Embed Size (px)
Citation preview


DISEASES OF FEMALE BREAST
By
Prof. Manal El-NemrPathology DepartmentZagazig University

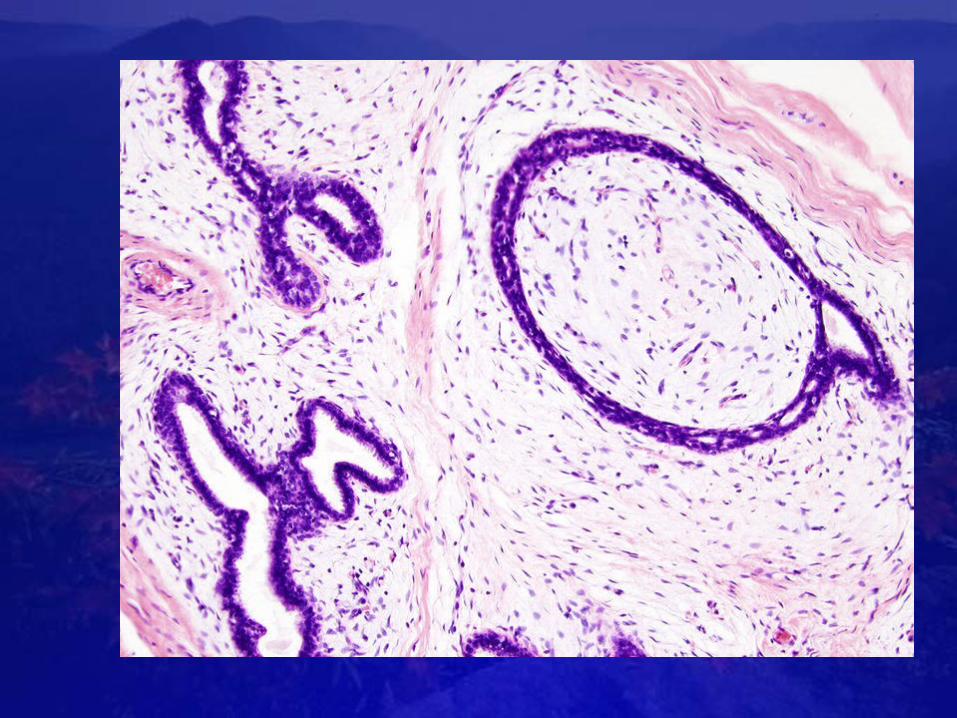
NORMAL ANATOMY OF THE BREAST:A breast is composed of 15 to 25
lactiferous ducts. These ducts start in the nipple and branch to give the terminal ductal lobular unit (TDLU) composed of the intralobular duct, multiple lobular ducts, ductules or
acini & intralobular connective tissue
This part is hormonally responsive.TDLU: site of origin of fibrocystic
change, hyperplasia and carcinomaDucts: site of origin of solitary
papillomas, duct ectasia & the rare ductal carcinomas

Breast profile:A ductsB lobulesC dilated section of duct to hold milkD nippleE fatF pectoralis major muscleG chest wall/rib cage
Enlargement:A normal duct cellsB basement membraneC lumen (center of duct)Find out where and

Female breastInflammation : mastitis,mammary duct ectasia&trumatic fat necrosis
Benign epithelial lesions: non proliferative changes &proliferative changes
Tumours: benign & malignant

I- INFLAMMATORYIDISEASES OF THE BREAST (MASTITIS)

A. ACUTE MASTITISDefinition: Acute inflammation of the
breast.
It usually occurs in lactating women as a result of infection
via the lactating duct system through cracks and fissures of the nipple.
Causative organisms: Staphylococcus aurous and less commonly Streptococci.

Pathologic features:Grossly:
- The breast show signs of inflammation (red, hot and tender)
- The condition is usually unilateral with single or multiple abscesses in cases of staphylococcus infection.
-Streptococci produce diffuse inflammation that may involve the entire
breast.
Microscopically: Abscess formation.

B- CHRONIC MASTITISChronic non specific mastitis:
It follows improper mangment of acute mastitis or is chronic from the start.
- Chronic specific (Granulomatous) mastitis: It may be a part of systemic
granulomatous diseases (e.g., sarcoidosis) or a chronic specific
infectious disease (e.g. T.B., tertiary stage of syphilis and actinomycosis);
taking place in immunocompromised patients.

