Embed Size (px)
Citation preview

Saeid R. Doustjalali1
Rohana Yusof1
Cheng-Har Yip2
Lai-Meng Looi3
Bhanumathy Pillay4
Onn H. Hashim1
1Department ofMolecular Medicine
2Department of Surgery3Department of Pathology,Faculty of Medicine,University of Malaya,Kuala Lumpur, Malaysia
4Gribbles Pathology,Wisma KT,Petaling Jaya,Selangor, Malaysia
Aberrant expression of acute-phase reactantproteins in sera and breast lesions of patientswith malignant and benign breast tumors
We have analyzed unfractionated sera of newly diagnosed patients (n = 10) with breastcarcinoma (BC), prior to treatment, and patients (n = 5) with fibrocystic disease of thebreast (FDB) by two-dimensional gel electrophoresis (2-DE) and silver staining. Thepatients’ 2-DE serum protein profiles obtained were then subjected to image analysisand compared to similar data generated from sera of normal healthy female controls(n = 10) of the same range of age. The relative expression of a1-antichymotrypsin(ACT), clusterin, and complement factor B was significantly higher in all BC patientsas compared to normal controls. However, the expression of a1-antitrypsin (AAT) inBC patients was apparently lower than that of the controls. Similar differential expres-sion of ACT was detected in the FDB patients. The aberrant expression of the serumacute-phase proteins of patients with BC and FDB was confirmed by competitiveenzyme-linked immunosorbent assay (ELISA). Similar altered proteins expressionwas also observed from immunohistochemical studies of malignant (n = 5) and benign(n = 5) breast lesions of the respective patients performed using antisera to the aber-rantly expressed proteins. However, the malignant breast lesions were instead posi-tively stained for AAT. The differential expression of the serum proteins was apparentlyabrogated when a six-month follow-up study was performed on nine of the BC patientssubsequent to treatment.
Keywords: Acute-phase protein / Breast cancer / Serum protein profilesDOI 10.1002/elps.200305950
1 Introduction
Acute-phase proteins are sensitive biomarkers for inflam-mation, infection, cancer, and trauma. They are valuableanalytes to monitor for assessment of diseases and injury.The analysis and studies of acute-phase proteins are cur-rently performed individually although the acute-phaseresponse is a highly orchestrated process involvingmany cell types and the simultaneous altered expressionof many serum proteins (see [1] for review). Acute-phaseproteins like the C-reactive protein [2] and serum amyloidA [3] are commonly used to provide indication of inflam-
mation. These proteins serve as effective biomarkers astheir levels are subjected to 1000-fold alteration in re-sponse to an inflammation. In the case of cancer, theacute-phase proteins provide a guide to the behavior ofmetastases. They are indicators of the risk of infection inleukopenic states, the risk of declining performance sta-tus in advance disease and the risk of progression orrecurrence in advance tumors at presentation (see [4] forreview). The proteomic approach may offer a paradigmshift in the study of acute-phase response. By subjectingsera or plasma to 2-D gel electrophoresis (2-DE), high-resolution profiles of proteins involved in an acute-phaseresponse may be studied simultaneously for both theirquantitative and qualitative differences (see [5] for review).
In the present study, we have subjected unfractionatedsera from patients with breast carcinoma (BC) and fibro-cystic disease of the breast (FDB) to 2-DE and comparedthe serum protein profiles obtained with similarly derived2-DE serum protein profiles of normal female controls.Our data demonstrate the aberrant expression of severalacute-phase proteins of patients with BC and FDB. This isconfirmed by ELISA as well as immunohistochemicalstudies of the patients’ tissues.
Correspondence: Prof. Onn H. Hashim, Department of Molecu-lar Medicine, Faculty of Medicine, University of Malaya, 50603Kuala Lumpur, MalaysiaE-mail: [email protected] or [email protected]: 1603-7967-4957
Abbreviations: AAT, a1-antitrypsin; ABG, a1-B glycoprotein;ACT, a1-antichymotrypsin; AHS, a2-HS glycoprotein; BC, breastcarcinoma; CFB, complement factor B; CLU, clusterin; FDB,fibrocystic disease of the breast; HAP, haptoglobin (b-chain);HRP, horseradish peroxidase; Ig, immunoglobulin; PR1–3, un-identified proteins
2392 Electrophoresis 2004, 25, 2392–2401
2004 WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim

Electrophoresis 2004, 25, 2392–2401 Aberrant acute-phase proteins expression in patients with breast tumor 2393
2 Materials and methods
2.1 Serum samples
Serum samples were obtained from ten female BCpatients (with ages ranging from 40–65 yrs) prior to treat-ment and five female patients with FDB (of similar agerange) at the University of Malaya Medical Centre, KualaLumpur. All BC patients were histopathologically con-firmed with infiltrating ductal carcinoma for either stage2a (T2N0M0) or stage 2b (T2N1M0). Control sera wereobtained from ten normal female volunteers of the samerange of age. Serum samples were again collected fromnine of the BC patients six months after treatment, whichinvolved mastectomy/lumpectomy, chemotherapy forsix cycles (FEC regime), followed by radiotherapy, andtamoxifen (at 20 mg daily) for nine of the oestrogen recep-tor positive patients. Samples obtained were with con-sent in accordance with approval granted by the EthicalCommittee (Institutional Review Board) of the MedicalCentre. All samples were kept at 2207C and subjectedto similar treatment.
