Embed Size (px)
Citation preview

ABSTRACT
Genetic polymorphisms in drug-metabolizing enzymes are now known to be the major
determinants of inter-individual variability in drug response leading to several forms of adverse
drug effects and reactions. Extensive studies has shown that identification of the genetic bases
for polymorphic expression of a gene is done through intronic or exomic Single Nucleotide
Polymorphisms (SNPs) which abolishes the need for different mechanism for explaining the
variability in drug metabolism and fully suggests that the human Cytochrome P450 (CYP)
genes are highly polymorphic. Genetic variation involved in drug metabolism may account for
variations in responses to some drugs and may affect receptor adaptation, toxicity, altered drug
effects and cross tolerance among various groups of individuals. Apart from the other relatively
known genes such as the gluthathione and N-acetyltransferase genes which are largely involved
and responsible for variances in drug metabolism and response. The Cytochrome P450 (CYP)
genes has been proved to be the most common. We have discussed the clinical importance of
the CYP2C9 gene alterations. This review may help researchers to understand the genetic
mechanism and adverse effect of the CYP2C9 gene polymorphism.
Keywords: Single Nucleotide Polymorphism, CYP 2C9, Adverse Drug Reactions, Drug
Metabolism, Warfarin
Name of Author(s) : Minari, J.B., Ogar G.O., Bello, B.
Affliation: Department of Cell Biology and Genetics, Faculty of Science, University of
Lagos.

Overview of the study
Genetic variation involved in drug metabolism may account for variations in responses to some
drugs and may affect receptor adaptation, toxicity, altered drug effects and cross tolerance.
There are several known genes which are largely responsible for variances in drug metabolism
and response (Sohayla et al., 2007). The most common are the Cytochrome P450 (CYP) genes,
which encode enzymes that influence the metabolism of more than 80 percent of current
prescription drugs (Gomes et al., 2009). Cytochrome P450 (CYP) enzymes are key players in
the Phase 1-dependent metabolism of drugs and other xenobiotics, mostly catalysing oxidations
of the substrates, but occasionally also reduction reactions. At present more than 57 active
human P450 genes and 58 pseudogenes are known. According to Berka et al. (2011) Human
CYPs are primarily membrane-associated proteins. The different alleles are summarized at the
Human CYP allele nomenclature committee home page (Figure 1) (www.cypalleles.ki.se)
(Ingelman-Sundberg et al.,2007). In the CYP gene family, the most penetrant genetic
alterations are gene deletions, missense mutations and mutations creating splicing defects and
premature stop codons (Ingelman-Sundberg and Rodriguez-Antona, 2006)). Various
physiological(e.g age, nutrition) and pathological(liver, kidney or heart diseases) factors can
also affect drug metabolism.(Rostami-Hodjegan and Tucker, 2007). Danielson (2002) has
earlier reported the contributory effects of Inhibitors (Sertraline,Sulphaphenazole) and Inducers
(Refampicin,Secobarbital) in the cyp2c9 genome.
The mutations in the CYP genes may cause absence of enzyme, diminished enzyme
expression, enzyme with altered substrate specificity or increased enzyme expression. Based
on the composition of alleles, the affected individual might be divided into four major
phenotypes: Poor Metabolizers (PMs), having two non-functional genes; Intermediate
Metabolizers (IMs), being deficient on one allele; Extensive Metabolizers (EMs), having two

copies of normal genes and Ultra rapid Metabolizers (UMs), having three or more functional
active gene copies (Ingelman-Sundberg and Rodriguez-Antona, 2005).
Figure 1: Importance of the different polymorphic CYP genes as assessed by the number of
hits at the human CYP allele nomenclature home page (www.cypalleles.ki.se)
Source: Ingelman-Sundberg et al.,2007

