Embed Size (px)
Citation preview

Devon Partnership NHS Trust Board of Directors papers are available at: www.dpt.nhs.uk/BoardPapers
Page 1 of 2
MEETING OF THE BOARD OF DIRECTORS – To be held in public
13:00 on Monday 12 March 2018
Easby Conference Room at Easby House, Langdon Hospital, Exeter Road, Dawlish EX7 0NR
A G E N D A
Service User Story
13:00 1.1 Sarah Brady, Lead Occupational Therapist and Katy Welsh, Lead Nurse – Primary Care Liaison, will be accompanying a service-user who is currently using the Trust’s Learning Disabilities services and who is passionate about speaking up for people with Learning Disabilities. All three will present work they have done to ask current service users their views and experiences of the Trust’s services and what is being done in response. Information will be in the form of a presentation and videos co-produced with service users, their family and staff.
Time Ref Opening Administration Action
13:30 2.1 Welcome and Apologies for Absence Note
2.2 Declarations of Interest and Register of Interests Inform
2.3 Minutes of the Meeting held on the 8 January 2018 Approve
2.4 Matters Arising and the Action Log Review
2.5 Chief Executive’s Report Melanie Walker, Chief Executive
Inform
Quality and Safety These papers provide assurance on the quality and safety of the Trust’s services
13:45 3.1 Quality and Safety Committee Report - Verbal Liz Childs, Non-Executive Director
Assure
Integrated Performance These papers support the Board’s oversight of clinical and organisational performance across the Trust
13:55 4.1 Integrated Performance and Clinical Operations Report Dr David Somerfield, Chief Operating Officer and Sarah Brampton, Director of Finance
Assure
Workforce and Organisational Development These papers provide assurance on the work undertaken across the Trust to ensure that high quality care is
delivered through an effective, skilled, motivated and well-led workforce
14:10 5.1 Workforce and Organisational Development Assurance Committee Report - Verbal Gerry Marshall, Non-Executive Director
Assure
5.2 Guardian of Safe Working Report Dr Helen Smith, Medical Director
Assure
5.3 Safer Staffing – Workforce Report Paul Keedwell, Director of Nursing and Practice
Assure
1. A
gend
a
Page 1 of 96

Devon Partnership NHS Trust Board of Directors papers are available at: www.dpt.nhs.uk/BoardPapers
Page 2 of 2
5.4 Gender Pay Gap Report Paul Keedwell, Director of Nursing and Practice
Approve
Finance and Investment These papers provide assurance on the effective investment, prioritisation and management of financial
resources
14:30 6.1 Finance and Investment Committee Report - Verbal Chair of Finance and Investment Committee
Assure
6.2 General Data Protection Regulations (GDPR) Briefing Sarah Brampton, Director of Finance
Assure
Governance
14:40 7.1 Audit Committee Report - Verbal Mary Moore, Non-Executive Director
Assure
7.2 Corporate Assurance Framework Fiona Barr, Corporate Governance Advisor
Receive
Closing Administration
14:50 8.1 Summary of Actions -
8.2 New Risks or Issues -
8.3 Items for the Next Meeting
• National NHS Survey
-
8.4 Any Other Business -
8.5 Reflection on the Meeting -
15:00 Close
Resolution to move to closed session In accordance with Section 1 (2) Public Bodies (Admissions to Meeting) Act 1960, the Board is invited to approve the following resolution: “That representatives of the press and other members of the public, be excluded from the remainder of this meeting having regard to the confidential nature of the business to be transacted, publicity on which would be prejudicial to the public interest”.
Date of Next Meeting: 14 May 2018
1. A
gend
a
Page 2 of 96

Report Summary
Report provided: Agenda
Item: 2.2
To note: X For assurance: Report
to: Board of Directors
For approval:
For information:
Meeting date:
12 March 2018
REGISTER OF INTERESTS AND CODE OF CONDUCT
Accountable Director(s):
Julie Dent, Chair
Presented & Approved by:
Fiona Barr, Corporate Governance Advisor
Report author(s):
Fiona Barr, Corporate Governance Advisor
Alignment to the Trust’s strategic aims:
Our aims:
To deliver consistently high quality care and treatment
To ensure our services are driven by the voices of people who use them
To build a reputation as a recognised centre of excellence and expertise
To attract and retain talented people and to create a great place to work, with a shared sense of pride and ambition
x
To challenge discrimination and stigma, and to champion recovery, inclusion and wellbeing
To be an efficient, thriving and successful organisation with a sustainable future
Purpose of report:
To ensure that Directors are independent in character and judgement and whether there are relationships or circumstances which are likely to affect, or could appear to affect, the Director’s judgement.
Summary of the key issues:
The register has been fully checked and revised to ensure compliance with the Fit and Proper Persons Requirements.
Recommendations:
Members of the Board are asked to:
• clarify information is correct and up to date
• approve the Register of Interests
• declare any new interests as they arise
Report previously presented to:
Committee/Group: Date: Report title: Outcome/action:
N/A
Summary of compliance implications:
Disclosure is made within the annual accounts and annual report.
Does this report provide assurance in respect of a new / existing risk/s?
Type of risk/s N/A Corporate Assurance Risk Register
Level of Assurance and trend: 1 to 10
Significant Limited None
2.2
Reg
iste
r of
Inte
rest
s
Page 3 of 96