C- FAT NECROSISCauses: 1. Trauma
2. A consequence of surgical intervention
3. Radiation therapy
Grossly: An early hemorrhagic area is noted,l
later onliquefactive necrosis.
Finally :gryeish white nodules with calcification

Microscopically:1 .Central necrotic fat cells are
surrounded by foamy, lipid-laden macrophages and PNLs.
2 .Late lesions show progressive fibrosis with lymphocytes and histiocytes and
giant cells .3 .Resolution takes place with
replacement of necrotic fat by fibrous tissues and calcified foci.

Microscopically:1 .Central necrotic fat cells are surrounded
by foamy, lipid-laden macrophages and PNLs.2 .Late lesions show progressive fibrosis
with lymphocytes and histiocytes .3 .Resolution takes place with replacement of
necrotic fat by macrophages and giant cells4 .Ultimately a calcified cyst is formed or
complete sclerosis takes place


D- MAMMARY DUCT ECTASIAEtiology: Unknown, but it may represent
a localized response to different components of stagnant colostrum.
Mechanism of mammary duct ectasia:1. Inspissations of secretions in
ducts.2. Dilatation of ducts.
3. Ductal rupture.4. Inflammatory reaction in surrounding
breast.

Microscopically: The ducts are dilated and filled
with acidophilic material. There is periductal chronic granulomatous inflammatory reaction with a striking predominance of plasma cells in some cases.

.Clinically: It can be mistaken for
carcinoma grossly and by mammography
The principal significance of this disorder is that it produces an irregular mass that mimics carcinoma

A. NON PROLIFERATIVE BREAST CHANGE (MAMMARY FIBROCYSTIC CHANGE)
Incidence: It is the most common disorder of breast lesions between 20 and 40 years.
Pathogenesis: It is clue to hormonal imbalance:
Excess estrogens, either absolute increase (e.g. functioning ovarian tumor) or with relative progesterone deficiency. It is
responsible for overgrowth of the mammary parenchyma and stroma not balanced by
regressive changes.N.B. The use of oral contraceptives decreases the risk of these changes

Non proliferative lesion
Grossly: A multifocal, bilateral disorder, sometimes unilateral .ill-defined breast mass,-
- rubbery to firm in consistancy. Cut surface shows some cysts
which are tiny or large (blue-dome cysts).

Microscopically: There are three principle morphologic changes:
1- Cysts: Pathologically dilated sacs lined by epithelium and containing fluid.
Numerous small cysts are usually seen surrounding a large cyst. Sometimes the
epithelial lining is flattened or absent leaving a thick fibrous cyst wall. Rupture
of the cysts initiates an inflammatory response in the stroma, with abundant
foamy macrophages and cholesterol clefts. Cystic changes are often accompanied by
apocrine metaplasia in which the cells have abundant granular eosinophilic
cytoplasm and rounded nuclei resembling normal apocrine epithelium of sweat
glands.

•2 -Fibrosis: The stroma shows marked fibrosis with lymphocytic
and plasma cell infiltrates.•3- Adenosis: Increased number of
acini per lobule. The acini are often enlarged but and lined by
columnar epithelium.


B-Proliferative changes
A -epithelial hyerplasia 1 -atypical ductal epithelial
hyperplasia :.Increase number of the layers of the
duct lining epithelium with atypical changes
2 -cribriform patteren : epithelial cells fill the duct lumen leaving intraepithelialal spaces called fenestration-

3 -duct papiliomatosis : epithelium may project as multiple small papillae into the ducts
3-atypical lobular hyperplasia : proliferation of the cells in terminal ductules that resemble lobular carcinoma in situ

B-Sclerosing adenosisGrossly: grayish white hard mass.
On cut section. The affected area is not well localized and don't have the white streaks of breast carcinoma. Microscopically:
.1-The number of the acini is increased .2-Proliferation of the lining epithelium and
myoepithelial cells in the small ductules 3-Marked stromal fibrosis compress and
distort the proliferating ducts

Epithelial hyperplasia


Clinical significance of benign epithelial changes
- Non proliferative changes do not increase the risk of cancer.
- Proliferative disease is associated with mild increase in risk.
- Proliferative disease With atypia confers moderate degree of increased
risk of cancer development.