Figure 2: Selected CYP2C9 substrates. The site(s) of oxidation of each substrate is indicated
by an arrow(s).
Source: www.ncbi.nlm.nih.gov, 2014
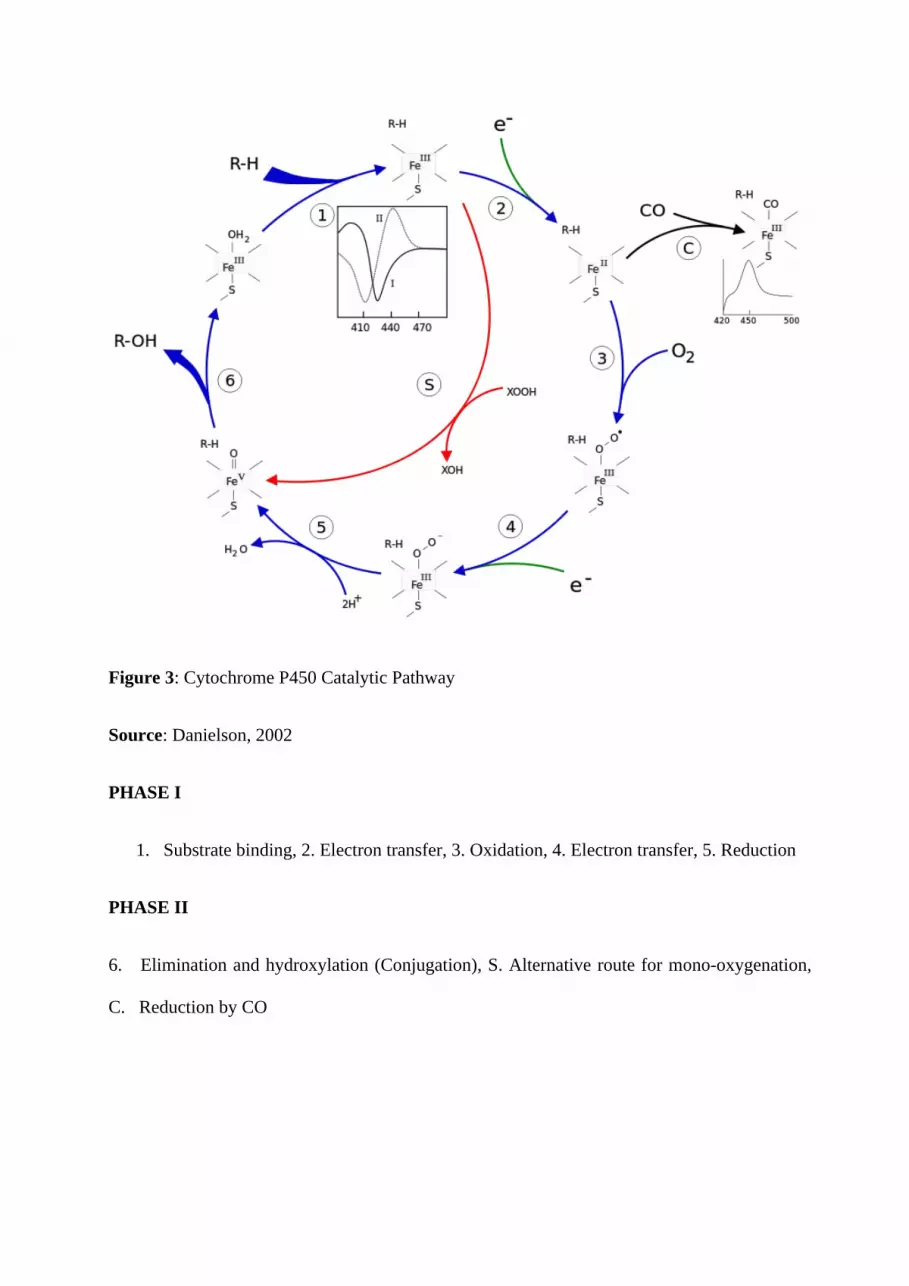
Figure 3: Cytochrome P450 Catalytic Pathway
Source: Danielson, 2002
PHASE I
1. Substrate binding, 2. Electron transfer, 3. Oxidation, 4. Electron transfer, 5. Reduction
PHASE II
6. Elimination and hydroxylation (Conjugation), S. Alternative route for mono-oxygenation,
C. Reduction by CO
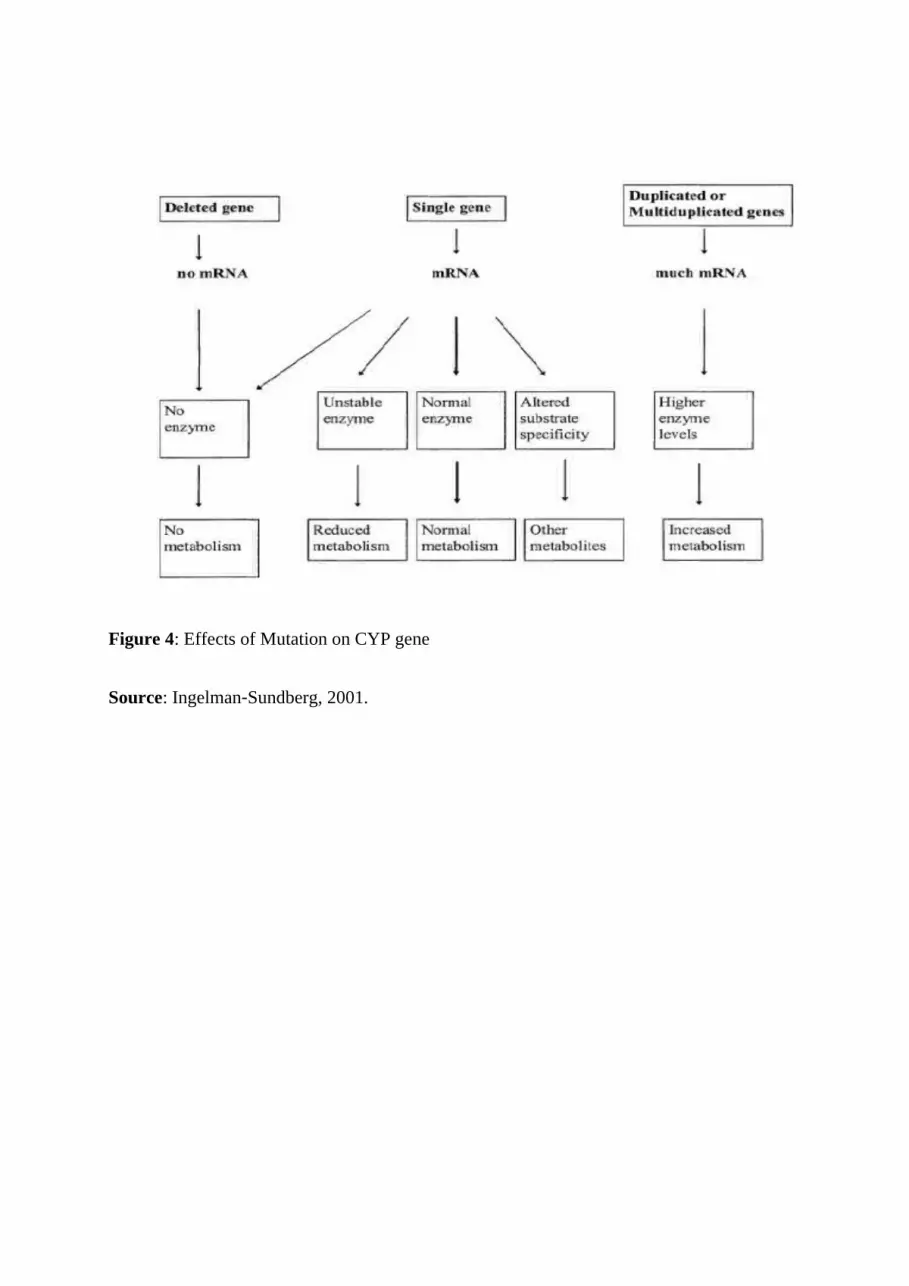
Figure 4: Effects of Mutation on CYP gene
Source: Ingelman‐Sundberg, 2001.

