ina 150-kD complex Less than 1 of total serum IGF-1 circulatesas a free hormone The IGF-1 cellular effects are mediated bythe IGF-1 receptor (IGF-1R) a heterotetrameric protein structur-ally similar to the insulin receptor IGF-1 acts to mediate tissuegrowth or locally synthesized IGF-1 acts in a paracrine mannerto regulate local GH target tissue growth 6
Several candidate genes that could account for the somato-troph clonal expansion have been examined in animal modelsThese include the retinoblastoma tumor suppression gene andp27 Disruption of the MENIN gene results in multiple endo-crine neoplasia type I Ras mutations have been reported to acti-vate GH secretion in experimental animal models as havemutations of a pituitary tumor-transforming gene Mutations inthe tumor suppressor gene arylhydrocarbon receptor interact-ing protein (AIP) are prevalent in young-onset GH excess pa-tients and familial isolated and young-onset pituitaryadenomas In a longitudinal international collaborative studyKorbonits et al7 identified AIP mutations in 467 of patientswith gigantism in their cohort of 216 patients Two histologicalsubtypes of GH-secreting pituitary adenoma have been identi-fied based on the pattern of cytoplasmic cytokeratin Sparselygranulate cytokeratin at histology suggest more invasive le-sions These lesions are more common in younger patients andare less response to somatostatin receptor ligand therapy8
Clinical features
First observed by Verga in 1864 acromegaly is characterized bydisproportionate skeletal tissue and organ growth At diagno-sis patients may exhibit a spectrum of clinical signs includingskeletal and acral overgrowth and soft tissue enlargement withfrontal bossing mandibular prognathism jaw malocclusionand overbite skin thickening and increased ring and shoe size(Table 1) Other features include hyperhidrosis paresthesiagoiter arthritis kyphoscoliosis headaches visual field deficitscolon polyps sleep apnea and daytime somnolence reproduct-ive disorders and cardiovascular disease9 It should be high-lighted that there is a large spectrum of clinical featuresassociated with acromegaly and patients may have a spectrumof mild to severe clinical phenotype therefore a high index ofsuspicion is required
Morbidity
Acromegaly often evades diagnosis until in its clinically obviouslater stages often resulting in a delay of 5ndash10 years after ap-proximate symptom onset10 Patients often present with
significant co-morbidities including hypertension diabetesmellitus and sleep apnea
Arterial hypertension is reported to affect up to 40 of pa-tients with acromegaly Experimental and clinical studies haveshown that both GH and IGF-1 exert direct effects on myocardialgrowth and function The key feature of acromegaly cardiomy-opathy is concentric biventricular hypertrophy Hypertrophy in-volves proliferation of the myocardial fibrous tissue whichresults in interstitial remodeling and subsequent impaired ven-tricular relaxation and diastolic dysfunction The cardiomyop-athy of acromegaly is further aggravated by hypertension andglucose abnormalities
Valvular heart disease and arrhythmias are more frequentlyobserved in patients with acromegaly with up to 40 of pa-tients suffering from conduction disorders Colao et al6 demon-strated a high prevalence of both mitral and aortic valvedysfunction in patients with active acromegaly If the disease isuncontrolled then diastolic and ultimately systolic heart failurecan develop
Impaired glucose tolerance and diabetes mellitus are fre-quently associated with acromegaly as GH excess promotesinsulin resistance in the liver and the periphery Hyperinsuli-naemia and increased gluconeogenesis are observed in patients
Table 1 Clinical features of acromegaly
Direct tumoreffects
Visual field deficit
Cranial nerve palsyHeadacheHypopituitarism
Soft tissue andskin changes
Increased skin thickness and soft tissuehyperplasia
HyperhidrosisSkin tags and acanthosis nigricans
Bone and jointfeatures
Somatic effects (Acral enlargement prognathismfrontal bossing)
ArthropathyosteoarthritisCarpal tunnel syndromeOsteopenia vertebral fracturesProximal myopathyHearing loss
Cardiovascularfeatures
Biventricular hypertrophy
Increased interventricular septum thickness (ec-centric hypertrophy)
Diastolic dysfunction at rest andor systolic dys-function on effort
Diastolic heart failureArrthymiasHypertensionEndothelial dysfunction and increased carotid IMT
Metabolicfeatures
Impaired fasting glucose
Impaired glucose toleranceDiabetes mellitusInsulin resistanceReduced total cholesterol and increased
triglyceridesIncreased nitrogen retention
Respiratoryfeatures
Upper airway obstruction
MacroglossiaSleep apnea
412 | QJM An International Journal of Medicine 2017 Vol 110 No 7
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
with acromegaly11 The exact prevalence of overt diabetes mel-litus in acromegaly is unknown but ranges from 19 to as highas 5212 The differing prevalence rates are likely due to the het-erogeneity of the case series in addition to the impact of revisedaccepted criteria for the diagnosis and classification of diabetesmellitus
Respiratory disorders can develop in patients with acromeg-aly as a result of anatomical changes affecting craniofacialbone and soft tissues as well as alterations in activity of re-spiratory muscles Sleep apnea can affect up to 60 of patientsmost often due macroglossia and anatomical narrowing of theupper airways Central sleep apnea has been observed in a mi-nority of cases13
Arthropathy affects 75 of patients with acromegaly and isthe leading cause of morbidity and functional disability forthese patients14 Pain is the most common symptom usuallyexacerbated by activity Carpal tunnel syndrome is present inup to 64 of patients at presentation15 With disease progres-sion the bone undergoes accelerated turnover and the articularcartilage thins with narrowing of joint spaces similar to fea-tures of osteoarthiritis A recent meta-analysis observed ahigher bone formation but with a greater frequency of vertebralfractures compared with controls16
In recent years particular focus has been placed on colorec-tal cancer (CRC) to a lesser extent on breast prostate and thy-roid cancer rates in patients with acromegaly The pooled oddratios are increased for benign neoplasia (248 for colonic aden-omas and 3557 for hyperplastic polyps) in addition to coloncancer (204ndash4351)17 Orme et al investigated the incidence andmortality for cancer in a cohort of 1239 patients They excludedall malignancies pre-diagnosed to the diagnosis of acromegalyand used reliable national cancer registers for cross-examin-ation The overall cancer incidence was lower in the acromegalypatients than in the normal population (79 vs 109 malignanciesrespectively) However the SIRs revealed a small increase incolon cancers in acromegaly patients (SIR 168) and the deathrate from colon cancer outnumbered that recorded in the nor-mal population (13 observed deaths vs 5 expected) The occur-rence of cancer was unrelated to either disease duration or ageat diagnosis but the standard mortality rate associated withcancer was higher with post-treatment levels of GHgt10 lgl18
More recent results from the German Acromegaly Registry for446 patients (6656 person-years from diagnosis) did not showany evidence for a higher incidence of cancer (SIR 075 95CI055ndash10) most notably CRC or breast cancer19
Mortality
It is well reported in the literature that untreated acromegaly isassociated with reduced life expectancy Analysis of the deter-minants of mortality indicate that 60 die from cardiovascu-lar disease 25 from respiratory disease and 15 frommalignancies With advances in the medical therapy surgicaltechniques and localized stereotactic radiotherapy overall mor-tality rates in acromegaly have improved Although mortality inacromegalic patients remains elevated compared with the gen-eral population in several studies the mortality increase is gen-erally less than 2-fold compared with the 2- to 3-fold mortalityrates seen in earlier series20
There is compelling evidence to support that the last avail-able follow-up GH value is the most predictive survival indexBates et al21 reported that in a cohort of 79 patients with acro-megaly the Standardised Mortality ratio (SMR) fell from 26 to20 if treatment reduced GH levels to under 10 mUl (5 lgl) Even
more significant was the fact that mortality was reduced to nor-mal if post-treatment GH levels of lt5 mUl (25 lgl) wereachieved21 In the West Midlands Acromegaly Study compari-son of crude death rates per 1000 population suggested that aGH of 2 lgl may be a more appropriate treatment target with astep-up in the death rate once GH exceeded 2 lgl22 The FinnishNationwide Survey of Mortality in Acromegaly reported similarfindings In a cohort of 334 acromegalic patients with 56 deathsexcess mortality was seen in those with post-treatment GH lev-els gt25 lgl (SMR 163 (11ndash235) Plt 0001)23
In a recent meta-analysis Holdaway et al focused on the re-lationship between biochemical measurements and mortalityduring follow-up after treatment for acromegaly24 Mortalitywas close to the expected level when last available GH wasunder 25 lgl (SMR 11 95 CI 09ndash14) but was significantlyelevated in those with last available GH above 25 lgl (SMR 1995 CI 15ndash24)
Therefore the biochemical aim of treatment in acromegalyshould be reduction of GH values to lt25 lgl and possibly evenlower to lt1 lgl although care must be taken that this is not atthe expense of inducing GH deficiency and hypopituitarismwhich in itself is associated with an adverse outcome20
The introduction of GH antagonists as medical treatment foracromegaly necessitates the use of IGF-I in the biochemicalmonitoring of patients treated with these agents Holdaway et alfound that those with normal IGF-1 had mortality close to theexpected values for the general population (SMR 11 95 CI 09ndash14) whereas the SMR for those with elevated IGF-1 at last fol-low-up remained significantly increased (SMR 25 95 CI 16ndash40) However it should be noted that two of the largest studiesin the meta-analysis comprising a total of 151 deaths in 753 pa-tients have failed to demonstrate any relationship betweenpost-treatment IGF-1 levels and mortality(Relative Risk 12 95CI 071ndash202 Pfrac14 05 and RR 046 95 CI 017ndash126 Pfrac14 013) sug-gesting that last available serum IGF-I may not be as reliable amarker of mortality in acromegaly as last available GH
There are also methodological problems with using the lastavailable GHIGF-I in the analysis for mortality because thisvalue is inherently biased and does not take into account priorGHIGF-1 levels Many studies were also performed using olderassays that may not be used in clinical practice today howeverit may take many years to get meaningful data on survival usingnewer more sensitive assays and these older studies have to beinterpreted with this in mind
In the West Midlands study compared with the generalpopulation the use of external radiotherapy was associatedwith increased mortality with an SMR of 158 (95 CI 122ndash204Pfrac14 0005) and when assessed on internal analysis within theacromegaly cohort resulted in an RR of 167 (95 CI 11ndash256Pfrac14 002) In the Finnish survey mortality was also increased inpatients who had been treated with radiotherapy [SMR 169(95 CI 105ndash 258) Plt 0001] In the Spanish acromegaly regis-try patients who died had a twice greater probability of havingbeen treated with radiotherapy than those who had survived(hazard ratio 229 95 CI 103ndash508 Pfrac14 0026)
Although hypopituitarism is associated with increased mor-tality first identified by Rosen and Bengtsson25 there is littledata on the role of hypopituitarism in patients with acromegalyIn the West Midlands study there was a trend (Pfrac14 007) towardreduced survival in patients with acromegaly who had a greaternumber of deficient hypothalamo-pituitary axes compared withthose without evidence of hypopituitarism Sherlock et alshowed that neither TSH deficiency nor gonadotropin defi-ciency was associated with increased mortality in acromegaly
R Dineen et al | 413
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
on internal analysis (gonadotropin deficiency was associatedwith increased SMR compared with the general population)however adrenocorticotrophic hormone (ACTH) deficiency wasassociated with increased mortality [RR 17 (95 CI 12ndash25)Pfrac14 0004] The cause of death was predominantly cardiovascu-lar and higher doses of hydrocortisone therapy were associatedwith increased mortality20
Other variables found to influence outcome included hyper-tension duration of the disorder before treatment and ageHypertension and glucose intolerance are important contribu-tory factors to the vascular morbidity associated with acromeg-aly However there are few published reports on their impacton mortality in acromegaly and how this correlates with GHand IGF-I levels Hypertension is considered one of the mostrelevant negative prognostic factors for mortality inacromegaly
Diagnosis
The diagnosis of acromegaly is based upon a combination ofclinical examination and biochemical demonstration of dysre-gulated autonomous GH secretion as well as elevated IGF-1 lev-els Serum GH concentrations are typically elevated but levelsmay fluctuate widely Measuring serum IGF-1 in a patient withclinically suspected acromegaly should be the initial test26 It isalso recommended to test patients without the typical clinicalappearance but who have associated comorbidities sleepapnea type 2 diabetes disabling arthritis carpal tunnel syn-drome hyperhidrosis and hypertension A normal IGF-1 level(using age- and sex-matched reference ranges) effectively ex-cludes the diagnosis of acromegaly False positives may occur inpregnancy patients taking estrogen therapy and late-stage ado-lescence Multiple factors can make the biochemical interpret-ation of IGF-1 level challenging including the presence ofcertain pathological conditions such as hepatic and renal fail-ure malnutrition hypothyroidism and uncontrolledhyperglycemia
Failure of normal suppression of serum GH following astandard 75 g-oral glucose load remains the gold-standard diag-nostic test and should be used to confirm the diagnosis in allcases with high or equivocal IGF-1 or in the presence of condi-tions interfering with the measurement where clinical suspi-cion is high27
The use of higher sensitivity immunofluorometric chemilu-minescent and immunoradiometric assays has been associatedwith significantly lower nadir GH during oral glucose tolerancetest (OGTT) in healthy controls than was previously thought(ranging from 0029ndash025 mgl) with a gender difference notedin some studies 27
As ultrasensitive immunoassays are not uniformly availableworldwide current guidelines suggest a cutoff for nadir GH afterOGTTlt 1 lgl acceptable for exclusion of the diagnosis26 Itshould be highlighted that this could result in inaccurate exclu-sion of mild active disease A further challenge in diagnosis isthe presence of discordant serum GH and IGF-1 levels ElevatedIGF-1 with normal GH may reflect early disease and should war-rant further investigation (including imaging) to clarify thediagnosis28
Current guidelines recommend contrast-enhanced pituitaryMRI as the first line imaging modality after biochemical con-firmation of acromegaly If MRI is contraindicated or unavail-able then pituitary computed tomography should be performedAt diagnosis macroadenomas are detected in 73 of patients2
Visual field testing is recommended in all patients with con-firmed pituitary tumors As onset is often insidious patients maynot be aware of any alteration in their vision and a baseline as-sessment facilitates accurate interpretation of further testing if adeterioration is reported by the patient or in response to therapy
Assessment of the integrity of the other pituitary hormonesby the combination of basal and appropriate dynamic testing isrecommended Hyperprolactinemia from tumor co-secretionoccurs in up to a third of patients and can contribute to hypo-gonadism but may also occur a result of lsquostalk effectrsquo due totumor compression of the pituitary stalk interrupting the deliv-ery of inhibitory dopamine to the pituitary29 Evaluating all pa-tients with acromegaly for associated co-morbidities isrecommended at diagnosis (Table 2) in addition to longitudinalmonitoring during follow-up26
Treatment
Treatment goals in acromegaly include symptom relief tumorcontrol with maintenance of pituitary function biochemicalnormalization of GHIGF-1 and reversal of the excess morbidityand mortality associated with the disorder Current modalitiesof treatment available include surgery medical therapy andradiotherapy Treatment is complex and frequently more thanone modality is required to achieve treatment goals The deci-sion to treat and the therapeutic intervention used is based on anumber of factors which need to be weighed and tailored care-fully for each patient in a multidisciplinary setting
The definition of biochemical remission is difficult due tovariability in the assay and reference ranges used It is crucialthat the same GH and IGF-1 assay is maintained in the same pa-tient throughout their management While it remains contro-versial the current recommended biochemical target is arandom GHlt 1 lgl26 The decline in IGF-1 is more delayed com-pared with GH likely due to differential half-life of IGF-bindingproteins IGF-1 levels measured at 12 weeks after surgery are avalid reflection of surgical remission If the IGF-1 level hasdeclined but is still not normal measurement of a repeat IGF-1level is warranted due to variability in the IGF-1 assay
A normal IGF-1 value and undetectable GH value are suffi-cient for indicating surgical remission However if the GH is de-tectable (ie gt04 lgL) measurement of GH after a glucose loadmay yield important information The mean value of severalsamples taken a few hours apart throughout the day can also beused (GH day curve (GHDC)) as it is significantly correlated withthe GH nadir during OGTT and with the IGF-1 level30 While theideal endocrine outcome of any therapy in acromegaly is a nor-mal IGF-1 value and undetectable GH value levels that are asso-ciated with a normalization of mortality (as discussed in thesection above relating to mortality) are acceptable
Surgery
Transphenoidal surgery by an experienced pituitary surgeon isthe initial treatment of choice recommended for the majority ofpatients26 Ninety percent of patients who undergo pituitary sur-gery are treated using the transphenoidal approach craniotomy israrely performed The development of endoscopic and microsurgi-cal transphenoidal surgery offers further advantages over the con-ventional techniques including the possibility of superior tumorclearance in previously difficult to access areas less surgical mor-bidity fewer complications and reduced postoperative pain31
The main postoperative complaints relate to the transphe-noidal approach including nasal congestion sinusitis and
414 | QJM An International Journal of Medicine 2017 Vol 110 No 7
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
epistaxis More serious complications include hemorrhage CSFleakage and risk of meningitis stroke visual impairment vas-cular injury transient diabetes insipidus (DI) (typically occur-ring as a result of intraoperative manipulation of the pituitarystalk) and hypopituitarism32 Despite significant co-morbiditiesin patients with acromegaly surgical mortality rates of lt05can be anticipated33
Several factors are associated with reduced surgical successrates including large tumor size extrasellar extension andhigher preoperative GH levels34 Recurrence rates peak in years1ndash5 postoperatively with reported recurrence rates of up to 8with recurrence rates being lower in microadenomas comparedwith macroadenomas35 A normal IGF value and undetectableGH value are sufficient for indicating surgical remission
The Acromegaly group consensus guidelines suggest that ina patient with persistent disease after surgery repeat surgerymay be an option if the tumor is accessible26 The decision toinitiate somatostatin therapy prior surgery remains controver-sial In a prospective study of 30 patients with newly diagnosedacromegaly reductions in GH and IGF-1 concentrations andtumor volume were observed following 24 weeks of preopera-tive lanreotide autogel therapy36 Further studies do not reportany difference in the long-term results37 Due to the lack ofrandomized controlled studies the Acromegaly group consen-sus recommend against the routine use of preoperative somato-statin therapy In certain circumstances particularly forpatients with severe soft tissue growth complicating anestheticrisk or with significant comorbidities that may be improved bypreoperative therapy pretreatment with somatostatin receptorligands (SRL) may be considered38
Surgical debulking may be considered in patients with lowpredictive surgical cure rate at diagnosis to improve the chanceof achieving target GHIGF-1 levels with subsequent medicaltherapy Pretreatment disease burden is inversely correlatedto somatostatin analogue responsiveness39 In addition tobiochemical testing of remission as outlined above a contrast-enhanced MRI is recommended at least 12 weeks postopera-tively to visualize residual tumor This provides a baseline forfuture surveillance Formal visual field testing should also beperformed for patients with pre-operative visual deficits
Successful surgery by an experience neurosurgeon in a spe-cialized pituitary center can result in immediate biochemical
remission elimination of direct mass effects in addition to pro-viding tissue for immunohistochemical analysis Hence surgeryremains the primary therapeutic intervention in most patientswith acromegaly26
Medical treatment
Medical therapy has an important role as an adjunctive treat-ment option for persistent disease following non-curative sur-gery and also as first line therapy where surgery is not a feasibletherapeutic option Consensus guidelines outline the recom-mended role of medical therapy in the treatment of patientswith acromegaly There are a number of options for medicaltherapy in acromegaly including somatostatin receptor ligandsGH receptor antagonists and dopamine agonists
Somatostatin receptor ligands
Somatostatin is distributed throughout the nervous system andexerts neural control over many physiological functions includ-ing the inhibition of GH release It exists in two biologically ac-tive molecular forms somatostatin-14 and somatostatin -28with a short half-life of 2-3 min Its action is mediated throughG-protein coupled cell-surface receptors identified in a varietyof tissues including the pituitary Both bioactive forms havehigh binding affinity toward all five identified receptor sub-types SSR1-SSR540 GH-secreting pituitary adenomas expresspredominantly SSR2 and SSR5 First generation somatostatinanalogs octreotide and lanreotide show high affinity binding toSSR2 and to a lesser extent to SSR541
Currently three long-acting SRL formulations are availableoctreotide LAR Lanreotide depotautogel and pasireotide Rapidacting subcutaneous octreotide is also available and is adminis-tered two-three times daily The long-acting octreotide LAR isadministered intramuscularly every 4ndash6 weeks The approvedstarting octreotide LAR dose is 20 mg monthly with dose titra-tion every 3ndash6 months to a maximum dose of 40 mg monthlyLanreotide is available in a microsphere formulation (depot) in-jected intramuscularly every 7ndash14 days and an aqueous solution(Autogel) administered by deep subcutaneous injection every 4ndash6 weeks For lanreotide autogeldepot the approved starting
Table 2 Assessment of acromegaly complications at diagnosis and during long-term monitoring
At diagnosis During long-term follow-up
BP measurement Every 6 months or when change of treatment (if hypertensive)Echocardiography AnnuallyECG AnnuallyEpworth scale or sleep study AnnuallyECHO Doppler of peripheral arterial and venous
systemAnnually particularly in gigantism
OGTT Fasting blood glucose every 6 months (particularly in uncontrolled disease andduring SRL therapy) HbA1c every 6 months if diabetes present
Total testosterone SHBG and prolactin (males) Annually (free testosterone when doubts in interpretation of total testosterone)LH FSH17b-estradiol and prolactin (females) AnnuallyAcroQol AnnuallyDEXA Every 2 years if patient with osteopeniaosteoporosisThoracic and lumbar spine Xray Every 2ndash3 years if osteoporosis risk factors kyphosis or symptomsColonoscopy Every 10 years (more frequently if IGF-1 remains persistently elevated or if abnormal
colonoscopy or family history of chronic cancer)Genetic screening for markers of familial acromeg-
aly (if suspicion)
R Dineen et al | 415
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
dose is 90 mg monthly with a maximum dose up to 120 mgmonthly26
A large body of evidence supports the efficacy of long -actingSRL therapy In a critical analysis of the largest studies octreo-tide LAR reduced GH tolt25 lgl and normalized the IGF-1 levelsin 66 and 63 respectively42 Similar targets were achievedwith lanreotide-SR in 52 and 47 of cases respectively An ear-lier meta-analysis by Freda et al43 reported the overall chance ofIGF-1 normalization was 67 with octreotide and 47 with lan-reotide SR The higher efficacy reported with octreotide may beaccounted by pre-selection of responsive cases (patients whoshowed response to short acting octreotide only being recruitedto studies) inclusion of both primary and secondary therapycases and small case series An inherent challenge to meta-analyses in such a complex condition is the lack of standardiza-tion of GH and IGF-1 assays making comparison of absolutevalues between studies impossible
Smaller tumors lower baseline GH and IGF-1 levels44 highSSR2 and SSR5 expression45 and those previously treated withsurgery are associated with a better response to SRL treatmentRoutine performance of somatostatin receptor scintigraphy oran acute GH response to a subcutaneous octreotide injection asa determinant of SRL response are not recommended26
Somatostatin receptor ligands also have proven efficacy intumor volume reduction This has been extensively reviewedrecently by Colao et al46 Tumor reduction may be mediated bydirect anti-proliferative effects via activation of somatostatinreceptors or indirectly through angiogenesis inhibitionSathyapalan et al47 showed a significant reduction in the func-tional vascularity of pituitary tumors in a small study of five pa-tients after 24 weeks of octreotide therapy
Published meta-analysis revealed that octreotide LAR andlanreotide formulation induce tumor shrinkage in 660 and328 of cases respectively4849 Tumor reduction is progressivewith prolonged treatment and decreased IGF-1 levels may beits best predictor followed by age and degree of GH decrease
A recent detailed review of published studies evaluatingsomatostatin analogues as first line therapy showed that 6-24months of octreotide LAR therapy achievedgt20-30 tumor vol-ume reduction in 73-85 of patients Unlike surgery primarymedical therapy cannot cure acromegaly Based on a recentmeta-analysis of available studies primary SRL therapy is asso-ciated with a lower remission rates compared to initial surgery(45 vs 67)49 However the accuracy of these remission ratesis questionable given the non-comparable nature and the het-erogeneity of studies included Primary SRL therapy can beoffered before surgery in patients with contraindications incases with unresectable tumor or with severe comorbidities26
During SRL treatment the most frequent side effects includeabdominal discomfort flatulence cramps and diarrheaGallbladder sludge or gallstones occur in 25 of subjects butare usually asymptomatic SRL treatment was initially thoughtto aggravate the increased risk of glucose intolerance in thesepatients but the overall effect on glucose metabolism is not clin-ically significant50
Pasireotide is a multireceptor-targeted somatostatin recep-tor ligand which has higher functional activity than octreotideon SSR subtypes except type 4 but in particular SSR551 In alarge phase III randomized trial in patients with acromegalywho were naive to medical therapy pasireotide LAR and octreo-tide LAR have a similar effect of tumor reduction despite thefact that pasireotide was superior to octreotide in providing bio-chemical control After 12 months of treatment 81 of pasireo-tide patients had20 reduction in tumor volume compared
with 77 of octreotide LAR patients52 Pasireotide has similarrates of gastrointestinal side effects to other SRLs however therates of hyperglycemia are significantly higher (occurring in 31ndash57 of patients)
Pegvisomant
Pegvisomant is a pegylated recombinant analog of human GHincorporating nine amino acid mutations Pegylation extendsthe half-life by reducing renal clearance53 The mutations resultin increased affinity to the GH receptor in addition to blockingthe second binding site on the receptor preventing GHR dimer-ization and signal transduction GH hypersecretion persists asit does not target the GH secreting tumor at the level of the pitu-itary hence GH measurements cannot be used to monitor dis-ease activity and IGF-1 becomes the sole marker to monitorbiochemical response during therapy
Pegvisomant has been shown to be highly effective in pro-viding biochemical control of acromegaly in multiple studies Ina 12-week double-blind placebo controlled study Trainer et al54
randomly assigned patients to receive placebo 10 15 or 20 mgof pegvisomant Normalization of IGF-1 (using age and sex-matched reference ranges) was achieved in 10 54 81 and89 respectively Symptom control was also observed The effi-cacy of pegvisomant over a longer period was subsequentlystudied Van der Lely et al55 reported 97 of patients achievingnormal IGF-1 levels in patients receiving therapy for 12 monthsor more (Figure 1) Dose reduction was required in 1190 pa-tients as IGF-1 levels dropped below normal reference range forage and sex
As mentioned above pegvisomant does not exert a centraleffect on pituitary GH secretion hence fears exist over the pos-sibility of increased tumor growth The German PegvisomantObservational Study is a multicenter surveillance study com-menced in 2004 to assess the efficacy and safety of pegvisomanttherapy in patients with acromegaly56 Neuroradiological moni-toring of tumor extension is performed with MRI imagingBuchfelder et al studied 3 years of follow-up data of 307 pa-tients Tumor progression was reported in between 2 and3 ofpatients treated an increase not outside the expected rate inpatients not treated with pegvisomant
Pegvisomant is administered as daily subcutaneous injec-tion It is generally well tolerated with adverse effects reportedinlt10 of patients These may include injection site reactionswith reversible lipohypertrophy and deranged liver functiontests (attributable to the polyethylene glycol pegylated vehicle)
The predominant limiting factor for use of this agent in clin-ical practice remains its considerable cost It is most often usedas a second line agent in cases resistant or intolerant to SRLtherapy or in combination with SRLrsquos in partially resistantcases It is also a potential treatment option in acromegaly pa-tients with difficult to control diabetes mellitus due to its favor-able effect on glycemic control
Dopamine agonists
Dopamine agonists bind to the D2 dopamine receptors in the pi-tuitary gland and suppress prolactin and GH secretion The useof bromocriptine a first-generation dopamine agonist is lim-ited by its side effect profile including GI symptoms lethargyand orthostatic hypotension It also compares poorly with som-atostatin receptor ligands in terms of efficacy with normaliza-tion of GHIGF-1 reported in only 10 of patients57
416 | QJM An International Journal of Medicine 2017 Vol 110 No 7