III- BREAST TUMORS

A- Epithelial Tumors1- Benign: - Duct papilloma.
- Adenoma (Tubular, lactating and nipple adenoma
2- Malignant: Breast carcinoma.B- Stromal tumors:
1- Benign:- Arising from intralobular stroma: Fibroadenoma and phylloides tumor.- Arising from interlobular stroma: Resembling connective tissue tumors
in other sites e.g. lipoma.2- Malignant: Sarcomas e.g. angiosarcoma, liposarcoma and
leiomyosarcoma.

FIBROADENOMAThe most common benign tumor of the
female breast between 20 and 30 years of age Types:
1- Peri- canalicular fibroadenoma2- Intra- canalicular
fibroadenoma.There are, however, mixed forms.
.

Grossly: Sharply circumscribed, freely mobile, variable sized spherical nodule. It increases in size with menses and pregnancy and may undergo atrophy with menopause. Nodules have smooth surface, they are gray colored and encapsulated .
Cut section shows whorly appearance in cases of pericanalicular type and slits in cases of intracanalicular type

•Microscopically: It is composed of proliferating ducts lined by inner cuboidal epithelial cells and outer flat myoepithelial cells. The ducts
are separated by abundant fibroblastic stroma which is
excessive in the intracanalicular type and so appears as to invaginate the glands & ducts giving them a slit
or star shape .


PHYLLOIDES TUMORSPhylloid as tumor is a giant, lobulated,
cystic mass arising from intralobular stroma (also known as giant intracanalicular
fibroadenoma).Incidence: They may occur at any age, but are
most common in the 6th decade.Grossly: The tumor is a rounded, well-
circumscribed; firm mass with ulceration of the overlying skin. Cut section is grayish- white in color with cleft-like spaces. Areas
of necrosis, cystic degeneration and hemorrhage may be seen especially in huge
lesions..

•Microscopically:•Low grade phylloides resembles
fibroadenoma but with more cellular myxoid stroma. The gland are compressed and distorted by the myxomatous stroma.
•High grade phylloides may be difficult to differentiate from other soft tissue sarcomas with increased stromal cellularity, anaplasia and high mitotic activity.

c- Duct papillomaMost of these lesions are solitary with
benign behavior and arise in the principal lactiferous ducts or sinuses. They lead to
bleeding per nipple.Grossly: Papilloma is a small pedunculated
and friable growth.Microscopically: It is composed of
multiple branching fibrovascular ;cores each having a Connective tissue axis lined
by luminal and myoepithelial cells. Multiple small duct papillomas are associated with increased risk of
malignant transformation.

Duct papilloma

BREAST CARCINOMAPREDISPOSING FACTORS
1- Hormones: Excessive estrogen stimulation whether endogenous (long
duration of reproductive life, nulliparity and ovarian tumors
elaborating estrogen) or exogenous estrogen therapy.
2- Atypical duct or lobular hyperplasia3- Obesity: Increased risk is due to synthesis of estrogen in fat depots.
4- Diet: High lipid diet5- Genetic predisposition: Increased risk
in first degree of cancer patients.


THE WHO CLASSIFICATION:A. Non invasive (non- infiltrating)
carcinoma:a- Ductal carcinoma in situ (intraductal
carcinoma)b- Intraductal carcinoma with Paget's
disease.c- Lobular carcinoma in situ.
B- Invasive carcinoma:1. Infiltrating duct carcinoma:
a. Not otherwise specified (NOS).b. Infiltrating duct carcinoma with
Paget's diseasec. With a predominant intraductal
component.2. Infiltrating lobular carcinoma.
3. Medullary carcinoma.4. Mucinous carcinoma (colloid carcinoma).

5. Tubular carcinoma.6. Adenoid cystic carcinoma.
7. Secretory (juvenile) carcinoma.8. Apocrine carcinoma.
9. Invasive papillary carcinoma.10. Carcinoma with metaplasia.
11. Carcinoma with osteoclast-like giant cells.
.