CYP2C9 is a major cytochrome P450 enzyme that is involved in the metabolic clearance of a
wide variety of therapeutic agents, including oral anticoagulants, oral hypoglycaemias, and
nonsteroidal anti-inflammatories. Disruption of CYP2C9 activity by metabolic inhibition or
pharmacogenetic variability underlies many of the adverse drug reactions that are associated
with the enzyme (Allan and Jeffery, 2005). The phenotypes CYP2C9*2 and CYP2C9*3 are the
two most common variations and are associated with reduced enzymatic activity. Impaired
metabolism of drugs metabolized by the CYP2C9 isoenzyme, such as phenytoin, S-warfarin
(Aquilante et al., 2006), tolbutamide, losartan, and nonsteroidal antiinflammatory drugs
(NSAIDs) (e.g., ibuprofen, diclofenac, piroxicam, tenoxicam, mefenamic acid) has been noted.
Noteworthy is that:
CYP2C9 gene is highly polymorphic. (www.imm.ki.se/cypalleles)
CYP2C9 gene is 55 kb long, including 9 exons.
Located on the long arm of chromosome 10.
The CYP2C9 gene encodes a protein of 492 amino acids.
(Wang et al., 2007)
CYP2C9 is a major liver P450 enzyme.
Metabolizes ~15% of the drugs that undergo phase I metabolism
(Rendic, 2002)
CYP2C9 is involved in the metabolic clearance of a wide variety of therapeutic agents.
(Allan and Jeffery, 2005)

Table 1: Common substrates for CYP2C9 by therapeutic class∗Source: Allan and Jeffery, 2005.
CLASS SUBSTRATES
Oral Anticoagulant Warfarin, Acenocoumarol(Phenprocoumon)
Oral
anticonvulsant
Phenytoin(Phenobarbital)
Non-Steroidal
Anti-inflammatory
Drugs (NSAID)
Flurbiprofen,diclofenac,Piroxicam,Suprofen,Ibuprofen,Mefenamic
acid,Celecoxib
Oral
hypoglycaemic
Tolbutamide,Glimepiride,Glyburide,Glipizide
Drug Substrate Metabolism by CYP2C9
Concerning gene variations, it is a well-known fact that CYP2C9 polymorphisms have
functional consequences for in vitro and in vivo pharmacokinetics and for clinical drug
response and side effects. There are more than 30 different SNPs described in the regulatory

and coding region of CYP2C9, but the polymorphic behaviour of CYP2C9 seems to be
determined mainly by 2 common coding variants: CYP2C9*2 (R144C) and CYP2C9*3
(I359L), both yielding enzymes with decreased activity. CYP2C9*2 and CYP2C9*3 are mainly
present in Caucasians (11% and 7% frequency, respectively) while the frequencies are lower in
Africans. In Asians, CYP2C9*2 has indeed not been detected (Kirchheiner & Brockmoller,
2005). CYP2C9 is the principal enzyme responsible for the metabolism of S-warfarin. Persons
who are CYP2C9 poor metabolizers have reduced S-warfarin clearance. Clinical studies have
shown that these persons require lower dosages of warfarin and are at an increased risk of
excessive anticoagulation (Aquilante et al., 2006). Kirchheiner and Brockmoller (2005)
observed that the most relevant CYP2C9 genetic variations which result in decreased activity
are, CYP2C9*2, mainly present in Caucasians with a 10-15% frequency, but almost present in
Africans and Asians, and CYP2C9*3, which has an allele frequency of 4-10% in Caucasians, 4-
7% in Asians and 1-2% in Africans. CYP2C9*2 and *3 were associated with a decrease in the
intrinsic clearance of S-warfarin, respectively, compared with the wild-type allele (Haining et
al., 1996). According to Aithal et al., (1999) Individuals who require a low dose of warfarin to
maintain optimum anticoagulation have a slightly higher frequency of variant alleles than those
who require a higher dose. Increased risk of bleeding was observed in patients with mutant
alleles (Poor Metabolizers), and subsequent dosage adjustments were required (Higashi et al.,
2002). CYP2C9 genotyping may help identify high-risk patients who are candidates for lower
warfarin doses, more frequent monitoring, or alternative drug treatments (Tang et al., 2001).
In vitro results have shown that the substrate affinity of CYP2C9.2 varies as compared with the
wild-type enzyme. Consequently, for some substrates, it is unaffected, but with some other
drugs such as acenocoumarol, the activity is severely decreased. The CYP2C9.3 protein,
containing the conservative amino acid substitution I359L, results in a significant reduction of
the catalytic activity with only around 10% of the intrinsic clearance of the wild-type enzyme
for most CYP2C9 substrates (Thijssen & Ritzen, 2003). CYP2C9 2 and/or 3 have been⁎ ⁎
shown to affect the oral clearance of at least 17 different CYP2C9 drugs: S-acenocoumarol, S-
phenprocoumon, S-warfarin, glimepiride, glyburide, tolbutamide, nateglinide, candesartan,
losartan, celecoxib, diclofenac, flubiprofen, S-ibuprofen, tenoxicam, fluvastatin, phenytoin and
torsemide (Kirchheiner & Brockmoller, 2005),