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
Cabergoline an ergot derivative dopamine agonist has beenused for decades in the treatment of hyperprolactinaemia andParkinsonrsquos disease Cabergoline is better tolerated and more ef-fective than bromocriptine however its use was superseded bythe development of SRL therapy showing higher efficacy rates
Clinical trials of cabergoline in acromegaly are small non-randomized and report variable results In a recent systematicreview of 10 trials with a total of 150 acromegaly patients con-trol of acromegaly was achieved in 34 of patients who receivedcabergoline therapy alone and 52 when added to SRL therapyin patients with suboptimal control58 Consequently currentguidelines recommend the use of cabergoline in patients withinadequate response to other medical treatment with highestbenefit expected in cases with modest persistent hormonal ele-vations26 Conflicting data exists as to whether the co-secretionof prolactin is predictive of response to dopamine agonist ther-apy Some studies conclude that tumors that co-secrete prolac-tin and GH have a greater response to dopamine agonisttherapy than those than solely secrete GH whereas othersshow no effect There remains little data available regardingtumor shrinkage in patients with acromegaly who are receivingdopamine agonist therapy59 Jaffe et al57 reported combined re-sults from a number of studies which revealed that 29 of pa-tients had some tumor shrinkage on dopamine agonist therapyand the majority of patients who had tumor shrinkage werealso hyperprolactinemic It is difficult to interpret these findinggiven the small number and heterogeneous characteristics ofthe patients included
The most frequent adverse effects of dopamine agonist ther-apy are nausea constipation headache mood disturbancenasal stuffiness and dizziness Cardiac valve abnormalitieswere described with high doses of cabergoline used inParkinsonrsquos disease but not with current recommended dosageused for patients with acromegaly60
DopastatinBIM-23A760 is a chimeric molecule hasbeen shown in vitro to have high affinity for both somatosta-tin receptor subtypes- 2 and 5 in addition to dopamine 2 recep-tor61 With increasing knowledge of the importance of SSR5 inregulation of GH in GH-secreting adenomas dopastatin isundergoing further development in clinical studies to deter-mine if there is a role for these compounds in the treatment ofacromegaly
Radiotherapy
Radiation therapy is used as adjuvant treatment in the settingof persistent disease despite surgery andor medical treatmentor if medical therapy is unavailable unsuccessful or not toler-ated Radiotherapy has been shown to be effective in loweringserum GH levels36 but conflicting results have been reported re-garding the normalization of IGF-1 levels62 Furthermore thedelay in therapeutic benefit and the high risk of developinghypopituitarism serve as arguments against the more routineuse of radiotherapy
Conventional radiotherapy has been used for gt30 years inthe adjunctive treatment of pituitary adenomas It is generallydelivered in fractionated doses 4ndash5 times per week so as to re-duce daily-fractionated dose The risk of adverse effects beingproportional to maximal dose per day63 Early studies of con-ventional radiotherapy reported high efficacy rate of 80ndash100however remission was defined as a GH level below 5-10 ngmlMore recent studies using revised biochemical remission tar-gets report a mean remission rate between 50 and 60 Jenkinset al64 assessed the effects of conventional pituitary irradiationin 884 patients of the UK National Acromegaly Register MeanGH levels declined from 135 to 53 ngml at 2 years after surgeryto 2 ngml by 10 years and a further decline to 11 ngml at 20years (Figure 2) Furthermore they observed a parallel fall in IGF-
Figure 1 Baseline and lowest values of individual serum insulin-like growth factor-1 concentrations achieved in 90 patients treated for 12 months or more with daily
pegvisomant (daggerPlt005 vs baseline DaggerPlt001 vs baseline) The shaded area represents the age-adjusted normal range for insulin-like growth factor-155
R Dineen et al | 417
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
1 levels with 63 of patients having a normal level by 10years64
Stereotactic radiotherapy offers improvement in immobil-ization imaging and treatment delivery from conventionaltechniques It can be delivered as a single fraction radiosurgeryusing a Gamma knife (a source of cobalt) or a linear acceleratoror a stereotactic conformal radiotherapy delivered as fractio-nated treatment using a linear accelerator There is no clear ad-vantage for either of the radiosurgical techniques in terms ofsparing normal tissue receiving high doses of radiation65 A crit-ical analysis of the literature reported variable rates of both bio-chemical and tumor response 17ndash82 and 37ndash100respectively66 The authors attributed the wide variability to theuse of different treatment schedules and definitions ofremission
Hypopituitarism is less frequent with radiosurgery than con-ventional radiotherapy At least 50 of patient treated with con-ventional radiotherapy will have acquired new anteriorpituitary hormonal deficits at 10 years67 In cohorts treatedsolely with stereotactic techniques rates of hypopituitarismvary between 0 and 2068 However it is likely that the candi-dates for stereotactic radiotherapy had smaller remnants of dis-ease and therefore less normal tissue irradiated
Annual hormonal testing is required due to the risk of latehypopituitarism26 Other complications following radiotherapyinclude the risk of second brain tumors stroke and rarely opticneuropathy cranial nerve deficits and radionecrosis a rare ad-verse effect of gamma knife radiotherapy69ndash71
Patients treated with conventional radiotherapy have beenreported to have increased mortality predominantly due tostroke independent of GHIGF-I levels and hypopituitarism20
Current guidelines recommend the use of stereotactic radio-therapy over conventional radiation therapy unless significantresidual tumor burden or the lesion is too close to the opticchiasm26
Conclusion
Prolonged exposure to elevated endogenous levels of GH andIGF-I results in a multisystem disease characterized by somaticovergrowth multiple co-morbidities and premature mortalityEarly detection prevents the development of irreversible com-plications of the disease including cardiomyopathy respiratory
dysfunction and arthropathy Despite the imprecision of assaysfor GH and IGF-I it is clear from epidemiologic studies that tightbiochemical control is essential to reduce morbidity controlsymptoms and improve mortality rates
Optimal implementation of current guidelines in routine clin-ical practice and maximal use of the medical treatment could im-prove the long-term control of patients with significant benefitsfor morbidity and mortality Another important aspect in thetreatment of patients with acromegaly is also the appropriate tar-geted treatment of co-morbidities associated with acromegaly
Achievement of the criteria for cure during or after therapyis determined by assessing biochemical control targeting con-trolled levels of GH and normalization of IGF-I levels monitor-ing tumor size assessing residual pituitary function andmonitoring co-morbidities
New therapeutic molecules currently in trials will hopefullyoffer further benefit to those patients resistant to current thera-peutic modes for this chronic progressive disorder
Conflict of interest None declared
References1 Melmed S Braunstein GD Horvath E Ezrin C Kovacs K
Pathophysiology of acromegaly Endocr Rev 1983 4271ndash902 Mestron A Webb SM Astorga R Benito P Catala M
Gaztambide S et al Epidemiology clinical characteristicsoutcome morbidity and mortality in acromegaly based onthe Spanish Acromegaly Registry (Registro Espanol deAcromegalia REA) Eur J Endocrinol 2004 151439ndash46
3 Jagannathan J Dumont AS Prevedello DM Oskouian RJLopes B Jane JA Jr and Laws ER Jr Genetics of pituitary aden-omas current theories and future implications NeurosurgFocus 2005 19E4
4 Zhu X Lin CR Prefontaine CG Tollkuhn J Rosenfeld MGGenetic control of pituitary developement and hypopituitar-ism Curr Opin Genet Dev 2005 15332ndash40
5 Melmed S Acromegaly pathogenesis and treatment J ClinInvest 2009 1193189ndash202
6 Colao A Ferone D Marzullo P Lombardi G Systemic compli-cations of acromegaly epidemiology pathogenesis andmanagement Endocr Rev 2004 25102ndash52
7 Korbonits M Gadelha MR Roncaroli F Grossman AB Ellard SEvanson J et al Landscape of familial isolated and young-onset pituitary adenomas prospective diagnosis in AIP mu-tation carriers J Clin Endocrinol Metab 2015 100E1242ndash54
8 Larkin S Reddy R Karavitaki N Cudlip S Wass J Ansorge OGranulation pattern but not GSP or GHR mutation is associ-ated with clinical characteristics in somatostatin-naive pa-tients with somatotroph adenomas Eur J Endocrinol 2013168491ndash9
9 Molitch ME Clinical manifestations of acromegaly EndocrinolMetab Clin North Am 1992 21597ndash614
10Reid TJ Post KD Bruce JN Nabi KM Reyes-Vidal CM et alFeatures at diagnosis of 324 patients with acromegaly didnot change from 1981 to 2006 acromegaly remains under-recognized and under-diagnosed Clin Endocrinol 201072203ndash8
11Moslashller N Joslashrgensen JO Abildgard N Orskov L Schmitz OChristiansen JS Effects of growth hormone on glucose me-tabolism Horm Res 1991 36 (Suppl 1)32ndash5
12Dreval AV Trigolosova IV Misnikova IV Kovalyova YATishenina RS Barsukov IA et al Prevalence of diabetes melli-tus in patients with acromegaly Endocr Connect 2014 393ndash8
Figure 2 Percentage of all patients achieving a serum GH level lt25 ngml (bars)
and the mean GH level (line) in the years after pituitary irradiation64
418 | QJM An International Journal of Medicine 2017 Vol 110 No 7
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
13Roemmler J Gutt B Fischer R Vay S Wiesmeth ABidlingmaier M et al Elevated incidence of sleep apnoea inacromegaly-correlation to disease activity Sleep Breath 2012161247ndash53
14Killinger Z Payer J Lazurova I Imrich R Homerova Z KuzmaM et al Arthropathy in acromegaly Rheum Dis Clin North Am2010 36713ndash20
15Kameyama S Tanaka R Hasegawa A Tamura T Kuroki MSubclinical carpal tunnel syndrome in acromegaly NeurolMed Chir 1993 33547ndash51
16Mazziotti G Biagioli E Maffezzoni F Spinello M Serra VMaroldi R et al Bone turnover bone mineral density and frac-ture risk in acromegaly a meta-analysis J Clin EndocrinolMetab 2015 100384ndash94
17Renehan AG OrsquoConnell J OrsquoHalloran D Shanahan F PottenCS OrsquoDwyer ST et al Acromegaly and colorectal cancer acomprehensive review of epidemiology biological mechan-isms and clinical implications Horm Metab Res 200335712ndash25
18Orme S McNally RJ Cartwright RA Belchetz PE Mortality andcancer incidence in acromegaly a restrospective cohortstudy J Clin Endocrinol Metab 1998 832730ndash4
19Petroff D Teuroonjes A Grussendorf M Droste M Dimopoulou CStalla G et al The Incidence of cancer among acromegaly pa-tients results from the German Acromegaly Registry J ClinEndocrinol Metab 2015 1003894ndash902
20Sherlock M Ayuk J Tomlinson JW Toogood AA Aragon-Alonso A Sheppard MC et al Mortality in patients with pitu-itary disease Endocr Rev 2010 31301ndash42
21Bates AS Vanrsquot H Jones JM Clayton RN An audit of outcomeof treatment in acromegaly Q J Med 1993 86293ndash9
22Ayuk J Clayton RN Holder G Sheppard MC Stewart PMBates AS Growth hormone and pituitary radiotherapy butnot serum insulin-like growth factor-I concentrations pre-dict excess mortality in patients with acromegaly J ClinEndocrinol Metab 2004 891613ndash7
23Kauppinen-Meuroakelin R Sane T Reunanen A Veuroalimeuroaki MJNiskanen L Markkanen H et al A nationwide survey of mor-tality in acromegaly J Clin Endocrinol Metab 2005 904081ndash6
24Holdaway IM Bolland MJ Gamble GD A meta-analysis of theeffect of lowering serum levels of GH and IGF-I on mortalityin acromegaly Eur J Endocrinol 2008 15989ndash95
25Rosen T Bengtsson BA Premature mortality due to cardio-vascular disease in hypopituitarism Lancet 1990 336285ndash8
26Katznelson L Laws ER Jr Melmed S Molitch ME Murad MHUtz A et al Acromegaly an endocrine society clinical practiceguideline J Clin Endocrinol Metab 2014 993933ndash51
27Freda PU Post KD Powell JS Wardlaw SL Evaluation of dis-ease status with sensitive measures of growth hormone se-cretion in 60 postoperative patients with acromegaly J ClinEndocrinol Metab 1998 833808ndash16
28Dimaraki EV Jaffe CA DeMott-Friberg R Chandler WFBarkan AL Acromegaly with apparently normal GH secretionimplications for diagnosis and follow-up J Clin EndocrinolMetab 2002 873537ndash42
29Losa M Von Werder K Pathophysiology and clinical aspectsof the ectopic GH-releasing hormone syndrome ClinEndocrinol 1997 47123ndash35
30Dobrashian RD OrsquoHalloran DJ Hunt A Beardwell CG ShaletSM Relationships between insulin-like growth factor-1 levelsand growth hormone concentrations during diurnal profilesand following oral glucose in acromegaly Clin Endocrinol 199338589ndash93
31Frank G Pasquini E Farneti G Mazzatenta D Sciarretta VGrasso V et al The endoscopic versus the traditional ap-proach in pituitary surgery Neuroendocrinology 2006 83240ndash8
32Marquez Y Tuchman A Zada G Surgery and radiosurgery foracromegaly a review of indications operative techniquesoutcomes and complications Int J Endocrinol 2012 2012386ndash401
33Laws ER Vance ML Thapar K Pituitary surgery for the man-agement of acromegaly Horm Res 2000 5371ndash5
34Salaun C Foubert L Vialatou M Kujas M Turpin G Prognosticfactors of surgical cure of growth hormone secreting pituitary aden-omas Ann Medecine Interne 1999 150195ndash8
35Kreutzer J Vance ML Lopes MB Laws ER Jr Surgical manage-ment of GH-secreting pituitary adenomas an outcome studyusing modern remission criteria J Clin Endocrinol Metab 2001864072ndash7
36Annamalai AK Webb A Kandasamy N Elkhawad M Moir SKhan F et al A comprehensive study of clinical biochemicalradiological vascular cardiac and sleep parameters in anunselected cohort of patients with acromegaly undergoingpresurgical somatostatin receptor ligand therapy J ClinEndocrinol Metab 2013 981040ndash50
37Shen M Shou X Wang Y Zhang Z Wu J Mao Y et al Effect ofpresurgical long-acting octreotide treatment in acromegalypatients with invasive pituitary macroadenomas a prospect-ive randomized study Endocr J 2010 571035ndash44
38Friedel ME Johnston D Singhal S Al Khalili K Farrell CJEvans JJ et al Airway management and perioperative con-cerns in acromegaly patients undergoing endoscopic trans-sphenoidal surgery for pituitary tumors Otolaryngol HeadNeck Surg 2013 149840ndash4
39Bhayana S Booth G Asa SL Kovacs Ezzat S The implicationof somatotroph adenoma phenotype to somatostatin analogresponsiveness in acromegaly J Clin Endocrinol Metab 2005906290ndash5
40Reisine T Bell GI Molecular biology of somatostatin recep-tors Endocr Rev 1995 16427ndash42
41Zatelli MC Piccin D Tagliati F et al Dopamine receptor sub-type 2 and somatostatin receptor subtype 5 expression influ-ences somatostatin analog effects on human somatotrophpituitary adenomas in vitro J Mol Endocrinol 2005 35333ndash41
42Murray RD Melmed S A critical analysis of clinically avail-able somatostatin analog formulations for therapy of acro-megaly J Clin Endocrinol Metab 2008 932957ndash68
43Freda PU Katznelson L Van der Lely A Reyes CM Zhao SRabinowitz D Long-acting somatostatin analog therapy ofacromegaly a meta-analysis J Clin Endocrinol Metab 2005904465ndash74
44Howlett TA Willis D Walker G Wass JA Trainer PJ Control ofgrowth hormone and IGF1 in patients with acromegaly in theUK responses to medical treatment with somatostatin ana-logues and dopamine agonists Clin Endocrinol 201379689ndash99
45Espinosa de los Monteros AL Carrasco C Albarran AAGadelha M Abreu A Mercado M The role of primary pharma-cological therapy in acromegaly Pituitary 2014 17 (Suppl1)S4ndashS10
46Colao AM Auriemma RS Pivonello R The effects of somato-statin analogue therapy on pituitary tumor volume in pa-tients with acromegaly Pituitary 2016 19210ndash21
47Sathyapalan T Lowry M Turnbull LW Rowland-Hill C AtkinSL Mechanism of action of octreotide in acromegalic tu-mours in vivo using dynamic contrast-enhanced magneticresonance imaging Pituitary 2007 10233ndash6
R Dineen et al | 419
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
48Giustina A Mazziotti G Torri V Spinello M Floriani IMelmed S Meta-analysis on the effects of octreotide ontumor mass in acromegaly PLoS One 2012 7e36411
49Abu Dabrh AM Mohammed K Asi N Farah WH Wang ZFarah MH et al Surgical interventions and medical treat-ments in treatment-naive patients with acromegaly system-atic review and meta-analysis J Clin Endocrinol Metab 2014994003ndash14
50Colao A Bronstein M Freda P Gu F Shen C-C Gadelha Met al Pasireotide versus octreotide in acromegaly a head-to-head superiority study J Clin Endocrinol Metab 2014 99791ndash9
51Schmid HA Schoeffter P Functional activity of the multili-gand analog SOM230 at human recombinant somatostatinreceptor subtypes supports its usefulness in neuroendocrinetumors Neuroendocrinology 2004 80 (Suppl 1)47ndash50
52Mazziotti G Floriani I Bonadonna S Torri V Chanson PGiustina A Effects of somatostatin analogs on glucosehomeostasis a metaanalysis of acromegaly studies J ClinEndocrinol Metab 2009 941500ndash8
53Higham CE Trainer PJ Growth hormone excess and the de-velopment of growth hormone receptor antagonists ExpPhysiol 2008 931157ndash69
54Trainer PJ Drake WM Katznelson L et al Treatment of acro-megaly with the growth hormone receptor antagonist pegvi-somant N Engl J Med 2000 3421171ndash7
55Van der Lely AJ Hutson RK Trainer PJ Besser GM Barkan ALKatznelson L et al Long-term treatment of acromegaly withpegvisomant a growth hormone receptor antagonist Lancet2001 3581754ndash9
56Buchfelder M Weigel D Droste M Mann K Saller B BrubachK et al Pituitary tumor size in acromegaly during pegvisom-ant treatment experience from MR re-evaluations of theGerman Pegvisomant Observational Study Eur J Endocrinol2009 16127ndash35
57 Jaffe CA Barkan AL Treatment of acromegaly with dopamineagonists Endocrinol Metab Clin North Am 1992 21713ndash35
58Sandret L Maison P Chanson P Place of cabergoline in acro-megaly a meta-analysis J Clin Endocrinol Metab 2011961327ndash35
59Sherlock M Woods C Sheppard C Medical therapy in acro-megaly Nat Rev Endocrinol 2011 7291ndash300
60Samson SL Ezzat S AACEACE disease state clinical reviewdopamine agonists for hyperprolactinemia and the risk ofcardiac valve disease Endocr Pract 2014 20608ndash16
61 Jaquet P Gunz G Saveanu A Dufour H Taylor J Dong J et alEfficacy of chimeric molecules directed towards multiplesomatostatin and dopamine receptors on inhibition of GHand prolactin secretion from GH-secreting pituitary aden-omas classified as partially responsive to somatostatin ana-log therapy Eur J Endocrinol 2005 153135ndash41
62Barkan AL Halasz I Dornfeld KJ Jaffe CA Friberg RDChandler WF et al Pituitary irradiation is ineffective in nor-malizing plasma insulin-like growth factor I in patients withacromegaly J Clin Endocrinol Metab 1997 823187ndash91
63Eastman RC Gorden P Glatstein E Roth J Radiation therapyof acromegaly Endocrinol Metab Clin North Am 199221693ndash712
64 Jenkins PJ Bates Carson MN Stewart PM Wass JAConventional pituitary irradiation is effective in loweringserum growth hormone and insulin-like growth factor-I inpatients with acromegaly J Clin Endocrinol Metab 2006911239ndash45
65Minniti G Gilbert DC Brada M Modern techniques for pituit-ary radiotherapy Rev Endocr Metab Disord 2008 10135ndash44
66Stapleton CJ Liu CY Weiss M The role of stereotactic radio-surgery in the multimodal management of growth hormone-secreting pituitary adenomas Neurosurg Focus 2010 29E11
67Biermasz NR van Dulken H Roelfsema F Long-term follow-up results of postoperative radiotherapy in 36 patients withacromegaly J Clin Endocrinol Metab 2000 852475ndash82
68Attanasio R Epaminonda P Motti E Giugni E Ventrella LCozzi R et al Gamma-knife radiosurgery in acromegaly a 4-year follow-up study J Clin Endocrinol Metab 2003 883105ndash12
69Minniti G Traish D Ashley S Gonsalves A Brada M Risk ofsecond brain tumor after conservative surgery and radiother-apy for pituitary adenoma update after an additional 10years J Clin Endocrinol Metab 2005 90800ndash4
70Brada M Burchell L Ashley S Traish D The incidence of cere-brovascular accidents in patients with pituitary adenoma IntJ Radiat Oncol Biol Phys 1999 45693ndash8
71Laws ER Sheehan JP Sheehan JM Jagnathan J Jane JA JrOskouian R Stereotactic radiosurgery for pituitary aden-omas a review of the literature J Neurooncol 2004 69257ndash72
420 | QJM An International Journal of Medicine 2017 Vol 110 No 7
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022

with acromegaly11 The exact prevalence of overt diabetes mel-litus in acromegaly is unknown but ranges from 19 to as highas 5212 The differing prevalence rates are likely due to the het-erogeneity of the case series in addition to the impact of revisedaccepted criteria for the diagnosis and classification of diabetesmellitus
Respiratory disorders can develop in patients with acromeg-aly as a result of anatomical changes affecting craniofacialbone and soft tissues as well as alterations in activity of re-spiratory muscles Sleep apnea can affect up to 60 of patientsmost often due macroglossia and anatomical narrowing of theupper airways Central sleep apnea has been observed in a mi-nority of cases13
Arthropathy affects 75 of patients with acromegaly and isthe leading cause of morbidity and functional disability forthese patients14 Pain is the most common symptom usuallyexacerbated by activity Carpal tunnel syndrome is present inup to 64 of patients at presentation15 With disease progres-sion the bone undergoes accelerated turnover and the articularcartilage thins with narrowing of joint spaces similar to fea-tures of osteoarthiritis A recent meta-analysis observed ahigher bone formation but with a greater frequency of vertebralfractures compared with controls16
In recent years particular focus has been placed on colorec-tal cancer (CRC) to a lesser extent on breast prostate and thy-roid cancer rates in patients with acromegaly The pooled oddratios are increased for benign neoplasia (248 for colonic aden-omas and 3557 for hyperplastic polyps) in addition to coloncancer (204ndash4351)17 Orme et al investigated the incidence andmortality for cancer in a cohort of 1239 patients They excludedall malignancies pre-diagnosed to the diagnosis of acromegalyand used reliable national cancer registers for cross-examin-ation The overall cancer incidence was lower in the acromegalypatients than in the normal population (79 vs 109 malignanciesrespectively) However the SIRs revealed a small increase incolon cancers in acromegaly patients (SIR 168) and the deathrate from colon cancer outnumbered that recorded in the nor-mal population (13 observed deaths vs 5 expected) The occur-rence of cancer was unrelated to either disease duration or ageat diagnosis but the standard mortality rate associated withcancer was higher with post-treatment levels of GHgt10 lgl18
More recent results from the German Acromegaly Registry for446 patients (6656 person-years from diagnosis) did not showany evidence for a higher incidence of cancer (SIR 075 95CI055ndash10) most notably CRC or breast cancer19
Mortality
It is well reported in the literature that untreated acromegaly isassociated with reduced life expectancy Analysis of the deter-minants of mortality indicate that 60 die from cardiovascu-lar disease 25 from respiratory disease and 15 frommalignancies With advances in the medical therapy surgicaltechniques and localized stereotactic radiotherapy overall mor-tality rates in acromegaly have improved Although mortality inacromegalic patients remains elevated compared with the gen-eral population in several studies the mortality increase is gen-erally less than 2-fold compared with the 2- to 3-fold mortalityrates seen in earlier series20
There is compelling evidence to support that the last avail-able follow-up GH value is the most predictive survival indexBates et al21 reported that in a cohort of 79 patients with acro-megaly the Standardised Mortality ratio (SMR) fell from 26 to20 if treatment reduced GH levels to under 10 mUl (5 lgl) Even
more significant was the fact that mortality was reduced to nor-mal if post-treatment GH levels of lt5 mUl (25 lgl) wereachieved21 In the West Midlands Acromegaly Study compari-son of crude death rates per 1000 population suggested that aGH of 2 lgl may be a more appropriate treatment target with astep-up in the death rate once GH exceeded 2 lgl22 The FinnishNationwide Survey of Mortality in Acromegaly reported similarfindings In a cohort of 334 acromegalic patients with 56 deathsexcess mortality was seen in those with post-treatment GH lev-els gt25 lgl (SMR 163 (11ndash235) Plt 0001)23
In a recent meta-analysis Holdaway et al focused on the re-lationship between biochemical measurements and mortalityduring follow-up after treatment for acromegaly24 Mortalitywas close to the expected level when last available GH wasunder 25 lgl (SMR 11 95 CI 09ndash14) but was significantlyelevated in those with last available GH above 25 lgl (SMR 1995 CI 15ndash24)
Therefore the biochemical aim of treatment in acromegalyshould be reduction of GH values to lt25 lgl and possibly evenlower to lt1 lgl although care must be taken that this is not atthe expense of inducing GH deficiency and hypopituitarismwhich in itself is associated with an adverse outcome20
The introduction of GH antagonists as medical treatment foracromegaly necessitates the use of IGF-I in the biochemicalmonitoring of patients treated with these agents Holdaway et alfound that those with normal IGF-1 had mortality close to theexpected values for the general population (SMR 11 95 CI 09ndash14) whereas the SMR for those with elevated IGF-1 at last fol-low-up remained significantly increased (SMR 25 95 CI 16ndash40) However it should be noted that two of the largest studiesin the meta-analysis comprising a total of 151 deaths in 753 pa-tients have failed to demonstrate any relationship betweenpost-treatment IGF-1 levels and mortality(Relative Risk 12 95CI 071ndash202 Pfrac14 05 and RR 046 95 CI 017ndash126 Pfrac14 013) sug-gesting that last available serum IGF-I may not be as reliable amarker of mortality in acromegaly as last available GH
There are also methodological problems with using the lastavailable GHIGF-I in the analysis for mortality because thisvalue is inherently biased and does not take into account priorGHIGF-1 levels Many studies were also performed using olderassays that may not be used in clinical practice today howeverit may take many years to get meaningful data on survival usingnewer more sensitive assays and these older studies have to beinterpreted with this in mind
In the West Midlands study compared with the generalpopulation the use of external radiotherapy was associatedwith increased mortality with an SMR of 158 (95 CI 122ndash204Pfrac14 0005) and when assessed on internal analysis within theacromegaly cohort resulted in an RR of 167 (95 CI 11ndash256Pfrac14 002) In the Finnish survey mortality was also increased inpatients who had been treated with radiotherapy [SMR 169(95 CI 105ndash 258) Plt 0001] In the Spanish acromegaly regis-try patients who died had a twice greater probability of havingbeen treated with radiotherapy than those who had survived(hazard ratio 229 95 CI 103ndash508 Pfrac14 0026)
Although hypopituitarism is associated with increased mor-tality first identified by Rosen and Bengtsson25 there is littledata on the role of hypopituitarism in patients with acromegalyIn the West Midlands study there was a trend (Pfrac14 007) towardreduced survival in patients with acromegaly who had a greaternumber of deficient hypothalamo-pituitary axes compared withthose without evidence of hypopituitarism Sherlock et alshowed that neither TSH deficiency nor gonadotropin defi-ciency was associated with increased mortality in acromegaly
R Dineen et al | 413
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
on internal analysis (gonadotropin deficiency was associatedwith increased SMR compared with the general population)however adrenocorticotrophic hormone (ACTH) deficiency wasassociated with increased mortality [RR 17 (95 CI 12ndash25)Pfrac14 0004] The cause of death was predominantly cardiovascu-lar and higher doses of hydrocortisone therapy were associatedwith increased mortality20
Other variables found to influence outcome included hyper-tension duration of the disorder before treatment and ageHypertension and glucose intolerance are important contribu-tory factors to the vascular morbidity associated with acromeg-aly However there are few published reports on their impacton mortality in acromegaly and how this correlates with GHand IGF-I levels Hypertension is considered one of the mostrelevant negative prognostic factors for mortality inacromegaly
Diagnosis
The diagnosis of acromegaly is based upon a combination ofclinical examination and biochemical demonstration of dysre-gulated autonomous GH secretion as well as elevated IGF-1 lev-els Serum GH concentrations are typically elevated but levelsmay fluctuate widely Measuring serum IGF-1 in a patient withclinically suspected acromegaly should be the initial test26 It isalso recommended to test patients without the typical clinicalappearance but who have associated comorbidities sleepapnea type 2 diabetes disabling arthritis carpal tunnel syn-drome hyperhidrosis and hypertension A normal IGF-1 level(using age- and sex-matched reference ranges) effectively ex-cludes the diagnosis of acromegaly False positives may occur inpregnancy patients taking estrogen therapy and late-stage ado-lescence Multiple factors can make the biochemical interpret-ation of IGF-1 level challenging including the presence ofcertain pathological conditions such as hepatic and renal fail-ure malnutrition hypothyroidism and uncontrolledhyperglycemia
Failure of normal suppression of serum GH following astandard 75 g-oral glucose load remains the gold-standard diag-nostic test and should be used to confirm the diagnosis in allcases with high or equivocal IGF-1 or in the presence of condi-tions interfering with the measurement where clinical suspi-cion is high27
The use of higher sensitivity immunofluorometric chemilu-minescent and immunoradiometric assays has been associatedwith significantly lower nadir GH during oral glucose tolerancetest (OGTT) in healthy controls than was previously thought(ranging from 0029ndash025 mgl) with a gender difference notedin some studies 27
As ultrasensitive immunoassays are not uniformly availableworldwide current guidelines suggest a cutoff for nadir GH afterOGTTlt 1 lgl acceptable for exclusion of the diagnosis26 Itshould be highlighted that this could result in inaccurate exclu-sion of mild active disease A further challenge in diagnosis isthe presence of discordant serum GH and IGF-1 levels ElevatedIGF-1 with normal GH may reflect early disease and should war-rant further investigation (including imaging) to clarify thediagnosis28
Current guidelines recommend contrast-enhanced pituitaryMRI as the first line imaging modality after biochemical con-firmation of acromegaly If MRI is contraindicated or unavail-able then pituitary computed tomography should be performedAt diagnosis macroadenomas are detected in 73 of patients2
Visual field testing is recommended in all patients with con-firmed pituitary tumors As onset is often insidious patients maynot be aware of any alteration in their vision and a baseline as-sessment facilitates accurate interpretation of further testing if adeterioration is reported by the patient or in response to therapy