2.2 Isoelectric focusing
Seven mL (450 mg protein) of unfractionated whole humanserum samples were diluted in 21 mL sample buffer con-taining 9 M urea, 0.5% v/v Triton X-100, 2% v/v IPG bufferpH 4–7, and 60 mM DTT and left at room temperature for30 min. The mixture was added with 172 mL rehydrationsolution containing 8 M urea, 0.5% v/v Triton X-100,0.5% v/v IPG buffer pH 4–7, and 12 mM DTT and incu-bated for another 30 min. Precast immobilized dry stripspH 4–7, 11 cm (Amersham Biosciences, Uppsala, Swe-den), were then rehydrated in the above prepared solutioncontaining the serum samples (200 mL) and incubated for18 h at room temperature. Swollen strips were then sub-jected to isoelectric focusing, which was performed intwo steps using the Multiphor II Electrophoresis System(Amersham Biosciences) by varying the voltage as pre-viously described [6].
2.3 SDS-PAGE
For the second dimension, the strips were incubated for15 min in a solution consisting of 6 M urea, 2% w/v SDS,30% v/v glycerol, and 0.06 M DTT that was dissolved in1.5 M Tris-HCl (pH 8.8). This was followed by incubationfor another 15 min in a similar solution but containing240 mM iodoacetamide instead of DTT. Strips wereplaced on a SDS-PAGE 8–18% gradient gel and electro-phoresed at 50 V for the first 30 min. The voltage wassubsequently increased to 600 V for the next 95 min.All samples were analyzed in triplicate.
2.4 Silver staining
The 2-DE gels were developed by silver staining as pre-viously described by Heukeshoven and Dernick [7]. Formass spectrometric analysis, gels were stained accord-ing to the method of Shevchenko [8].
2.5 MALDI-TOF protein analysis
Protein spots were initially identified by comparing re-solved serum protein profiles with the SWISS ExPASystandard plasma protein reference [9]. Confirmation ofa1-antichymotrypsin (ACT), a1-antitrypsin (AAT), a1-B gly-coprotein (ABG), a2-HS glycoprotein (AHS), complementfactor B (CFB), and b-chain of haptoglobin (HAP) was per-formed by using the Ettan MALDI-ToF Pro. In-gel trypsindigestion was performed according to the method ofShevchenko [8]. Mass analyses were performed by mix-ing 1 mL of extracted sample with equal volume of matrixsolution consisting of 10 mg/mL a-cyano-4-hydroxycin-namic acid in 0.5% TFA and 50% ACN. Only 0.3 mL ofthe solution was finally spotted onto the slide loader.
2.6 N-Terminal peptide sequencing
Clusterin (CLU) as well as AHS and ABG spots werefurther confirmed by subjecting to N-terminal peptide se-quencing performed by Midwest Analytical Inc.,St. Louis,MO, USA, subsequent to their transfer onto PVDF mem-brane and staining with Coomassie Brilliant Blue R-250.
2.7 Database searches
The MASCOT program (www.matrixscience.com) wasused to search protein database. MASCOT uses peptidemass fingerprints (PMFs) to search database for match-ing peptides from known proteins. The following parame-ters were used in the searches: trypsin digest (one missedcleavage allowed); species: Homo sapiens; mass value:monoisotropic; peptide mass tolerance: 6 0.1 Da; pep-tide charge state: 11 and NCBInr database. Identificationwas again confirmed using the Amersham BiosciencesEttan MALDI software.
2.8 Image analysis
Protein spots were analyzed in terms of volume, per-formed by using the Molecular Analyst PDQuest densi-tometry software (Bio-Rad, Hercules, CA, USA). Thebackground was subtracted and analysis was restrictedto ten clusters of protein spots with Mr � 30 000 distinc-tively separated by 2-DE, i.e., ACT (6 spots), AAT (4 spots),
2004 WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim
Pro
teo
mic
san
d2-
DE

2394 S. R. Doustjalali et al. Electrophoresis 2004, 25, 2392–2401
CLU (6 spots), AHS (5 spots), CFB (7 spots), HAP (6 spots),ABG (4 spots), PR1 (4 spots), PR2 (3 spots), and PR3(6 spots). Albumin, serum polypeptides having idio-typic and/or allotypic variations (such as the heavy andlight chains of all isotypes of immunoglobulins and thea-chains of haptoglobin) and the low-Mr protein spots,the majority of which were not well resolved under thesettings of our experiments, were not assessed. Thepercentage of volume contribution refers to the volumepercentage of a protein taken against the total spot vol-ume of all proteins including the unresolved peptides ineach gel.