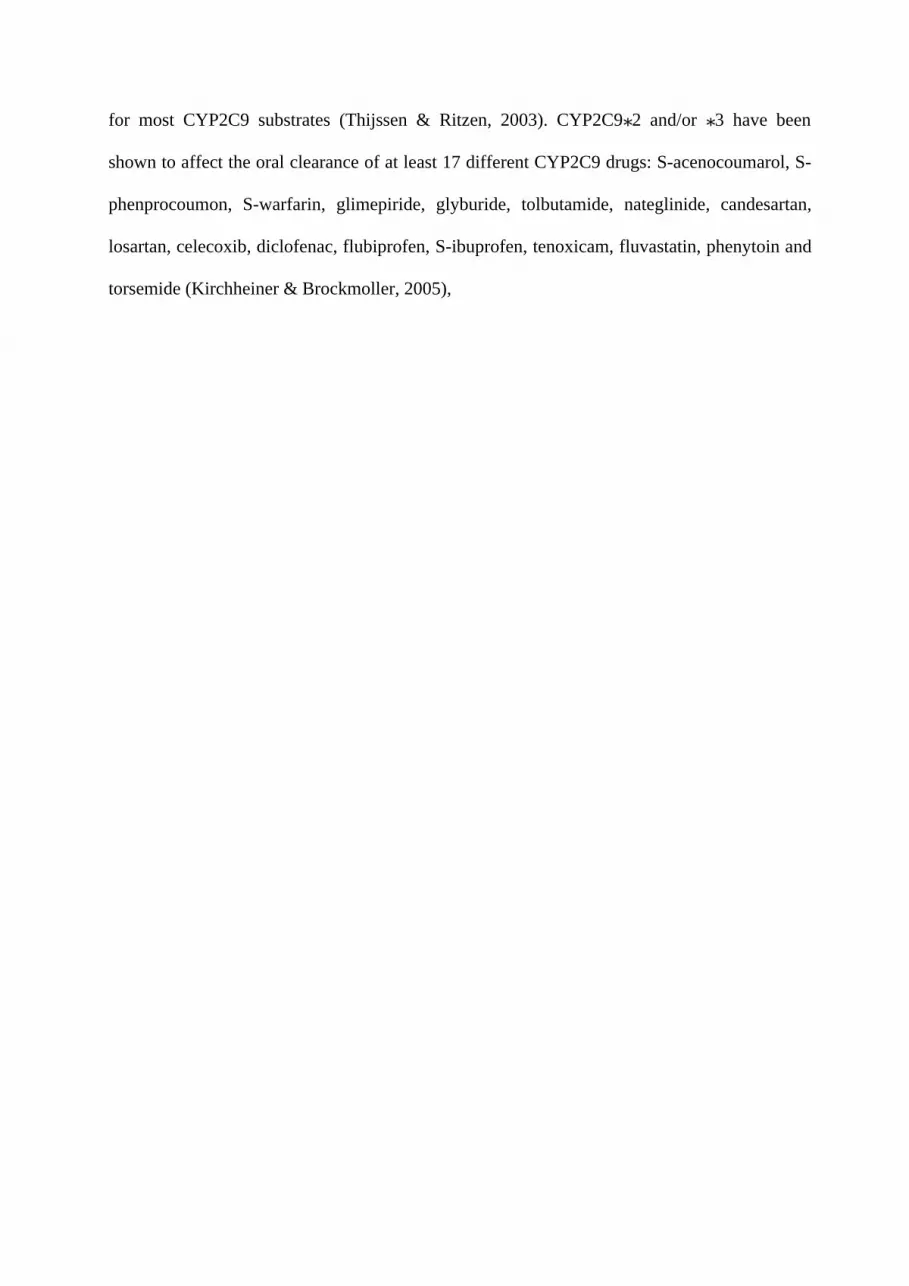
Figure 5: Potential Benefit of Adjusting Dose to Genotype
Source: Kirchheiner et al., 2005
GENETIC POLYMORPHISM OF CYP2C9 GENE

Genetic polymorphism exists for CYP2C9 expression because the CYP2C9 gene is
highly polymorphic (Sim, 2011).
Common Variants: CYP2C9*1 (wild-type)
CYP2C9*2
CYP2C9*3
CYP2C9*5
CYP2C9*6
CYP2C9*11
More than 50 single nucleotide polymorphisms (SNPs) have been described in the
coding regions of the CYP2C9 gene (Sim, 2011)
Genetic variants in CYP2C9 could cause great changes in the encoded protein’s
metabolic activity and cause severe adverse drug reactions(Van-Booven et al., 2010)
ADVERSE DRUG REACTIONS(ADRs):
Caused 5% of hospitalization
Experienced by 10% of the hospitalized patients
Over 2million serious ADRs yearly
4th leading cause of death
59% of drugs causing ADRs are metabolized by polymorphic enzymes.
(source: Food and Drug Administration, 2014)