Assessment of the integrity of the other pituitary hormonesby the combination of basal and appropriate dynamic testing isrecommended Hyperprolactinemia from tumor co-secretionoccurs in up to a third of patients and can contribute to hypo-gonadism but may also occur a result of lsquostalk effectrsquo due totumor compression of the pituitary stalk interrupting the deliv-ery of inhibitory dopamine to the pituitary29 Evaluating all pa-tients with acromegaly for associated co-morbidities isrecommended at diagnosis (Table 2) in addition to longitudinalmonitoring during follow-up26
Treatment
Treatment goals in acromegaly include symptom relief tumorcontrol with maintenance of pituitary function biochemicalnormalization of GHIGF-1 and reversal of the excess morbidityand mortality associated with the disorder Current modalitiesof treatment available include surgery medical therapy andradiotherapy Treatment is complex and frequently more thanone modality is required to achieve treatment goals The deci-sion to treat and the therapeutic intervention used is based on anumber of factors which need to be weighed and tailored care-fully for each patient in a multidisciplinary setting
The definition of biochemical remission is difficult due tovariability in the assay and reference ranges used It is crucialthat the same GH and IGF-1 assay is maintained in the same pa-tient throughout their management While it remains contro-versial the current recommended biochemical target is arandom GHlt 1 lgl26 The decline in IGF-1 is more delayed com-pared with GH likely due to differential half-life of IGF-bindingproteins IGF-1 levels measured at 12 weeks after surgery are avalid reflection of surgical remission If the IGF-1 level hasdeclined but is still not normal measurement of a repeat IGF-1level is warranted due to variability in the IGF-1 assay
A normal IGF-1 value and undetectable GH value are suffi-cient for indicating surgical remission However if the GH is de-tectable (ie gt04 lgL) measurement of GH after a glucose loadmay yield important information The mean value of severalsamples taken a few hours apart throughout the day can also beused (GH day curve (GHDC)) as it is significantly correlated withthe GH nadir during OGTT and with the IGF-1 level30 While theideal endocrine outcome of any therapy in acromegaly is a nor-mal IGF-1 value and undetectable GH value levels that are asso-ciated with a normalization of mortality (as discussed in thesection above relating to mortality) are acceptable
Surgery
Transphenoidal surgery by an experienced pituitary surgeon isthe initial treatment of choice recommended for the majority ofpatients26 Ninety percent of patients who undergo pituitary sur-gery are treated using the transphenoidal approach craniotomy israrely performed The development of endoscopic and microsurgi-cal transphenoidal surgery offers further advantages over the con-ventional techniques including the possibility of superior tumorclearance in previously difficult to access areas less surgical mor-bidity fewer complications and reduced postoperative pain31
The main postoperative complaints relate to the transphe-noidal approach including nasal congestion sinusitis and
414 | QJM An International Journal of Medicine 2017 Vol 110 No 7
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
epistaxis More serious complications include hemorrhage CSFleakage and risk of meningitis stroke visual impairment vas-cular injury transient diabetes insipidus (DI) (typically occur-ring as a result of intraoperative manipulation of the pituitarystalk) and hypopituitarism32 Despite significant co-morbiditiesin patients with acromegaly surgical mortality rates of lt05can be anticipated33
Several factors are associated with reduced surgical successrates including large tumor size extrasellar extension andhigher preoperative GH levels34 Recurrence rates peak in years1ndash5 postoperatively with reported recurrence rates of up to 8with recurrence rates being lower in microadenomas comparedwith macroadenomas35 A normal IGF value and undetectableGH value are sufficient for indicating surgical remission
The Acromegaly group consensus guidelines suggest that ina patient with persistent disease after surgery repeat surgerymay be an option if the tumor is accessible26 The decision toinitiate somatostatin therapy prior surgery remains controver-sial In a prospective study of 30 patients with newly diagnosedacromegaly reductions in GH and IGF-1 concentrations andtumor volume were observed following 24 weeks of preopera-tive lanreotide autogel therapy36 Further studies do not reportany difference in the long-term results37 Due to the lack ofrandomized controlled studies the Acromegaly group consen-sus recommend against the routine use of preoperative somato-statin therapy In certain circumstances particularly forpatients with severe soft tissue growth complicating anestheticrisk or with significant comorbidities that may be improved bypreoperative therapy pretreatment with somatostatin receptorligands (SRL) may be considered38
Surgical debulking may be considered in patients with lowpredictive surgical cure rate at diagnosis to improve the chanceof achieving target GHIGF-1 levels with subsequent medicaltherapy Pretreatment disease burden is inversely correlatedto somatostatin analogue responsiveness39 In addition tobiochemical testing of remission as outlined above a contrast-enhanced MRI is recommended at least 12 weeks postopera-tively to visualize residual tumor This provides a baseline forfuture surveillance Formal visual field testing should also beperformed for patients with pre-operative visual deficits
Successful surgery by an experience neurosurgeon in a spe-cialized pituitary center can result in immediate biochemical
remission elimination of direct mass effects in addition to pro-viding tissue for immunohistochemical analysis Hence surgeryremains the primary therapeutic intervention in most patientswith acromegaly26
Medical treatment
Medical therapy has an important role as an adjunctive treat-ment option for persistent disease following non-curative sur-gery and also as first line therapy where surgery is not a feasibletherapeutic option Consensus guidelines outline the recom-mended role of medical therapy in the treatment of patientswith acromegaly There are a number of options for medicaltherapy in acromegaly including somatostatin receptor ligandsGH receptor antagonists and dopamine agonists
Somatostatin receptor ligands
Somatostatin is distributed throughout the nervous system andexerts neural control over many physiological functions includ-ing the inhibition of GH release It exists in two biologically ac-tive molecular forms somatostatin-14 and somatostatin -28with a short half-life of 2-3 min Its action is mediated throughG-protein coupled cell-surface receptors identified in a varietyof tissues including the pituitary Both bioactive forms havehigh binding affinity toward all five identified receptor sub-types SSR1-SSR540 GH-secreting pituitary adenomas expresspredominantly SSR2 and SSR5 First generation somatostatinanalogs octreotide and lanreotide show high affinity binding toSSR2 and to a lesser extent to SSR541
Currently three long-acting SRL formulations are availableoctreotide LAR Lanreotide depotautogel and pasireotide Rapidacting subcutaneous octreotide is also available and is adminis-tered two-three times daily The long-acting octreotide LAR isadministered intramuscularly every 4ndash6 weeks The approvedstarting octreotide LAR dose is 20 mg monthly with dose titra-tion every 3ndash6 months to a maximum dose of 40 mg monthlyLanreotide is available in a microsphere formulation (depot) in-jected intramuscularly every 7ndash14 days and an aqueous solution(Autogel) administered by deep subcutaneous injection every 4ndash6 weeks For lanreotide autogeldepot the approved starting
Table 2 Assessment of acromegaly complications at diagnosis and during long-term monitoring
At diagnosis During long-term follow-up
BP measurement Every 6 months or when change of treatment (if hypertensive)Echocardiography AnnuallyECG AnnuallyEpworth scale or sleep study AnnuallyECHO Doppler of peripheral arterial and venous
systemAnnually particularly in gigantism
OGTT Fasting blood glucose every 6 months (particularly in uncontrolled disease andduring SRL therapy) HbA1c every 6 months if diabetes present
Total testosterone SHBG and prolactin (males) Annually (free testosterone when doubts in interpretation of total testosterone)LH FSH17b-estradiol and prolactin (females) AnnuallyAcroQol AnnuallyDEXA Every 2 years if patient with osteopeniaosteoporosisThoracic and lumbar spine Xray Every 2ndash3 years if osteoporosis risk factors kyphosis or symptomsColonoscopy Every 10 years (more frequently if IGF-1 remains persistently elevated or if abnormal
colonoscopy or family history of chronic cancer)Genetic screening for markers of familial acromeg-
aly (if suspicion)
R Dineen et al | 415
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
dose is 90 mg monthly with a maximum dose up to 120 mgmonthly26
A large body of evidence supports the efficacy of long -actingSRL therapy In a critical analysis of the largest studies octreo-tide LAR reduced GH tolt25 lgl and normalized the IGF-1 levelsin 66 and 63 respectively42 Similar targets were achievedwith lanreotide-SR in 52 and 47 of cases respectively An ear-lier meta-analysis by Freda et al43 reported the overall chance ofIGF-1 normalization was 67 with octreotide and 47 with lan-reotide SR The higher efficacy reported with octreotide may beaccounted by pre-selection of responsive cases (patients whoshowed response to short acting octreotide only being recruitedto studies) inclusion of both primary and secondary therapycases and small case series An inherent challenge to meta-analyses in such a complex condition is the lack of standardiza-tion of GH and IGF-1 assays making comparison of absolutevalues between studies impossible
Smaller tumors lower baseline GH and IGF-1 levels44 highSSR2 and SSR5 expression45 and those previously treated withsurgery are associated with a better response to SRL treatmentRoutine performance of somatostatin receptor scintigraphy oran acute GH response to a subcutaneous octreotide injection asa determinant of SRL response are not recommended26
Somatostatin receptor ligands also have proven efficacy intumor volume reduction This has been extensively reviewedrecently by Colao et al46 Tumor reduction may be mediated bydirect anti-proliferative effects via activation of somatostatinreceptors or indirectly through angiogenesis inhibitionSathyapalan et al47 showed a significant reduction in the func-tional vascularity of pituitary tumors in a small study of five pa-tients after 24 weeks of octreotide therapy
Published meta-analysis revealed that octreotide LAR andlanreotide formulation induce tumor shrinkage in 660 and328 of cases respectively4849 Tumor reduction is progressivewith prolonged treatment and decreased IGF-1 levels may beits best predictor followed by age and degree of GH decrease
A recent detailed review of published studies evaluatingsomatostatin analogues as first line therapy showed that 6-24months of octreotide LAR therapy achievedgt20-30 tumor vol-ume reduction in 73-85 of patients Unlike surgery primarymedical therapy cannot cure acromegaly Based on a recentmeta-analysis of available studies primary SRL therapy is asso-ciated with a lower remission rates compared to initial surgery(45 vs 67)49 However the accuracy of these remission ratesis questionable given the non-comparable nature and the het-erogeneity of studies included Primary SRL therapy can beoffered before surgery in patients with contraindications incases with unresectable tumor or with severe comorbidities26
During SRL treatment the most frequent side effects includeabdominal discomfort flatulence cramps and diarrheaGallbladder sludge or gallstones occur in 25 of subjects butare usually asymptomatic SRL treatment was initially thoughtto aggravate the increased risk of glucose intolerance in thesepatients but the overall effect on glucose metabolism is not clin-ically significant50
Pasireotide is a multireceptor-targeted somatostatin recep-tor ligand which has higher functional activity than octreotideon SSR subtypes except type 4 but in particular SSR551 In alarge phase III randomized trial in patients with acromegalywho were naive to medical therapy pasireotide LAR and octreo-tide LAR have a similar effect of tumor reduction despite thefact that pasireotide was superior to octreotide in providing bio-chemical control After 12 months of treatment 81 of pasireo-tide patients had20 reduction in tumor volume compared
with 77 of octreotide LAR patients52 Pasireotide has similarrates of gastrointestinal side effects to other SRLs however therates of hyperglycemia are significantly higher (occurring in 31ndash57 of patients)
Pegvisomant
Pegvisomant is a pegylated recombinant analog of human GHincorporating nine amino acid mutations Pegylation extendsthe half-life by reducing renal clearance53 The mutations resultin increased affinity to the GH receptor in addition to blockingthe second binding site on the receptor preventing GHR dimer-ization and signal transduction GH hypersecretion persists asit does not target the GH secreting tumor at the level of the pitu-itary hence GH measurements cannot be used to monitor dis-ease activity and IGF-1 becomes the sole marker to monitorbiochemical response during therapy
Pegvisomant has been shown to be highly effective in pro-viding biochemical control of acromegaly in multiple studies Ina 12-week double-blind placebo controlled study Trainer et al54
randomly assigned patients to receive placebo 10 15 or 20 mgof pegvisomant Normalization of IGF-1 (using age and sex-matched reference ranges) was achieved in 10 54 81 and89 respectively Symptom control was also observed The effi-cacy of pegvisomant over a longer period was subsequentlystudied Van der Lely et al55 reported 97 of patients achievingnormal IGF-1 levels in patients receiving therapy for 12 monthsor more (Figure 1) Dose reduction was required in 1190 pa-tients as IGF-1 levels dropped below normal reference range forage and sex
As mentioned above pegvisomant does not exert a centraleffect on pituitary GH secretion hence fears exist over the pos-sibility of increased tumor growth The German PegvisomantObservational Study is a multicenter surveillance study com-menced in 2004 to assess the efficacy and safety of pegvisomanttherapy in patients with acromegaly56 Neuroradiological moni-toring of tumor extension is performed with MRI imagingBuchfelder et al studied 3 years of follow-up data of 307 pa-tients Tumor progression was reported in between 2 and3 ofpatients treated an increase not outside the expected rate inpatients not treated with pegvisomant
Pegvisomant is administered as daily subcutaneous injec-tion It is generally well tolerated with adverse effects reportedinlt10 of patients These may include injection site reactionswith reversible lipohypertrophy and deranged liver functiontests (attributable to the polyethylene glycol pegylated vehicle)
The predominant limiting factor for use of this agent in clin-ical practice remains its considerable cost It is most often usedas a second line agent in cases resistant or intolerant to SRLtherapy or in combination with SRLrsquos in partially resistantcases It is also a potential treatment option in acromegaly pa-tients with difficult to control diabetes mellitus due to its favor-able effect on glycemic control
Dopamine agonists
Dopamine agonists bind to the D2 dopamine receptors in the pi-tuitary gland and suppress prolactin and GH secretion The useof bromocriptine a first-generation dopamine agonist is lim-ited by its side effect profile including GI symptoms lethargyand orthostatic hypotension It also compares poorly with som-atostatin receptor ligands in terms of efficacy with normaliza-tion of GHIGF-1 reported in only 10 of patients57
416 | QJM An International Journal of Medicine 2017 Vol 110 No 7
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
Cabergoline an ergot derivative dopamine agonist has beenused for decades in the treatment of hyperprolactinaemia andParkinsonrsquos disease Cabergoline is better tolerated and more ef-fective than bromocriptine however its use was superseded bythe development of SRL therapy showing higher efficacy rates
Clinical trials of cabergoline in acromegaly are small non-randomized and report variable results In a recent systematicreview of 10 trials with a total of 150 acromegaly patients con-trol of acromegaly was achieved in 34 of patients who receivedcabergoline therapy alone and 52 when added to SRL therapyin patients with suboptimal control58 Consequently currentguidelines recommend the use of cabergoline in patients withinadequate response to other medical treatment with highestbenefit expected in cases with modest persistent hormonal ele-vations26 Conflicting data exists as to whether the co-secretionof prolactin is predictive of response to dopamine agonist ther-apy Some studies conclude that tumors that co-secrete prolac-tin and GH have a greater response to dopamine agonisttherapy than those than solely secrete GH whereas othersshow no effect There remains little data available regardingtumor shrinkage in patients with acromegaly who are receivingdopamine agonist therapy59 Jaffe et al57 reported combined re-sults from a number of studies which revealed that 29 of pa-tients had some tumor shrinkage on dopamine agonist therapyand the majority of patients who had tumor shrinkage werealso hyperprolactinemic It is difficult to interpret these findinggiven the small number and heterogeneous characteristics ofthe patients included
The most frequent adverse effects of dopamine agonist ther-apy are nausea constipation headache mood disturbancenasal stuffiness and dizziness Cardiac valve abnormalitieswere described with high doses of cabergoline used inParkinsonrsquos disease but not with current recommended dosageused for patients with acromegaly60
DopastatinBIM-23A760 is a chimeric molecule hasbeen shown in vitro to have high affinity for both somatosta-tin receptor subtypes- 2 and 5 in addition to dopamine 2 recep-tor61 With increasing knowledge of the importance of SSR5 inregulation of GH in GH-secreting adenomas dopastatin isundergoing further development in clinical studies to deter-mine if there is a role for these compounds in the treatment ofacromegaly
Radiotherapy
Radiation therapy is used as adjuvant treatment in the settingof persistent disease despite surgery andor medical treatmentor if medical therapy is unavailable unsuccessful or not toler-ated Radiotherapy has been shown to be effective in loweringserum GH levels36 but conflicting results have been reported re-garding the normalization of IGF-1 levels62 Furthermore thedelay in therapeutic benefit and the high risk of developinghypopituitarism serve as arguments against the more routineuse of radiotherapy
Conventional radiotherapy has been used for gt30 years inthe adjunctive treatment of pituitary adenomas It is generallydelivered in fractionated doses 4ndash5 times per week so as to re-duce daily-fractionated dose The risk of adverse effects beingproportional to maximal dose per day63 Early studies of con-ventional radiotherapy reported high efficacy rate of 80ndash100however remission was defined as a GH level below 5-10 ngmlMore recent studies using revised biochemical remission tar-gets report a mean remission rate between 50 and 60 Jenkinset al64 assessed the effects of conventional pituitary irradiationin 884 patients of the UK National Acromegaly Register MeanGH levels declined from 135 to 53 ngml at 2 years after surgeryto 2 ngml by 10 years and a further decline to 11 ngml at 20years (Figure 2) Furthermore they observed a parallel fall in IGF-
Figure 1 Baseline and lowest values of individual serum insulin-like growth factor-1 concentrations achieved in 90 patients treated for 12 months or more with daily
pegvisomant (daggerPlt005 vs baseline DaggerPlt001 vs baseline) The shaded area represents the age-adjusted normal range for insulin-like growth factor-155
R Dineen et al | 417
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
1 levels with 63 of patients having a normal level by 10years64
Stereotactic radiotherapy offers improvement in immobil-ization imaging and treatment delivery from conventionaltechniques It can be delivered as a single fraction radiosurgeryusing a Gamma knife (a source of cobalt) or a linear acceleratoror a stereotactic conformal radiotherapy delivered as fractio-nated treatment using a linear accelerator There is no clear ad-vantage for either of the radiosurgical techniques in terms ofsparing normal tissue receiving high doses of radiation65 A crit-ical analysis of the literature reported variable rates of both bio-chemical and tumor response 17ndash82 and 37ndash100respectively66 The authors attributed the wide variability to theuse of different treatment schedules and definitions ofremission
Hypopituitarism is less frequent with radiosurgery than con-ventional radiotherapy At least 50 of patient treated with con-ventional radiotherapy will have acquired new anteriorpituitary hormonal deficits at 10 years67 In cohorts treatedsolely with stereotactic techniques rates of hypopituitarismvary between 0 and 2068 However it is likely that the candi-dates for stereotactic radiotherapy had smaller remnants of dis-ease and therefore less normal tissue irradiated
Annual hormonal testing is required due to the risk of latehypopituitarism26 Other complications following radiotherapyinclude the risk of second brain tumors stroke and rarely opticneuropathy cranial nerve deficits and radionecrosis a rare ad-verse effect of gamma knife radiotherapy69ndash71
Patients treated with conventional radiotherapy have beenreported to have increased mortality predominantly due tostroke independent of GHIGF-I levels and hypopituitarism20
Current guidelines recommend the use of stereotactic radio-therapy over conventional radiation therapy unless significantresidual tumor burden or the lesion is too close to the opticchiasm26
Conclusion
Prolonged exposure to elevated endogenous levels of GH andIGF-I results in a multisystem disease characterized by somaticovergrowth multiple co-morbidities and premature mortalityEarly detection prevents the development of irreversible com-plications of the disease including cardiomyopathy respiratory
dysfunction and arthropathy Despite the imprecision of assaysfor GH and IGF-I it is clear from epidemiologic studies that tightbiochemical control is essential to reduce morbidity controlsymptoms and improve mortality rates
Optimal implementation of current guidelines in routine clin-ical practice and maximal use of the medical treatment could im-prove the long-term control of patients with significant benefitsfor morbidity and mortality Another important aspect in thetreatment of patients with acromegaly is also the appropriate tar-geted treatment of co-morbidities associated with acromegaly
Achievement of the criteria for cure during or after therapyis determined by assessing biochemical control targeting con-trolled levels of GH and normalization of IGF-I levels monitor-ing tumor size assessing residual pituitary function andmonitoring co-morbidities
New therapeutic molecules currently in trials will hopefullyoffer further benefit to those patients resistant to current thera-peutic modes for this chronic progressive disorder
Conflict of interest None declared
References1 Melmed S Braunstein GD Horvath E Ezrin C Kovacs K
Pathophysiology of acromegaly Endocr Rev 1983 4271ndash902 Mestron A Webb SM Astorga R Benito P Catala M
Gaztambide S et al Epidemiology clinical characteristicsoutcome morbidity and mortality in acromegaly based onthe Spanish Acromegaly Registry (Registro Espanol deAcromegalia REA) Eur J Endocrinol 2004 151439ndash46
3 Jagannathan J Dumont AS Prevedello DM Oskouian RJLopes B Jane JA Jr and Laws ER Jr Genetics of pituitary aden-omas current theories and future implications NeurosurgFocus 2005 19E4
4 Zhu X Lin CR Prefontaine CG Tollkuhn J Rosenfeld MGGenetic control of pituitary developement and hypopituitar-ism Curr Opin Genet Dev 2005 15332ndash40
5 Melmed S Acromegaly pathogenesis and treatment J ClinInvest 2009 1193189ndash202
6 Colao A Ferone D Marzullo P Lombardi G Systemic compli-cations of acromegaly epidemiology pathogenesis andmanagement Endocr Rev 2004 25102ndash52
7 Korbonits M Gadelha MR Roncaroli F Grossman AB Ellard SEvanson J et al Landscape of familial isolated and young-onset pituitary adenomas prospective diagnosis in AIP mu-tation carriers J Clin Endocrinol Metab 2015 100E1242ndash54
8 Larkin S Reddy R Karavitaki N Cudlip S Wass J Ansorge OGranulation pattern but not GSP or GHR mutation is associ-ated with clinical characteristics in somatostatin-naive pa-tients with somatotroph adenomas Eur J Endocrinol 2013168491ndash9
9 Molitch ME Clinical manifestations of acromegaly EndocrinolMetab Clin North Am 1992 21597ndash614
10Reid TJ Post KD Bruce JN Nabi KM Reyes-Vidal CM et alFeatures at diagnosis of 324 patients with acromegaly didnot change from 1981 to 2006 acromegaly remains under-recognized and under-diagnosed Clin Endocrinol 201072203ndash8
11Moslashller N Joslashrgensen JO Abildgard N Orskov L Schmitz OChristiansen JS Effects of growth hormone on glucose me-tabolism Horm Res 1991 36 (Suppl 1)32ndash5
12Dreval AV Trigolosova IV Misnikova IV Kovalyova YATishenina RS Barsukov IA et al Prevalence of diabetes melli-tus in patients with acromegaly Endocr Connect 2014 393ndash8
Figure 2 Percentage of all patients achieving a serum GH level lt25 ngml (bars)
and the mean GH level (line) in the years after pituitary irradiation64
418 | QJM An International Journal of Medicine 2017 Vol 110 No 7
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
13Roemmler J Gutt B Fischer R Vay S Wiesmeth ABidlingmaier M et al Elevated incidence of sleep apnoea inacromegaly-correlation to disease activity Sleep Breath 2012161247ndash53
14Killinger Z Payer J Lazurova I Imrich R Homerova Z KuzmaM et al Arthropathy in acromegaly Rheum Dis Clin North Am2010 36713ndash20
15Kameyama S Tanaka R Hasegawa A Tamura T Kuroki MSubclinical carpal tunnel syndrome in acromegaly NeurolMed Chir 1993 33547ndash51
16Mazziotti G Biagioli E Maffezzoni F Spinello M Serra VMaroldi R et al Bone turnover bone mineral density and frac-ture risk in acromegaly a meta-analysis J Clin EndocrinolMetab 2015 100384ndash94
17Renehan AG OrsquoConnell J OrsquoHalloran D Shanahan F PottenCS OrsquoDwyer ST et al Acromegaly and colorectal cancer acomprehensive review of epidemiology biological mechan-isms and clinical implications Horm Metab Res 200335712ndash25
18Orme S McNally RJ Cartwright RA Belchetz PE Mortality andcancer incidence in acromegaly a restrospective cohortstudy J Clin Endocrinol Metab 1998 832730ndash4
19Petroff D Teuroonjes A Grussendorf M Droste M Dimopoulou CStalla G et al The Incidence of cancer among acromegaly pa-tients results from the German Acromegaly Registry J ClinEndocrinol Metab 2015 1003894ndash902
20Sherlock M Ayuk J Tomlinson JW Toogood AA Aragon-Alonso A Sheppard MC et al Mortality in patients with pitu-itary disease Endocr Rev 2010 31301ndash42
21Bates AS Vanrsquot H Jones JM Clayton RN An audit of outcomeof treatment in acromegaly Q J Med 1993 86293ndash9
22Ayuk J Clayton RN Holder G Sheppard MC Stewart PMBates AS Growth hormone and pituitary radiotherapy butnot serum insulin-like growth factor-I concentrations pre-dict excess mortality in patients with acromegaly J ClinEndocrinol Metab 2004 891613ndash7
23Kauppinen-Meuroakelin R Sane T Reunanen A Veuroalimeuroaki MJNiskanen L Markkanen H et al A nationwide survey of mor-tality in acromegaly J Clin Endocrinol Metab 2005 904081ndash6
24Holdaway IM Bolland MJ Gamble GD A meta-analysis of theeffect of lowering serum levels of GH and IGF-I on mortalityin acromegaly Eur J Endocrinol 2008 15989ndash95
25Rosen T Bengtsson BA Premature mortality due to cardio-vascular disease in hypopituitarism Lancet 1990 336285ndash8
26Katznelson L Laws ER Jr Melmed S Molitch ME Murad MHUtz A et al Acromegaly an endocrine society clinical practiceguideline J Clin Endocrinol Metab 2014 993933ndash51
27Freda PU Post KD Powell JS Wardlaw SL Evaluation of dis-ease status with sensitive measures of growth hormone se-cretion in 60 postoperative patients with acromegaly J ClinEndocrinol Metab 1998 833808ndash16
28Dimaraki EV Jaffe CA DeMott-Friberg R Chandler WFBarkan AL Acromegaly with apparently normal GH secretionimplications for diagnosis and follow-up J Clin EndocrinolMetab 2002 873537ndash42
29Losa M Von Werder K Pathophysiology and clinical aspectsof the ectopic GH-releasing hormone syndrome ClinEndocrinol 1997 47123ndash35
30Dobrashian RD OrsquoHalloran DJ Hunt A Beardwell CG ShaletSM Relationships between insulin-like growth factor-1 levelsand growth hormone concentrations during diurnal profilesand following oral glucose in acromegaly Clin Endocrinol 199338589ndash93
31Frank G Pasquini E Farneti G Mazzatenta D Sciarretta VGrasso V et al The endoscopic versus the traditional ap-proach in pituitary surgery Neuroendocrinology 2006 83240ndash8
32Marquez Y Tuchman A Zada G Surgery and radiosurgery foracromegaly a review of indications operative techniquesoutcomes and complications Int J Endocrinol 2012 2012386ndash401
33Laws ER Vance ML Thapar K Pituitary surgery for the man-agement of acromegaly Horm Res 2000 5371ndash5
34Salaun C Foubert L Vialatou M Kujas M Turpin G Prognosticfactors of surgical cure of growth hormone secreting pituitary aden-omas Ann Medecine Interne 1999 150195ndash8
35Kreutzer J Vance ML Lopes MB Laws ER Jr Surgical manage-ment of GH-secreting pituitary adenomas an outcome studyusing modern remission criteria J Clin Endocrinol Metab 2001864072ndash7
36Annamalai AK Webb A Kandasamy N Elkhawad M Moir SKhan F et al A comprehensive study of clinical biochemicalradiological vascular cardiac and sleep parameters in anunselected cohort of patients with acromegaly undergoingpresurgical somatostatin receptor ligand therapy J ClinEndocrinol Metab 2013 981040ndash50
37Shen M Shou X Wang Y Zhang Z Wu J Mao Y et al Effect ofpresurgical long-acting octreotide treatment in acromegalypatients with invasive pituitary macroadenomas a prospect-ive randomized study Endocr J 2010 571035ndash44
38Friedel ME Johnston D Singhal S Al Khalili K Farrell CJEvans JJ et al Airway management and perioperative con-cerns in acromegaly patients undergoing endoscopic trans-sphenoidal surgery for pituitary tumors Otolaryngol HeadNeck Surg 2013 149840ndash4
39Bhayana S Booth G Asa SL Kovacs Ezzat S The implicationof somatotroph adenoma phenotype to somatostatin analogresponsiveness in acromegaly J Clin Endocrinol Metab 2005906290ndash5
40Reisine T Bell GI Molecular biology of somatostatin recep-tors Endocr Rev 1995 16427ndash42
41Zatelli MC Piccin D Tagliati F et al Dopamine receptor sub-type 2 and somatostatin receptor subtype 5 expression influ-ences somatostatin analog effects on human somatotrophpituitary adenomas in vitro J Mol Endocrinol 2005 35333ndash41
42Murray RD Melmed S A critical analysis of clinically avail-able somatostatin analog formulations for therapy of acro-megaly J Clin Endocrinol Metab 2008 932957ndash68
43Freda PU Katznelson L Van der Lely A Reyes CM Zhao SRabinowitz D Long-acting somatostatin analog therapy ofacromegaly a meta-analysis J Clin Endocrinol Metab 2005904465ndash74
44Howlett TA Willis D Walker G Wass JA Trainer PJ Control ofgrowth hormone and IGF1 in patients with acromegaly in theUK responses to medical treatment with somatostatin ana-logues and dopamine agonists Clin Endocrinol 201379689ndash99
45Espinosa de los Monteros AL Carrasco C Albarran AAGadelha M Abreu A Mercado M The role of primary pharma-cological therapy in acromegaly Pituitary 2014 17 (Suppl1)S4ndashS10