Distribution: About 50% of breast carcinoma arise in the upper outer quadrant, 10% in each ~of the remaining quadrants and 20% in the central or subareolar region

A- NON INVASIVE CARCINOMA (CARCINOMA IN- SITU)a. Ductal carcinoma in situ:
Definition: It is proliferation of malignant ductal epithelial
cells, inside the duct system, not invading the basement
membrane.Grossly: Poorly defined focus of
firm consistency due to marked dilatation and solidification of
the ducts. Cut section shows cord-like ducts with normal
breast parenchyma between them . In comedo carcinoma, necrotic cheesy material is seen inside the ducts and is extruded from
them.

•Microscopically: The ducts are dilated and filled by pleomorphic malignant
epithelial cells. Several patterns may be seen:
•i- Comedo carcinoma: The ductal proliferation is associated with central necrosis.
•ii- Cribriform pattern: The malignant cells are arranged in a sieve-like configuration.
•iii. Papillary pattern: The cells are arranged as intraductal papillary growth that
lacks a connective tissue core



b. Lobular carcinoma in situ:It is always an incidental biopsy finding,
since it is not associated with calcification or stromal reaction that
produces mammographic changes.Microscopically: The acini are distended with malignant cells, which are loosely cohesive
with oval or round nuclei and small nucleoli. There is no invasion of the
basement membrane.

Lobular carcinoma in situ

B- INVASIVE BREAST CARCINOMAClinical features of invasive
carcinomas:1- Nipple retraction due to fixation of
the tumor to the overlying in skin with retraction of the fibrotic
stroma.2; Peau d'orange appearance of the skin:
this is due to obstruction of the dermal lymphatics by tumor emboli with
skin edema except at points of attachment of adenxa.
3- Cancer en cuirasse: It is hardening and fixation of the breast due to
lymphedema and invasion of pectoral muscle.

Infiltrating duct carcinoma, not otherwise specific (NOS):
It is the most common type (70-80 %)Grossly:
shape sharply delimited,color grayish-white,
Capsule uncapsulated nodules consistany stony hard .
Cut section: gritty sensation of unripe pear is noticed and with areas of
necrosis. The mass has infiltrative attachment to the surrounding-structures with possible fixation to the chest wall, dimpling of the skin (peau d'orange appearance) and
retraction of the nipple.

Microscopically: The tumor consists of small masses, cords and sheets of malignant epithelial cells separated by fibrous tissue stroma. The fibrous stroma may show excessive desmoplastic reaction.

•Desmoplasia is usually only associated with malignant
neoplasms, which can evoke a fibrosis response by invading healthy tissue. Infiltrating
metastatic ductal carcinomas of the breast often have a
scirrhous, stellate appearance caused by desmoplastic formations


Infiltrating lobular carcinoma:It is frequently multifocal and,
bilateral.Grossly: The tumor is rubbery and poorly
circumscribed, but sometimes it appears as infiltrating duct carcinoma.
Microscopically: Strands of malignant cells are loosely dispersed throughout the
stroma in an Indian-file pattern. The cells are monomorphic with large
hyperchromatic nuclei and a little amount of cytoplasm.



Colloid (mucinous) carcinoma:Rare variant occurs in older women and
has a good prognosis.Grossly: The tumor is soft gelatinous in
consistency and appears pale blue in color.
Microscopically: there are two patterns of growth:
i- Pure mucinous carcinoma: Appears as lakes of mucin with small islands of
neoplastic cells. The cells are distended with multiple vacuoles which, sometimes,
give it a signet ring appearance.ii- Mixed mucinous and non mucinous duct
carcinoma.


Medullary carcinoma:It occurs at a younger age group and
accounts for 1% of mammary carcinoma.Grossly: The lesion takes the form of large fleshy well circumscribed tumor
masses.Microscopically: It is characterized by syncytium-like sheets of malignant cells
with vesicular pleomorphic nuclei containing prominent nucleoli and
frequent mitosis. There is lymphocytic filtrate between these sheets with scanty
fibrous component.


Paget's disease of the breast:It is a rare manifestation of breast
cancer. It presents as unilateral erythermatous eruption with a scale crust
(may be mistaken for eczema)Grossly: The skin of the areola and nipple
appears red, moist, and granular and is eroded with an associated malignant mass
in the breast.Microscopically: Infiltration of the
epidermis with malignant Paget's cells which are large oval cells with pale
cytoplasm, vesicular nuclei and prominent nucleoli. The dermis shows edema with
chronic inflammatory cells.Presence of Paget's cells in the epidermis is the hall mark for diagnosis: of Paget's
disease.