Multiple in vivo studies also show that several mutant CYP2C9 genotypes are associated with
significant reduction of in metabolism and daily dose requirements of selected CYP2C9
substrate. In fact, adverse drug reactions (ADRs) often result from unanticipated changes in
CYP2C9 enzyme activity secondary to genetic polymorphisms. Especially for CYP2C9
substrates such as warfarin and phenytoin, diminished metabolic capacity because of genetic
polymorphisms or drug-drug interactions can lead to toxicity at normal therapeutic doses (Sim,
2011). The gene coding for the CYP2C9 enzyme is highly poly- morphic, including functional
variants of major pharma- cogenetic importance. Changes in metabolic activity caused by
genetic variants in CYP2C9 play a major role in pathogenesis caused by adverse drug
reactions. Patients with low enzyme activity are at risk of adverse drug reaction, especially for
CYP2C9 substrates with a narrow therapeutic window, such as S-warfarin, pheny- toin,
glipizide, and tolbutamide (Pirmohamed and Park, 2003)
The CYP2C9*3 allele has stronger pharmacokinetic effects than CYP2C9*2. For most
substrates, CYP2C9*3 heterozygous individuals had approximately 50% of the wild type total
oral clearance and CYP2C9*3 homozygous individuals had a 5- to 10-fold reduction. With
respect to CYP2C9*2, a significant effect was found for Swarfarin, acenocoumarol,
tolbutamide and celecoxib clearance but not for other drugs (Kirchheiner & Brockmoller,
2005).
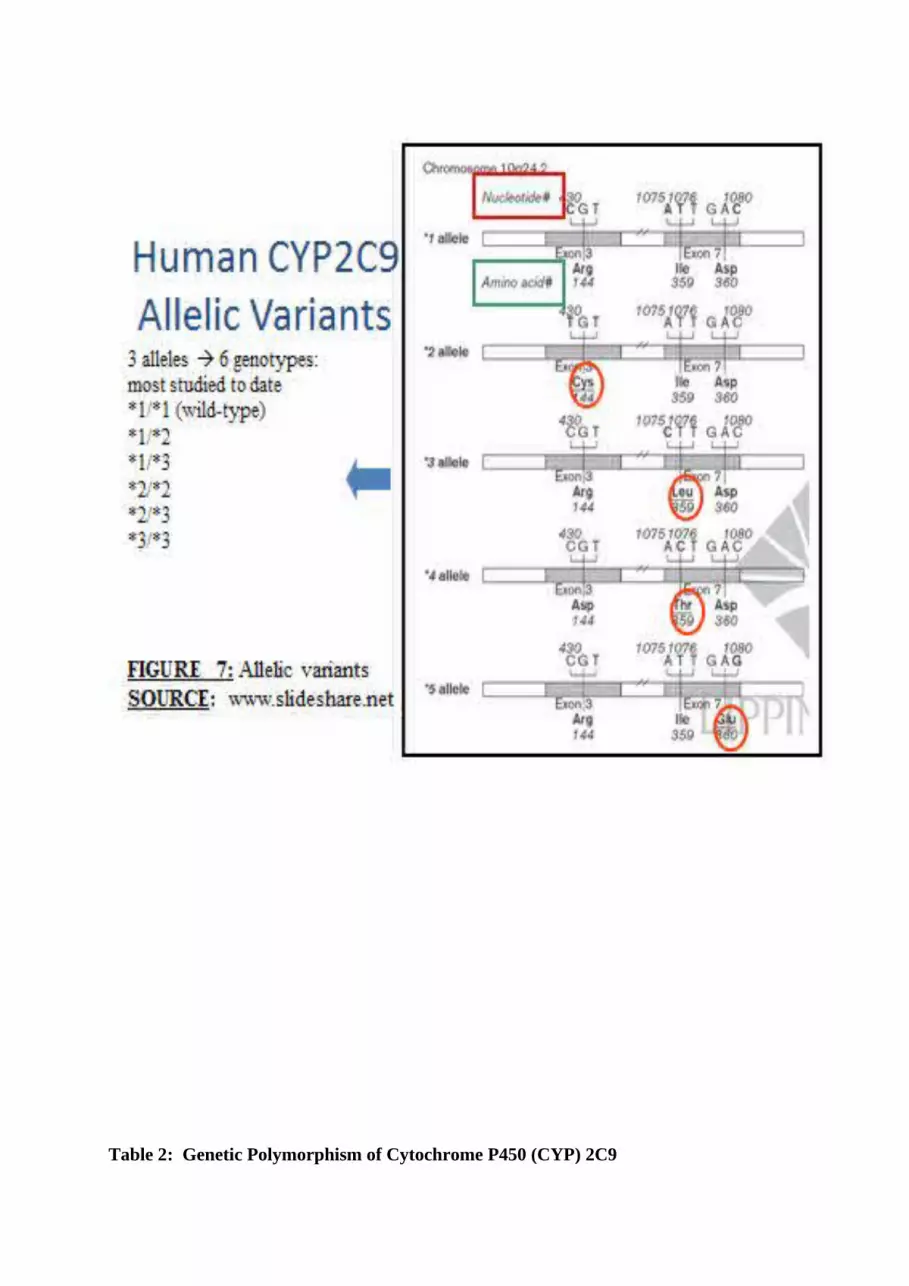
Table 2: Genetic Polymorphism of Cytochrome P450 (CYP) 2C9