2.9 Competitive ELISA
Microtiter plates (Nunc, Demark) were coated overnightat 47C with human serum at 1:1000 dilution in 0.05 M car-bonate-bicarbonate buffer, pH 9.6. Plates were washedextensively with phosphate-buffered saline (PBS) con-taining 0.05% v/v Tween 20 (PBS-Tween). Nonspecificbinding sites were blocked with 0.5% gelatine in PBS-Tween. After washing, plates were incubated with variousappropriately diluted primary antisera comprising sheepanti-human AAT (Code PC034), sheep anti-human ACT(Code PC033), sheep anti-human CFB (Code PC029),and mouse anti-human CLU (Cat. No. 05–354) in theabsence and presence of sera of patients and normalcontrols at 1:1000 dilution in PBS-Tween for 1.5 h atroom temperature. With exception of the mouse anti-hu-man CLU, which was purchased from Upstate Biotech-nology (Lake Placid, NY, USA), all other primary antiseraused were supplied by the Binding Site Limited (Birming-ham, UK). Blanks were prepared by addition of PBS-Tween instead. Following extensive wash with PBS-Tween, 200 mL of diluted horseradish peroxidase (HRP)-conjugated secondary antisera of either donkey anti-sheep immunoglobulin G (IgG) (Code AP360; the BindingSite Limited) or goat anti-mouse IgG (Product No. A 2304;Sigma Aldrich, St. Louis, MO, USA) were added to eachwell. Plates were further incubated for 1 h at room temper-ature and washed extensively with PBS-Tween. Enzymeactivity was revealed with 0.5 mg/mL o-phenylenedia-mine dihydrochloride and 0.012% v/v H2O2 in 1 M sodiumcitrate buffer, pH 5. Reactions were terminated by addi-tion of 100 mL H2SO4 and absorbance values were readat 490 nm. The amount of specific acute-phase proteinsin the test sera is proportional to the inhibition of substratehydrolysis.
2.10 Immunohistochemical studies
Sections (5 mm thick) from malignant infiltrative ductal car-cinoma, benign and normal breast lesions were mountedon adhesive-coated slides, deparaffinized, and rehydrat-
ed through xylene and alcohol. Mounted slides werewashed in tap water for 5 min and kept in DAKO Targetretrieval solution (Glostrup, Denmark) for 40 min at 967C.After cooling for 20 min slides were washed in tap waterand kept in PBS for another 10 min. Endogenous perox-idase was blocked with 3% H2O2 in 0.1% sodium azidefor 15 min and washed with PBS. Nonspecific bindingwas blocked with diluted swine serum in PBS. Sectionswere incubated with diluted primary antisera that weresimilar to that used in ELISA for 1 h at room temperature.The primary antibody for AAT, ACT, CFB, and CLU usedwere diluted at 1:600, 1:200, 1:400, and 1:400, respec-tively. After PBS washes, the sections were incubatedwith HRP-conjugated secondary antisera (at 1:100 dilu-tion), also similar to that used for the ELISA, for 30 min.Staining was performed by incubating with freshly pre-pared diaminobenzidine tetrahydrochloride chromogensolution for 10 min subsequent to washes with PBS. Sec-tions were washed in running tap water and lightly coun-terstained with hematoxylin, followed by dehydration andcoverslip mounting. Negative controls were obtained byomitting the primary antibody. Protein expression wasscored as follows: negative if no staining was seen or ifimmunoreactivity was observed in less than 10% of tumorcells, and positive if more than 10% of tumor cellsshowed staining.
2.11 Statistical analysis
All values are presented as mean 6 SD. The Student’st-test was used to analyze the significance of differencesbetween normal subjects and patients. A p-value of lessthan 0.05 was considered significant.
3 Results
Separation of unfractionated sera of normal healthyfemale controls by 2-DE generated high-resolution serumprofiles comprising only the high-abundance proteins.Proteins that were detected by silver staining includealbumin, the heavy and light chains of IgA, IgG, and IgM,CLU, AHS, ABG, AAT, CFB, and HAP (Fig. 1a). Whenunfractionated serum samples from ten newly diagnosedfemale patients with BC and five female patients with FDBof the same range of age were subjected to 2-DE and sil-ver staining, different protein profiles were obtained.Panels b and c of Fig. 1 demonstrate typical representa-tive unfractionated 2-DE serum protein profiles of the BCand FDB patients, respectively. When compared to thecontrol profiles, the 63 kDa PR3 polypeptide was appar-ently not expressed in the serum protein profiles of all BCpatients and faintly detected in one of the FDB patients.
2004 WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim

Electrophoresis 2004, 25, 2392–2401 Aberrant acute-phase proteins expression in patients with breast tumor 2395
Figure 1. Typical serum protein profiles of normal healthyfemale controls and patients with BC and FDB.Unfractionated serum samples of normal healthy femalecontrols were subjected to 2-DE and silver staining. (a)Typical serum protein profile of a normal female subject.Besides albumin and immunoglobulins, the methodresolved nine clearly detectable clusters of protein spotsincluding AAT, AHS, HAP, CLU, ABG, CFB, PR1, PR2 andPR3. (b), (c) Typical representative unfractionated serumprotein profiles of the BC and FDB patients, respectively.The ACT spots were additionally detected whilst the 63kDa PR3 polypeptides were generally not expressed in allBC and FDB patients. Acid sides of all 2-DE gels are to theleft and relative molecular mass declines from the top.