46Colao AM Auriemma RS Pivonello R The effects of somato-statin analogue therapy on pituitary tumor volume in pa-tients with acromegaly Pituitary 2016 19210ndash21
47Sathyapalan T Lowry M Turnbull LW Rowland-Hill C AtkinSL Mechanism of action of octreotide in acromegalic tu-mours in vivo using dynamic contrast-enhanced magneticresonance imaging Pituitary 2007 10233ndash6
R Dineen et al | 419
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
48Giustina A Mazziotti G Torri V Spinello M Floriani IMelmed S Meta-analysis on the effects of octreotide ontumor mass in acromegaly PLoS One 2012 7e36411
49Abu Dabrh AM Mohammed K Asi N Farah WH Wang ZFarah MH et al Surgical interventions and medical treat-ments in treatment-naive patients with acromegaly system-atic review and meta-analysis J Clin Endocrinol Metab 2014994003ndash14
50Colao A Bronstein M Freda P Gu F Shen C-C Gadelha Met al Pasireotide versus octreotide in acromegaly a head-to-head superiority study J Clin Endocrinol Metab 2014 99791ndash9
51Schmid HA Schoeffter P Functional activity of the multili-gand analog SOM230 at human recombinant somatostatinreceptor subtypes supports its usefulness in neuroendocrinetumors Neuroendocrinology 2004 80 (Suppl 1)47ndash50
52Mazziotti G Floriani I Bonadonna S Torri V Chanson PGiustina A Effects of somatostatin analogs on glucosehomeostasis a metaanalysis of acromegaly studies J ClinEndocrinol Metab 2009 941500ndash8
53Higham CE Trainer PJ Growth hormone excess and the de-velopment of growth hormone receptor antagonists ExpPhysiol 2008 931157ndash69
54Trainer PJ Drake WM Katznelson L et al Treatment of acro-megaly with the growth hormone receptor antagonist pegvi-somant N Engl J Med 2000 3421171ndash7
55Van der Lely AJ Hutson RK Trainer PJ Besser GM Barkan ALKatznelson L et al Long-term treatment of acromegaly withpegvisomant a growth hormone receptor antagonist Lancet2001 3581754ndash9
56Buchfelder M Weigel D Droste M Mann K Saller B BrubachK et al Pituitary tumor size in acromegaly during pegvisom-ant treatment experience from MR re-evaluations of theGerman Pegvisomant Observational Study Eur J Endocrinol2009 16127ndash35
57 Jaffe CA Barkan AL Treatment of acromegaly with dopamineagonists Endocrinol Metab Clin North Am 1992 21713ndash35
58Sandret L Maison P Chanson P Place of cabergoline in acro-megaly a meta-analysis J Clin Endocrinol Metab 2011961327ndash35
59Sherlock M Woods C Sheppard C Medical therapy in acro-megaly Nat Rev Endocrinol 2011 7291ndash300
60Samson SL Ezzat S AACEACE disease state clinical reviewdopamine agonists for hyperprolactinemia and the risk ofcardiac valve disease Endocr Pract 2014 20608ndash16
61 Jaquet P Gunz G Saveanu A Dufour H Taylor J Dong J et alEfficacy of chimeric molecules directed towards multiplesomatostatin and dopamine receptors on inhibition of GHand prolactin secretion from GH-secreting pituitary aden-omas classified as partially responsive to somatostatin ana-log therapy Eur J Endocrinol 2005 153135ndash41
62Barkan AL Halasz I Dornfeld KJ Jaffe CA Friberg RDChandler WF et al Pituitary irradiation is ineffective in nor-malizing plasma insulin-like growth factor I in patients withacromegaly J Clin Endocrinol Metab 1997 823187ndash91
63Eastman RC Gorden P Glatstein E Roth J Radiation therapyof acromegaly Endocrinol Metab Clin North Am 199221693ndash712
64 Jenkins PJ Bates Carson MN Stewart PM Wass JAConventional pituitary irradiation is effective in loweringserum growth hormone and insulin-like growth factor-I inpatients with acromegaly J Clin Endocrinol Metab 2006911239ndash45
65Minniti G Gilbert DC Brada M Modern techniques for pituit-ary radiotherapy Rev Endocr Metab Disord 2008 10135ndash44
66Stapleton CJ Liu CY Weiss M The role of stereotactic radio-surgery in the multimodal management of growth hormone-secreting pituitary adenomas Neurosurg Focus 2010 29E11
67Biermasz NR van Dulken H Roelfsema F Long-term follow-up results of postoperative radiotherapy in 36 patients withacromegaly J Clin Endocrinol Metab 2000 852475ndash82
68Attanasio R Epaminonda P Motti E Giugni E Ventrella LCozzi R et al Gamma-knife radiosurgery in acromegaly a 4-year follow-up study J Clin Endocrinol Metab 2003 883105ndash12
69Minniti G Traish D Ashley S Gonsalves A Brada M Risk ofsecond brain tumor after conservative surgery and radiother-apy for pituitary adenoma update after an additional 10years J Clin Endocrinol Metab 2005 90800ndash4
70Brada M Burchell L Ashley S Traish D The incidence of cere-brovascular accidents in patients with pituitary adenoma IntJ Radiat Oncol Biol Phys 1999 45693ndash8
71Laws ER Sheehan JP Sheehan JM Jagnathan J Jane JA JrOskouian R Stereotactic radiosurgery for pituitary aden-omas a review of the literature J Neurooncol 2004 69257ndash72
420 | QJM An International Journal of Medicine 2017 Vol 110 No 7
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022

on internal analysis (gonadotropin deficiency was associatedwith increased SMR compared with the general population)however adrenocorticotrophic hormone (ACTH) deficiency wasassociated with increased mortality [RR 17 (95 CI 12ndash25)Pfrac14 0004] The cause of death was predominantly cardiovascu-lar and higher doses of hydrocortisone therapy were associatedwith increased mortality20
Other variables found to influence outcome included hyper-tension duration of the disorder before treatment and ageHypertension and glucose intolerance are important contribu-tory factors to the vascular morbidity associated with acromeg-aly However there are few published reports on their impacton mortality in acromegaly and how this correlates with GHand IGF-I levels Hypertension is considered one of the mostrelevant negative prognostic factors for mortality inacromegaly
Diagnosis
The diagnosis of acromegaly is based upon a combination ofclinical examination and biochemical demonstration of dysre-gulated autonomous GH secretion as well as elevated IGF-1 lev-els Serum GH concentrations are typically elevated but levelsmay fluctuate widely Measuring serum IGF-1 in a patient withclinically suspected acromegaly should be the initial test26 It isalso recommended to test patients without the typical clinicalappearance but who have associated comorbidities sleepapnea type 2 diabetes disabling arthritis carpal tunnel syn-drome hyperhidrosis and hypertension A normal IGF-1 level(using age- and sex-matched reference ranges) effectively ex-cludes the diagnosis of acromegaly False positives may occur inpregnancy patients taking estrogen therapy and late-stage ado-lescence Multiple factors can make the biochemical interpret-ation of IGF-1 level challenging including the presence ofcertain pathological conditions such as hepatic and renal fail-ure malnutrition hypothyroidism and uncontrolledhyperglycemia
Failure of normal suppression of serum GH following astandard 75 g-oral glucose load remains the gold-standard diag-nostic test and should be used to confirm the diagnosis in allcases with high or equivocal IGF-1 or in the presence of condi-tions interfering with the measurement where clinical suspi-cion is high27
The use of higher sensitivity immunofluorometric chemilu-minescent and immunoradiometric assays has been associatedwith significantly lower nadir GH during oral glucose tolerancetest (OGTT) in healthy controls than was previously thought(ranging from 0029ndash025 mgl) with a gender difference notedin some studies 27
As ultrasensitive immunoassays are not uniformly availableworldwide current guidelines suggest a cutoff for nadir GH afterOGTTlt 1 lgl acceptable for exclusion of the diagnosis26 Itshould be highlighted that this could result in inaccurate exclu-sion of mild active disease A further challenge in diagnosis isthe presence of discordant serum GH and IGF-1 levels ElevatedIGF-1 with normal GH may reflect early disease and should war-rant further investigation (including imaging) to clarify thediagnosis28
Current guidelines recommend contrast-enhanced pituitaryMRI as the first line imaging modality after biochemical con-firmation of acromegaly If MRI is contraindicated or unavail-able then pituitary computed tomography should be performedAt diagnosis macroadenomas are detected in 73 of patients2
Visual field testing is recommended in all patients with con-firmed pituitary tumors As onset is often insidious patients maynot be aware of any alteration in their vision and a baseline as-sessment facilitates accurate interpretation of further testing if adeterioration is reported by the patient or in response to therapy
Assessment of the integrity of the other pituitary hormonesby the combination of basal and appropriate dynamic testing isrecommended Hyperprolactinemia from tumor co-secretionoccurs in up to a third of patients and can contribute to hypo-gonadism but may also occur a result of lsquostalk effectrsquo due totumor compression of the pituitary stalk interrupting the deliv-ery of inhibitory dopamine to the pituitary29 Evaluating all pa-tients with acromegaly for associated co-morbidities isrecommended at diagnosis (Table 2) in addition to longitudinalmonitoring during follow-up26
Treatment
Treatment goals in acromegaly include symptom relief tumorcontrol with maintenance of pituitary function biochemicalnormalization of GHIGF-1 and reversal of the excess morbidityand mortality associated with the disorder Current modalitiesof treatment available include surgery medical therapy andradiotherapy Treatment is complex and frequently more thanone modality is required to achieve treatment goals The deci-sion to treat and the therapeutic intervention used is based on anumber of factors which need to be weighed and tailored care-fully for each patient in a multidisciplinary setting
The definition of biochemical remission is difficult due tovariability in the assay and reference ranges used It is crucialthat the same GH and IGF-1 assay is maintained in the same pa-tient throughout their management While it remains contro-versial the current recommended biochemical target is arandom GHlt 1 lgl26 The decline in IGF-1 is more delayed com-pared with GH likely due to differential half-life of IGF-bindingproteins IGF-1 levels measured at 12 weeks after surgery are avalid reflection of surgical remission If the IGF-1 level hasdeclined but is still not normal measurement of a repeat IGF-1level is warranted due to variability in the IGF-1 assay
A normal IGF-1 value and undetectable GH value are suffi-cient for indicating surgical remission However if the GH is de-tectable (ie gt04 lgL) measurement of GH after a glucose loadmay yield important information The mean value of severalsamples taken a few hours apart throughout the day can also beused (GH day curve (GHDC)) as it is significantly correlated withthe GH nadir during OGTT and with the IGF-1 level30 While theideal endocrine outcome of any therapy in acromegaly is a nor-mal IGF-1 value and undetectable GH value levels that are asso-ciated with a normalization of mortality (as discussed in thesection above relating to mortality) are acceptable
Surgery
Transphenoidal surgery by an experienced pituitary surgeon isthe initial treatment of choice recommended for the majority ofpatients26 Ninety percent of patients who undergo pituitary sur-gery are treated using the transphenoidal approach craniotomy israrely performed The development of endoscopic and microsurgi-cal transphenoidal surgery offers further advantages over the con-ventional techniques including the possibility of superior tumorclearance in previously difficult to access areas less surgical mor-bidity fewer complications and reduced postoperative pain31
The main postoperative complaints relate to the transphe-noidal approach including nasal congestion sinusitis and
414 | QJM An International Journal of Medicine 2017 Vol 110 No 7
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
epistaxis More serious complications include hemorrhage CSFleakage and risk of meningitis stroke visual impairment vas-cular injury transient diabetes insipidus (DI) (typically occur-ring as a result of intraoperative manipulation of the pituitarystalk) and hypopituitarism32 Despite significant co-morbiditiesin patients with acromegaly surgical mortality rates of lt05can be anticipated33
Several factors are associated with reduced surgical successrates including large tumor size extrasellar extension andhigher preoperative GH levels34 Recurrence rates peak in years1ndash5 postoperatively with reported recurrence rates of up to 8with recurrence rates being lower in microadenomas comparedwith macroadenomas35 A normal IGF value and undetectableGH value are sufficient for indicating surgical remission
The Acromegaly group consensus guidelines suggest that ina patient with persistent disease after surgery repeat surgerymay be an option if the tumor is accessible26 The decision toinitiate somatostatin therapy prior surgery remains controver-sial In a prospective study of 30 patients with newly diagnosedacromegaly reductions in GH and IGF-1 concentrations andtumor volume were observed following 24 weeks of preopera-tive lanreotide autogel therapy36 Further studies do not reportany difference in the long-term results37 Due to the lack ofrandomized controlled studies the Acromegaly group consen-sus recommend against the routine use of preoperative somato-statin therapy In certain circumstances particularly forpatients with severe soft tissue growth complicating anestheticrisk or with significant comorbidities that may be improved bypreoperative therapy pretreatment with somatostatin receptorligands (SRL) may be considered38
Surgical debulking may be considered in patients with lowpredictive surgical cure rate at diagnosis to improve the chanceof achieving target GHIGF-1 levels with subsequent medicaltherapy Pretreatment disease burden is inversely correlatedto somatostatin analogue responsiveness39 In addition tobiochemical testing of remission as outlined above a contrast-enhanced MRI is recommended at least 12 weeks postopera-tively to visualize residual tumor This provides a baseline forfuture surveillance Formal visual field testing should also beperformed for patients with pre-operative visual deficits
Successful surgery by an experience neurosurgeon in a spe-cialized pituitary center can result in immediate biochemical
remission elimination of direct mass effects in addition to pro-viding tissue for immunohistochemical analysis Hence surgeryremains the primary therapeutic intervention in most patientswith acromegaly26
Medical treatment
Medical therapy has an important role as an adjunctive treat-ment option for persistent disease following non-curative sur-gery and also as first line therapy where surgery is not a feasibletherapeutic option Consensus guidelines outline the recom-mended role of medical therapy in the treatment of patientswith acromegaly There are a number of options for medicaltherapy in acromegaly including somatostatin receptor ligandsGH receptor antagonists and dopamine agonists
Somatostatin receptor ligands
Somatostatin is distributed throughout the nervous system andexerts neural control over many physiological functions includ-ing the inhibition of GH release It exists in two biologically ac-tive molecular forms somatostatin-14 and somatostatin -28with a short half-life of 2-3 min Its action is mediated throughG-protein coupled cell-surface receptors identified in a varietyof tissues including the pituitary Both bioactive forms havehigh binding affinity toward all five identified receptor sub-types SSR1-SSR540 GH-secreting pituitary adenomas expresspredominantly SSR2 and SSR5 First generation somatostatinanalogs octreotide and lanreotide show high affinity binding toSSR2 and to a lesser extent to SSR541
Currently three long-acting SRL formulations are availableoctreotide LAR Lanreotide depotautogel and pasireotide Rapidacting subcutaneous octreotide is also available and is adminis-tered two-three times daily The long-acting octreotide LAR isadministered intramuscularly every 4ndash6 weeks The approvedstarting octreotide LAR dose is 20 mg monthly with dose titra-tion every 3ndash6 months to a maximum dose of 40 mg monthlyLanreotide is available in a microsphere formulation (depot) in-jected intramuscularly every 7ndash14 days and an aqueous solution(Autogel) administered by deep subcutaneous injection every 4ndash6 weeks For lanreotide autogeldepot the approved starting
Table 2 Assessment of acromegaly complications at diagnosis and during long-term monitoring
At diagnosis During long-term follow-up
BP measurement Every 6 months or when change of treatment (if hypertensive)Echocardiography AnnuallyECG AnnuallyEpworth scale or sleep study AnnuallyECHO Doppler of peripheral arterial and venous
systemAnnually particularly in gigantism
OGTT Fasting blood glucose every 6 months (particularly in uncontrolled disease andduring SRL therapy) HbA1c every 6 months if diabetes present
Total testosterone SHBG and prolactin (males) Annually (free testosterone when doubts in interpretation of total testosterone)LH FSH17b-estradiol and prolactin (females) AnnuallyAcroQol AnnuallyDEXA Every 2 years if patient with osteopeniaosteoporosisThoracic and lumbar spine Xray Every 2ndash3 years if osteoporosis risk factors kyphosis or symptomsColonoscopy Every 10 years (more frequently if IGF-1 remains persistently elevated or if abnormal
colonoscopy or family history of chronic cancer)Genetic screening for markers of familial acromeg-
aly (if suspicion)
R Dineen et al | 415
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
dose is 90 mg monthly with a maximum dose up to 120 mgmonthly26
A large body of evidence supports the efficacy of long -actingSRL therapy In a critical analysis of the largest studies octreo-tide LAR reduced GH tolt25 lgl and normalized the IGF-1 levelsin 66 and 63 respectively42 Similar targets were achievedwith lanreotide-SR in 52 and 47 of cases respectively An ear-lier meta-analysis by Freda et al43 reported the overall chance ofIGF-1 normalization was 67 with octreotide and 47 with lan-reotide SR The higher efficacy reported with octreotide may beaccounted by pre-selection of responsive cases (patients whoshowed response to short acting octreotide only being recruitedto studies) inclusion of both primary and secondary therapycases and small case series An inherent challenge to meta-analyses in such a complex condition is the lack of standardiza-tion of GH and IGF-1 assays making comparison of absolutevalues between studies impossible
Smaller tumors lower baseline GH and IGF-1 levels44 highSSR2 and SSR5 expression45 and those previously treated withsurgery are associated with a better response to SRL treatmentRoutine performance of somatostatin receptor scintigraphy oran acute GH response to a subcutaneous octreotide injection asa determinant of SRL response are not recommended26
Somatostatin receptor ligands also have proven efficacy intumor volume reduction This has been extensively reviewedrecently by Colao et al46 Tumor reduction may be mediated bydirect anti-proliferative effects via activation of somatostatinreceptors or indirectly through angiogenesis inhibitionSathyapalan et al47 showed a significant reduction in the func-tional vascularity of pituitary tumors in a small study of five pa-tients after 24 weeks of octreotide therapy
Published meta-analysis revealed that octreotide LAR andlanreotide formulation induce tumor shrinkage in 660 and328 of cases respectively4849 Tumor reduction is progressivewith prolonged treatment and decreased IGF-1 levels may beits best predictor followed by age and degree of GH decrease
A recent detailed review of published studies evaluatingsomatostatin analogues as first line therapy showed that 6-24months of octreotide LAR therapy achievedgt20-30 tumor vol-ume reduction in 73-85 of patients Unlike surgery primarymedical therapy cannot cure acromegaly Based on a recentmeta-analysis of available studies primary SRL therapy is asso-ciated with a lower remission rates compared to initial surgery(45 vs 67)49 However the accuracy of these remission ratesis questionable given the non-comparable nature and the het-erogeneity of studies included Primary SRL therapy can beoffered before surgery in patients with contraindications incases with unresectable tumor or with severe comorbidities26
During SRL treatment the most frequent side effects includeabdominal discomfort flatulence cramps and diarrheaGallbladder sludge or gallstones occur in 25 of subjects butare usually asymptomatic SRL treatment was initially thoughtto aggravate the increased risk of glucose intolerance in thesepatients but the overall effect on glucose metabolism is not clin-ically significant50
Pasireotide is a multireceptor-targeted somatostatin recep-tor ligand which has higher functional activity than octreotideon SSR subtypes except type 4 but in particular SSR551 In alarge phase III randomized trial in patients with acromegalywho were naive to medical therapy pasireotide LAR and octreo-tide LAR have a similar effect of tumor reduction despite thefact that pasireotide was superior to octreotide in providing bio-chemical control After 12 months of treatment 81 of pasireo-tide patients had20 reduction in tumor volume compared
with 77 of octreotide LAR patients52 Pasireotide has similarrates of gastrointestinal side effects to other SRLs however therates of hyperglycemia are significantly higher (occurring in 31ndash57 of patients)
Pegvisomant
Pegvisomant is a pegylated recombinant analog of human GHincorporating nine amino acid mutations Pegylation extendsthe half-life by reducing renal clearance53 The mutations resultin increased affinity to the GH receptor in addition to blockingthe second binding site on the receptor preventing GHR dimer-ization and signal transduction GH hypersecretion persists asit does not target the GH secreting tumor at the level of the pitu-itary hence GH measurements cannot be used to monitor dis-ease activity and IGF-1 becomes the sole marker to monitorbiochemical response during therapy
Pegvisomant has been shown to be highly effective in pro-viding biochemical control of acromegaly in multiple studies Ina 12-week double-blind placebo controlled study Trainer et al54
randomly assigned patients to receive placebo 10 15 or 20 mgof pegvisomant Normalization of IGF-1 (using age and sex-matched reference ranges) was achieved in 10 54 81 and89 respectively Symptom control was also observed The effi-cacy of pegvisomant over a longer period was subsequentlystudied Van der Lely et al55 reported 97 of patients achievingnormal IGF-1 levels in patients receiving therapy for 12 monthsor more (Figure 1) Dose reduction was required in 1190 pa-tients as IGF-1 levels dropped below normal reference range forage and sex
As mentioned above pegvisomant does not exert a centraleffect on pituitary GH secretion hence fears exist over the pos-sibility of increased tumor growth The German PegvisomantObservational Study is a multicenter surveillance study com-menced in 2004 to assess the efficacy and safety of pegvisomanttherapy in patients with acromegaly56 Neuroradiological moni-toring of tumor extension is performed with MRI imagingBuchfelder et al studied 3 years of follow-up data of 307 pa-tients Tumor progression was reported in between 2 and3 ofpatients treated an increase not outside the expected rate inpatients not treated with pegvisomant
Pegvisomant is administered as daily subcutaneous injec-tion It is generally well tolerated with adverse effects reportedinlt10 of patients These may include injection site reactionswith reversible lipohypertrophy and deranged liver functiontests (attributable to the polyethylene glycol pegylated vehicle)
The predominant limiting factor for use of this agent in clin-ical practice remains its considerable cost It is most often usedas a second line agent in cases resistant or intolerant to SRLtherapy or in combination with SRLrsquos in partially resistantcases It is also a potential treatment option in acromegaly pa-tients with difficult to control diabetes mellitus due to its favor-able effect on glycemic control
Dopamine agonists
Dopamine agonists bind to the D2 dopamine receptors in the pi-tuitary gland and suppress prolactin and GH secretion The useof bromocriptine a first-generation dopamine agonist is lim-ited by its side effect profile including GI symptoms lethargyand orthostatic hypotension It also compares poorly with som-atostatin receptor ligands in terms of efficacy with normaliza-tion of GHIGF-1 reported in only 10 of patients57
416 | QJM An International Journal of Medicine 2017 Vol 110 No 7
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
Cabergoline an ergot derivative dopamine agonist has beenused for decades in the treatment of hyperprolactinaemia andParkinsonrsquos disease Cabergoline is better tolerated and more ef-fective than bromocriptine however its use was superseded bythe development of SRL therapy showing higher efficacy rates
Clinical trials of cabergoline in acromegaly are small non-randomized and report variable results In a recent systematicreview of 10 trials with a total of 150 acromegaly patients con-trol of acromegaly was achieved in 34 of patients who receivedcabergoline therapy alone and 52 when added to SRL therapyin patients with suboptimal control58 Consequently currentguidelines recommend the use of cabergoline in patients withinadequate response to other medical treatment with highestbenefit expected in cases with modest persistent hormonal ele-vations26 Conflicting data exists as to whether the co-secretionof prolactin is predictive of response to dopamine agonist ther-apy Some studies conclude that tumors that co-secrete prolac-tin and GH have a greater response to dopamine agonisttherapy than those than solely secrete GH whereas othersshow no effect There remains little data available regardingtumor shrinkage in patients with acromegaly who are receivingdopamine agonist therapy59 Jaffe et al57 reported combined re-sults from a number of studies which revealed that 29 of pa-tients had some tumor shrinkage on dopamine agonist therapyand the majority of patients who had tumor shrinkage werealso hyperprolactinemic It is difficult to interpret these findinggiven the small number and heterogeneous characteristics ofthe patients included
The most frequent adverse effects of dopamine agonist ther-apy are nausea constipation headache mood disturbancenasal stuffiness and dizziness Cardiac valve abnormalitieswere described with high doses of cabergoline used inParkinsonrsquos disease but not with current recommended dosageused for patients with acromegaly60
DopastatinBIM-23A760 is a chimeric molecule hasbeen shown in vitro to have high affinity for both somatosta-tin receptor subtypes- 2 and 5 in addition to dopamine 2 recep-tor61 With increasing knowledge of the importance of SSR5 inregulation of GH in GH-secreting adenomas dopastatin isundergoing further development in clinical studies to deter-mine if there is a role for these compounds in the treatment ofacromegaly
Radiotherapy
Radiation therapy is used as adjuvant treatment in the settingof persistent disease despite surgery andor medical treatmentor if medical therapy is unavailable unsuccessful or not toler-ated Radiotherapy has been shown to be effective in loweringserum GH levels36 but conflicting results have been reported re-garding the normalization of IGF-1 levels62 Furthermore thedelay in therapeutic benefit and the high risk of developinghypopituitarism serve as arguments against the more routineuse of radiotherapy
Conventional radiotherapy has been used for gt30 years inthe adjunctive treatment of pituitary adenomas It is generallydelivered in fractionated doses 4ndash5 times per week so as to re-duce daily-fractionated dose The risk of adverse effects beingproportional to maximal dose per day63 Early studies of con-ventional radiotherapy reported high efficacy rate of 80ndash100however remission was defined as a GH level below 5-10 ngmlMore recent studies using revised biochemical remission tar-gets report a mean remission rate between 50 and 60 Jenkinset al64 assessed the effects of conventional pituitary irradiationin 884 patients of the UK National Acromegaly Register MeanGH levels declined from 135 to 53 ngml at 2 years after surgeryto 2 ngml by 10 years and a further decline to 11 ngml at 20years (Figure 2) Furthermore they observed a parallel fall in IGF-
Figure 1 Baseline and lowest values of individual serum insulin-like growth factor-1 concentrations achieved in 90 patients treated for 12 months or more with daily
pegvisomant (daggerPlt005 vs baseline DaggerPlt001 vs baseline) The shaded area represents the age-adjusted normal range for insulin-like growth factor-155
R Dineen et al | 417
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
1 levels with 63 of patients having a normal level by 10years64
Stereotactic radiotherapy offers improvement in immobil-ization imaging and treatment delivery from conventionaltechniques It can be delivered as a single fraction radiosurgeryusing a Gamma knife (a source of cobalt) or a linear acceleratoror a stereotactic conformal radiotherapy delivered as fractio-nated treatment using a linear accelerator There is no clear ad-vantage for either of the radiosurgical techniques in terms ofsparing normal tissue receiving high doses of radiation65 A crit-ical analysis of the literature reported variable rates of both bio-chemical and tumor response 17ndash82 and 37ndash100respectively66 The authors attributed the wide variability to theuse of different treatment schedules and definitions ofremission
Hypopituitarism is less frequent with radiosurgery than con-ventional radiotherapy At least 50 of patient treated with con-ventional radiotherapy will have acquired new anteriorpituitary hormonal deficits at 10 years67 In cohorts treatedsolely with stereotactic techniques rates of hypopituitarismvary between 0 and 2068 However it is likely that the candi-dates for stereotactic radiotherapy had smaller remnants of dis-ease and therefore less normal tissue irradiated
Annual hormonal testing is required due to the risk of latehypopituitarism26 Other complications following radiotherapyinclude the risk of second brain tumors stroke and rarely opticneuropathy cranial nerve deficits and radionecrosis a rare ad-verse effect of gamma knife radiotherapy69ndash71
Patients treated with conventional radiotherapy have beenreported to have increased mortality predominantly due tostroke independent of GHIGF-I levels and hypopituitarism20
Current guidelines recommend the use of stereotactic radio-therapy over conventional radiation therapy unless significantresidual tumor burden or the lesion is too close to the opticchiasm26
Conclusion
Prolonged exposure to elevated endogenous levels of GH andIGF-I results in a multisystem disease characterized by somaticovergrowth multiple co-morbidities and premature mortalityEarly detection prevents the development of irreversible com-plications of the disease including cardiomyopathy respiratory
dysfunction and arthropathy Despite the imprecision of assaysfor GH and IGF-I it is clear from epidemiologic studies that tightbiochemical control is essential to reduce morbidity controlsymptoms and improve mortality rates
Optimal implementation of current guidelines in routine clin-ical practice and maximal use of the medical treatment could im-prove the long-term control of patients with significant benefitsfor morbidity and mortality Another important aspect in thetreatment of patients with acromegaly is also the appropriate tar-geted treatment of co-morbidities associated with acromegaly
Achievement of the criteria for cure during or after therapyis determined by assessing biochemical control targeting con-trolled levels of GH and normalization of IGF-I levels monitor-ing tumor size assessing residual pituitary function andmonitoring co-morbidities