Source: www.pharmacologyweekly.com
Allele Location 2C9 Enzyme
Activity
CYP2C9*1 10q24.1 Normal
CYP2C9*2 Exon 3 Reduced
CYP2C9*3 Exon 7 Reduced
CYP2C9*4 Exon 7 Reduced
CYP2C9*5 Exon 7 Reduced
CYP2C9*6 Exon 5 None
CYP2C9*11 Exon 7 Reduced
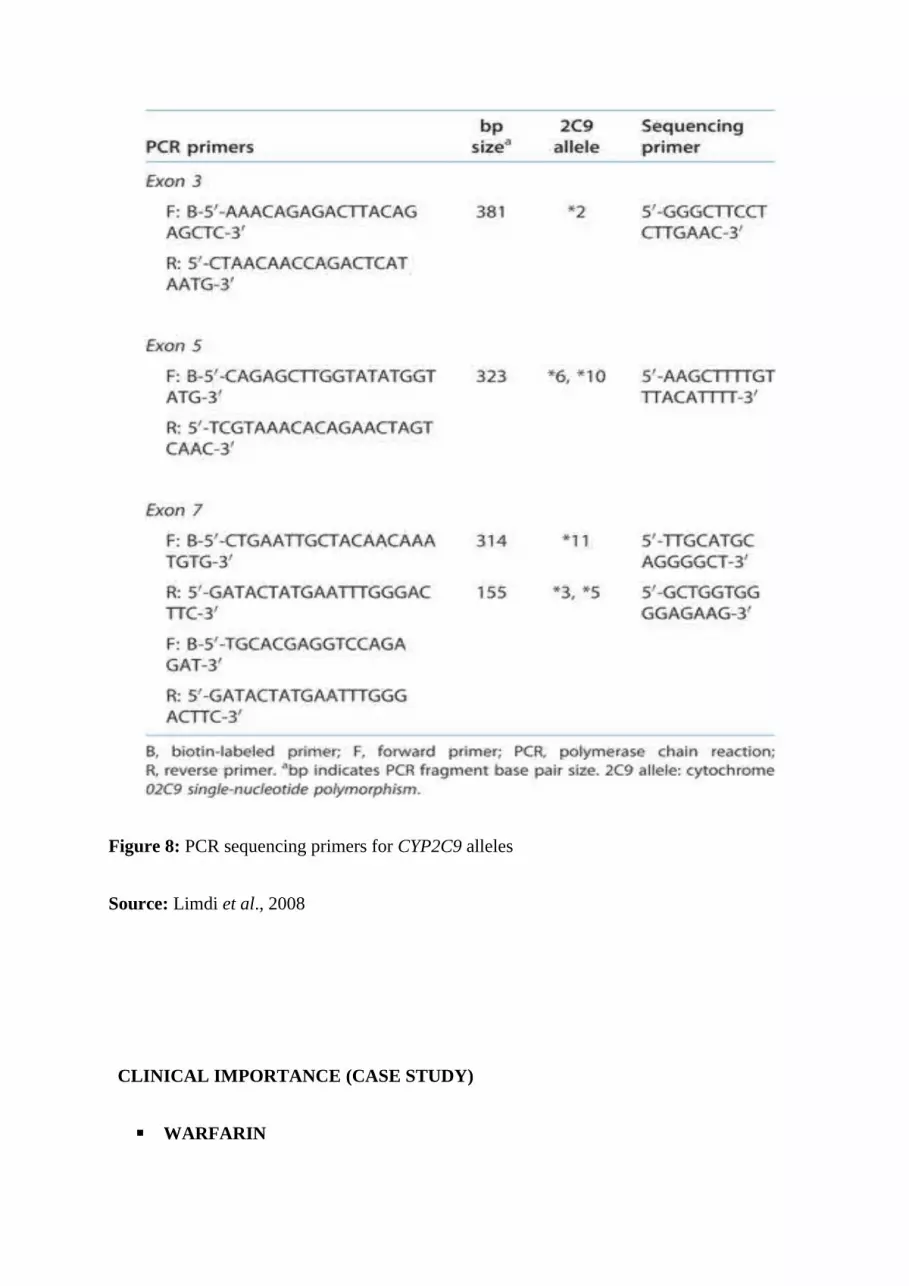
Figure 8: PCR sequencing primers for CYP2C9 alleles
Source: Limdi et al., 2008
CLINICAL IMPORTANCE (CASE STUDY)
WARFARIN

• Widely prescribed anticoagulant drug used to decrease the tendency for thrombosis
and also prevent blood clots(Thrombosis). (Holbrook et al., 2006)
• Clinical consequence of CYP2C9 Poor Metabolizer is evident in decreased clearance of
warfarin. (Buzková et al., 2006)
• The only common adverse effect of warfarin is haemorrhage (bleeding) (Holbrook et
al., 2012)
• Therapeutic range: International Normalized Ratio 2-3 (2.5-3.5 for prosthetic heart
valves)
• INR <2: risk of thromboembolic event, INR >3: risk of bleeding complications
(Mushiroda et al., 2006)
• In December of 2011, the FDA warned that it was investigating Pradaxa due to a greater
amount of injury or death reports than expected. USA Today reported that in 2011, the
FDA received reports of 3,781 Pradaxa adverse effects and 542 deaths among users,
more than all other medications.
• In September of 2012, The Journal for The American Medical Association warned that
the FDA may have rushed approval of Pradaxa, overlooking key side effects like
internal bleeding.
• In its March, 2012 report, the Journal of Neurosurgery detailed a specific case and
concerns by doctors that once Pradaxa causes internal bleeding, there is very little they
can do to stop it. Source: www.drugrisk.com,2014