The spots of ACT, which were generally not expressed inthe 2-DE serum protein profiles of normal healthy femalecontrols, were clearly detected in the serum protein pro-files of all BC and FDB patients.
Preliminary identification of the protein spots was per-formed by comparing resolved 2-DE serum protein pro-files with the standard SWISS ExPASy plasma proteinreference [9]. The spot clusters of AAT, ABG, AHS, CFB,HAP, and ACTwere then confirmed by mass spectrometryusing the Ettan MALDI-ToF Pro (Table 1). Mass spectro-metric analyses were performed on digested spots of theindividual respective proteins that were then pooled andconcentrated by lyophilization. The Mr referred in Table 1are the nominal masses of the amino acid backbones ofthe proteins (without modifications) calculated from thedata bank. Confirmation of CLU as well as AHS and ABGwas performed by N-terminal peptide sequencing of theprotein spot clusters (N-terminal sequences of DQTVSDNELQ, APHGP GLIYR, and AIFYE TQPSL, respectively).In addition to the above proteins, three other spot clus-ters, termed PR1, PR2, and PR3, were also detected.Identities of these proteins were not resolved even whensubjected to the Ettan MALDI-ToF protein analysis. Whencompared to the SWISS ExPASy standard plasma pro-tein reference [9], PR3 appeared to be closely related tothe unidentified protein with primary accession numberP30087. Peptide sequencing was not possible as theprotein spots would not stain with Coomassie BrilliantBlue R-250, Ponceau S, and Amido Black dyes.
Image analysis performed on triplicate 2-DE gels of eachserum sample indicated high reproducibility of percent-age values of volume contribution of all serum proteinspots analyzed (Table 2). When the analysis was per-formed on the silver-stained 2-DE serum protein profilesof ten BC patients as compared to ten normal female con-trols, higher expression of ACT (31-fold; p = 0.0001), CLU(9-fold; p = 0.0001), CFB (4-fold; p = 0.0001), and PR2 (8-fold; p = 0.0008) in the 2-DE serum protein profiles of BCpatients was significantly demonstrated (Fig. 2). However,the expression of AAT and PR3 appeared to be lower by0.3-fold (p = 0.0001) and 674-fold (p = 0.0001), respec-tively, in patients. The relative expression of the serumproteins analyzed is summarized in Table 3.
Similar analyses performed on sera of the five patientswith FDB (ages 40 to 65 years) as compared to that iso-lated from ten healthy volunteers of the same range of agealso demonstrated aberrant protein expression. Never-theless, only two serum proteins were differentiallyexpressed. Like that of the BC sera, the higher expressionof ACT (34-fold; p = 0.0001) and lower expression of PR3(72-fold; p = 0.0001) were significantly detected in the2-DE serum protein profiles of FDB patients. However,
2004 WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim

2396 S. R. Doustjalali et al. Electrophoresis 2004, 25, 2392–2401
Table 1. Mass spectrometric identification of spot clusters from serum protein profiles
Spot IDa) MASCOTaccessionnumberb)
Mr (kDa)/calculatedpI
No. of peaksmatched(No. of peakssearched)
MASCOTscore
Sequencepercentcoverage
AAT giu1942953 44.26/5.43 9 (12) 99 33ACT giu6980544 45.27/5.26 8 (21) 60 24ABG giu23503038 54.17/5.45 8 (22) 58 21CFB giu584908 85.47/6.67 19 (34) 103 34AHS giu4502005 39.30/5.43 7 (22) 55 27HAP giu3337390 38.20/6.14 6 (9) 60 17
a) Spot IDs are as in Fig. 1. Mr, nominal massb) Accession numbers are from the MASCOT database (www.matrixscience.com)
the expression of CLU, AAT, ABG, AHS, HAP, CFB, PR1,and PR2 proteins was comparable to that of the controls(Fig. 2; Table 3).
Figure 2. Mean percentage of volume contribution of2-DE detectable serum proteins of patients with breasttumors. Volumes of protein spots were analyzed by theMolecular Analyst PDQuest densitometry software (Bio-Rad, Hercules, CA, USA). Analysis was restricted to tenclusters of protein spots. Albumin, immunoglobulins, andunresolved protein spots were not included in the analy-sis. CON, BC, and FDB refer to normal controls (n = 10),breast carcinoma patients (n = 10) and patients with fibro-cystic disease of the breast (n = 5), respectively. The rela-tive expression of the serum proteins analyzed is summa-rized in Table 3.
In the case of the BC patients, a follow-up study was per-formed on sera of nine of the patients who respondedpositively to treatment after six months. Panel a of Fig. 3demonstrates a typical representative unfractionated2-DE serum protein profile of the treated BC patients.The differential expression of ACT, CLU, AAT, CFB, andPR2 was apparently normalized subsequent to treatment.