SPREAD OF BREAST CANCER:- Direct spread: To the mammary tissue,
pectoralis muscle, ribs, pleura and skin.
- Lymphatic spread: To axillary, internal mammary, mediastinal and
supraclavicular lymph nodes.- Blood spread: To the lung, liver and
bones.



T.N.M. STAGING SYSTEM OF BREAST CANCERTi. Carcinoma in situ.
T1: Tumor mass 2 cm in diameter.T2: Tumor mass 2-5 cm in diameter.T3: Tumor mass 5 cm in diameter.
T4: Tumor mass of any size with invasion of skin or chest wall.
N0. No lymph node metastasis.N1: Metastasis to ipsilateral axillary
nodes without fixation.N2: Metastasis to ipsilateral axillary
nodes with fixation.N3: Metastasis to ipsilateral
infraclavicular or supraclavicular,nodes.
M0: No distant metastasis.M1: Distant metastasis.

Right Breast Carcinoma, Autopsy
Case A71-205 - Clinical. This
patient, a 44 year old white female with a 1 1/2 year history of right breast mass and
pain, refused hospitalization for a probable carcinoma of the right breast when seen by her doctor six
months prior to admission. Four weeks prior to admission, the patient developed nausea, vomiting,
coughing, shortness of breath, fatigue and increasing weakness.


Physical examination on admission revealed a very weak female with a right breast
mass with "peau d'orange" skin
retraction, muscle retraction, and
nontender axillary lymphadenopathy. These
features are recognizable on this
slide. Chest x-ray revealed
the diffuse lymphangitic spread of carcinoma on the lungs
bilaterally with a questionable invasion
of rib and calcification of the right axillary lymph
node.



PROGNOSTIC FACTORS IN BREAST CANCER1- Lymph node metastasis: It is the most
important prognostic factor. Large number involved nodes,
macrometastasis and invasion of the capsule are associated with poor
prognosis.2- Local extension to the skin or
skeletal muscle is associated with poor prognosis.
3- Tumor size: Large size is associated with increased incidence of distant
metastasis.4- Histologic subtype: Tubular, papillary, mucoid and medullary carcinomas favor good prognosis.

5- Tumor grade: High grade tumors are associated with poor prognosis.
6- Estrogen and progesterone receptors: Most tumors with estrogen receptors
regress after hormonal therapy.7- High proliferation rate, measured by
flow cytometry or Ki-67 protein overexpression, is an indicator of
poor prognosis.8- Aneuploid tumors have worse
prognosis.Cell division that result in unequal
separation in genetic material .45 ,47

A gene that causes the transformation of normal cells into
cancerous tumor cells, especially a viral
gene that transforms a host cell into a tumor
cell.
Read more: http://www.answers.com/topic/oncogene#ixzz1H
kqSTpsA
9- Expression of oncogenes, (c-erb B-2, c-myc) and
loss of expression of tumor
suppressor genes (p53, Rb) are
associated with poor prognosis.

THE MALE BREASTGynecomastia
It is unilateral or bilateral enlargement of the male breast which
presents as button-like subareolar enlargement.
Causes: Hormonal imbalance with an increase of estrogenic substances:1- At puberty or in old age (most
frequent).2- Liver cirrhosis.
3- Functioning testicular tumors especially Leydig cell tumors.
Microscopically: Increased dense collagenous connective tissue with
hyperplasia of the ductal epithelium showing micropapillary epithelial
hyperplasia of the duct lining.

Carcinoma of the male breast:It is very rare (1% of that in
women) and occurs more commonly in old age types of female breast
cancer can occur except lobular carcinoma. Dissemination follows the
same pattern as in women. Distant metastases to the brain lung, bones
and liver are common.
























![[Radiological control intraoperatory of a surgical piece in non palpable breast lesions]](https://img.dokumen.tips/doc/110x75/635663192d28d280ca03140f/radiological-control-intraoperatory-of-a-surgical-piece-in-non-palpable-breast.jpg)