Figure 10: CYP2C9 Polymorphisms and Warfarin Dose
Source: Gage et al., 2004
*1/*1=EMs(wild type)
*1/*2=IMs
*1/*3=PMs
*1/*5=IMs
*2/*2=IMs
*2/*3=PMs
*3/*3=PMs

Table 3: Adverse Drug Reactions of Important Substrates
Source: Ingelman‐Sundberg , 2001
DRUGS SUBSTRATES ADVERSE EFFECTS IN POOR METABOLIZERS
Oral Anticoagulants Warfarin Increased bleeding,Internal or external hemorrhage, hematuria
Oral Antiglycaemics Tolbutamide Hypoglycaemia
Oral Anticonvulsant Phenytoin Ataxia
NSAID Celecoxib Platelet dysfunction, renal and gastrointestinal toxicity

Figure 11: Examples of dose adjustments based on Phenotypes
Source: Kirchheiner et al., 2005

Table 4: Allele Frequencies of CYP2C9 Polymorphisms(Known variants)
Source: Kirchheiner and Brockmoller, 2005.
Allele and Genotype African
subjects(%)
Asian subjects(%) White subjects(%)
CYP2C9*2 4 0 11
CYP2C9*3 2 3 7
CYP2C9*4 0 ? 0
CYP2C9*5 1.8 ? 0
CYP2C9*6 0.6 ? 0
CYP2C9*11 2.7 ? 0.4
In conclusion,

The CYP2C9 polymorphism is clinically highly significant and also substrate dependent.
Genotyping of CYP2C9 polymorphism has to be taken into account for appropriate dosing in
many different therapies.
References
Aithal, G.P., Day, C.P., Kesteven, P.J. (1999). Association of polymorphisms in the
cytochrome P450 CYP2C9 with warfarin dose requirements and risk of bleeding
complications. Lancet; 353:717-9
Allan, E.R. and Jeffrey, P.J. (2005). Clinical and Toxicological Relevance of CYP2C9: Drug-
Drug Interactions and Pharmacogenetics. Annual Review of Pharmacology and Toxicology.
45:477–94
Aquilante, C.L., Langaee, T.Y. and Lopez, L.M. (2006). Influence of coagulation factor,
vitamin K epoxide reductase complex subunit 1, and cytochrome P450 2C9 gene
polymorphisms on warfarin dose requirements. Clinical Pharmacology and Therapy.79
(4):291–302.
Buzková, H., Pechandová, K., Slanař, O. and Perlík, F. (2006). Genetic Polymorphism
of Cytochrome P450 and Methods for its Determination. Prague Medical Report .4:383–393
Danielson, P.B. (2002). The Cytochrome P450 Superfamily: Biochemistry, Evolution and Drug
Metabolism in Humans. Current Drug Metabolism.3:561-597
Fareed M. and Afzal M. (2013). "Single nucleotide polymorphism in genome-wide association
of human population: A tool for broad spectrum service". Egyptian Journal of Medical Human
Genetics.14: 123–134.
Gage, B.F., Eby, C., Milligan, P.E., Banet, G.A., Duncan, J.R. and McLeod, H.L. (2004). Use
of pharmacogenetics and clinical factors to predict the maintenance dose of warfarin. Thromb
Haemost; 91: 87-94
Genetic polymorphism of cytochrome (CYP) 2C9. www.pharmacologyweekly.com/drug-table-
cytochrome-cyp2c9-genetic-polymorphisms-pharmacogenetics. Retrieved 02/07/2014
Gomes, A.M., Winter, S., Klein, K., Turpeinen, M., Schaeffeler, E., Schwab, M. and Zanger,
U.M. (2009). "Pharmacogenomics of human liver cytochrome P450 oxidoreductase:
multifactorial analysis and impact on microsomal drug oxidation". Pharmacogenomics 10 (4):
579–99
Guengerich, F.P. (2006). Cytochrome P450s and other enzymes in drug metabolism and
toxicity. American Association of Pharmaceutical Scientists Journal; 10; 8(1):101‐11.
Haining, R.L., Hunter, A.P. and Veronese, M.E. (1996). Allelic variants of human cytochrome
P450 2C9:baculovirus mediated expression, purification, structure, characterization, substrate
stereoselectivity and prochiral selectivity of the wild- type and 1359L mutant forms. Archive of
Biochemistry and Biophysics.333:447-58
Hanioka, N., Kimura, S. and Meyer, U.A. (1990). The Human CYP2D locus associated with a
common genetic defect in drug oxidation: a G1938-a base change in intron 3 of a mutant
CYP2D6 allele results in an aberrant 3i splice recognition site. American Journal of Human
Genetics; 47:994-1000
Higashi, M.K., Veenstra, D.L., Kondo, L.M. (2002). Association between CYP2C9 genetic
variants and anticoagulation-related outcomes during warfarin therapy. Journal of American
Medical Association.287(13):1690–1698.
Holbrook, A.M., Pereira, J.A., Labiris, R., McDonald, H., Douketis, J.D., Crowther, M., and
Wells, P.S. (2005). "Systematic overview of warfarin and its drug and food interactions".
Archives of Internal Medicine; 165 (10): 1095–106
Holbrook, A., Schulman, S.,Witt, D.M., Vandvik, P.O.,Fish, J., Kovacs, M.J., Svensson,
P.J.,Veenstra, D.L., Crowther, M. and Guyatt, G.H. (2012). "Evidence-based management of