Table 2. Reproducibility assessment of replicate 2-DEgels
Serumproteins
Mean % of volume contribution 6 RSD(%)
Gel 1 Gel 2 Gel 3
ControlABG 0.9637 0.9636 0.9635 0.01AAT 11.0854 11.0854 11.0853 0.0009ACT 0 0 0 0AHS 3.4055 3.4056 3.4055 0.002CLU 0.2473 0.2474 0.2475 0.04HAP 6.4636 6.4636 6.4635 0.001CFB 0 0 0 0PR1 1.1139 1.1138 1.1139 0.008PR2 0 0 0 0PR3 1.7202 1.7203 1.7202 0.005
PatientABG 1.4092 1.4093 1.4092 0.007AAT 4.2289 4.2288 4.2289 0.002ACT 2.9575 2.9576 2.9575 0.003AHS 4.4385 4.3284 4.3285 0.002CLU 3.4371 3.4372 3.4371 0.002HAP 3.0984 3.0983 3.0985 0.003CFB 2.0774 2.0775 2.0773 0.004PR1 1.2977 1.2976 1.2975 0.007PR2 2.1649 2.1648 2.1649 0.004PR3 0 0 0 0
This was observed in the 2-DE serum protein profiles of allthe BC patients that were studied. However, the expres-sion of PR3 remained lower (36-fold; p = 0.0001) in thetreated BC patients as compared to normal controls(Fig. 3, panel b).
For confirmation of the aberrantly expressed known pro-teins in sera of the BC and FDB patients, competitiveELISA was carried out using antisera against four of the
2004 WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim

Electrophoresis 2004, 25, 2392–2401 Aberrant acute-phase proteins expression in patients with breast tumor 2397
Table 3. Relative expression of serum proteins analyzed by 2-DE and ELISA
Serumproteins
Analysis by 2-DE Analysis by ELISA
Fold changesa)
in BC patientsFold changesa)
in FDB patientsFold changesa)
in BC patientsFold changesa)
in FDB patients
AAT 20.3 (p = 0.0001) n.s. 20.2 (p = 0.01) n.s.ABG n.s. n.s. n.d. n.d.ACT 131 (p = 0.0001) 134 (p = 0.0001) 10.4 (p = 0.007) 10.3 (p = 0.03)AHS n.s. n.s. n.d. n.d.CFB 14 (p = 0.0001) n.s. 10.2 (p = 0.001) n.s.CLU 19 (p = 0.0001) n.s. 10.6 (p = 0.0001) n.s.HAP n.s. n.s. n.d. n.d.PR1 n.s. n.s. n.d. n.d.PR2 18 (p = 0.0008) n.s. n.d. n.d.PR3 2674b) (p = 0.0001) 272 (p = 0.0001) n.d. n.d.
a) Fold changes is relative to that of the control valuesb) Generally not detected in protein profiles of patients(1) Increase in expression; (2) decrease in expression; (n.s.) not significant; (n.d.) not determined
Figure 3. Analysis of serum protein profiles of BCpatients six months after treatment. Serum samples ofnine treated BC patients were obtained and subjected to2-DE and silver staining. (a) Typical representative serumprotein profile of the treated BC patients. Volumes of pro-tein spots were analyzed by Molecular Analyst PDQuestdensitometry software (Bio-Rad). (b) Volume analysis ofthe six clusters of protein spots that were differentiallyexpressed prior to treatment. CON, BC, and TBC refer tonormal controls (n = 10) and BC patients before (n = 10)and after (n = 9) treatment, respectively.
aberrantly expressed proteins. Figure 4 demonstratesresults of the competitive ELISA performed in the pres-ence of sera of control subjects (n = 10), BC patientsprior to treatment (n = 10), FDB patients (n = 5), andtreated BC patients (n = 9). Higher levels of ACT (panelb; 0.4-fold; p = 0.007), CLU (panel c; 0.6-fold; p =0.0001), CFB (panel d; 0.2-fold; p = 0.001), and lowerlevels of AAT (panel a; 0.2-fold; p = 0.01) were signifi-cantly detected in sera of the nontreated BC patients ascompared to normal controls. In the case of FDBpatients, ACT (panel b) was the only tested protein withlevel that was significantly higher (0.3-fold; p = 0.03) thanthat of normal controls. There was no significant differ-ence in the levels of the four proteins that were testedbetween the treated BC patients and control subjects.The relative expression of the serum proteins analyzedby ELISA are summarized in Table 3.