New therapeutic molecules currently in trials will hopefullyoffer further benefit to those patients resistant to current thera-peutic modes for this chronic progressive disorder
Conflict of interest None declared
References1 Melmed S Braunstein GD Horvath E Ezrin C Kovacs K
Pathophysiology of acromegaly Endocr Rev 1983 4271ndash902 Mestron A Webb SM Astorga R Benito P Catala M
Gaztambide S et al Epidemiology clinical characteristicsoutcome morbidity and mortality in acromegaly based onthe Spanish Acromegaly Registry (Registro Espanol deAcromegalia REA) Eur J Endocrinol 2004 151439ndash46
3 Jagannathan J Dumont AS Prevedello DM Oskouian RJLopes B Jane JA Jr and Laws ER Jr Genetics of pituitary aden-omas current theories and future implications NeurosurgFocus 2005 19E4
4 Zhu X Lin CR Prefontaine CG Tollkuhn J Rosenfeld MGGenetic control of pituitary developement and hypopituitar-ism Curr Opin Genet Dev 2005 15332ndash40
5 Melmed S Acromegaly pathogenesis and treatment J ClinInvest 2009 1193189ndash202
6 Colao A Ferone D Marzullo P Lombardi G Systemic compli-cations of acromegaly epidemiology pathogenesis andmanagement Endocr Rev 2004 25102ndash52
7 Korbonits M Gadelha MR Roncaroli F Grossman AB Ellard SEvanson J et al Landscape of familial isolated and young-onset pituitary adenomas prospective diagnosis in AIP mu-tation carriers J Clin Endocrinol Metab 2015 100E1242ndash54
8 Larkin S Reddy R Karavitaki N Cudlip S Wass J Ansorge OGranulation pattern but not GSP or GHR mutation is associ-ated with clinical characteristics in somatostatin-naive pa-tients with somatotroph adenomas Eur J Endocrinol 2013168491ndash9
9 Molitch ME Clinical manifestations of acromegaly EndocrinolMetab Clin North Am 1992 21597ndash614
10Reid TJ Post KD Bruce JN Nabi KM Reyes-Vidal CM et alFeatures at diagnosis of 324 patients with acromegaly didnot change from 1981 to 2006 acromegaly remains under-recognized and under-diagnosed Clin Endocrinol 201072203ndash8
11Moslashller N Joslashrgensen JO Abildgard N Orskov L Schmitz OChristiansen JS Effects of growth hormone on glucose me-tabolism Horm Res 1991 36 (Suppl 1)32ndash5
12Dreval AV Trigolosova IV Misnikova IV Kovalyova YATishenina RS Barsukov IA et al Prevalence of diabetes melli-tus in patients with acromegaly Endocr Connect 2014 393ndash8
Figure 2 Percentage of all patients achieving a serum GH level lt25 ngml (bars)
and the mean GH level (line) in the years after pituitary irradiation64
418 | QJM An International Journal of Medicine 2017 Vol 110 No 7
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
13Roemmler J Gutt B Fischer R Vay S Wiesmeth ABidlingmaier M et al Elevated incidence of sleep apnoea inacromegaly-correlation to disease activity Sleep Breath 2012161247ndash53
14Killinger Z Payer J Lazurova I Imrich R Homerova Z KuzmaM et al Arthropathy in acromegaly Rheum Dis Clin North Am2010 36713ndash20
15Kameyama S Tanaka R Hasegawa A Tamura T Kuroki MSubclinical carpal tunnel syndrome in acromegaly NeurolMed Chir 1993 33547ndash51
16Mazziotti G Biagioli E Maffezzoni F Spinello M Serra VMaroldi R et al Bone turnover bone mineral density and frac-ture risk in acromegaly a meta-analysis J Clin EndocrinolMetab 2015 100384ndash94
17Renehan AG OrsquoConnell J OrsquoHalloran D Shanahan F PottenCS OrsquoDwyer ST et al Acromegaly and colorectal cancer acomprehensive review of epidemiology biological mechan-isms and clinical implications Horm Metab Res 200335712ndash25
18Orme S McNally RJ Cartwright RA Belchetz PE Mortality andcancer incidence in acromegaly a restrospective cohortstudy J Clin Endocrinol Metab 1998 832730ndash4
19Petroff D Teuroonjes A Grussendorf M Droste M Dimopoulou CStalla G et al The Incidence of cancer among acromegaly pa-tients results from the German Acromegaly Registry J ClinEndocrinol Metab 2015 1003894ndash902
20Sherlock M Ayuk J Tomlinson JW Toogood AA Aragon-Alonso A Sheppard MC et al Mortality in patients with pitu-itary disease Endocr Rev 2010 31301ndash42
21Bates AS Vanrsquot H Jones JM Clayton RN An audit of outcomeof treatment in acromegaly Q J Med 1993 86293ndash9
22Ayuk J Clayton RN Holder G Sheppard MC Stewart PMBates AS Growth hormone and pituitary radiotherapy butnot serum insulin-like growth factor-I concentrations pre-dict excess mortality in patients with acromegaly J ClinEndocrinol Metab 2004 891613ndash7
23Kauppinen-Meuroakelin R Sane T Reunanen A Veuroalimeuroaki MJNiskanen L Markkanen H et al A nationwide survey of mor-tality in acromegaly J Clin Endocrinol Metab 2005 904081ndash6
24Holdaway IM Bolland MJ Gamble GD A meta-analysis of theeffect of lowering serum levels of GH and IGF-I on mortalityin acromegaly Eur J Endocrinol 2008 15989ndash95
25Rosen T Bengtsson BA Premature mortality due to cardio-vascular disease in hypopituitarism Lancet 1990 336285ndash8
26Katznelson L Laws ER Jr Melmed S Molitch ME Murad MHUtz A et al Acromegaly an endocrine society clinical practiceguideline J Clin Endocrinol Metab 2014 993933ndash51
27Freda PU Post KD Powell JS Wardlaw SL Evaluation of dis-ease status with sensitive measures of growth hormone se-cretion in 60 postoperative patients with acromegaly J ClinEndocrinol Metab 1998 833808ndash16
28Dimaraki EV Jaffe CA DeMott-Friberg R Chandler WFBarkan AL Acromegaly with apparently normal GH secretionimplications for diagnosis and follow-up J Clin EndocrinolMetab 2002 873537ndash42
29Losa M Von Werder K Pathophysiology and clinical aspectsof the ectopic GH-releasing hormone syndrome ClinEndocrinol 1997 47123ndash35
30Dobrashian RD OrsquoHalloran DJ Hunt A Beardwell CG ShaletSM Relationships between insulin-like growth factor-1 levelsand growth hormone concentrations during diurnal profilesand following oral glucose in acromegaly Clin Endocrinol 199338589ndash93
31Frank G Pasquini E Farneti G Mazzatenta D Sciarretta VGrasso V et al The endoscopic versus the traditional ap-proach in pituitary surgery Neuroendocrinology 2006 83240ndash8
32Marquez Y Tuchman A Zada G Surgery and radiosurgery foracromegaly a review of indications operative techniquesoutcomes and complications Int J Endocrinol 2012 2012386ndash401
33Laws ER Vance ML Thapar K Pituitary surgery for the man-agement of acromegaly Horm Res 2000 5371ndash5
34Salaun C Foubert L Vialatou M Kujas M Turpin G Prognosticfactors of surgical cure of growth hormone secreting pituitary aden-omas Ann Medecine Interne 1999 150195ndash8
35Kreutzer J Vance ML Lopes MB Laws ER Jr Surgical manage-ment of GH-secreting pituitary adenomas an outcome studyusing modern remission criteria J Clin Endocrinol Metab 2001864072ndash7
36Annamalai AK Webb A Kandasamy N Elkhawad M Moir SKhan F et al A comprehensive study of clinical biochemicalradiological vascular cardiac and sleep parameters in anunselected cohort of patients with acromegaly undergoingpresurgical somatostatin receptor ligand therapy J ClinEndocrinol Metab 2013 981040ndash50
37Shen M Shou X Wang Y Zhang Z Wu J Mao Y et al Effect ofpresurgical long-acting octreotide treatment in acromegalypatients with invasive pituitary macroadenomas a prospect-ive randomized study Endocr J 2010 571035ndash44
38Friedel ME Johnston D Singhal S Al Khalili K Farrell CJEvans JJ et al Airway management and perioperative con-cerns in acromegaly patients undergoing endoscopic trans-sphenoidal surgery for pituitary tumors Otolaryngol HeadNeck Surg 2013 149840ndash4
39Bhayana S Booth G Asa SL Kovacs Ezzat S The implicationof somatotroph adenoma phenotype to somatostatin analogresponsiveness in acromegaly J Clin Endocrinol Metab 2005906290ndash5
40Reisine T Bell GI Molecular biology of somatostatin recep-tors Endocr Rev 1995 16427ndash42
41Zatelli MC Piccin D Tagliati F et al Dopamine receptor sub-type 2 and somatostatin receptor subtype 5 expression influ-ences somatostatin analog effects on human somatotrophpituitary adenomas in vitro J Mol Endocrinol 2005 35333ndash41
42Murray RD Melmed S A critical analysis of clinically avail-able somatostatin analog formulations for therapy of acro-megaly J Clin Endocrinol Metab 2008 932957ndash68
43Freda PU Katznelson L Van der Lely A Reyes CM Zhao SRabinowitz D Long-acting somatostatin analog therapy ofacromegaly a meta-analysis J Clin Endocrinol Metab 2005904465ndash74
44Howlett TA Willis D Walker G Wass JA Trainer PJ Control ofgrowth hormone and IGF1 in patients with acromegaly in theUK responses to medical treatment with somatostatin ana-logues and dopamine agonists Clin Endocrinol 201379689ndash99
45Espinosa de los Monteros AL Carrasco C Albarran AAGadelha M Abreu A Mercado M The role of primary pharma-cological therapy in acromegaly Pituitary 2014 17 (Suppl1)S4ndashS10
46Colao AM Auriemma RS Pivonello R The effects of somato-statin analogue therapy on pituitary tumor volume in pa-tients with acromegaly Pituitary 2016 19210ndash21
47Sathyapalan T Lowry M Turnbull LW Rowland-Hill C AtkinSL Mechanism of action of octreotide in acromegalic tu-mours in vivo using dynamic contrast-enhanced magneticresonance imaging Pituitary 2007 10233ndash6
R Dineen et al | 419
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
48Giustina A Mazziotti G Torri V Spinello M Floriani IMelmed S Meta-analysis on the effects of octreotide ontumor mass in acromegaly PLoS One 2012 7e36411
49Abu Dabrh AM Mohammed K Asi N Farah WH Wang ZFarah MH et al Surgical interventions and medical treat-ments in treatment-naive patients with acromegaly system-atic review and meta-analysis J Clin Endocrinol Metab 2014994003ndash14
50Colao A Bronstein M Freda P Gu F Shen C-C Gadelha Met al Pasireotide versus octreotide in acromegaly a head-to-head superiority study J Clin Endocrinol Metab 2014 99791ndash9
51Schmid HA Schoeffter P Functional activity of the multili-gand analog SOM230 at human recombinant somatostatinreceptor subtypes supports its usefulness in neuroendocrinetumors Neuroendocrinology 2004 80 (Suppl 1)47ndash50
52Mazziotti G Floriani I Bonadonna S Torri V Chanson PGiustina A Effects of somatostatin analogs on glucosehomeostasis a metaanalysis of acromegaly studies J ClinEndocrinol Metab 2009 941500ndash8
53Higham CE Trainer PJ Growth hormone excess and the de-velopment of growth hormone receptor antagonists ExpPhysiol 2008 931157ndash69
54Trainer PJ Drake WM Katznelson L et al Treatment of acro-megaly with the growth hormone receptor antagonist pegvi-somant N Engl J Med 2000 3421171ndash7
55Van der Lely AJ Hutson RK Trainer PJ Besser GM Barkan ALKatznelson L et al Long-term treatment of acromegaly withpegvisomant a growth hormone receptor antagonist Lancet2001 3581754ndash9
56Buchfelder M Weigel D Droste M Mann K Saller B BrubachK et al Pituitary tumor size in acromegaly during pegvisom-ant treatment experience from MR re-evaluations of theGerman Pegvisomant Observational Study Eur J Endocrinol2009 16127ndash35
57 Jaffe CA Barkan AL Treatment of acromegaly with dopamineagonists Endocrinol Metab Clin North Am 1992 21713ndash35
58Sandret L Maison P Chanson P Place of cabergoline in acro-megaly a meta-analysis J Clin Endocrinol Metab 2011961327ndash35
59Sherlock M Woods C Sheppard C Medical therapy in acro-megaly Nat Rev Endocrinol 2011 7291ndash300
60Samson SL Ezzat S AACEACE disease state clinical reviewdopamine agonists for hyperprolactinemia and the risk ofcardiac valve disease Endocr Pract 2014 20608ndash16
61 Jaquet P Gunz G Saveanu A Dufour H Taylor J Dong J et alEfficacy of chimeric molecules directed towards multiplesomatostatin and dopamine receptors on inhibition of GHand prolactin secretion from GH-secreting pituitary aden-omas classified as partially responsive to somatostatin ana-log therapy Eur J Endocrinol 2005 153135ndash41
62Barkan AL Halasz I Dornfeld KJ Jaffe CA Friberg RDChandler WF et al Pituitary irradiation is ineffective in nor-malizing plasma insulin-like growth factor I in patients withacromegaly J Clin Endocrinol Metab 1997 823187ndash91
63Eastman RC Gorden P Glatstein E Roth J Radiation therapyof acromegaly Endocrinol Metab Clin North Am 199221693ndash712
64 Jenkins PJ Bates Carson MN Stewart PM Wass JAConventional pituitary irradiation is effective in loweringserum growth hormone and insulin-like growth factor-I inpatients with acromegaly J Clin Endocrinol Metab 2006911239ndash45
65Minniti G Gilbert DC Brada M Modern techniques for pituit-ary radiotherapy Rev Endocr Metab Disord 2008 10135ndash44
66Stapleton CJ Liu CY Weiss M The role of stereotactic radio-surgery in the multimodal management of growth hormone-secreting pituitary adenomas Neurosurg Focus 2010 29E11
67Biermasz NR van Dulken H Roelfsema F Long-term follow-up results of postoperative radiotherapy in 36 patients withacromegaly J Clin Endocrinol Metab 2000 852475ndash82
68Attanasio R Epaminonda P Motti E Giugni E Ventrella LCozzi R et al Gamma-knife radiosurgery in acromegaly a 4-year follow-up study J Clin Endocrinol Metab 2003 883105ndash12
69Minniti G Traish D Ashley S Gonsalves A Brada M Risk ofsecond brain tumor after conservative surgery and radiother-apy for pituitary adenoma update after an additional 10years J Clin Endocrinol Metab 2005 90800ndash4
70Brada M Burchell L Ashley S Traish D The incidence of cere-brovascular accidents in patients with pituitary adenoma IntJ Radiat Oncol Biol Phys 1999 45693ndash8
71Laws ER Sheehan JP Sheehan JM Jagnathan J Jane JA JrOskouian R Stereotactic radiosurgery for pituitary aden-omas a review of the literature J Neurooncol 2004 69257ndash72
420 | QJM An International Journal of Medicine 2017 Vol 110 No 7
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022

epistaxis More serious complications include hemorrhage CSFleakage and risk of meningitis stroke visual impairment vas-cular injury transient diabetes insipidus (DI) (typically occur-ring as a result of intraoperative manipulation of the pituitarystalk) and hypopituitarism32 Despite significant co-morbiditiesin patients with acromegaly surgical mortality rates of lt05can be anticipated33
Several factors are associated with reduced surgical successrates including large tumor size extrasellar extension andhigher preoperative GH levels34 Recurrence rates peak in years1ndash5 postoperatively with reported recurrence rates of up to 8with recurrence rates being lower in microadenomas comparedwith macroadenomas35 A normal IGF value and undetectableGH value are sufficient for indicating surgical remission
The Acromegaly group consensus guidelines suggest that ina patient with persistent disease after surgery repeat surgerymay be an option if the tumor is accessible26 The decision toinitiate somatostatin therapy prior surgery remains controver-sial In a prospective study of 30 patients with newly diagnosedacromegaly reductions in GH and IGF-1 concentrations andtumor volume were observed following 24 weeks of preopera-tive lanreotide autogel therapy36 Further studies do not reportany difference in the long-term results37 Due to the lack ofrandomized controlled studies the Acromegaly group consen-sus recommend against the routine use of preoperative somato-statin therapy In certain circumstances particularly forpatients with severe soft tissue growth complicating anestheticrisk or with significant comorbidities that may be improved bypreoperative therapy pretreatment with somatostatin receptorligands (SRL) may be considered38
Surgical debulking may be considered in patients with lowpredictive surgical cure rate at diagnosis to improve the chanceof achieving target GHIGF-1 levels with subsequent medicaltherapy Pretreatment disease burden is inversely correlatedto somatostatin analogue responsiveness39 In addition tobiochemical testing of remission as outlined above a contrast-enhanced MRI is recommended at least 12 weeks postopera-tively to visualize residual tumor This provides a baseline forfuture surveillance Formal visual field testing should also beperformed for patients with pre-operative visual deficits
Successful surgery by an experience neurosurgeon in a spe-cialized pituitary center can result in immediate biochemical
remission elimination of direct mass effects in addition to pro-viding tissue for immunohistochemical analysis Hence surgeryremains the primary therapeutic intervention in most patientswith acromegaly26
Medical treatment
Medical therapy has an important role as an adjunctive treat-ment option for persistent disease following non-curative sur-gery and also as first line therapy where surgery is not a feasibletherapeutic option Consensus guidelines outline the recom-mended role of medical therapy in the treatment of patientswith acromegaly There are a number of options for medicaltherapy in acromegaly including somatostatin receptor ligandsGH receptor antagonists and dopamine agonists
Somatostatin receptor ligands
Somatostatin is distributed throughout the nervous system andexerts neural control over many physiological functions includ-ing the inhibition of GH release It exists in two biologically ac-tive molecular forms somatostatin-14 and somatostatin -28with a short half-life of 2-3 min Its action is mediated throughG-protein coupled cell-surface receptors identified in a varietyof tissues including the pituitary Both bioactive forms havehigh binding affinity toward all five identified receptor sub-types SSR1-SSR540 GH-secreting pituitary adenomas expresspredominantly SSR2 and SSR5 First generation somatostatinanalogs octreotide and lanreotide show high affinity binding toSSR2 and to a lesser extent to SSR541
Currently three long-acting SRL formulations are availableoctreotide LAR Lanreotide depotautogel and pasireotide Rapidacting subcutaneous octreotide is also available and is adminis-tered two-three times daily The long-acting octreotide LAR isadministered intramuscularly every 4ndash6 weeks The approvedstarting octreotide LAR dose is 20 mg monthly with dose titra-tion every 3ndash6 months to a maximum dose of 40 mg monthlyLanreotide is available in a microsphere formulation (depot) in-jected intramuscularly every 7ndash14 days and an aqueous solution(Autogel) administered by deep subcutaneous injection every 4ndash6 weeks For lanreotide autogeldepot the approved starting
Table 2 Assessment of acromegaly complications at diagnosis and during long-term monitoring
At diagnosis During long-term follow-up
BP measurement Every 6 months or when change of treatment (if hypertensive)Echocardiography AnnuallyECG AnnuallyEpworth scale or sleep study AnnuallyECHO Doppler of peripheral arterial and venous
systemAnnually particularly in gigantism
OGTT Fasting blood glucose every 6 months (particularly in uncontrolled disease andduring SRL therapy) HbA1c every 6 months if diabetes present
Total testosterone SHBG and prolactin (males) Annually (free testosterone when doubts in interpretation of total testosterone)LH FSH17b-estradiol and prolactin (females) AnnuallyAcroQol AnnuallyDEXA Every 2 years if patient with osteopeniaosteoporosisThoracic and lumbar spine Xray Every 2ndash3 years if osteoporosis risk factors kyphosis or symptomsColonoscopy Every 10 years (more frequently if IGF-1 remains persistently elevated or if abnormal
colonoscopy or family history of chronic cancer)Genetic screening for markers of familial acromeg-
aly (if suspicion)
R Dineen et al | 415
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
dose is 90 mg monthly with a maximum dose up to 120 mgmonthly26
A large body of evidence supports the efficacy of long -actingSRL therapy In a critical analysis of the largest studies octreo-tide LAR reduced GH tolt25 lgl and normalized the IGF-1 levelsin 66 and 63 respectively42 Similar targets were achievedwith lanreotide-SR in 52 and 47 of cases respectively An ear-lier meta-analysis by Freda et al43 reported the overall chance ofIGF-1 normalization was 67 with octreotide and 47 with lan-reotide SR The higher efficacy reported with octreotide may beaccounted by pre-selection of responsive cases (patients whoshowed response to short acting octreotide only being recruitedto studies) inclusion of both primary and secondary therapycases and small case series An inherent challenge to meta-analyses in such a complex condition is the lack of standardiza-tion of GH and IGF-1 assays making comparison of absolutevalues between studies impossible
Smaller tumors lower baseline GH and IGF-1 levels44 highSSR2 and SSR5 expression45 and those previously treated withsurgery are associated with a better response to SRL treatmentRoutine performance of somatostatin receptor scintigraphy oran acute GH response to a subcutaneous octreotide injection asa determinant of SRL response are not recommended26
Somatostatin receptor ligands also have proven efficacy intumor volume reduction This has been extensively reviewedrecently by Colao et al46 Tumor reduction may be mediated bydirect anti-proliferative effects via activation of somatostatinreceptors or indirectly through angiogenesis inhibitionSathyapalan et al47 showed a significant reduction in the func-tional vascularity of pituitary tumors in a small study of five pa-tients after 24 weeks of octreotide therapy
Published meta-analysis revealed that octreotide LAR andlanreotide formulation induce tumor shrinkage in 660 and328 of cases respectively4849 Tumor reduction is progressivewith prolonged treatment and decreased IGF-1 levels may beits best predictor followed by age and degree of GH decrease
A recent detailed review of published studies evaluatingsomatostatin analogues as first line therapy showed that 6-24months of octreotide LAR therapy achievedgt20-30 tumor vol-ume reduction in 73-85 of patients Unlike surgery primarymedical therapy cannot cure acromegaly Based on a recentmeta-analysis of available studies primary SRL therapy is asso-ciated with a lower remission rates compared to initial surgery(45 vs 67)49 However the accuracy of these remission ratesis questionable given the non-comparable nature and the het-erogeneity of studies included Primary SRL therapy can beoffered before surgery in patients with contraindications incases with unresectable tumor or with severe comorbidities26
During SRL treatment the most frequent side effects includeabdominal discomfort flatulence cramps and diarrheaGallbladder sludge or gallstones occur in 25 of subjects butare usually asymptomatic SRL treatment was initially thoughtto aggravate the increased risk of glucose intolerance in thesepatients but the overall effect on glucose metabolism is not clin-ically significant50
Pasireotide is a multireceptor-targeted somatostatin recep-tor ligand which has higher functional activity than octreotideon SSR subtypes except type 4 but in particular SSR551 In alarge phase III randomized trial in patients with acromegalywho were naive to medical therapy pasireotide LAR and octreo-tide LAR have a similar effect of tumor reduction despite thefact that pasireotide was superior to octreotide in providing bio-chemical control After 12 months of treatment 81 of pasireo-tide patients had20 reduction in tumor volume compared
with 77 of octreotide LAR patients52 Pasireotide has similarrates of gastrointestinal side effects to other SRLs however therates of hyperglycemia are significantly higher (occurring in 31ndash57 of patients)
Pegvisomant
Pegvisomant is a pegylated recombinant analog of human GHincorporating nine amino acid mutations Pegylation extendsthe half-life by reducing renal clearance53 The mutations resultin increased affinity to the GH receptor in addition to blockingthe second binding site on the receptor preventing GHR dimer-ization and signal transduction GH hypersecretion persists asit does not target the GH secreting tumor at the level of the pitu-itary hence GH measurements cannot be used to monitor dis-ease activity and IGF-1 becomes the sole marker to monitorbiochemical response during therapy
Pegvisomant has been shown to be highly effective in pro-viding biochemical control of acromegaly in multiple studies Ina 12-week double-blind placebo controlled study Trainer et al54
randomly assigned patients to receive placebo 10 15 or 20 mgof pegvisomant Normalization of IGF-1 (using age and sex-matched reference ranges) was achieved in 10 54 81 and89 respectively Symptom control was also observed The effi-cacy of pegvisomant over a longer period was subsequentlystudied Van der Lely et al55 reported 97 of patients achievingnormal IGF-1 levels in patients receiving therapy for 12 monthsor more (Figure 1) Dose reduction was required in 1190 pa-tients as IGF-1 levels dropped below normal reference range forage and sex
As mentioned above pegvisomant does not exert a centraleffect on pituitary GH secretion hence fears exist over the pos-sibility of increased tumor growth The German PegvisomantObservational Study is a multicenter surveillance study com-menced in 2004 to assess the efficacy and safety of pegvisomanttherapy in patients with acromegaly56 Neuroradiological moni-toring of tumor extension is performed with MRI imagingBuchfelder et al studied 3 years of follow-up data of 307 pa-tients Tumor progression was reported in between 2 and3 ofpatients treated an increase not outside the expected rate inpatients not treated with pegvisomant
Pegvisomant is administered as daily subcutaneous injec-tion It is generally well tolerated with adverse effects reportedinlt10 of patients These may include injection site reactionswith reversible lipohypertrophy and deranged liver functiontests (attributable to the polyethylene glycol pegylated vehicle)
The predominant limiting factor for use of this agent in clin-ical practice remains its considerable cost It is most often usedas a second line agent in cases resistant or intolerant to SRLtherapy or in combination with SRLrsquos in partially resistantcases It is also a potential treatment option in acromegaly pa-tients with difficult to control diabetes mellitus due to its favor-able effect on glycemic control
Dopamine agonists
Dopamine agonists bind to the D2 dopamine receptors in the pi-tuitary gland and suppress prolactin and GH secretion The useof bromocriptine a first-generation dopamine agonist is lim-ited by its side effect profile including GI symptoms lethargyand orthostatic hypotension It also compares poorly with som-atostatin receptor ligands in terms of efficacy with normaliza-tion of GHIGF-1 reported in only 10 of patients57
416 | QJM An International Journal of Medicine 2017 Vol 110 No 7
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
Cabergoline an ergot derivative dopamine agonist has beenused for decades in the treatment of hyperprolactinaemia andParkinsonrsquos disease Cabergoline is better tolerated and more ef-fective than bromocriptine however its use was superseded bythe development of SRL therapy showing higher efficacy rates
Clinical trials of cabergoline in acromegaly are small non-randomized and report variable results In a recent systematicreview of 10 trials with a total of 150 acromegaly patients con-trol of acromegaly was achieved in 34 of patients who receivedcabergoline therapy alone and 52 when added to SRL therapyin patients with suboptimal control58 Consequently currentguidelines recommend the use of cabergoline in patients withinadequate response to other medical treatment with highestbenefit expected in cases with modest persistent hormonal ele-vations26 Conflicting data exists as to whether the co-secretionof prolactin is predictive of response to dopamine agonist ther-apy Some studies conclude that tumors that co-secrete prolac-tin and GH have a greater response to dopamine agonisttherapy than those than solely secrete GH whereas othersshow no effect There remains little data available regardingtumor shrinkage in patients with acromegaly who are receivingdopamine agonist therapy59 Jaffe et al57 reported combined re-sults from a number of studies which revealed that 29 of pa-tients had some tumor shrinkage on dopamine agonist therapyand the majority of patients who had tumor shrinkage werealso hyperprolactinemic It is difficult to interpret these findinggiven the small number and heterogeneous characteristics ofthe patients included
The most frequent adverse effects of dopamine agonist ther-apy are nausea constipation headache mood disturbancenasal stuffiness and dizziness Cardiac valve abnormalitieswere described with high doses of cabergoline used inParkinsonrsquos disease but not with current recommended dosageused for patients with acromegaly60
DopastatinBIM-23A760 is a chimeric molecule hasbeen shown in vitro to have high affinity for both somatosta-tin receptor subtypes- 2 and 5 in addition to dopamine 2 recep-tor61 With increasing knowledge of the importance of SSR5 inregulation of GH in GH-secreting adenomas dopastatin isundergoing further development in clinical studies to deter-mine if there is a role for these compounds in the treatment ofacromegaly
Radiotherapy
Radiation therapy is used as adjuvant treatment in the settingof persistent disease despite surgery andor medical treatmentor if medical therapy is unavailable unsuccessful or not toler-ated Radiotherapy has been shown to be effective in loweringserum GH levels36 but conflicting results have been reported re-garding the normalization of IGF-1 levels62 Furthermore thedelay in therapeutic benefit and the high risk of developinghypopituitarism serve as arguments against the more routineuse of radiotherapy
Conventional radiotherapy has been used for gt30 years inthe adjunctive treatment of pituitary adenomas It is generallydelivered in fractionated doses 4ndash5 times per week so as to re-duce daily-fractionated dose The risk of adverse effects beingproportional to maximal dose per day63 Early studies of con-ventional radiotherapy reported high efficacy rate of 80ndash100however remission was defined as a GH level below 5-10 ngmlMore recent studies using revised biochemical remission tar-gets report a mean remission rate between 50 and 60 Jenkinset al64 assessed the effects of conventional pituitary irradiationin 884 patients of the UK National Acromegaly Register MeanGH levels declined from 135 to 53 ngml at 2 years after surgeryto 2 ngml by 10 years and a further decline to 11 ngml at 20years (Figure 2) Furthermore they observed a parallel fall in IGF-
Figure 1 Baseline and lowest values of individual serum insulin-like growth factor-1 concentrations achieved in 90 patients treated for 12 months or more with daily
pegvisomant (daggerPlt005 vs baseline DaggerPlt001 vs baseline) The shaded area represents the age-adjusted normal range for insulin-like growth factor-155
R Dineen et al | 417
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
1 levels with 63 of patients having a normal level by 10years64
Stereotactic radiotherapy offers improvement in immobil-ization imaging and treatment delivery from conventionaltechniques It can be delivered as a single fraction radiosurgeryusing a Gamma knife (a source of cobalt) or a linear acceleratoror a stereotactic conformal radiotherapy delivered as fractio-nated treatment using a linear accelerator There is no clear ad-vantage for either of the radiosurgical techniques in terms ofsparing normal tissue receiving high doses of radiation65 A crit-ical analysis of the literature reported variable rates of both bio-chemical and tumor response 17ndash82 and 37ndash100respectively66 The authors attributed the wide variability to theuse of different treatment schedules and definitions ofremission
Hypopituitarism is less frequent with radiosurgery than con-ventional radiotherapy At least 50 of patient treated with con-ventional radiotherapy will have acquired new anteriorpituitary hormonal deficits at 10 years67 In cohorts treatedsolely with stereotactic techniques rates of hypopituitarismvary between 0 and 2068 However it is likely that the candi-dates for stereotactic radiotherapy had smaller remnants of dis-ease and therefore less normal tissue irradiated
Annual hormonal testing is required due to the risk of latehypopituitarism26 Other complications following radiotherapyinclude the risk of second brain tumors stroke and rarely opticneuropathy cranial nerve deficits and radionecrosis a rare ad-verse effect of gamma knife radiotherapy69ndash71