anticoagulant therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed:
American College of Chest Physicians Evidence-Based Clinical Practice Guideline". Chest
Journal; 141:52–84
Http://www.slideshare.net/lukelightning/ cyp2c9-haplotype-structure-and-association-with-
clinical-outcomes. Retrieved 15/08/2014
Huang, S.M., Goodsaid, F., Rahman, A., Frueh, F. and Lesko, L.J. (2006). Application of
pharmacogenomics in clinical pharmacology. Toxicology Mechanisms and Methods ; 16: 89-
99.
Human CYP allele nomenclature committee home page (www.cypalleles.ki.se). Retrieved
18/07/2014.
Huang, S.M., Goodsaid, F. and Rahman A. (2006). Application of pharmacogenomics in
clinical pharmacology. Toxicology Mechanisms and Methods ; 16:89-99.
http://www.fda.gov/cder/genomics/publications/2006_Huang_Cogenomicis_Clin_pharm.pdf
Ingelman‐Sundberg, M. (2001).Genetic susceptibility to adverse effects of drugs and
environmental toxicants. The role of the CYP family of enzymes. Mutation Research; 482(1‐2):11‐9.
Ingelman-Sundberg M. and Rodriguez-Antona, (2006). Cytochrome P450 pharmacogenetics
and cancer. Oncogene.25; 1679-1691.
Kirchheiner, J., Fuhr, U. and Brockmöller, J. (2005). Pharmacogenetics-based therapeutic
recommendations — ready for clinical practice? Nature Reviews Drug Discovery 4, 639-647.
(http://www.nature.com/nrd/journal/v4/n8/fig_tab/nrd1801_F1.html#figure-title). Retrieved
05/08/2014

Kirchheiner, J. and Brockmoller, J. (2005). Clinical consequences of cytochrome P450 2C9
polymorphisms. Clinical Pharmacology & Therapeutics; 77:1–16.
Mushiroda, T., Ohnishi, Y., Saito, S., Takahashi, A., Kikuchi, Y., Shimomura, H., Wanibuchi,
Y., Suzuki, T., Kamatani, N. and Nakamura, Y. (2006) Association of VKORC1 and CYP2C9
polymorphisms with warfarin dose requirements in Japanese patients. Journal of Human
Genetics; 51(3):249-53.
Limdi, N.A., McGwin, G., Goldstein, J.A., Beasley, T.M., Arnett, D.K., Adler, B.K., Baird,
M.E. and Acton, R.T. (2008). Influence of CYP2C9 and VKORC1 1173C/T Genotype on the
Risk of Hemorrhagic Complications in African-American and European-American Patients on
Warfarin. Clinical Pharmacology & Therapeutics; 83(2):312-21
Rendic, S. (2002). Summary of information on human CYP enzymes: human P450 metabolism
data. Drug Metabolism Revised; 34: 83–448.
Pirmohamed, M. and Park, B.K. 2003. Cytochrome P450 enzyme polymorphisms and adverse
drug reactions. Toxicology.192:23–32
Selected drug substrates of cyp2c9 involve in drug metabolism
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1873650/figure/fig01/. Retrieved 01/09/2014
Sim, S.C. (2011). "CYP2C9 allele nomenclature". Cytochrome P450 (CYP) Allele
Nomenclature Committee. (www.cypalleles.ki.se). Retrieved 18/07/2014.
Sohayla, M., Ayman, Z. and Ayman, E. (2007). Genetic Polymorphism of Cytochrome P450 -
2d6*4 In Cannabis Smokers. The Internet Journal of Toxicology; 5:1-10
Tang, C., Shou, M. and Rushmore, T. (2001). In-vitro metabolism of celecoxib, a
cyclooxygenase-2-inhibitor,by allelic variant forms of human liver microsomal cytochrome
P450 2C9:correlation with CYP2C9 genotype and invivo pharmacokinetics.
Pharmacogenetics.11:223-35
Thum, T. and Borlak, J. (2000). Gene expression in distinct regions of the heart. Lancet.355:
979–83.
Van Booven, D., Marsh, S., McLeod, H., Carrillo, M.W., Sangkuhl, K., Klein, T.E. and
Altman, R.B. (2010). Cytochrome P450 2C9-CYP2C9. Pharmacogenetics and Genomics.20:
277–281.
U.S Food and Drug Administration. Pradaxa side effects and complications.
http://www.drugrisk.com/pradaxa/side-effects. Retrieved 01/09/2014
Wang, J.F., Wei, D.Q., Li, L., Zheng, S.Y., Li, Y.X. and Chou K.C. (2007). 3D structure
modeling of cytochrome P450 2C19 and its implication for personalized drug design.
Biochemistry and Biophysics Research Community; 355 513–519
Wang, B.; Wang, J.; Huang, S.Q.; Su, H.H.; Zhou, S.F. (2009).Genetic polymorphism of the
human cytochrome P450 2C9 gene and its clinical significance. Current Drug Metabolism; 10:
781–834.
![Metabolic activation of benzo[a]pyrene in vitro by hepatic cytochrome P450 contrasts with detoxification in vivo: experiments with hepatic cytochrome P450 reductase null mice](https://img.dokumen.tips/doc/110x75/6357cde43cd558f04e05031c/metabolic-activation-of-benzoapyrene-in-vitro-by-hepatic-cytochrome-p450-contrasts.jpg)





