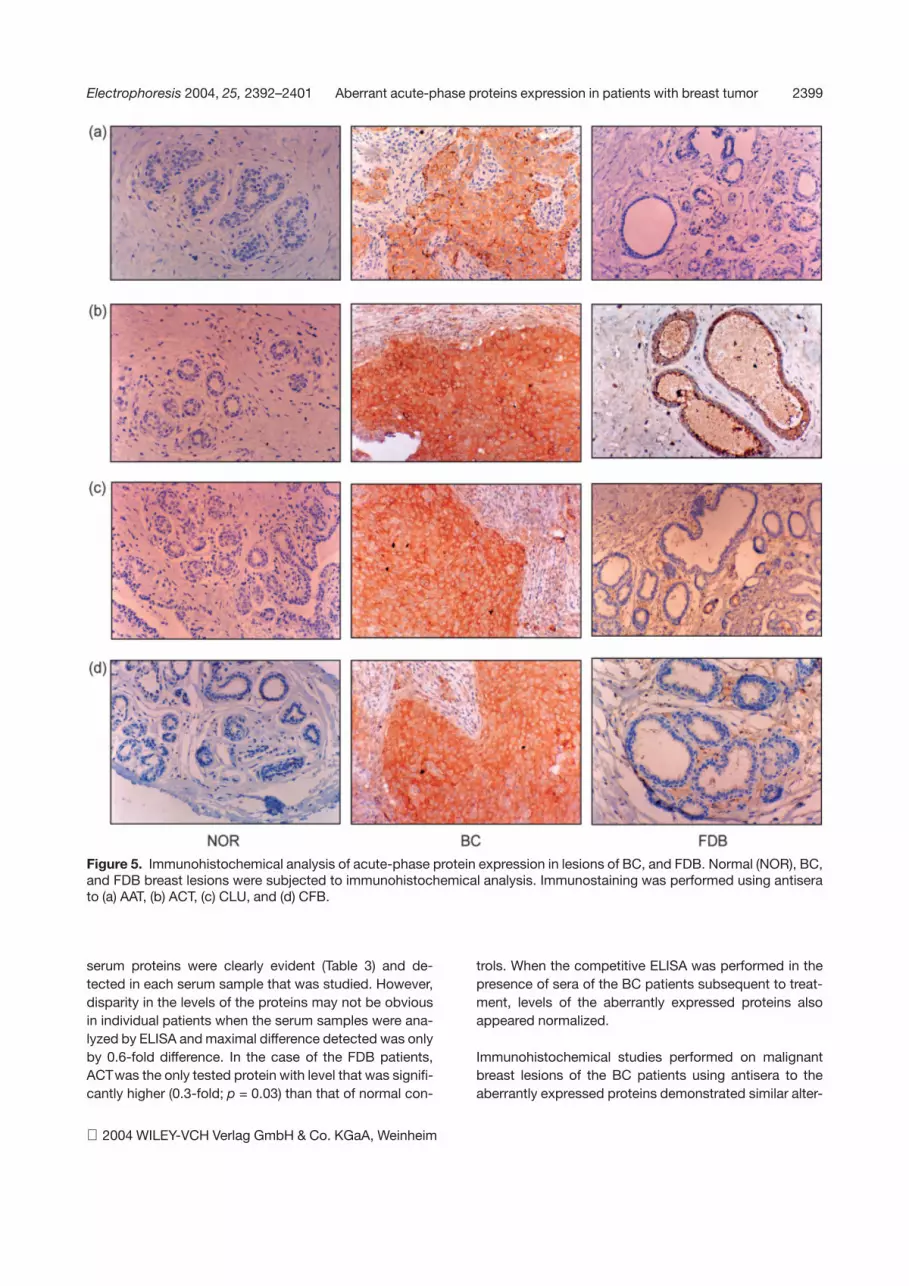
Figure 5 demonstrates results of the immunoperoxidasestudies performed to observe the expression of AAT,ACT, CLU, and CFB in malignant breast lesions with infil-trative ductal carcinoma (n = 5) and benign breast lesionsfrom FDB patients (n = 5), as opposed to normal breastlesions (n = 5). The expression of AAT, ACT, CLU, andCFB was negative in all normal breast lesions studied,with exception of one tissue sample which showed posi-tive staining for CFB. The expression of CLU and CFBwas moderately positive in all malignant breast lesionsand negative in all benign breast lesions, whilst theexpression of ACT was moderately positive in all breastlesions of both the BC and FDB patients. However, theexpression of AAT was positive in the malignant breastlesions of the five BC patients and negative in the benignbreast lesions of the five FDB patients.
2004 WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim

2398 S. R. Doustjalali et al. Electrophoresis 2004, 25, 2392–2401
Figure 4. Analysis of serum acute-phase protein expres-sion by competitive ELISA. Competitive ELISA was per-formed using (a) sheep anti-human AAT, (b) sheep anti-human ACT, (c) mouse anti-human CLU, and (d) sheepanti-human CFB as the primary antibodies, in the pres-ence of sera of control subjects (CON, n = 10), nontreatedpatients with BC (BC, n = 10), FDB patients (FDB, n = 5),and treated BC patients (TBC, n = 9). Analysis was per-formed in triplicate. The amount of AAT, ACT, CLU, andCFB in the test sera is proportional to the inhibition of sub-strate hydrolysis. The relative expression of the serumproteins analyzed by ELISA are summarized in Table 3.
4 Discussion
Comparing the 2-DE serum protein profiles of the BCpatients with that obtained from healthy female controlsindicated differential expression of six detectable pro-teins. The expression of ACT in the serum protein profilesof BC patients was conspicuous although the acute-phase protein spots were generally not detected in con-trol profiles. Whilst the percentages of volume contribu-tion of the CLU, CFB, and PR2 spots were also signifi-cantly higher in BC patients, the expression of AAT andPR3 was apparently lower. Amongst the higher expressedproteins, ACT demonstrated the maximal differencewith 31-fold increment. The levels of CLU, CFB, and PR2were significantly higher by 9-, 4-, and 8-fold difference,respectively. PR3 was generally not detected in serumprotein profiles of BC patients whilst the expression ofAAT was lowered by 0.3-fold. Comparable expressionwas detected for ABG, AHS, HAP, and PR1.