Patients treated with conventional radiotherapy have beenreported to have increased mortality predominantly due tostroke independent of GHIGF-I levels and hypopituitarism20
Current guidelines recommend the use of stereotactic radio-therapy over conventional radiation therapy unless significantresidual tumor burden or the lesion is too close to the opticchiasm26
Conclusion
Prolonged exposure to elevated endogenous levels of GH andIGF-I results in a multisystem disease characterized by somaticovergrowth multiple co-morbidities and premature mortalityEarly detection prevents the development of irreversible com-plications of the disease including cardiomyopathy respiratory
dysfunction and arthropathy Despite the imprecision of assaysfor GH and IGF-I it is clear from epidemiologic studies that tightbiochemical control is essential to reduce morbidity controlsymptoms and improve mortality rates
Optimal implementation of current guidelines in routine clin-ical practice and maximal use of the medical treatment could im-prove the long-term control of patients with significant benefitsfor morbidity and mortality Another important aspect in thetreatment of patients with acromegaly is also the appropriate tar-geted treatment of co-morbidities associated with acromegaly
Achievement of the criteria for cure during or after therapyis determined by assessing biochemical control targeting con-trolled levels of GH and normalization of IGF-I levels monitor-ing tumor size assessing residual pituitary function andmonitoring co-morbidities
New therapeutic molecules currently in trials will hopefullyoffer further benefit to those patients resistant to current thera-peutic modes for this chronic progressive disorder
Conflict of interest None declared
References1 Melmed S Braunstein GD Horvath E Ezrin C Kovacs K
Pathophysiology of acromegaly Endocr Rev 1983 4271ndash902 Mestron A Webb SM Astorga R Benito P Catala M
Gaztambide S et al Epidemiology clinical characteristicsoutcome morbidity and mortality in acromegaly based onthe Spanish Acromegaly Registry (Registro Espanol deAcromegalia REA) Eur J Endocrinol 2004 151439ndash46
3 Jagannathan J Dumont AS Prevedello DM Oskouian RJLopes B Jane JA Jr and Laws ER Jr Genetics of pituitary aden-omas current theories and future implications NeurosurgFocus 2005 19E4
4 Zhu X Lin CR Prefontaine CG Tollkuhn J Rosenfeld MGGenetic control of pituitary developement and hypopituitar-ism Curr Opin Genet Dev 2005 15332ndash40
5 Melmed S Acromegaly pathogenesis and treatment J ClinInvest 2009 1193189ndash202
6 Colao A Ferone D Marzullo P Lombardi G Systemic compli-cations of acromegaly epidemiology pathogenesis andmanagement Endocr Rev 2004 25102ndash52
7 Korbonits M Gadelha MR Roncaroli F Grossman AB Ellard SEvanson J et al Landscape of familial isolated and young-onset pituitary adenomas prospective diagnosis in AIP mu-tation carriers J Clin Endocrinol Metab 2015 100E1242ndash54
8 Larkin S Reddy R Karavitaki N Cudlip S Wass J Ansorge OGranulation pattern but not GSP or GHR mutation is associ-ated with clinical characteristics in somatostatin-naive pa-tients with somatotroph adenomas Eur J Endocrinol 2013168491ndash9
9 Molitch ME Clinical manifestations of acromegaly EndocrinolMetab Clin North Am 1992 21597ndash614
10Reid TJ Post KD Bruce JN Nabi KM Reyes-Vidal CM et alFeatures at diagnosis of 324 patients with acromegaly didnot change from 1981 to 2006 acromegaly remains under-recognized and under-diagnosed Clin Endocrinol 201072203ndash8
11Moslashller N Joslashrgensen JO Abildgard N Orskov L Schmitz OChristiansen JS Effects of growth hormone on glucose me-tabolism Horm Res 1991 36 (Suppl 1)32ndash5
12Dreval AV Trigolosova IV Misnikova IV Kovalyova YATishenina RS Barsukov IA et al Prevalence of diabetes melli-tus in patients with acromegaly Endocr Connect 2014 393ndash8
Figure 2 Percentage of all patients achieving a serum GH level lt25 ngml (bars)
and the mean GH level (line) in the years after pituitary irradiation64
418 | QJM An International Journal of Medicine 2017 Vol 110 No 7
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
13Roemmler J Gutt B Fischer R Vay S Wiesmeth ABidlingmaier M et al Elevated incidence of sleep apnoea inacromegaly-correlation to disease activity Sleep Breath 2012161247ndash53
14Killinger Z Payer J Lazurova I Imrich R Homerova Z KuzmaM et al Arthropathy in acromegaly Rheum Dis Clin North Am2010 36713ndash20
15Kameyama S Tanaka R Hasegawa A Tamura T Kuroki MSubclinical carpal tunnel syndrome in acromegaly NeurolMed Chir 1993 33547ndash51
16Mazziotti G Biagioli E Maffezzoni F Spinello M Serra VMaroldi R et al Bone turnover bone mineral density and frac-ture risk in acromegaly a meta-analysis J Clin EndocrinolMetab 2015 100384ndash94
17Renehan AG OrsquoConnell J OrsquoHalloran D Shanahan F PottenCS OrsquoDwyer ST et al Acromegaly and colorectal cancer acomprehensive review of epidemiology biological mechan-isms and clinical implications Horm Metab Res 200335712ndash25
18Orme S McNally RJ Cartwright RA Belchetz PE Mortality andcancer incidence in acromegaly a restrospective cohortstudy J Clin Endocrinol Metab 1998 832730ndash4
19Petroff D Teuroonjes A Grussendorf M Droste M Dimopoulou CStalla G et al The Incidence of cancer among acromegaly pa-tients results from the German Acromegaly Registry J ClinEndocrinol Metab 2015 1003894ndash902
20Sherlock M Ayuk J Tomlinson JW Toogood AA Aragon-Alonso A Sheppard MC et al Mortality in patients with pitu-itary disease Endocr Rev 2010 31301ndash42
21Bates AS Vanrsquot H Jones JM Clayton RN An audit of outcomeof treatment in acromegaly Q J Med 1993 86293ndash9
22Ayuk J Clayton RN Holder G Sheppard MC Stewart PMBates AS Growth hormone and pituitary radiotherapy butnot serum insulin-like growth factor-I concentrations pre-dict excess mortality in patients with acromegaly J ClinEndocrinol Metab 2004 891613ndash7
23Kauppinen-Meuroakelin R Sane T Reunanen A Veuroalimeuroaki MJNiskanen L Markkanen H et al A nationwide survey of mor-tality in acromegaly J Clin Endocrinol Metab 2005 904081ndash6
24Holdaway IM Bolland MJ Gamble GD A meta-analysis of theeffect of lowering serum levels of GH and IGF-I on mortalityin acromegaly Eur J Endocrinol 2008 15989ndash95
25Rosen T Bengtsson BA Premature mortality due to cardio-vascular disease in hypopituitarism Lancet 1990 336285ndash8
26Katznelson L Laws ER Jr Melmed S Molitch ME Murad MHUtz A et al Acromegaly an endocrine society clinical practiceguideline J Clin Endocrinol Metab 2014 993933ndash51
27Freda PU Post KD Powell JS Wardlaw SL Evaluation of dis-ease status with sensitive measures of growth hormone se-cretion in 60 postoperative patients with acromegaly J ClinEndocrinol Metab 1998 833808ndash16
28Dimaraki EV Jaffe CA DeMott-Friberg R Chandler WFBarkan AL Acromegaly with apparently normal GH secretionimplications for diagnosis and follow-up J Clin EndocrinolMetab 2002 873537ndash42
29Losa M Von Werder K Pathophysiology and clinical aspectsof the ectopic GH-releasing hormone syndrome ClinEndocrinol 1997 47123ndash35
30Dobrashian RD OrsquoHalloran DJ Hunt A Beardwell CG ShaletSM Relationships between insulin-like growth factor-1 levelsand growth hormone concentrations during diurnal profilesand following oral glucose in acromegaly Clin Endocrinol 199338589ndash93
31Frank G Pasquini E Farneti G Mazzatenta D Sciarretta VGrasso V et al The endoscopic versus the traditional ap-proach in pituitary surgery Neuroendocrinology 2006 83240ndash8
32Marquez Y Tuchman A Zada G Surgery and radiosurgery foracromegaly a review of indications operative techniquesoutcomes and complications Int J Endocrinol 2012 2012386ndash401
33Laws ER Vance ML Thapar K Pituitary surgery for the man-agement of acromegaly Horm Res 2000 5371ndash5
34Salaun C Foubert L Vialatou M Kujas M Turpin G Prognosticfactors of surgical cure of growth hormone secreting pituitary aden-omas Ann Medecine Interne 1999 150195ndash8
35Kreutzer J Vance ML Lopes MB Laws ER Jr Surgical manage-ment of GH-secreting pituitary adenomas an outcome studyusing modern remission criteria J Clin Endocrinol Metab 2001864072ndash7
36Annamalai AK Webb A Kandasamy N Elkhawad M Moir SKhan F et al A comprehensive study of clinical biochemicalradiological vascular cardiac and sleep parameters in anunselected cohort of patients with acromegaly undergoingpresurgical somatostatin receptor ligand therapy J ClinEndocrinol Metab 2013 981040ndash50
37Shen M Shou X Wang Y Zhang Z Wu J Mao Y et al Effect ofpresurgical long-acting octreotide treatment in acromegalypatients with invasive pituitary macroadenomas a prospect-ive randomized study Endocr J 2010 571035ndash44
38Friedel ME Johnston D Singhal S Al Khalili K Farrell CJEvans JJ et al Airway management and perioperative con-cerns in acromegaly patients undergoing endoscopic trans-sphenoidal surgery for pituitary tumors Otolaryngol HeadNeck Surg 2013 149840ndash4
39Bhayana S Booth G Asa SL Kovacs Ezzat S The implicationof somatotroph adenoma phenotype to somatostatin analogresponsiveness in acromegaly J Clin Endocrinol Metab 2005906290ndash5
40Reisine T Bell GI Molecular biology of somatostatin recep-tors Endocr Rev 1995 16427ndash42
41Zatelli MC Piccin D Tagliati F et al Dopamine receptor sub-type 2 and somatostatin receptor subtype 5 expression influ-ences somatostatin analog effects on human somatotrophpituitary adenomas in vitro J Mol Endocrinol 2005 35333ndash41
42Murray RD Melmed S A critical analysis of clinically avail-able somatostatin analog formulations for therapy of acro-megaly J Clin Endocrinol Metab 2008 932957ndash68
43Freda PU Katznelson L Van der Lely A Reyes CM Zhao SRabinowitz D Long-acting somatostatin analog therapy ofacromegaly a meta-analysis J Clin Endocrinol Metab 2005904465ndash74
44Howlett TA Willis D Walker G Wass JA Trainer PJ Control ofgrowth hormone and IGF1 in patients with acromegaly in theUK responses to medical treatment with somatostatin ana-logues and dopamine agonists Clin Endocrinol 201379689ndash99
45Espinosa de los Monteros AL Carrasco C Albarran AAGadelha M Abreu A Mercado M The role of primary pharma-cological therapy in acromegaly Pituitary 2014 17 (Suppl1)S4ndashS10
46Colao AM Auriemma RS Pivonello R The effects of somato-statin analogue therapy on pituitary tumor volume in pa-tients with acromegaly Pituitary 2016 19210ndash21
47Sathyapalan T Lowry M Turnbull LW Rowland-Hill C AtkinSL Mechanism of action of octreotide in acromegalic tu-mours in vivo using dynamic contrast-enhanced magneticresonance imaging Pituitary 2007 10233ndash6
R Dineen et al | 419
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
48Giustina A Mazziotti G Torri V Spinello M Floriani IMelmed S Meta-analysis on the effects of octreotide ontumor mass in acromegaly PLoS One 2012 7e36411
49Abu Dabrh AM Mohammed K Asi N Farah WH Wang ZFarah MH et al Surgical interventions and medical treat-ments in treatment-naive patients with acromegaly system-atic review and meta-analysis J Clin Endocrinol Metab 2014994003ndash14
50Colao A Bronstein M Freda P Gu F Shen C-C Gadelha Met al Pasireotide versus octreotide in acromegaly a head-to-head superiority study J Clin Endocrinol Metab 2014 99791ndash9
51Schmid HA Schoeffter P Functional activity of the multili-gand analog SOM230 at human recombinant somatostatinreceptor subtypes supports its usefulness in neuroendocrinetumors Neuroendocrinology 2004 80 (Suppl 1)47ndash50
52Mazziotti G Floriani I Bonadonna S Torri V Chanson PGiustina A Effects of somatostatin analogs on glucosehomeostasis a metaanalysis of acromegaly studies J ClinEndocrinol Metab 2009 941500ndash8
53Higham CE Trainer PJ Growth hormone excess and the de-velopment of growth hormone receptor antagonists ExpPhysiol 2008 931157ndash69
54Trainer PJ Drake WM Katznelson L et al Treatment of acro-megaly with the growth hormone receptor antagonist pegvi-somant N Engl J Med 2000 3421171ndash7
55Van der Lely AJ Hutson RK Trainer PJ Besser GM Barkan ALKatznelson L et al Long-term treatment of acromegaly withpegvisomant a growth hormone receptor antagonist Lancet2001 3581754ndash9
56Buchfelder M Weigel D Droste M Mann K Saller B BrubachK et al Pituitary tumor size in acromegaly during pegvisom-ant treatment experience from MR re-evaluations of theGerman Pegvisomant Observational Study Eur J Endocrinol2009 16127ndash35
57 Jaffe CA Barkan AL Treatment of acromegaly with dopamineagonists Endocrinol Metab Clin North Am 1992 21713ndash35
58Sandret L Maison P Chanson P Place of cabergoline in acro-megaly a meta-analysis J Clin Endocrinol Metab 2011961327ndash35
59Sherlock M Woods C Sheppard C Medical therapy in acro-megaly Nat Rev Endocrinol 2011 7291ndash300
60Samson SL Ezzat S AACEACE disease state clinical reviewdopamine agonists for hyperprolactinemia and the risk ofcardiac valve disease Endocr Pract 2014 20608ndash16
61 Jaquet P Gunz G Saveanu A Dufour H Taylor J Dong J et alEfficacy of chimeric molecules directed towards multiplesomatostatin and dopamine receptors on inhibition of GHand prolactin secretion from GH-secreting pituitary aden-omas classified as partially responsive to somatostatin ana-log therapy Eur J Endocrinol 2005 153135ndash41
62Barkan AL Halasz I Dornfeld KJ Jaffe CA Friberg RDChandler WF et al Pituitary irradiation is ineffective in nor-malizing plasma insulin-like growth factor I in patients withacromegaly J Clin Endocrinol Metab 1997 823187ndash91
63Eastman RC Gorden P Glatstein E Roth J Radiation therapyof acromegaly Endocrinol Metab Clin North Am 199221693ndash712
64 Jenkins PJ Bates Carson MN Stewart PM Wass JAConventional pituitary irradiation is effective in loweringserum growth hormone and insulin-like growth factor-I inpatients with acromegaly J Clin Endocrinol Metab 2006911239ndash45
65Minniti G Gilbert DC Brada M Modern techniques for pituit-ary radiotherapy Rev Endocr Metab Disord 2008 10135ndash44
66Stapleton CJ Liu CY Weiss M The role of stereotactic radio-surgery in the multimodal management of growth hormone-secreting pituitary adenomas Neurosurg Focus 2010 29E11
67Biermasz NR van Dulken H Roelfsema F Long-term follow-up results of postoperative radiotherapy in 36 patients withacromegaly J Clin Endocrinol Metab 2000 852475ndash82
68Attanasio R Epaminonda P Motti E Giugni E Ventrella LCozzi R et al Gamma-knife radiosurgery in acromegaly a 4-year follow-up study J Clin Endocrinol Metab 2003 883105ndash12
69Minniti G Traish D Ashley S Gonsalves A Brada M Risk ofsecond brain tumor after conservative surgery and radiother-apy for pituitary adenoma update after an additional 10years J Clin Endocrinol Metab 2005 90800ndash4
70Brada M Burchell L Ashley S Traish D The incidence of cere-brovascular accidents in patients with pituitary adenoma IntJ Radiat Oncol Biol Phys 1999 45693ndash8
71Laws ER Sheehan JP Sheehan JM Jagnathan J Jane JA JrOskouian R Stereotactic radiosurgery for pituitary aden-omas a review of the literature J Neurooncol 2004 69257ndash72
420 | QJM An International Journal of Medicine 2017 Vol 110 No 7
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022

dose is 90 mg monthly with a maximum dose up to 120 mgmonthly26
A large body of evidence supports the efficacy of long -actingSRL therapy In a critical analysis of the largest studies octreo-tide LAR reduced GH tolt25 lgl and normalized the IGF-1 levelsin 66 and 63 respectively42 Similar targets were achievedwith lanreotide-SR in 52 and 47 of cases respectively An ear-lier meta-analysis by Freda et al43 reported the overall chance ofIGF-1 normalization was 67 with octreotide and 47 with lan-reotide SR The higher efficacy reported with octreotide may beaccounted by pre-selection of responsive cases (patients whoshowed response to short acting octreotide only being recruitedto studies) inclusion of both primary and secondary therapycases and small case series An inherent challenge to meta-analyses in such a complex condition is the lack of standardiza-tion of GH and IGF-1 assays making comparison of absolutevalues between studies impossible
Smaller tumors lower baseline GH and IGF-1 levels44 highSSR2 and SSR5 expression45 and those previously treated withsurgery are associated with a better response to SRL treatmentRoutine performance of somatostatin receptor scintigraphy oran acute GH response to a subcutaneous octreotide injection asa determinant of SRL response are not recommended26
Somatostatin receptor ligands also have proven efficacy intumor volume reduction This has been extensively reviewedrecently by Colao et al46 Tumor reduction may be mediated bydirect anti-proliferative effects via activation of somatostatinreceptors or indirectly through angiogenesis inhibitionSathyapalan et al47 showed a significant reduction in the func-tional vascularity of pituitary tumors in a small study of five pa-tients after 24 weeks of octreotide therapy
Published meta-analysis revealed that octreotide LAR andlanreotide formulation induce tumor shrinkage in 660 and328 of cases respectively4849 Tumor reduction is progressivewith prolonged treatment and decreased IGF-1 levels may beits best predictor followed by age and degree of GH decrease
A recent detailed review of published studies evaluatingsomatostatin analogues as first line therapy showed that 6-24months of octreotide LAR therapy achievedgt20-30 tumor vol-ume reduction in 73-85 of patients Unlike surgery primarymedical therapy cannot cure acromegaly Based on a recentmeta-analysis of available studies primary SRL therapy is asso-ciated with a lower remission rates compared to initial surgery(45 vs 67)49 However the accuracy of these remission ratesis questionable given the non-comparable nature and the het-erogeneity of studies included Primary SRL therapy can beoffered before surgery in patients with contraindications incases with unresectable tumor or with severe comorbidities26
During SRL treatment the most frequent side effects includeabdominal discomfort flatulence cramps and diarrheaGallbladder sludge or gallstones occur in 25 of subjects butare usually asymptomatic SRL treatment was initially thoughtto aggravate the increased risk of glucose intolerance in thesepatients but the overall effect on glucose metabolism is not clin-ically significant50
Pasireotide is a multireceptor-targeted somatostatin recep-tor ligand which has higher functional activity than octreotideon SSR subtypes except type 4 but in particular SSR551 In alarge phase III randomized trial in patients with acromegalywho were naive to medical therapy pasireotide LAR and octreo-tide LAR have a similar effect of tumor reduction despite thefact that pasireotide was superior to octreotide in providing bio-chemical control After 12 months of treatment 81 of pasireo-tide patients had20 reduction in tumor volume compared
with 77 of octreotide LAR patients52 Pasireotide has similarrates of gastrointestinal side effects to other SRLs however therates of hyperglycemia are significantly higher (occurring in 31ndash57 of patients)
Pegvisomant
Pegvisomant is a pegylated recombinant analog of human GHincorporating nine amino acid mutations Pegylation extendsthe half-life by reducing renal clearance53 The mutations resultin increased affinity to the GH receptor in addition to blockingthe second binding site on the receptor preventing GHR dimer-ization and signal transduction GH hypersecretion persists asit does not target the GH secreting tumor at the level of the pitu-itary hence GH measurements cannot be used to monitor dis-ease activity and IGF-1 becomes the sole marker to monitorbiochemical response during therapy
Pegvisomant has been shown to be highly effective in pro-viding biochemical control of acromegaly in multiple studies Ina 12-week double-blind placebo controlled study Trainer et al54
randomly assigned patients to receive placebo 10 15 or 20 mgof pegvisomant Normalization of IGF-1 (using age and sex-matched reference ranges) was achieved in 10 54 81 and89 respectively Symptom control was also observed The effi-cacy of pegvisomant over a longer period was subsequentlystudied Van der Lely et al55 reported 97 of patients achievingnormal IGF-1 levels in patients receiving therapy for 12 monthsor more (Figure 1) Dose reduction was required in 1190 pa-tients as IGF-1 levels dropped below normal reference range forage and sex
As mentioned above pegvisomant does not exert a centraleffect on pituitary GH secretion hence fears exist over the pos-sibility of increased tumor growth The German PegvisomantObservational Study is a multicenter surveillance study com-menced in 2004 to assess the efficacy and safety of pegvisomanttherapy in patients with acromegaly56 Neuroradiological moni-toring of tumor extension is performed with MRI imagingBuchfelder et al studied 3 years of follow-up data of 307 pa-tients Tumor progression was reported in between 2 and3 ofpatients treated an increase not outside the expected rate inpatients not treated with pegvisomant
Pegvisomant is administered as daily subcutaneous injec-tion It is generally well tolerated with adverse effects reportedinlt10 of patients These may include injection site reactionswith reversible lipohypertrophy and deranged liver functiontests (attributable to the polyethylene glycol pegylated vehicle)
The predominant limiting factor for use of this agent in clin-ical practice remains its considerable cost It is most often usedas a second line agent in cases resistant or intolerant to SRLtherapy or in combination with SRLrsquos in partially resistantcases It is also a potential treatment option in acromegaly pa-tients with difficult to control diabetes mellitus due to its favor-able effect on glycemic control
Dopamine agonists
Dopamine agonists bind to the D2 dopamine receptors in the pi-tuitary gland and suppress prolactin and GH secretion The useof bromocriptine a first-generation dopamine agonist is lim-ited by its side effect profile including GI symptoms lethargyand orthostatic hypotension It also compares poorly with som-atostatin receptor ligands in terms of efficacy with normaliza-tion of GHIGF-1 reported in only 10 of patients57
416 | QJM An International Journal of Medicine 2017 Vol 110 No 7
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
Cabergoline an ergot derivative dopamine agonist has beenused for decades in the treatment of hyperprolactinaemia andParkinsonrsquos disease Cabergoline is better tolerated and more ef-fective than bromocriptine however its use was superseded bythe development of SRL therapy showing higher efficacy rates
Clinical trials of cabergoline in acromegaly are small non-randomized and report variable results In a recent systematicreview of 10 trials with a total of 150 acromegaly patients con-trol of acromegaly was achieved in 34 of patients who receivedcabergoline therapy alone and 52 when added to SRL therapyin patients with suboptimal control58 Consequently currentguidelines recommend the use of cabergoline in patients withinadequate response to other medical treatment with highestbenefit expected in cases with modest persistent hormonal ele-vations26 Conflicting data exists as to whether the co-secretionof prolactin is predictive of response to dopamine agonist ther-apy Some studies conclude that tumors that co-secrete prolac-tin and GH have a greater response to dopamine agonisttherapy than those than solely secrete GH whereas othersshow no effect There remains little data available regardingtumor shrinkage in patients with acromegaly who are receivingdopamine agonist therapy59 Jaffe et al57 reported combined re-sults from a number of studies which revealed that 29 of pa-tients had some tumor shrinkage on dopamine agonist therapyand the majority of patients who had tumor shrinkage werealso hyperprolactinemic It is difficult to interpret these findinggiven the small number and heterogeneous characteristics ofthe patients included
The most frequent adverse effects of dopamine agonist ther-apy are nausea constipation headache mood disturbancenasal stuffiness and dizziness Cardiac valve abnormalitieswere described with high doses of cabergoline used inParkinsonrsquos disease but not with current recommended dosageused for patients with acromegaly60
DopastatinBIM-23A760 is a chimeric molecule hasbeen shown in vitro to have high affinity for both somatosta-tin receptor subtypes- 2 and 5 in addition to dopamine 2 recep-tor61 With increasing knowledge of the importance of SSR5 inregulation of GH in GH-secreting adenomas dopastatin isundergoing further development in clinical studies to deter-mine if there is a role for these compounds in the treatment ofacromegaly
Radiotherapy
Radiation therapy is used as adjuvant treatment in the settingof persistent disease despite surgery andor medical treatmentor if medical therapy is unavailable unsuccessful or not toler-ated Radiotherapy has been shown to be effective in loweringserum GH levels36 but conflicting results have been reported re-garding the normalization of IGF-1 levels62 Furthermore thedelay in therapeutic benefit and the high risk of developinghypopituitarism serve as arguments against the more routineuse of radiotherapy
Conventional radiotherapy has been used for gt30 years inthe adjunctive treatment of pituitary adenomas It is generallydelivered in fractionated doses 4ndash5 times per week so as to re-duce daily-fractionated dose The risk of adverse effects beingproportional to maximal dose per day63 Early studies of con-ventional radiotherapy reported high efficacy rate of 80ndash100however remission was defined as a GH level below 5-10 ngmlMore recent studies using revised biochemical remission tar-gets report a mean remission rate between 50 and 60 Jenkinset al64 assessed the effects of conventional pituitary irradiationin 884 patients of the UK National Acromegaly Register MeanGH levels declined from 135 to 53 ngml at 2 years after surgeryto 2 ngml by 10 years and a further decline to 11 ngml at 20years (Figure 2) Furthermore they observed a parallel fall in IGF-
Figure 1 Baseline and lowest values of individual serum insulin-like growth factor-1 concentrations achieved in 90 patients treated for 12 months or more with daily
pegvisomant (daggerPlt005 vs baseline DaggerPlt001 vs baseline) The shaded area represents the age-adjusted normal range for insulin-like growth factor-155
R Dineen et al | 417
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
1 levels with 63 of patients having a normal level by 10years64
Stereotactic radiotherapy offers improvement in immobil-ization imaging and treatment delivery from conventionaltechniques It can be delivered as a single fraction radiosurgeryusing a Gamma knife (a source of cobalt) or a linear acceleratoror a stereotactic conformal radiotherapy delivered as fractio-nated treatment using a linear accelerator There is no clear ad-vantage for either of the radiosurgical techniques in terms ofsparing normal tissue receiving high doses of radiation65 A crit-ical analysis of the literature reported variable rates of both bio-chemical and tumor response 17ndash82 and 37ndash100respectively66 The authors attributed the wide variability to theuse of different treatment schedules and definitions ofremission
Hypopituitarism is less frequent with radiosurgery than con-ventional radiotherapy At least 50 of patient treated with con-ventional radiotherapy will have acquired new anteriorpituitary hormonal deficits at 10 years67 In cohorts treatedsolely with stereotactic techniques rates of hypopituitarismvary between 0 and 2068 However it is likely that the candi-dates for stereotactic radiotherapy had smaller remnants of dis-ease and therefore less normal tissue irradiated
Annual hormonal testing is required due to the risk of latehypopituitarism26 Other complications following radiotherapyinclude the risk of second brain tumors stroke and rarely opticneuropathy cranial nerve deficits and radionecrosis a rare ad-verse effect of gamma knife radiotherapy69ndash71
Patients treated with conventional radiotherapy have beenreported to have increased mortality predominantly due tostroke independent of GHIGF-I levels and hypopituitarism20
Current guidelines recommend the use of stereotactic radio-therapy over conventional radiation therapy unless significantresidual tumor burden or the lesion is too close to the opticchiasm26
Conclusion
Prolonged exposure to elevated endogenous levels of GH andIGF-I results in a multisystem disease characterized by somaticovergrowth multiple co-morbidities and premature mortalityEarly detection prevents the development of irreversible com-plications of the disease including cardiomyopathy respiratory
dysfunction and arthropathy Despite the imprecision of assaysfor GH and IGF-I it is clear from epidemiologic studies that tightbiochemical control is essential to reduce morbidity controlsymptoms and improve mortality rates
Optimal implementation of current guidelines in routine clin-ical practice and maximal use of the medical treatment could im-prove the long-term control of patients with significant benefitsfor morbidity and mortality Another important aspect in thetreatment of patients with acromegaly is also the appropriate tar-geted treatment of co-morbidities associated with acromegaly
Achievement of the criteria for cure during or after therapyis determined by assessing biochemical control targeting con-trolled levels of GH and normalization of IGF-I levels monitor-ing tumor size assessing residual pituitary function andmonitoring co-morbidities
New therapeutic molecules currently in trials will hopefullyoffer further benefit to those patients resistant to current thera-peutic modes for this chronic progressive disorder
Conflict of interest None declared
References1 Melmed S Braunstein GD Horvath E Ezrin C Kovacs K
Pathophysiology of acromegaly Endocr Rev 1983 4271ndash902 Mestron A Webb SM Astorga R Benito P Catala M
Gaztambide S et al Epidemiology clinical characteristicsoutcome morbidity and mortality in acromegaly based onthe Spanish Acromegaly Registry (Registro Espanol deAcromegalia REA) Eur J Endocrinol 2004 151439ndash46
3 Jagannathan J Dumont AS Prevedello DM Oskouian RJLopes B Jane JA Jr and Laws ER Jr Genetics of pituitary aden-omas current theories and future implications NeurosurgFocus 2005 19E4
4 Zhu X Lin CR Prefontaine CG Tollkuhn J Rosenfeld MGGenetic control of pituitary developement and hypopituitar-ism Curr Opin Genet Dev 2005 15332ndash40
5 Melmed S Acromegaly pathogenesis and treatment J ClinInvest 2009 1193189ndash202
6 Colao A Ferone D Marzullo P Lombardi G Systemic compli-cations of acromegaly epidemiology pathogenesis andmanagement Endocr Rev 2004 25102ndash52
7 Korbonits M Gadelha MR Roncaroli F Grossman AB Ellard SEvanson J et al Landscape of familial isolated and young-onset pituitary adenomas prospective diagnosis in AIP mu-tation carriers J Clin Endocrinol Metab 2015 100E1242ndash54
8 Larkin S Reddy R Karavitaki N Cudlip S Wass J Ansorge OGranulation pattern but not GSP or GHR mutation is associ-ated with clinical characteristics in somatostatin-naive pa-tients with somatotroph adenomas Eur J Endocrinol 2013168491ndash9
9 Molitch ME Clinical manifestations of acromegaly EndocrinolMetab Clin North Am 1992 21597ndash614
10Reid TJ Post KD Bruce JN Nabi KM Reyes-Vidal CM et alFeatures at diagnosis of 324 patients with acromegaly didnot change from 1981 to 2006 acromegaly remains under-recognized and under-diagnosed Clin Endocrinol 201072203ndash8
11Moslashller N Joslashrgensen JO Abildgard N Orskov L Schmitz OChristiansen JS Effects of growth hormone on glucose me-tabolism Horm Res 1991 36 (Suppl 1)32ndash5
12Dreval AV Trigolosova IV Misnikova IV Kovalyova YATishenina RS Barsukov IA et al Prevalence of diabetes melli-tus in patients with acromegaly Endocr Connect 2014 393ndash8
Figure 2 Percentage of all patients achieving a serum GH level lt25 ngml (bars)
and the mean GH level (line) in the years after pituitary irradiation64