When comparative analysis was made between the 2-DEserum protein profiles of FDB patients and normal con-trols, the expression of only two proteins was found tobe significantly different. Like that of the BC patients,patients with FDB also demonstrated higher expressionof ACT and lower expression of PR3. The level of ACTwas similarly increased by more than 30-fold but thedecrease of PR3 expression was by 72-fold difference.Comparable expression was detected for the other serumproteins that were studied. Each serum cohort of the BCpatients, FDB patients and normal female subjects gener-ated typical 2-DE protein profiles that were visually andanalytically discernible for the aberrantly expressed pro-teins.
When a six-month follow-up study was performed on nineof the BC patients subsequent to treatment, the differen-tial expression of ACT, CLU, AAT, CFB, and PR2, but notPR3, was abrogated. Changes in the expression of theserum proteins of patients with BC subsequent to treat-ment may provide useful information for monitoring pro-gression of the disease since all the nine BC patients hadresponded positively to treatment.
The aberrant expression of proteins that were identified(i.e., AAT, ACT, CLU, and CFB) in the sera of BC and FDBpatients was subsequently confirmed by competitiveELISA. Enhanced levels of ACT, CLU, and CFB and lowerlevel of AAT were detected in sera of the nontreated BCpatients although the average magnitude of deviationwas much smaller as compared to the 2-DE experiments.This is indicative of the gross higher sensitivity of 2-DE ascompared to ELISA when used to differentiate the levelsof the serum proteins. When analyzed by 2-DE, differ-ences between the concentrations of patient and control
2004 WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim
Electrophoresis 2004, 25, 2392–2401 Aberrant acute-phase proteins expression in patients with breast tumor 2399
Figure 5. Immunohistochemical analysis of acute-phase protein expression in lesions of BC, and FDB. Normal (NOR), BC,and FDB breast lesions were subjected to immunohistochemical analysis. Immunostaining was performed using antiserato (a) AAT, (b) ACT, (c) CLU, and (d) CFB.
serum proteins were clearly evident (Table 3) and de-tected in each serum sample that was studied. However,disparity in the levels of the proteins may not be obviousin individual patients when the serum samples were ana-lyzed by ELISA and maximal difference detected was onlyby 0.6-fold difference. In the case of the FDB patients,ACTwas the only tested protein with level that was signifi-cantly higher (0.3-fold; p = 0.03) than that of normal con-
trols. When the competitive ELISA was performed in thepresence of sera of the BC patients subsequent to treat-ment, levels of the aberrantly expressed proteins alsoappeared normalized.
Immunohistochemical studies performed on malignantbreast lesions of the BC patients using antisera to theaberrantly expressed proteins demonstrated similar alter-
2004 WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim

2400 S. R. Doustjalali et al. Electrophoresis 2004, 25, 2392–2401
ed expression of AAT, ACT, CLU, and CFB. Breast lesionsof the BC patients were moderately positive for CLU,CFB, and ACT. This is compatible with the data generatedfrom the 2-DE serum protein profiles. However, the malig-nant BC lesions were positive for AAT although our dataobtained from the 2-DE experiments on sera of patientswith BC demonstrated lower expression of the acute-phase protein. Immunohistochemical studies performedon benign breast lesions of the FDB patients demon-strated similar altered expression of ACT. The lesions ofpatients with FDB were moderately positive for ACT butnegatively stained for AAT, CLU and CFB. This is well cor-related to the data obtained from the 2-DE experimentson sera.
Alteration of the levels of specific proteins in the seraas well as tissues of BC and FDB patients may be attribut-ed to the changes of their synthesis, secretion and/orplasma/cell clearance. It is unlikely to be a consequenceof hormones like oestrogen on the liver as the levels ofother serum proteins like HAP, AHS, and ABG were notaffected. Enhanced expression of CLU in breast lesionsof BC patients has been previously reported [10]. Theincreased CLU expression in BC tended to correlateinversely with the apoptotic activity of the breast epithelia.The data of our study demonstrate that the expression ofCLU was not only potentiated in the malignant breastlesions of BC patients but also in their sera, and that thetypical overexpression was not observed in FDB patients.Although CLU was not previously listed as an acute-phase protein [1], its ninefold increase in the sera of BCpatients, as shown in this study, categorizes it as one bydefinition.
Unlike CLU, enhanced expression of the acute-phaseproteins ACT and CFB in patients with BC has not beendescribed. ACT is normally present at 0.3–0.6 mg/mL innormal human female serum. Such protein concentrationis usually undetectable when unfractionated serum wassubjected to 2-DE and silver staining under the conditionsof our experiments. The presence of ACTcomplexed withprostate-specific antigen in the cyst fluid of women withgross cystic breast disease has been earlier reported[11, 12]. ACT is apparently synthesised by human benignand malignant breast epithelial cells [13, 14], which mayprovide explanation to its enhanced serum and tissueexpression in the BC and FDB patients subsequent tothe onset of the diseases. The higher expression of ACTin the patients with BC and FDB may also be attributed toits enhanced synthesis in the liver.