418 | QJM An International Journal of Medicine 2017 Vol 110 No 7
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
13Roemmler J Gutt B Fischer R Vay S Wiesmeth ABidlingmaier M et al Elevated incidence of sleep apnoea inacromegaly-correlation to disease activity Sleep Breath 2012161247ndash53
14Killinger Z Payer J Lazurova I Imrich R Homerova Z KuzmaM et al Arthropathy in acromegaly Rheum Dis Clin North Am2010 36713ndash20
15Kameyama S Tanaka R Hasegawa A Tamura T Kuroki MSubclinical carpal tunnel syndrome in acromegaly NeurolMed Chir 1993 33547ndash51
16Mazziotti G Biagioli E Maffezzoni F Spinello M Serra VMaroldi R et al Bone turnover bone mineral density and frac-ture risk in acromegaly a meta-analysis J Clin EndocrinolMetab 2015 100384ndash94
17Renehan AG OrsquoConnell J OrsquoHalloran D Shanahan F PottenCS OrsquoDwyer ST et al Acromegaly and colorectal cancer acomprehensive review of epidemiology biological mechan-isms and clinical implications Horm Metab Res 200335712ndash25
18Orme S McNally RJ Cartwright RA Belchetz PE Mortality andcancer incidence in acromegaly a restrospective cohortstudy J Clin Endocrinol Metab 1998 832730ndash4
19Petroff D Teuroonjes A Grussendorf M Droste M Dimopoulou CStalla G et al The Incidence of cancer among acromegaly pa-tients results from the German Acromegaly Registry J ClinEndocrinol Metab 2015 1003894ndash902
20Sherlock M Ayuk J Tomlinson JW Toogood AA Aragon-Alonso A Sheppard MC et al Mortality in patients with pitu-itary disease Endocr Rev 2010 31301ndash42
21Bates AS Vanrsquot H Jones JM Clayton RN An audit of outcomeof treatment in acromegaly Q J Med 1993 86293ndash9
22Ayuk J Clayton RN Holder G Sheppard MC Stewart PMBates AS Growth hormone and pituitary radiotherapy butnot serum insulin-like growth factor-I concentrations pre-dict excess mortality in patients with acromegaly J ClinEndocrinol Metab 2004 891613ndash7
23Kauppinen-Meuroakelin R Sane T Reunanen A Veuroalimeuroaki MJNiskanen L Markkanen H et al A nationwide survey of mor-tality in acromegaly J Clin Endocrinol Metab 2005 904081ndash6
24Holdaway IM Bolland MJ Gamble GD A meta-analysis of theeffect of lowering serum levels of GH and IGF-I on mortalityin acromegaly Eur J Endocrinol 2008 15989ndash95
25Rosen T Bengtsson BA Premature mortality due to cardio-vascular disease in hypopituitarism Lancet 1990 336285ndash8
26Katznelson L Laws ER Jr Melmed S Molitch ME Murad MHUtz A et al Acromegaly an endocrine society clinical practiceguideline J Clin Endocrinol Metab 2014 993933ndash51
27Freda PU Post KD Powell JS Wardlaw SL Evaluation of dis-ease status with sensitive measures of growth hormone se-cretion in 60 postoperative patients with acromegaly J ClinEndocrinol Metab 1998 833808ndash16
28Dimaraki EV Jaffe CA DeMott-Friberg R Chandler WFBarkan AL Acromegaly with apparently normal GH secretionimplications for diagnosis and follow-up J Clin EndocrinolMetab 2002 873537ndash42
29Losa M Von Werder K Pathophysiology and clinical aspectsof the ectopic GH-releasing hormone syndrome ClinEndocrinol 1997 47123ndash35
30Dobrashian RD OrsquoHalloran DJ Hunt A Beardwell CG ShaletSM Relationships between insulin-like growth factor-1 levelsand growth hormone concentrations during diurnal profilesand following oral glucose in acromegaly Clin Endocrinol 199338589ndash93
31Frank G Pasquini E Farneti G Mazzatenta D Sciarretta VGrasso V et al The endoscopic versus the traditional ap-proach in pituitary surgery Neuroendocrinology 2006 83240ndash8
32Marquez Y Tuchman A Zada G Surgery and radiosurgery foracromegaly a review of indications operative techniquesoutcomes and complications Int J Endocrinol 2012 2012386ndash401
33Laws ER Vance ML Thapar K Pituitary surgery for the man-agement of acromegaly Horm Res 2000 5371ndash5
34Salaun C Foubert L Vialatou M Kujas M Turpin G Prognosticfactors of surgical cure of growth hormone secreting pituitary aden-omas Ann Medecine Interne 1999 150195ndash8
35Kreutzer J Vance ML Lopes MB Laws ER Jr Surgical manage-ment of GH-secreting pituitary adenomas an outcome studyusing modern remission criteria J Clin Endocrinol Metab 2001864072ndash7
36Annamalai AK Webb A Kandasamy N Elkhawad M Moir SKhan F et al A comprehensive study of clinical biochemicalradiological vascular cardiac and sleep parameters in anunselected cohort of patients with acromegaly undergoingpresurgical somatostatin receptor ligand therapy J ClinEndocrinol Metab 2013 981040ndash50
37Shen M Shou X Wang Y Zhang Z Wu J Mao Y et al Effect ofpresurgical long-acting octreotide treatment in acromegalypatients with invasive pituitary macroadenomas a prospect-ive randomized study Endocr J 2010 571035ndash44
38Friedel ME Johnston D Singhal S Al Khalili K Farrell CJEvans JJ et al Airway management and perioperative con-cerns in acromegaly patients undergoing endoscopic trans-sphenoidal surgery for pituitary tumors Otolaryngol HeadNeck Surg 2013 149840ndash4
39Bhayana S Booth G Asa SL Kovacs Ezzat S The implicationof somatotroph adenoma phenotype to somatostatin analogresponsiveness in acromegaly J Clin Endocrinol Metab 2005906290ndash5
40Reisine T Bell GI Molecular biology of somatostatin recep-tors Endocr Rev 1995 16427ndash42
41Zatelli MC Piccin D Tagliati F et al Dopamine receptor sub-type 2 and somatostatin receptor subtype 5 expression influ-ences somatostatin analog effects on human somatotrophpituitary adenomas in vitro J Mol Endocrinol 2005 35333ndash41
42Murray RD Melmed S A critical analysis of clinically avail-able somatostatin analog formulations for therapy of acro-megaly J Clin Endocrinol Metab 2008 932957ndash68
43Freda PU Katznelson L Van der Lely A Reyes CM Zhao SRabinowitz D Long-acting somatostatin analog therapy ofacromegaly a meta-analysis J Clin Endocrinol Metab 2005904465ndash74
44Howlett TA Willis D Walker G Wass JA Trainer PJ Control ofgrowth hormone and IGF1 in patients with acromegaly in theUK responses to medical treatment with somatostatin ana-logues and dopamine agonists Clin Endocrinol 201379689ndash99
45Espinosa de los Monteros AL Carrasco C Albarran AAGadelha M Abreu A Mercado M The role of primary pharma-cological therapy in acromegaly Pituitary 2014 17 (Suppl1)S4ndashS10
46Colao AM Auriemma RS Pivonello R The effects of somato-statin analogue therapy on pituitary tumor volume in pa-tients with acromegaly Pituitary 2016 19210ndash21
47Sathyapalan T Lowry M Turnbull LW Rowland-Hill C AtkinSL Mechanism of action of octreotide in acromegalic tu-mours in vivo using dynamic contrast-enhanced magneticresonance imaging Pituitary 2007 10233ndash6
R Dineen et al | 419
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
48Giustina A Mazziotti G Torri V Spinello M Floriani IMelmed S Meta-analysis on the effects of octreotide ontumor mass in acromegaly PLoS One 2012 7e36411
49Abu Dabrh AM Mohammed K Asi N Farah WH Wang ZFarah MH et al Surgical interventions and medical treat-ments in treatment-naive patients with acromegaly system-atic review and meta-analysis J Clin Endocrinol Metab 2014994003ndash14
50Colao A Bronstein M Freda P Gu F Shen C-C Gadelha Met al Pasireotide versus octreotide in acromegaly a head-to-head superiority study J Clin Endocrinol Metab 2014 99791ndash9
51Schmid HA Schoeffter P Functional activity of the multili-gand analog SOM230 at human recombinant somatostatinreceptor subtypes supports its usefulness in neuroendocrinetumors Neuroendocrinology 2004 80 (Suppl 1)47ndash50
52Mazziotti G Floriani I Bonadonna S Torri V Chanson PGiustina A Effects of somatostatin analogs on glucosehomeostasis a metaanalysis of acromegaly studies J ClinEndocrinol Metab 2009 941500ndash8
53Higham CE Trainer PJ Growth hormone excess and the de-velopment of growth hormone receptor antagonists ExpPhysiol 2008 931157ndash69
54Trainer PJ Drake WM Katznelson L et al Treatment of acro-megaly with the growth hormone receptor antagonist pegvi-somant N Engl J Med 2000 3421171ndash7
55Van der Lely AJ Hutson RK Trainer PJ Besser GM Barkan ALKatznelson L et al Long-term treatment of acromegaly withpegvisomant a growth hormone receptor antagonist Lancet2001 3581754ndash9
56Buchfelder M Weigel D Droste M Mann K Saller B BrubachK et al Pituitary tumor size in acromegaly during pegvisom-ant treatment experience from MR re-evaluations of theGerman Pegvisomant Observational Study Eur J Endocrinol2009 16127ndash35
57 Jaffe CA Barkan AL Treatment of acromegaly with dopamineagonists Endocrinol Metab Clin North Am 1992 21713ndash35
58Sandret L Maison P Chanson P Place of cabergoline in acro-megaly a meta-analysis J Clin Endocrinol Metab 2011961327ndash35
59Sherlock M Woods C Sheppard C Medical therapy in acro-megaly Nat Rev Endocrinol 2011 7291ndash300
60Samson SL Ezzat S AACEACE disease state clinical reviewdopamine agonists for hyperprolactinemia and the risk ofcardiac valve disease Endocr Pract 2014 20608ndash16
61 Jaquet P Gunz G Saveanu A Dufour H Taylor J Dong J et alEfficacy of chimeric molecules directed towards multiplesomatostatin and dopamine receptors on inhibition of GHand prolactin secretion from GH-secreting pituitary aden-omas classified as partially responsive to somatostatin ana-log therapy Eur J Endocrinol 2005 153135ndash41
62Barkan AL Halasz I Dornfeld KJ Jaffe CA Friberg RDChandler WF et al Pituitary irradiation is ineffective in nor-malizing plasma insulin-like growth factor I in patients withacromegaly J Clin Endocrinol Metab 1997 823187ndash91
63Eastman RC Gorden P Glatstein E Roth J Radiation therapyof acromegaly Endocrinol Metab Clin North Am 199221693ndash712
64 Jenkins PJ Bates Carson MN Stewart PM Wass JAConventional pituitary irradiation is effective in loweringserum growth hormone and insulin-like growth factor-I inpatients with acromegaly J Clin Endocrinol Metab 2006911239ndash45
65Minniti G Gilbert DC Brada M Modern techniques for pituit-ary radiotherapy Rev Endocr Metab Disord 2008 10135ndash44
66Stapleton CJ Liu CY Weiss M The role of stereotactic radio-surgery in the multimodal management of growth hormone-secreting pituitary adenomas Neurosurg Focus 2010 29E11
67Biermasz NR van Dulken H Roelfsema F Long-term follow-up results of postoperative radiotherapy in 36 patients withacromegaly J Clin Endocrinol Metab 2000 852475ndash82
68Attanasio R Epaminonda P Motti E Giugni E Ventrella LCozzi R et al Gamma-knife radiosurgery in acromegaly a 4-year follow-up study J Clin Endocrinol Metab 2003 883105ndash12
69Minniti G Traish D Ashley S Gonsalves A Brada M Risk ofsecond brain tumor after conservative surgery and radiother-apy for pituitary adenoma update after an additional 10years J Clin Endocrinol Metab 2005 90800ndash4
70Brada M Burchell L Ashley S Traish D The incidence of cere-brovascular accidents in patients with pituitary adenoma IntJ Radiat Oncol Biol Phys 1999 45693ndash8
71Laws ER Sheehan JP Sheehan JM Jagnathan J Jane JA JrOskouian R Stereotactic radiosurgery for pituitary aden-omas a review of the literature J Neurooncol 2004 69257ndash72
420 | QJM An International Journal of Medicine 2017 Vol 110 No 7
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
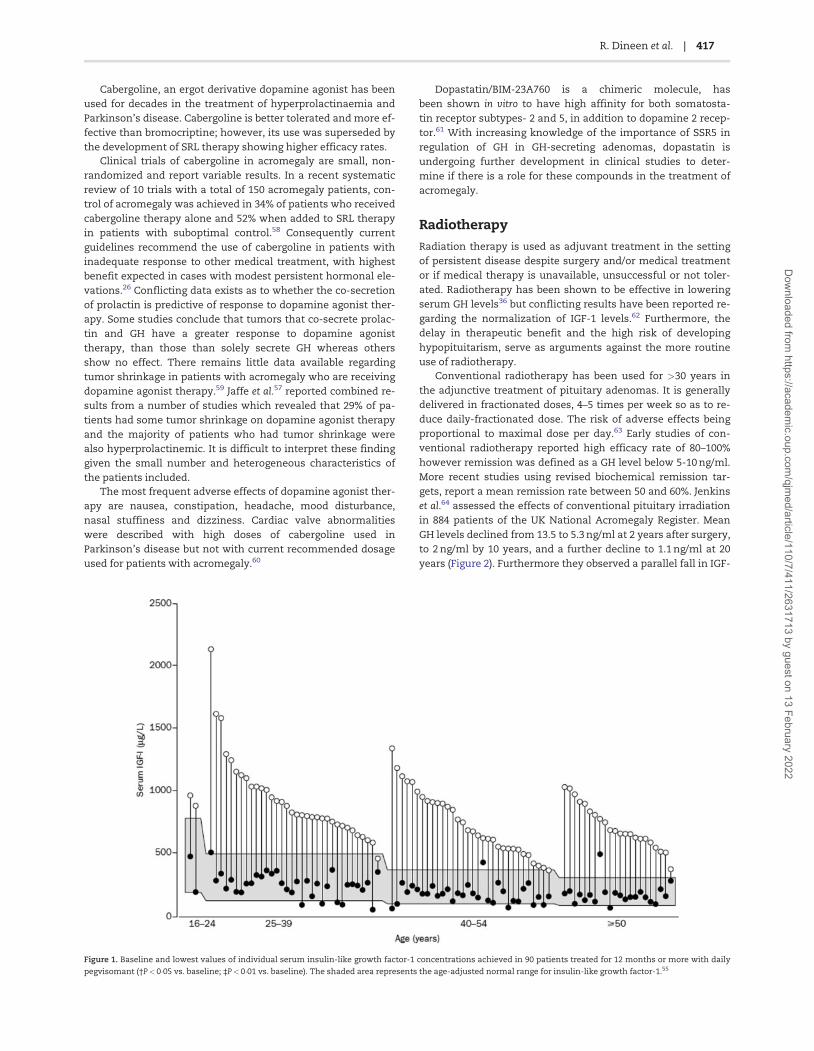
Cabergoline an ergot derivative dopamine agonist has beenused for decades in the treatment of hyperprolactinaemia andParkinsonrsquos disease Cabergoline is better tolerated and more ef-fective than bromocriptine however its use was superseded bythe development of SRL therapy showing higher efficacy rates
Clinical trials of cabergoline in acromegaly are small non-randomized and report variable results In a recent systematicreview of 10 trials with a total of 150 acromegaly patients con-trol of acromegaly was achieved in 34 of patients who receivedcabergoline therapy alone and 52 when added to SRL therapyin patients with suboptimal control58 Consequently currentguidelines recommend the use of cabergoline in patients withinadequate response to other medical treatment with highestbenefit expected in cases with modest persistent hormonal ele-vations26 Conflicting data exists as to whether the co-secretionof prolactin is predictive of response to dopamine agonist ther-apy Some studies conclude that tumors that co-secrete prolac-tin and GH have a greater response to dopamine agonisttherapy than those than solely secrete GH whereas othersshow no effect There remains little data available regardingtumor shrinkage in patients with acromegaly who are receivingdopamine agonist therapy59 Jaffe et al57 reported combined re-sults from a number of studies which revealed that 29 of pa-tients had some tumor shrinkage on dopamine agonist therapyand the majority of patients who had tumor shrinkage werealso hyperprolactinemic It is difficult to interpret these findinggiven the small number and heterogeneous characteristics ofthe patients included
The most frequent adverse effects of dopamine agonist ther-apy are nausea constipation headache mood disturbancenasal stuffiness and dizziness Cardiac valve abnormalitieswere described with high doses of cabergoline used inParkinsonrsquos disease but not with current recommended dosageused for patients with acromegaly60
DopastatinBIM-23A760 is a chimeric molecule hasbeen shown in vitro to have high affinity for both somatosta-tin receptor subtypes- 2 and 5 in addition to dopamine 2 recep-tor61 With increasing knowledge of the importance of SSR5 inregulation of GH in GH-secreting adenomas dopastatin isundergoing further development in clinical studies to deter-mine if there is a role for these compounds in the treatment ofacromegaly
Radiotherapy
Radiation therapy is used as adjuvant treatment in the settingof persistent disease despite surgery andor medical treatmentor if medical therapy is unavailable unsuccessful or not toler-ated Radiotherapy has been shown to be effective in loweringserum GH levels36 but conflicting results have been reported re-garding the normalization of IGF-1 levels62 Furthermore thedelay in therapeutic benefit and the high risk of developinghypopituitarism serve as arguments against the more routineuse of radiotherapy
Conventional radiotherapy has been used for gt30 years inthe adjunctive treatment of pituitary adenomas It is generallydelivered in fractionated doses 4ndash5 times per week so as to re-duce daily-fractionated dose The risk of adverse effects beingproportional to maximal dose per day63 Early studies of con-ventional radiotherapy reported high efficacy rate of 80ndash100however remission was defined as a GH level below 5-10 ngmlMore recent studies using revised biochemical remission tar-gets report a mean remission rate between 50 and 60 Jenkinset al64 assessed the effects of conventional pituitary irradiationin 884 patients of the UK National Acromegaly Register MeanGH levels declined from 135 to 53 ngml at 2 years after surgeryto 2 ngml by 10 years and a further decline to 11 ngml at 20years (Figure 2) Furthermore they observed a parallel fall in IGF-
Figure 1 Baseline and lowest values of individual serum insulin-like growth factor-1 concentrations achieved in 90 patients treated for 12 months or more with daily
pegvisomant (daggerPlt005 vs baseline DaggerPlt001 vs baseline) The shaded area represents the age-adjusted normal range for insulin-like growth factor-155
R Dineen et al | 417
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
1 levels with 63 of patients having a normal level by 10years64
Stereotactic radiotherapy offers improvement in immobil-ization imaging and treatment delivery from conventionaltechniques It can be delivered as a single fraction radiosurgeryusing a Gamma knife (a source of cobalt) or a linear acceleratoror a stereotactic conformal radiotherapy delivered as fractio-nated treatment using a linear accelerator There is no clear ad-vantage for either of the radiosurgical techniques in terms ofsparing normal tissue receiving high doses of radiation65 A crit-ical analysis of the literature reported variable rates of both bio-chemical and tumor response 17ndash82 and 37ndash100respectively66 The authors attributed the wide variability to theuse of different treatment schedules and definitions ofremission
Hypopituitarism is less frequent with radiosurgery than con-ventional radiotherapy At least 50 of patient treated with con-ventional radiotherapy will have acquired new anteriorpituitary hormonal deficits at 10 years67 In cohorts treatedsolely with stereotactic techniques rates of hypopituitarismvary between 0 and 2068 However it is likely that the candi-dates for stereotactic radiotherapy had smaller remnants of dis-ease and therefore less normal tissue irradiated
Annual hormonal testing is required due to the risk of latehypopituitarism26 Other complications following radiotherapyinclude the risk of second brain tumors stroke and rarely opticneuropathy cranial nerve deficits and radionecrosis a rare ad-verse effect of gamma knife radiotherapy69ndash71
Patients treated with conventional radiotherapy have beenreported to have increased mortality predominantly due tostroke independent of GHIGF-I levels and hypopituitarism20
Current guidelines recommend the use of stereotactic radio-therapy over conventional radiation therapy unless significantresidual tumor burden or the lesion is too close to the opticchiasm26
Conclusion
Prolonged exposure to elevated endogenous levels of GH andIGF-I results in a multisystem disease characterized by somaticovergrowth multiple co-morbidities and premature mortalityEarly detection prevents the development of irreversible com-plications of the disease including cardiomyopathy respiratory
dysfunction and arthropathy Despite the imprecision of assaysfor GH and IGF-I it is clear from epidemiologic studies that tightbiochemical control is essential to reduce morbidity controlsymptoms and improve mortality rates
Optimal implementation of current guidelines in routine clin-ical practice and maximal use of the medical treatment could im-prove the long-term control of patients with significant benefitsfor morbidity and mortality Another important aspect in thetreatment of patients with acromegaly is also the appropriate tar-geted treatment of co-morbidities associated with acromegaly
Achievement of the criteria for cure during or after therapyis determined by assessing biochemical control targeting con-trolled levels of GH and normalization of IGF-I levels monitor-ing tumor size assessing residual pituitary function andmonitoring co-morbidities
New therapeutic molecules currently in trials will hopefullyoffer further benefit to those patients resistant to current thera-peutic modes for this chronic progressive disorder
Conflict of interest None declared
References1 Melmed S Braunstein GD Horvath E Ezrin C Kovacs K
Pathophysiology of acromegaly Endocr Rev 1983 4271ndash902 Mestron A Webb SM Astorga R Benito P Catala M
Gaztambide S et al Epidemiology clinical characteristicsoutcome morbidity and mortality in acromegaly based onthe Spanish Acromegaly Registry (Registro Espanol deAcromegalia REA) Eur J Endocrinol 2004 151439ndash46
3 Jagannathan J Dumont AS Prevedello DM Oskouian RJLopes B Jane JA Jr and Laws ER Jr Genetics of pituitary aden-omas current theories and future implications NeurosurgFocus 2005 19E4
4 Zhu X Lin CR Prefontaine CG Tollkuhn J Rosenfeld MGGenetic control of pituitary developement and hypopituitar-ism Curr Opin Genet Dev 2005 15332ndash40
5 Melmed S Acromegaly pathogenesis and treatment J ClinInvest 2009 1193189ndash202
6 Colao A Ferone D Marzullo P Lombardi G Systemic compli-cations of acromegaly epidemiology pathogenesis andmanagement Endocr Rev 2004 25102ndash52
7 Korbonits M Gadelha MR Roncaroli F Grossman AB Ellard SEvanson J et al Landscape of familial isolated and young-onset pituitary adenomas prospective diagnosis in AIP mu-tation carriers J Clin Endocrinol Metab 2015 100E1242ndash54
8 Larkin S Reddy R Karavitaki N Cudlip S Wass J Ansorge OGranulation pattern but not GSP or GHR mutation is associ-ated with clinical characteristics in somatostatin-naive pa-tients with somatotroph adenomas Eur J Endocrinol 2013168491ndash9
9 Molitch ME Clinical manifestations of acromegaly EndocrinolMetab Clin North Am 1992 21597ndash614
10Reid TJ Post KD Bruce JN Nabi KM Reyes-Vidal CM et alFeatures at diagnosis of 324 patients with acromegaly didnot change from 1981 to 2006 acromegaly remains under-recognized and under-diagnosed Clin Endocrinol 201072203ndash8
11Moslashller N Joslashrgensen JO Abildgard N Orskov L Schmitz OChristiansen JS Effects of growth hormone on glucose me-tabolism Horm Res 1991 36 (Suppl 1)32ndash5
12Dreval AV Trigolosova IV Misnikova IV Kovalyova YATishenina RS Barsukov IA et al Prevalence of diabetes melli-tus in patients with acromegaly Endocr Connect 2014 393ndash8
Figure 2 Percentage of all patients achieving a serum GH level lt25 ngml (bars)
and the mean GH level (line) in the years after pituitary irradiation64
418 | QJM An International Journal of Medicine 2017 Vol 110 No 7
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
13Roemmler J Gutt B Fischer R Vay S Wiesmeth ABidlingmaier M et al Elevated incidence of sleep apnoea inacromegaly-correlation to disease activity Sleep Breath 2012161247ndash53
14Killinger Z Payer J Lazurova I Imrich R Homerova Z KuzmaM et al Arthropathy in acromegaly Rheum Dis Clin North Am2010 36713ndash20
15Kameyama S Tanaka R Hasegawa A Tamura T Kuroki MSubclinical carpal tunnel syndrome in acromegaly NeurolMed Chir 1993 33547ndash51
16Mazziotti G Biagioli E Maffezzoni F Spinello M Serra VMaroldi R et al Bone turnover bone mineral density and frac-ture risk in acromegaly a meta-analysis J Clin EndocrinolMetab 2015 100384ndash94
17Renehan AG OrsquoConnell J OrsquoHalloran D Shanahan F PottenCS OrsquoDwyer ST et al Acromegaly and colorectal cancer acomprehensive review of epidemiology biological mechan-isms and clinical implications Horm Metab Res 200335712ndash25
18Orme S McNally RJ Cartwright RA Belchetz PE Mortality andcancer incidence in acromegaly a restrospective cohortstudy J Clin Endocrinol Metab 1998 832730ndash4
19Petroff D Teuroonjes A Grussendorf M Droste M Dimopoulou CStalla G et al The Incidence of cancer among acromegaly pa-tients results from the German Acromegaly Registry J ClinEndocrinol Metab 2015 1003894ndash902
20Sherlock M Ayuk J Tomlinson JW Toogood AA Aragon-Alonso A Sheppard MC et al Mortality in patients with pitu-itary disease Endocr Rev 2010 31301ndash42
21Bates AS Vanrsquot H Jones JM Clayton RN An audit of outcomeof treatment in acromegaly Q J Med 1993 86293ndash9
22Ayuk J Clayton RN Holder G Sheppard MC Stewart PMBates AS Growth hormone and pituitary radiotherapy butnot serum insulin-like growth factor-I concentrations pre-dict excess mortality in patients with acromegaly J ClinEndocrinol Metab 2004 891613ndash7
23Kauppinen-Meuroakelin R Sane T Reunanen A Veuroalimeuroaki MJNiskanen L Markkanen H et al A nationwide survey of mor-tality in acromegaly J Clin Endocrinol Metab 2005 904081ndash6
24Holdaway IM Bolland MJ Gamble GD A meta-analysis of theeffect of lowering serum levels of GH and IGF-I on mortalityin acromegaly Eur J Endocrinol 2008 15989ndash95
25Rosen T Bengtsson BA Premature mortality due to cardio-vascular disease in hypopituitarism Lancet 1990 336285ndash8
26Katznelson L Laws ER Jr Melmed S Molitch ME Murad MHUtz A et al Acromegaly an endocrine society clinical practiceguideline J Clin Endocrinol Metab 2014 993933ndash51
27Freda PU Post KD Powell JS Wardlaw SL Evaluation of dis-ease status with sensitive measures of growth hormone se-cretion in 60 postoperative patients with acromegaly J ClinEndocrinol Metab 1998 833808ndash16
28Dimaraki EV Jaffe CA DeMott-Friberg R Chandler WFBarkan AL Acromegaly with apparently normal GH secretionimplications for diagnosis and follow-up J Clin EndocrinolMetab 2002 873537ndash42
29Losa M Von Werder K Pathophysiology and clinical aspectsof the ectopic GH-releasing hormone syndrome ClinEndocrinol 1997 47123ndash35
30Dobrashian RD OrsquoHalloran DJ Hunt A Beardwell CG ShaletSM Relationships between insulin-like growth factor-1 levelsand growth hormone concentrations during diurnal profilesand following oral glucose in acromegaly Clin Endocrinol 199338589ndash93
31Frank G Pasquini E Farneti G Mazzatenta D Sciarretta VGrasso V et al The endoscopic versus the traditional ap-proach in pituitary surgery Neuroendocrinology 2006 83240ndash8
32Marquez Y Tuchman A Zada G Surgery and radiosurgery foracromegaly a review of indications operative techniquesoutcomes and complications Int J Endocrinol 2012 2012386ndash401
33Laws ER Vance ML Thapar K Pituitary surgery for the man-agement of acromegaly Horm Res 2000 5371ndash5
34Salaun C Foubert L Vialatou M Kujas M Turpin G Prognosticfactors of surgical cure of growth hormone secreting pituitary aden-omas Ann Medecine Interne 1999 150195ndash8
35Kreutzer J Vance ML Lopes MB Laws ER Jr Surgical manage-ment of GH-secreting pituitary adenomas an outcome studyusing modern remission criteria J Clin Endocrinol Metab 2001864072ndash7
36Annamalai AK Webb A Kandasamy N Elkhawad M Moir SKhan F et al A comprehensive study of clinical biochemicalradiological vascular cardiac and sleep parameters in anunselected cohort of patients with acromegaly undergoingpresurgical somatostatin receptor ligand therapy J ClinEndocrinol Metab 2013 981040ndash50
37Shen M Shou X Wang Y Zhang Z Wu J Mao Y et al Effect ofpresurgical long-acting octreotide treatment in acromegalypatients with invasive pituitary macroadenomas a prospect-ive randomized study Endocr J 2010 571035ndash44
38Friedel ME Johnston D Singhal S Al Khalili K Farrell CJEvans JJ et al Airway management and perioperative con-cerns in acromegaly patients undergoing endoscopic trans-sphenoidal surgery for pituitary tumors Otolaryngol HeadNeck Surg 2013 149840ndash4
39Bhayana S Booth G Asa SL Kovacs Ezzat S The implicationof somatotroph adenoma phenotype to somatostatin analogresponsiveness in acromegaly J Clin Endocrinol Metab 2005906290ndash5
40Reisine T Bell GI Molecular biology of somatostatin recep-tors Endocr Rev 1995 16427ndash42
41Zatelli MC Piccin D Tagliati F et al Dopamine receptor sub-type 2 and somatostatin receptor subtype 5 expression influ-ences somatostatin analog effects on human somatotrophpituitary adenomas in vitro J Mol Endocrinol 2005 35333ndash41
42Murray RD Melmed S A critical analysis of clinically avail-able somatostatin analog formulations for therapy of acro-megaly J Clin Endocrinol Metab 2008 932957ndash68
43Freda PU Katznelson L Van der Lely A Reyes CM Zhao SRabinowitz D Long-acting somatostatin analog therapy ofacromegaly a meta-analysis J Clin Endocrinol Metab 2005904465ndash74
44Howlett TA Willis D Walker G Wass JA Trainer PJ Control ofgrowth hormone and IGF1 in patients with acromegaly in theUK responses to medical treatment with somatostatin ana-logues and dopamine agonists Clin Endocrinol 201379689ndash99
45Espinosa de los Monteros AL Carrasco C Albarran AAGadelha M Abreu A Mercado M The role of primary pharma-cological therapy in acromegaly Pituitary 2014 17 (Suppl1)S4ndashS10
46Colao AM Auriemma RS Pivonello R The effects of somato-statin analogue therapy on pituitary tumor volume in pa-tients with acromegaly Pituitary 2016 19210ndash21
47Sathyapalan T Lowry M Turnbull LW Rowland-Hill C AtkinSL Mechanism of action of octreotide in acromegalic tu-mours in vivo using dynamic contrast-enhanced magneticresonance imaging Pituitary 2007 10233ndash6
R Dineen et al | 419
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
48Giustina A Mazziotti G Torri V Spinello M Floriani IMelmed S Meta-analysis on the effects of octreotide ontumor mass in acromegaly PLoS One 2012 7e36411
49Abu Dabrh AM Mohammed K Asi N Farah WH Wang ZFarah MH et al Surgical interventions and medical treat-ments in treatment-naive patients with acromegaly system-atic review and meta-analysis J Clin Endocrinol Metab 2014994003ndash14
50Colao A Bronstein M Freda P Gu F Shen C-C Gadelha Met al Pasireotide versus octreotide in acromegaly a head-to-head superiority study J Clin Endocrinol Metab 2014 99791ndash9
51Schmid HA Schoeffter P Functional activity of the multili-gand analog SOM230 at human recombinant somatostatinreceptor subtypes supports its usefulness in neuroendocrinetumors Neuroendocrinology 2004 80 (Suppl 1)47ndash50
52Mazziotti G Floriani I Bonadonna S Torri V Chanson PGiustina A Effects of somatostatin analogs on glucosehomeostasis a metaanalysis of acromegaly studies J ClinEndocrinol Metab 2009 941500ndash8
53Higham CE Trainer PJ Growth hormone excess and the de-velopment of growth hormone receptor antagonists ExpPhysiol 2008 931157ndash69
54Trainer PJ Drake WM Katznelson L et al Treatment of acro-megaly with the growth hormone receptor antagonist pegvi-somant N Engl J Med 2000 3421171ndash7
55Van der Lely AJ Hutson RK Trainer PJ Besser GM Barkan ALKatznelson L et al Long-term treatment of acromegaly withpegvisomant a growth hormone receptor antagonist Lancet2001 3581754ndash9
56Buchfelder M Weigel D Droste M Mann K Saller B BrubachK et al Pituitary tumor size in acromegaly during pegvisom-ant treatment experience from MR re-evaluations of theGerman Pegvisomant Observational Study Eur J Endocrinol2009 16127ndash35
57 Jaffe CA Barkan AL Treatment of acromegaly with dopamineagonists Endocrinol Metab Clin North Am 1992 21713ndash35
58Sandret L Maison P Chanson P Place of cabergoline in acro-megaly a meta-analysis J Clin Endocrinol Metab 2011961327ndash35
59Sherlock M Woods C Sheppard C Medical therapy in acro-megaly Nat Rev Endocrinol 2011 7291ndash300
60Samson SL Ezzat S AACEACE disease state clinical reviewdopamine agonists for hyperprolactinemia and the risk ofcardiac valve disease Endocr Pract 2014 20608ndash16
61 Jaquet P Gunz G Saveanu A Dufour H Taylor J Dong J et alEfficacy of chimeric molecules directed towards multiplesomatostatin and dopamine receptors on inhibition of GHand prolactin secretion from GH-secreting pituitary aden-omas classified as partially responsive to somatostatin ana-log therapy Eur J Endocrinol 2005 153135ndash41
62Barkan AL Halasz I Dornfeld KJ Jaffe CA Friberg RDChandler WF et al Pituitary irradiation is ineffective in nor-malizing plasma insulin-like growth factor I in patients withacromegaly J Clin Endocrinol Metab 1997 823187ndash91
63Eastman RC Gorden P Glatstein E Roth J Radiation therapyof acromegaly Endocrinol Metab Clin North Am 199221693ndash712
64 Jenkins PJ Bates Carson MN Stewart PM Wass JAConventional pituitary irradiation is effective in loweringserum growth hormone and insulin-like growth factor-I inpatients with acromegaly J Clin Endocrinol Metab 2006911239ndash45
65Minniti G Gilbert DC Brada M Modern techniques for pituit-ary radiotherapy Rev Endocr Metab Disord 2008 10135ndash44
66Stapleton CJ Liu CY Weiss M The role of stereotactic radio-surgery in the multimodal management of growth hormone-secreting pituitary adenomas Neurosurg Focus 2010 29E11
67Biermasz NR van Dulken H Roelfsema F Long-term follow-up results of postoperative radiotherapy in 36 patients withacromegaly J Clin Endocrinol Metab 2000 852475ndash82
68Attanasio R Epaminonda P Motti E Giugni E Ventrella LCozzi R et al Gamma-knife radiosurgery in acromegaly a 4-year follow-up study J Clin Endocrinol Metab 2003 883105ndash12
69Minniti G Traish D Ashley S Gonsalves A Brada M Risk ofsecond brain tumor after conservative surgery and radiother-apy for pituitary adenoma update after an additional 10years J Clin Endocrinol Metab 2005 90800ndash4
70Brada M Burchell L Ashley S Traish D The incidence of cere-brovascular accidents in patients with pituitary adenoma IntJ Radiat Oncol Biol Phys 1999 45693ndash8
71Laws ER Sheehan JP Sheehan JM Jagnathan J Jane JA JrOskouian R Stereotactic radiosurgery for pituitary aden-omas a review of the literature J Neurooncol 2004 69257ndash72
420 | QJM An International Journal of Medicine 2017 Vol 110 No 7
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022

1 levels with 63 of patients having a normal level by 10years64