In the case of AAT, previous studies performed on severalcancers including BC have indicated an association withan increase in the level of plasma AAT, especially in thelate metastatic stages of the disease [15]. In contrast to
the earlier findings, the data of our 2-DE study demon-strate significantly lower percentage of volume contribu-tion of AAT in sera of BC patients (average of less than33% reduction) as compared to that of normal controls.However, our immunoperoxidase experiments perform-ed on malignant breast lesions of BC patients demon-strated positive AAT stains. This is similar to the dataofKoenig et al. [16], which demonstrated positive AATstaining in 3 of the 5 infiltrative ductal carcinoma thatwere studied. Like ACT, AAT is also synthesized by thehuman MCF-7 breast cancer cells [17], and the synthe-sis of AAT is inversely correlated to their anchorage-independent growth [18]. It was speculated that AATmay play the role of a tumor suppressor as it apparentlyblocked the release of growth modulating substances[19]. The positive AAT stain observed in the malignantbreast lesions of BC patients in our study may be areflection of an acute-phase response to contain thegrowth of the malignant cells. In the long term, this maycause depletion of AAT in the serum as observed fromthe results of our 2-DE experiments. As such a responseis unwarranted in benign conditions, the inverse relation-ship was not observed in the FDB patients. Our 2-DEserum protein profile data of FDB patients were well cor-related to that obtained from immunohistochemicalstudies of breast lesions in the lack of significant differ-ence of their expression of AAT between patients andnormal controls.
We would like to thank Ms. Komala S. Muniandy for herexpert technical assistance in the use of the EttanMALDI-ToF Pro. We are also grateful to Ms. Angela NgMin Hwei, for extending her help in the immunohisto-chemical work. This work was funded by IRPA grant 06-02-03-1005, from the Ministry of Science, Technologyand the Environment, Malaysia.
Received November 25, 2003
5 References
[1] Gabay, C., Kushner, I., N. Eng. J. Med. 1999, 340, 448–454.
[2] van Leeuwen, M. A., van Rijswijk, M. H., Sluiter, W. J., vanRiel, P. L., Kuper, I. H., van de Putte, L. B., Pepys, M. B., Lim-burg, P. C., J. Rheumatol. 1997, 24, 20–27.
[3] Malle, E., De Beer, F. C., Eur. J. Clin. Invest. 1996, 26, 427–435.
[4] Cooper, E. H., Immunol. Ser. 1990, 53, 521–536.
[5] Anderson, N. L., Anderson, N. G., Mol. Cell. Proteomics 2002,1, 845–867.
[6] Abdul Rahman, M., Karsani, S. A., Othman, I., Abdul Rahman,P. S., Hashim, O. H., Biochem. Biophys. Res. Commun. 2002,295, 1007–1013.
[7] Heukeshoven, J., Dernick, R., Electrophoresis 1998, 9, 28–32.
2004 WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim

Electrophoresis 2004, 25, 2392–2401 Aberrant acute-phase proteins expression in patients with breast tumor 2401
[8] Shevchenko, A., Wilm, M., Vorm, O., Mann, M., Anal. Chem.1996, 68, 850–858.
[9] Sanchez, J. C., Appel, R. D., Golaz, O., Pasquali, C., Ravier,F., Bairoch, A., Hochstrasser, D. F., Electrophoresis 1995, 16,1131–1151.
[10] Redondo, M., Villar, E., Torres-Munoz, J., Tellez, T., Morell,M., Petito, C. K., Am. J. Pathol. 2000, 157, 393–399.
[11] Black, M. H., Giai, M., Ponzone, R., Sismondi, P., Yu, H., Dia-mandis, E. P., Clin. Cancer Res. 2000, 6, 467–473.
[12] Malatesta, M., Mannello, F., Sebastiani, M., Gazanelli, G.,J. Clin. Lab. Anal. 2001, 15, 81–86.
[13] Tokes, Z. A., Gendler, S. J., Dermer, G. B., J. Supramol.Struct. Cell Biochem. 1981, 17, 69–77.
[14] Gendler, S. J., Dermer, G. B., Silverman, L. M., Tokes, Z. A.,Cancer Res. 1982, 42, 4567–4573.
[15] Varela, A. S., Lopez Saez, J. J., Cancer Lett. 1995, 89, 15–21.
[16] Koenig, C., Dadmanesh, F., Bratthauer, G. L., Tavassoli, F. A.,Int. J. Surg. Pathol. 2000, 8, 303–315.
[17] Tamir, S., Kadner, S. S., Katz, J., Finlay, T. H., Endocrinology1990, 127, 1319–1328.
[18] Finlay, T. H., Tamir, S., Kadner, S. S., Yavelow, J., Levitz, M.,Endocrinology 1993, 133, 996–1002.
[19] Yavelow, J., Tuccillo, A., Kadner, S. S., Katz, J., Finlay, T. H.,J. Clin. Endocrinol. Metab. 1997, 82, 745–752.
2004 WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim





