Stereotactic radiotherapy offers improvement in immobil-ization imaging and treatment delivery from conventionaltechniques It can be delivered as a single fraction radiosurgeryusing a Gamma knife (a source of cobalt) or a linear acceleratoror a stereotactic conformal radiotherapy delivered as fractio-nated treatment using a linear accelerator There is no clear ad-vantage for either of the radiosurgical techniques in terms ofsparing normal tissue receiving high doses of radiation65 A crit-ical analysis of the literature reported variable rates of both bio-chemical and tumor response 17ndash82 and 37ndash100respectively66 The authors attributed the wide variability to theuse of different treatment schedules and definitions ofremission
Hypopituitarism is less frequent with radiosurgery than con-ventional radiotherapy At least 50 of patient treated with con-ventional radiotherapy will have acquired new anteriorpituitary hormonal deficits at 10 years67 In cohorts treatedsolely with stereotactic techniques rates of hypopituitarismvary between 0 and 2068 However it is likely that the candi-dates for stereotactic radiotherapy had smaller remnants of dis-ease and therefore less normal tissue irradiated
Annual hormonal testing is required due to the risk of latehypopituitarism26 Other complications following radiotherapyinclude the risk of second brain tumors stroke and rarely opticneuropathy cranial nerve deficits and radionecrosis a rare ad-verse effect of gamma knife radiotherapy69ndash71
Patients treated with conventional radiotherapy have beenreported to have increased mortality predominantly due tostroke independent of GHIGF-I levels and hypopituitarism20
Current guidelines recommend the use of stereotactic radio-therapy over conventional radiation therapy unless significantresidual tumor burden or the lesion is too close to the opticchiasm26
Conclusion
Prolonged exposure to elevated endogenous levels of GH andIGF-I results in a multisystem disease characterized by somaticovergrowth multiple co-morbidities and premature mortalityEarly detection prevents the development of irreversible com-plications of the disease including cardiomyopathy respiratory
dysfunction and arthropathy Despite the imprecision of assaysfor GH and IGF-I it is clear from epidemiologic studies that tightbiochemical control is essential to reduce morbidity controlsymptoms and improve mortality rates
Optimal implementation of current guidelines in routine clin-ical practice and maximal use of the medical treatment could im-prove the long-term control of patients with significant benefitsfor morbidity and mortality Another important aspect in thetreatment of patients with acromegaly is also the appropriate tar-geted treatment of co-morbidities associated with acromegaly
Achievement of the criteria for cure during or after therapyis determined by assessing biochemical control targeting con-trolled levels of GH and normalization of IGF-I levels monitor-ing tumor size assessing residual pituitary function andmonitoring co-morbidities
New therapeutic molecules currently in trials will hopefullyoffer further benefit to those patients resistant to current thera-peutic modes for this chronic progressive disorder
Conflict of interest None declared
References1 Melmed S Braunstein GD Horvath E Ezrin C Kovacs K
Pathophysiology of acromegaly Endocr Rev 1983 4271ndash902 Mestron A Webb SM Astorga R Benito P Catala M
Gaztambide S et al Epidemiology clinical characteristicsoutcome morbidity and mortality in acromegaly based onthe Spanish Acromegaly Registry (Registro Espanol deAcromegalia REA) Eur J Endocrinol 2004 151439ndash46
3 Jagannathan J Dumont AS Prevedello DM Oskouian RJLopes B Jane JA Jr and Laws ER Jr Genetics of pituitary aden-omas current theories and future implications NeurosurgFocus 2005 19E4
4 Zhu X Lin CR Prefontaine CG Tollkuhn J Rosenfeld MGGenetic control of pituitary developement and hypopituitar-ism Curr Opin Genet Dev 2005 15332ndash40
5 Melmed S Acromegaly pathogenesis and treatment J ClinInvest 2009 1193189ndash202
6 Colao A Ferone D Marzullo P Lombardi G Systemic compli-cations of acromegaly epidemiology pathogenesis andmanagement Endocr Rev 2004 25102ndash52
7 Korbonits M Gadelha MR Roncaroli F Grossman AB Ellard SEvanson J et al Landscape of familial isolated and young-onset pituitary adenomas prospective diagnosis in AIP mu-tation carriers J Clin Endocrinol Metab 2015 100E1242ndash54
8 Larkin S Reddy R Karavitaki N Cudlip S Wass J Ansorge OGranulation pattern but not GSP or GHR mutation is associ-ated with clinical characteristics in somatostatin-naive pa-tients with somatotroph adenomas Eur J Endocrinol 2013168491ndash9
9 Molitch ME Clinical manifestations of acromegaly EndocrinolMetab Clin North Am 1992 21597ndash614
10Reid TJ Post KD Bruce JN Nabi KM Reyes-Vidal CM et alFeatures at diagnosis of 324 patients with acromegaly didnot change from 1981 to 2006 acromegaly remains under-recognized and under-diagnosed Clin Endocrinol 201072203ndash8
11Moslashller N Joslashrgensen JO Abildgard N Orskov L Schmitz OChristiansen JS Effects of growth hormone on glucose me-tabolism Horm Res 1991 36 (Suppl 1)32ndash5
12Dreval AV Trigolosova IV Misnikova IV Kovalyova YATishenina RS Barsukov IA et al Prevalence of diabetes melli-tus in patients with acromegaly Endocr Connect 2014 393ndash8
Figure 2 Percentage of all patients achieving a serum GH level lt25 ngml (bars)
and the mean GH level (line) in the years after pituitary irradiation64
418 | QJM An International Journal of Medicine 2017 Vol 110 No 7
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
13Roemmler J Gutt B Fischer R Vay S Wiesmeth ABidlingmaier M et al Elevated incidence of sleep apnoea inacromegaly-correlation to disease activity Sleep Breath 2012161247ndash53
14Killinger Z Payer J Lazurova I Imrich R Homerova Z KuzmaM et al Arthropathy in acromegaly Rheum Dis Clin North Am2010 36713ndash20
15Kameyama S Tanaka R Hasegawa A Tamura T Kuroki MSubclinical carpal tunnel syndrome in acromegaly NeurolMed Chir 1993 33547ndash51
16Mazziotti G Biagioli E Maffezzoni F Spinello M Serra VMaroldi R et al Bone turnover bone mineral density and frac-ture risk in acromegaly a meta-analysis J Clin EndocrinolMetab 2015 100384ndash94
17Renehan AG OrsquoConnell J OrsquoHalloran D Shanahan F PottenCS OrsquoDwyer ST et al Acromegaly and colorectal cancer acomprehensive review of epidemiology biological mechan-isms and clinical implications Horm Metab Res 200335712ndash25
18Orme S McNally RJ Cartwright RA Belchetz PE Mortality andcancer incidence in acromegaly a restrospective cohortstudy J Clin Endocrinol Metab 1998 832730ndash4
19Petroff D Teuroonjes A Grussendorf M Droste M Dimopoulou CStalla G et al The Incidence of cancer among acromegaly pa-tients results from the German Acromegaly Registry J ClinEndocrinol Metab 2015 1003894ndash902
20Sherlock M Ayuk J Tomlinson JW Toogood AA Aragon-Alonso A Sheppard MC et al Mortality in patients with pitu-itary disease Endocr Rev 2010 31301ndash42
21Bates AS Vanrsquot H Jones JM Clayton RN An audit of outcomeof treatment in acromegaly Q J Med 1993 86293ndash9
22Ayuk J Clayton RN Holder G Sheppard MC Stewart PMBates AS Growth hormone and pituitary radiotherapy butnot serum insulin-like growth factor-I concentrations pre-dict excess mortality in patients with acromegaly J ClinEndocrinol Metab 2004 891613ndash7
23Kauppinen-Meuroakelin R Sane T Reunanen A Veuroalimeuroaki MJNiskanen L Markkanen H et al A nationwide survey of mor-tality in acromegaly J Clin Endocrinol Metab 2005 904081ndash6
24Holdaway IM Bolland MJ Gamble GD A meta-analysis of theeffect of lowering serum levels of GH and IGF-I on mortalityin acromegaly Eur J Endocrinol 2008 15989ndash95
25Rosen T Bengtsson BA Premature mortality due to cardio-vascular disease in hypopituitarism Lancet 1990 336285ndash8
26Katznelson L Laws ER Jr Melmed S Molitch ME Murad MHUtz A et al Acromegaly an endocrine society clinical practiceguideline J Clin Endocrinol Metab 2014 993933ndash51
27Freda PU Post KD Powell JS Wardlaw SL Evaluation of dis-ease status with sensitive measures of growth hormone se-cretion in 60 postoperative patients with acromegaly J ClinEndocrinol Metab 1998 833808ndash16
28Dimaraki EV Jaffe CA DeMott-Friberg R Chandler WFBarkan AL Acromegaly with apparently normal GH secretionimplications for diagnosis and follow-up J Clin EndocrinolMetab 2002 873537ndash42
29Losa M Von Werder K Pathophysiology and clinical aspectsof the ectopic GH-releasing hormone syndrome ClinEndocrinol 1997 47123ndash35
30Dobrashian RD OrsquoHalloran DJ Hunt A Beardwell CG ShaletSM Relationships between insulin-like growth factor-1 levelsand growth hormone concentrations during diurnal profilesand following oral glucose in acromegaly Clin Endocrinol 199338589ndash93
31Frank G Pasquini E Farneti G Mazzatenta D Sciarretta VGrasso V et al The endoscopic versus the traditional ap-proach in pituitary surgery Neuroendocrinology 2006 83240ndash8
32Marquez Y Tuchman A Zada G Surgery and radiosurgery foracromegaly a review of indications operative techniquesoutcomes and complications Int J Endocrinol 2012 2012386ndash401
33Laws ER Vance ML Thapar K Pituitary surgery for the man-agement of acromegaly Horm Res 2000 5371ndash5
34Salaun C Foubert L Vialatou M Kujas M Turpin G Prognosticfactors of surgical cure of growth hormone secreting pituitary aden-omas Ann Medecine Interne 1999 150195ndash8
35Kreutzer J Vance ML Lopes MB Laws ER Jr Surgical manage-ment of GH-secreting pituitary adenomas an outcome studyusing modern remission criteria J Clin Endocrinol Metab 2001864072ndash7
36Annamalai AK Webb A Kandasamy N Elkhawad M Moir SKhan F et al A comprehensive study of clinical biochemicalradiological vascular cardiac and sleep parameters in anunselected cohort of patients with acromegaly undergoingpresurgical somatostatin receptor ligand therapy J ClinEndocrinol Metab 2013 981040ndash50
37Shen M Shou X Wang Y Zhang Z Wu J Mao Y et al Effect ofpresurgical long-acting octreotide treatment in acromegalypatients with invasive pituitary macroadenomas a prospect-ive randomized study Endocr J 2010 571035ndash44
38Friedel ME Johnston D Singhal S Al Khalili K Farrell CJEvans JJ et al Airway management and perioperative con-cerns in acromegaly patients undergoing endoscopic trans-sphenoidal surgery for pituitary tumors Otolaryngol HeadNeck Surg 2013 149840ndash4
39Bhayana S Booth G Asa SL Kovacs Ezzat S The implicationof somatotroph adenoma phenotype to somatostatin analogresponsiveness in acromegaly J Clin Endocrinol Metab 2005906290ndash5
40Reisine T Bell GI Molecular biology of somatostatin recep-tors Endocr Rev 1995 16427ndash42
41Zatelli MC Piccin D Tagliati F et al Dopamine receptor sub-type 2 and somatostatin receptor subtype 5 expression influ-ences somatostatin analog effects on human somatotrophpituitary adenomas in vitro J Mol Endocrinol 2005 35333ndash41
42Murray RD Melmed S A critical analysis of clinically avail-able somatostatin analog formulations for therapy of acro-megaly J Clin Endocrinol Metab 2008 932957ndash68
43Freda PU Katznelson L Van der Lely A Reyes CM Zhao SRabinowitz D Long-acting somatostatin analog therapy ofacromegaly a meta-analysis J Clin Endocrinol Metab 2005904465ndash74
44Howlett TA Willis D Walker G Wass JA Trainer PJ Control ofgrowth hormone and IGF1 in patients with acromegaly in theUK responses to medical treatment with somatostatin ana-logues and dopamine agonists Clin Endocrinol 201379689ndash99
45Espinosa de los Monteros AL Carrasco C Albarran AAGadelha M Abreu A Mercado M The role of primary pharma-cological therapy in acromegaly Pituitary 2014 17 (Suppl1)S4ndashS10
46Colao AM Auriemma RS Pivonello R The effects of somato-statin analogue therapy on pituitary tumor volume in pa-tients with acromegaly Pituitary 2016 19210ndash21
47Sathyapalan T Lowry M Turnbull LW Rowland-Hill C AtkinSL Mechanism of action of octreotide in acromegalic tu-mours in vivo using dynamic contrast-enhanced magneticresonance imaging Pituitary 2007 10233ndash6
R Dineen et al | 419
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
48Giustina A Mazziotti G Torri V Spinello M Floriani IMelmed S Meta-analysis on the effects of octreotide ontumor mass in acromegaly PLoS One 2012 7e36411
49Abu Dabrh AM Mohammed K Asi N Farah WH Wang ZFarah MH et al Surgical interventions and medical treat-ments in treatment-naive patients with acromegaly system-atic review and meta-analysis J Clin Endocrinol Metab 2014994003ndash14
50Colao A Bronstein M Freda P Gu F Shen C-C Gadelha Met al Pasireotide versus octreotide in acromegaly a head-to-head superiority study J Clin Endocrinol Metab 2014 99791ndash9
51Schmid HA Schoeffter P Functional activity of the multili-gand analog SOM230 at human recombinant somatostatinreceptor subtypes supports its usefulness in neuroendocrinetumors Neuroendocrinology 2004 80 (Suppl 1)47ndash50
52Mazziotti G Floriani I Bonadonna S Torri V Chanson PGiustina A Effects of somatostatin analogs on glucosehomeostasis a metaanalysis of acromegaly studies J ClinEndocrinol Metab 2009 941500ndash8
53Higham CE Trainer PJ Growth hormone excess and the de-velopment of growth hormone receptor antagonists ExpPhysiol 2008 931157ndash69
54Trainer PJ Drake WM Katznelson L et al Treatment of acro-megaly with the growth hormone receptor antagonist pegvi-somant N Engl J Med 2000 3421171ndash7
55Van der Lely AJ Hutson RK Trainer PJ Besser GM Barkan ALKatznelson L et al Long-term treatment of acromegaly withpegvisomant a growth hormone receptor antagonist Lancet2001 3581754ndash9
56Buchfelder M Weigel D Droste M Mann K Saller B BrubachK et al Pituitary tumor size in acromegaly during pegvisom-ant treatment experience from MR re-evaluations of theGerman Pegvisomant Observational Study Eur J Endocrinol2009 16127ndash35
57 Jaffe CA Barkan AL Treatment of acromegaly with dopamineagonists Endocrinol Metab Clin North Am 1992 21713ndash35
58Sandret L Maison P Chanson P Place of cabergoline in acro-megaly a meta-analysis J Clin Endocrinol Metab 2011961327ndash35
59Sherlock M Woods C Sheppard C Medical therapy in acro-megaly Nat Rev Endocrinol 2011 7291ndash300
60Samson SL Ezzat S AACEACE disease state clinical reviewdopamine agonists for hyperprolactinemia and the risk ofcardiac valve disease Endocr Pract 2014 20608ndash16
61 Jaquet P Gunz G Saveanu A Dufour H Taylor J Dong J et alEfficacy of chimeric molecules directed towards multiplesomatostatin and dopamine receptors on inhibition of GHand prolactin secretion from GH-secreting pituitary aden-omas classified as partially responsive to somatostatin ana-log therapy Eur J Endocrinol 2005 153135ndash41
62Barkan AL Halasz I Dornfeld KJ Jaffe CA Friberg RDChandler WF et al Pituitary irradiation is ineffective in nor-malizing plasma insulin-like growth factor I in patients withacromegaly J Clin Endocrinol Metab 1997 823187ndash91
63Eastman RC Gorden P Glatstein E Roth J Radiation therapyof acromegaly Endocrinol Metab Clin North Am 199221693ndash712
64 Jenkins PJ Bates Carson MN Stewart PM Wass JAConventional pituitary irradiation is effective in loweringserum growth hormone and insulin-like growth factor-I inpatients with acromegaly J Clin Endocrinol Metab 2006911239ndash45
65Minniti G Gilbert DC Brada M Modern techniques for pituit-ary radiotherapy Rev Endocr Metab Disord 2008 10135ndash44
66Stapleton CJ Liu CY Weiss M The role of stereotactic radio-surgery in the multimodal management of growth hormone-secreting pituitary adenomas Neurosurg Focus 2010 29E11
67Biermasz NR van Dulken H Roelfsema F Long-term follow-up results of postoperative radiotherapy in 36 patients withacromegaly J Clin Endocrinol Metab 2000 852475ndash82
68Attanasio R Epaminonda P Motti E Giugni E Ventrella LCozzi R et al Gamma-knife radiosurgery in acromegaly a 4-year follow-up study J Clin Endocrinol Metab 2003 883105ndash12
69Minniti G Traish D Ashley S Gonsalves A Brada M Risk ofsecond brain tumor after conservative surgery and radiother-apy for pituitary adenoma update after an additional 10years J Clin Endocrinol Metab 2005 90800ndash4
70Brada M Burchell L Ashley S Traish D The incidence of cere-brovascular accidents in patients with pituitary adenoma IntJ Radiat Oncol Biol Phys 1999 45693ndash8
71Laws ER Sheehan JP Sheehan JM Jagnathan J Jane JA JrOskouian R Stereotactic radiosurgery for pituitary aden-omas a review of the literature J Neurooncol 2004 69257ndash72
420 | QJM An International Journal of Medicine 2017 Vol 110 No 7
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
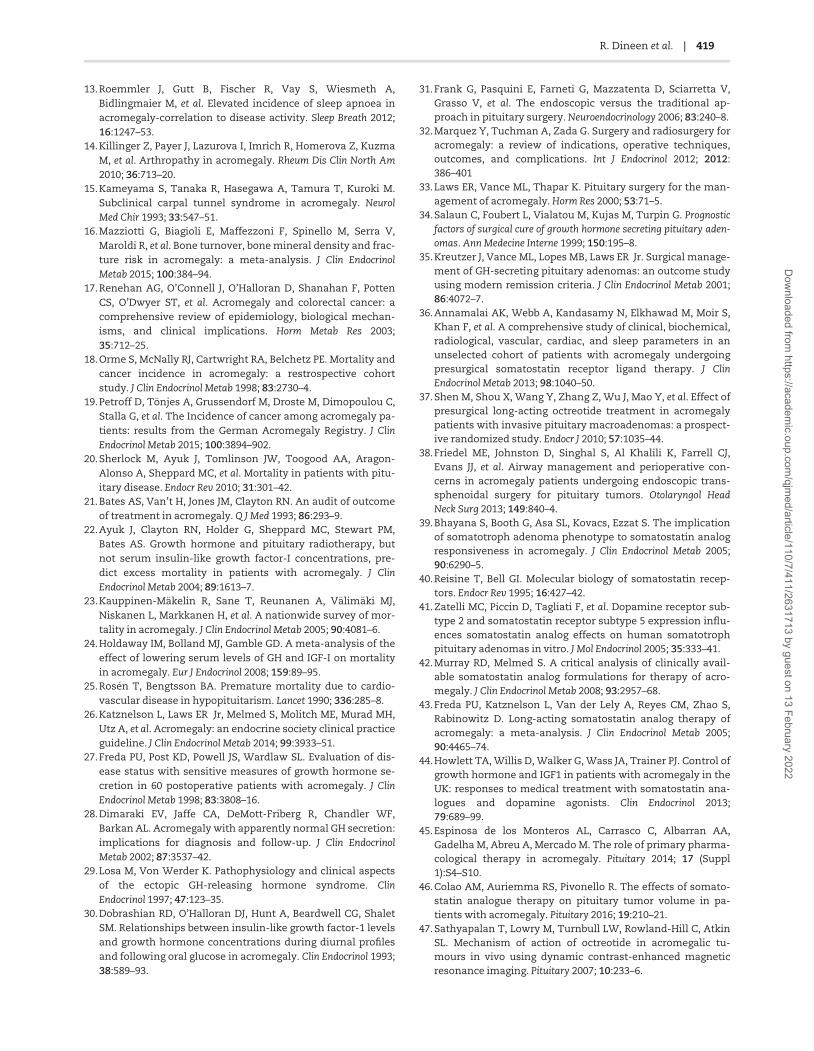
13Roemmler J Gutt B Fischer R Vay S Wiesmeth ABidlingmaier M et al Elevated incidence of sleep apnoea inacromegaly-correlation to disease activity Sleep Breath 2012161247ndash53
14Killinger Z Payer J Lazurova I Imrich R Homerova Z KuzmaM et al Arthropathy in acromegaly Rheum Dis Clin North Am2010 36713ndash20
15Kameyama S Tanaka R Hasegawa A Tamura T Kuroki MSubclinical carpal tunnel syndrome in acromegaly NeurolMed Chir 1993 33547ndash51
16Mazziotti G Biagioli E Maffezzoni F Spinello M Serra VMaroldi R et al Bone turnover bone mineral density and frac-ture risk in acromegaly a meta-analysis J Clin EndocrinolMetab 2015 100384ndash94
17Renehan AG OrsquoConnell J OrsquoHalloran D Shanahan F PottenCS OrsquoDwyer ST et al Acromegaly and colorectal cancer acomprehensive review of epidemiology biological mechan-isms and clinical implications Horm Metab Res 200335712ndash25
18Orme S McNally RJ Cartwright RA Belchetz PE Mortality andcancer incidence in acromegaly a restrospective cohortstudy J Clin Endocrinol Metab 1998 832730ndash4
19Petroff D Teuroonjes A Grussendorf M Droste M Dimopoulou CStalla G et al The Incidence of cancer among acromegaly pa-tients results from the German Acromegaly Registry J ClinEndocrinol Metab 2015 1003894ndash902
20Sherlock M Ayuk J Tomlinson JW Toogood AA Aragon-Alonso A Sheppard MC et al Mortality in patients with pitu-itary disease Endocr Rev 2010 31301ndash42
21Bates AS Vanrsquot H Jones JM Clayton RN An audit of outcomeof treatment in acromegaly Q J Med 1993 86293ndash9
22Ayuk J Clayton RN Holder G Sheppard MC Stewart PMBates AS Growth hormone and pituitary radiotherapy butnot serum insulin-like growth factor-I concentrations pre-dict excess mortality in patients with acromegaly J ClinEndocrinol Metab 2004 891613ndash7
23Kauppinen-Meuroakelin R Sane T Reunanen A Veuroalimeuroaki MJNiskanen L Markkanen H et al A nationwide survey of mor-tality in acromegaly J Clin Endocrinol Metab 2005 904081ndash6
24Holdaway IM Bolland MJ Gamble GD A meta-analysis of theeffect of lowering serum levels of GH and IGF-I on mortalityin acromegaly Eur J Endocrinol 2008 15989ndash95
25Rosen T Bengtsson BA Premature mortality due to cardio-vascular disease in hypopituitarism Lancet 1990 336285ndash8
26Katznelson L Laws ER Jr Melmed S Molitch ME Murad MHUtz A et al Acromegaly an endocrine society clinical practiceguideline J Clin Endocrinol Metab 2014 993933ndash51
27Freda PU Post KD Powell JS Wardlaw SL Evaluation of dis-ease status with sensitive measures of growth hormone se-cretion in 60 postoperative patients with acromegaly J ClinEndocrinol Metab 1998 833808ndash16
28Dimaraki EV Jaffe CA DeMott-Friberg R Chandler WFBarkan AL Acromegaly with apparently normal GH secretionimplications for diagnosis and follow-up J Clin EndocrinolMetab 2002 873537ndash42
29Losa M Von Werder K Pathophysiology and clinical aspectsof the ectopic GH-releasing hormone syndrome ClinEndocrinol 1997 47123ndash35
30Dobrashian RD OrsquoHalloran DJ Hunt A Beardwell CG ShaletSM Relationships between insulin-like growth factor-1 levelsand growth hormone concentrations during diurnal profilesand following oral glucose in acromegaly Clin Endocrinol 199338589ndash93
31Frank G Pasquini E Farneti G Mazzatenta D Sciarretta VGrasso V et al The endoscopic versus the traditional ap-proach in pituitary surgery Neuroendocrinology 2006 83240ndash8
32Marquez Y Tuchman A Zada G Surgery and radiosurgery foracromegaly a review of indications operative techniquesoutcomes and complications Int J Endocrinol 2012 2012386ndash401
33Laws ER Vance ML Thapar K Pituitary surgery for the man-agement of acromegaly Horm Res 2000 5371ndash5
34Salaun C Foubert L Vialatou M Kujas M Turpin G Prognosticfactors of surgical cure of growth hormone secreting pituitary aden-omas Ann Medecine Interne 1999 150195ndash8
35Kreutzer J Vance ML Lopes MB Laws ER Jr Surgical manage-ment of GH-secreting pituitary adenomas an outcome studyusing modern remission criteria J Clin Endocrinol Metab 2001864072ndash7
36Annamalai AK Webb A Kandasamy N Elkhawad M Moir SKhan F et al A comprehensive study of clinical biochemicalradiological vascular cardiac and sleep parameters in anunselected cohort of patients with acromegaly undergoingpresurgical somatostatin receptor ligand therapy J ClinEndocrinol Metab 2013 981040ndash50
37Shen M Shou X Wang Y Zhang Z Wu J Mao Y et al Effect ofpresurgical long-acting octreotide treatment in acromegalypatients with invasive pituitary macroadenomas a prospect-ive randomized study Endocr J 2010 571035ndash44
38Friedel ME Johnston D Singhal S Al Khalili K Farrell CJEvans JJ et al Airway management and perioperative con-cerns in acromegaly patients undergoing endoscopic trans-sphenoidal surgery for pituitary tumors Otolaryngol HeadNeck Surg 2013 149840ndash4
39Bhayana S Booth G Asa SL Kovacs Ezzat S The implicationof somatotroph adenoma phenotype to somatostatin analogresponsiveness in acromegaly J Clin Endocrinol Metab 2005906290ndash5
40Reisine T Bell GI Molecular biology of somatostatin recep-tors Endocr Rev 1995 16427ndash42
41Zatelli MC Piccin D Tagliati F et al Dopamine receptor sub-type 2 and somatostatin receptor subtype 5 expression influ-ences somatostatin analog effects on human somatotrophpituitary adenomas in vitro J Mol Endocrinol 2005 35333ndash41
42Murray RD Melmed S A critical analysis of clinically avail-able somatostatin analog formulations for therapy of acro-megaly J Clin Endocrinol Metab 2008 932957ndash68
43Freda PU Katznelson L Van der Lely A Reyes CM Zhao SRabinowitz D Long-acting somatostatin analog therapy ofacromegaly a meta-analysis J Clin Endocrinol Metab 2005904465ndash74
44Howlett TA Willis D Walker G Wass JA Trainer PJ Control ofgrowth hormone and IGF1 in patients with acromegaly in theUK responses to medical treatment with somatostatin ana-logues and dopamine agonists Clin Endocrinol 201379689ndash99
45Espinosa de los Monteros AL Carrasco C Albarran AAGadelha M Abreu A Mercado M The role of primary pharma-cological therapy in acromegaly Pituitary 2014 17 (Suppl1)S4ndashS10
46Colao AM Auriemma RS Pivonello R The effects of somato-statin analogue therapy on pituitary tumor volume in pa-tients with acromegaly Pituitary 2016 19210ndash21
47Sathyapalan T Lowry M Turnbull LW Rowland-Hill C AtkinSL Mechanism of action of octreotide in acromegalic tu-mours in vivo using dynamic contrast-enhanced magneticresonance imaging Pituitary 2007 10233ndash6
R Dineen et al | 419
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022
48Giustina A Mazziotti G Torri V Spinello M Floriani IMelmed S Meta-analysis on the effects of octreotide ontumor mass in acromegaly PLoS One 2012 7e36411
49Abu Dabrh AM Mohammed K Asi N Farah WH Wang ZFarah MH et al Surgical interventions and medical treat-ments in treatment-naive patients with acromegaly system-atic review and meta-analysis J Clin Endocrinol Metab 2014994003ndash14
50Colao A Bronstein M Freda P Gu F Shen C-C Gadelha Met al Pasireotide versus octreotide in acromegaly a head-to-head superiority study J Clin Endocrinol Metab 2014 99791ndash9
51Schmid HA Schoeffter P Functional activity of the multili-gand analog SOM230 at human recombinant somatostatinreceptor subtypes supports its usefulness in neuroendocrinetumors Neuroendocrinology 2004 80 (Suppl 1)47ndash50
52Mazziotti G Floriani I Bonadonna S Torri V Chanson PGiustina A Effects of somatostatin analogs on glucosehomeostasis a metaanalysis of acromegaly studies J ClinEndocrinol Metab 2009 941500ndash8
53Higham CE Trainer PJ Growth hormone excess and the de-velopment of growth hormone receptor antagonists ExpPhysiol 2008 931157ndash69
54Trainer PJ Drake WM Katznelson L et al Treatment of acro-megaly with the growth hormone receptor antagonist pegvi-somant N Engl J Med 2000 3421171ndash7
55Van der Lely AJ Hutson RK Trainer PJ Besser GM Barkan ALKatznelson L et al Long-term treatment of acromegaly withpegvisomant a growth hormone receptor antagonist Lancet2001 3581754ndash9
56Buchfelder M Weigel D Droste M Mann K Saller B BrubachK et al Pituitary tumor size in acromegaly during pegvisom-ant treatment experience from MR re-evaluations of theGerman Pegvisomant Observational Study Eur J Endocrinol2009 16127ndash35
57 Jaffe CA Barkan AL Treatment of acromegaly with dopamineagonists Endocrinol Metab Clin North Am 1992 21713ndash35
58Sandret L Maison P Chanson P Place of cabergoline in acro-megaly a meta-analysis J Clin Endocrinol Metab 2011961327ndash35
59Sherlock M Woods C Sheppard C Medical therapy in acro-megaly Nat Rev Endocrinol 2011 7291ndash300
60Samson SL Ezzat S AACEACE disease state clinical reviewdopamine agonists for hyperprolactinemia and the risk ofcardiac valve disease Endocr Pract 2014 20608ndash16
61 Jaquet P Gunz G Saveanu A Dufour H Taylor J Dong J et alEfficacy of chimeric molecules directed towards multiplesomatostatin and dopamine receptors on inhibition of GHand prolactin secretion from GH-secreting pituitary aden-omas classified as partially responsive to somatostatin ana-log therapy Eur J Endocrinol 2005 153135ndash41
62Barkan AL Halasz I Dornfeld KJ Jaffe CA Friberg RDChandler WF et al Pituitary irradiation is ineffective in nor-malizing plasma insulin-like growth factor I in patients withacromegaly J Clin Endocrinol Metab 1997 823187ndash91
63Eastman RC Gorden P Glatstein E Roth J Radiation therapyof acromegaly Endocrinol Metab Clin North Am 199221693ndash712
64 Jenkins PJ Bates Carson MN Stewart PM Wass JAConventional pituitary irradiation is effective in loweringserum growth hormone and insulin-like growth factor-I inpatients with acromegaly J Clin Endocrinol Metab 2006911239ndash45
65Minniti G Gilbert DC Brada M Modern techniques for pituit-ary radiotherapy Rev Endocr Metab Disord 2008 10135ndash44
66Stapleton CJ Liu CY Weiss M The role of stereotactic radio-surgery in the multimodal management of growth hormone-secreting pituitary adenomas Neurosurg Focus 2010 29E11
67Biermasz NR van Dulken H Roelfsema F Long-term follow-up results of postoperative radiotherapy in 36 patients withacromegaly J Clin Endocrinol Metab 2000 852475ndash82
68Attanasio R Epaminonda P Motti E Giugni E Ventrella LCozzi R et al Gamma-knife radiosurgery in acromegaly a 4-year follow-up study J Clin Endocrinol Metab 2003 883105ndash12
69Minniti G Traish D Ashley S Gonsalves A Brada M Risk ofsecond brain tumor after conservative surgery and radiother-apy for pituitary adenoma update after an additional 10years J Clin Endocrinol Metab 2005 90800ndash4
70Brada M Burchell L Ashley S Traish D The incidence of cere-brovascular accidents in patients with pituitary adenoma IntJ Radiat Oncol Biol Phys 1999 45693ndash8
71Laws ER Sheehan JP Sheehan JM Jagnathan J Jane JA JrOskouian R Stereotactic radiosurgery for pituitary aden-omas a review of the literature J Neurooncol 2004 69257ndash72
420 | QJM An International Journal of Medicine 2017 Vol 110 No 7
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022

48Giustina A Mazziotti G Torri V Spinello M Floriani IMelmed S Meta-analysis on the effects of octreotide ontumor mass in acromegaly PLoS One 2012 7e36411
49Abu Dabrh AM Mohammed K Asi N Farah WH Wang ZFarah MH et al Surgical interventions and medical treat-ments in treatment-naive patients with acromegaly system-atic review and meta-analysis J Clin Endocrinol Metab 2014994003ndash14
50Colao A Bronstein M Freda P Gu F Shen C-C Gadelha Met al Pasireotide versus octreotide in acromegaly a head-to-head superiority study J Clin Endocrinol Metab 2014 99791ndash9
51Schmid HA Schoeffter P Functional activity of the multili-gand analog SOM230 at human recombinant somatostatinreceptor subtypes supports its usefulness in neuroendocrinetumors Neuroendocrinology 2004 80 (Suppl 1)47ndash50
52Mazziotti G Floriani I Bonadonna S Torri V Chanson PGiustina A Effects of somatostatin analogs on glucosehomeostasis a metaanalysis of acromegaly studies J ClinEndocrinol Metab 2009 941500ndash8
53Higham CE Trainer PJ Growth hormone excess and the de-velopment of growth hormone receptor antagonists ExpPhysiol 2008 931157ndash69
54Trainer PJ Drake WM Katznelson L et al Treatment of acro-megaly with the growth hormone receptor antagonist pegvi-somant N Engl J Med 2000 3421171ndash7
55Van der Lely AJ Hutson RK Trainer PJ Besser GM Barkan ALKatznelson L et al Long-term treatment of acromegaly withpegvisomant a growth hormone receptor antagonist Lancet2001 3581754ndash9
56Buchfelder M Weigel D Droste M Mann K Saller B BrubachK et al Pituitary tumor size in acromegaly during pegvisom-ant treatment experience from MR re-evaluations of theGerman Pegvisomant Observational Study Eur J Endocrinol2009 16127ndash35
57 Jaffe CA Barkan AL Treatment of acromegaly with dopamineagonists Endocrinol Metab Clin North Am 1992 21713ndash35
58Sandret L Maison P Chanson P Place of cabergoline in acro-megaly a meta-analysis J Clin Endocrinol Metab 2011961327ndash35
59Sherlock M Woods C Sheppard C Medical therapy in acro-megaly Nat Rev Endocrinol 2011 7291ndash300
60Samson SL Ezzat S AACEACE disease state clinical reviewdopamine agonists for hyperprolactinemia and the risk ofcardiac valve disease Endocr Pract 2014 20608ndash16
61 Jaquet P Gunz G Saveanu A Dufour H Taylor J Dong J et alEfficacy of chimeric molecules directed towards multiplesomatostatin and dopamine receptors on inhibition of GHand prolactin secretion from GH-secreting pituitary aden-omas classified as partially responsive to somatostatin ana-log therapy Eur J Endocrinol 2005 153135ndash41
62Barkan AL Halasz I Dornfeld KJ Jaffe CA Friberg RDChandler WF et al Pituitary irradiation is ineffective in nor-malizing plasma insulin-like growth factor I in patients withacromegaly J Clin Endocrinol Metab 1997 823187ndash91
63Eastman RC Gorden P Glatstein E Roth J Radiation therapyof acromegaly Endocrinol Metab Clin North Am 199221693ndash712
64 Jenkins PJ Bates Carson MN Stewart PM Wass JAConventional pituitary irradiation is effective in loweringserum growth hormone and insulin-like growth factor-I inpatients with acromegaly J Clin Endocrinol Metab 2006911239ndash45
65Minniti G Gilbert DC Brada M Modern techniques for pituit-ary radiotherapy Rev Endocr Metab Disord 2008 10135ndash44
66Stapleton CJ Liu CY Weiss M The role of stereotactic radio-surgery in the multimodal management of growth hormone-secreting pituitary adenomas Neurosurg Focus 2010 29E11
67Biermasz NR van Dulken H Roelfsema F Long-term follow-up results of postoperative radiotherapy in 36 patients withacromegaly J Clin Endocrinol Metab 2000 852475ndash82
68Attanasio R Epaminonda P Motti E Giugni E Ventrella LCozzi R et al Gamma-knife radiosurgery in acromegaly a 4-year follow-up study J Clin Endocrinol Metab 2003 883105ndash12
69Minniti G Traish D Ashley S Gonsalves A Brada M Risk ofsecond brain tumor after conservative surgery and radiother-apy for pituitary adenoma update after an additional 10years J Clin Endocrinol Metab 2005 90800ndash4
70Brada M Burchell L Ashley S Traish D The incidence of cere-brovascular accidents in patients with pituitary adenoma IntJ Radiat Oncol Biol Phys 1999 45693ndash8
71Laws ER Sheehan JP Sheehan JM Jagnathan J Jane JA JrOskouian R Stereotactic radiosurgery for pituitary aden-omas a review of the literature J Neurooncol 2004 69257ndash72
420 | QJM An International Journal of Medicine 2017 Vol 110 No 7
Dow
nloaded from httpsacadem
icoupcomqjm
edarticle11074112631713 by guest on 13 February 2022





