Board of Directors meeting, 12 March 2018 Agenda Item 2.2
BOARD OF DIRECTORS - REGISTER OF INTERESTS – March 2018
Designation
Name Declaration Type of Interest Mitigations
Chair Julie Dent • Director of AM and JE Dent Partnership Non-Financial Personal Declaration
• Director – Higherway Limited Non-Financial Personal Declaration
• Partner – Higherway Farm Limited Non-Financial Personal Declaration
• Chair of Devon Libraries Unlimited Non-Financial Personal County Council is aware.
• Faculty for Eden Consultancy Non-Financial Professional Separate contract
• Parish Councillor, Templeton Non-Financial Personal Declaration
Chief Executive Melanie Walker • Chair – Modbury Scout Group Non-Financial Personal Declaration
• Member of NHS Confederation Mental Health Network Board
Non-Financial Personal Declaration
• Chair of Board of Trustees for Space (Devon Youth services)
Non-Financial Personal Declaration
Non-Executive Director
Liz Childs • Executive Coach Financial Not to coach in DPT if expenses to be incurred
• Involvement with Compassion in Dying and its member organisation, Dignity in Dying
Non-Financial Personal Keep work separate
• Consultant – independent professional services Financial Discuss with the Chair any potential conflicts in advance of agreeing a brief
Non-Executive Director
David Gebbie • Owner of OTB Eveling LLP (law firm) Financial Declaration
Non-Executive Director
Gerry Marshall • Chair of Trustees: Circles UK (Circles of Support and Accountability national body - volunteers working with released sex offenders)
Non-Financial Personal Declaration
• Trustee: Howard League for Penal Reform Non-Financial Personal Declaration
• Criminal Justice adviser: Tutu Foundation UK Non-Financial Personal Declaration
• Assessor for Restorative Services Quality Mark (Restorative Justice Council)
Financial Declaration
• Leadership consultancy through "Leadership Insight" Financial Declaration
• Director – Gerry Marshall Associates Financial Declaration
2.2
Reg
iste
r of
Inte
rest
s
Page 4 of 96

Board of Directors meeting, 12 March 2018 Agenda Item 2.2
Designation
Name Declaration Type of Interest Mitigations
Non-Executive Director
(Hilda) Mary Moore
• Trustee – SeeAbility Non-Financial Personal Declaration
• Director – Mary Moore Limited Consultancy Financial Declaration
Corporate Governance Advisor
Fiona Barr • Director – ZERB1 Ltd Financial No work undertaken for DPT or within Devon STP
Director of Finance
Sarah Brampton • Member of Healthcare Financial Management Association (HFMA)
Non-Financial Professional Declaration
• Member of HFMA for the South West Non-Financial Professional Declaration
• Governor for Exeter College Non-Financial Professional Declaration
• Chair of Exeter College Audit Committee Non-Financial Professional Declaration
• Chair for the NHS Providers Finance Network Non-Financial Professional Declaration
• Secondment to Cornwall as System Finance Director Non-Financial Professional Declaration
Executive Director of Nursing and Practice
Paul Keedwell • Directorship of Shant Manas, an Indian mental health charity
Non-Financial Professional Declaration
• Honorary Associate Professor of University of Exeter Medical School
Non-Financial Professional Declaration
Chief Operating Officer
Dr David Somerfield
• Trustee - The Lupton Trust, Brixham Non-Financial Personal Declaration
• Fellow and Associate Registrar with the Royal College of Psychiatry
Non-Financial Personal Declaration
• Spouse is Sister at South Devon Healthcare NHS Foundation Trust
Non-Financial Personal Declaration
Medical Director Dr Helen Smith • Specialist Advisor for the Academic Health Science Network
Financial Personal Declaration
• Specialist advisor for the Care Quality Commission Non-Financial Professional Declaration
• Clinical Lead for South of England Quality Improvement Patient Safety Collaborative
Non-Financial Professional Declaration
• Spouse is responsible office for South of England Quality Improvement Patient Safety Collaborative
Non-Financial Personal Declaration
2.2
Reg
iste
r of
Inte
rest
s
Page 5 of 96
Board of Directors meeting, 12 March 2018 Agenda Item 2.2
Designation
Name Declaration Type of Interest Mitigations
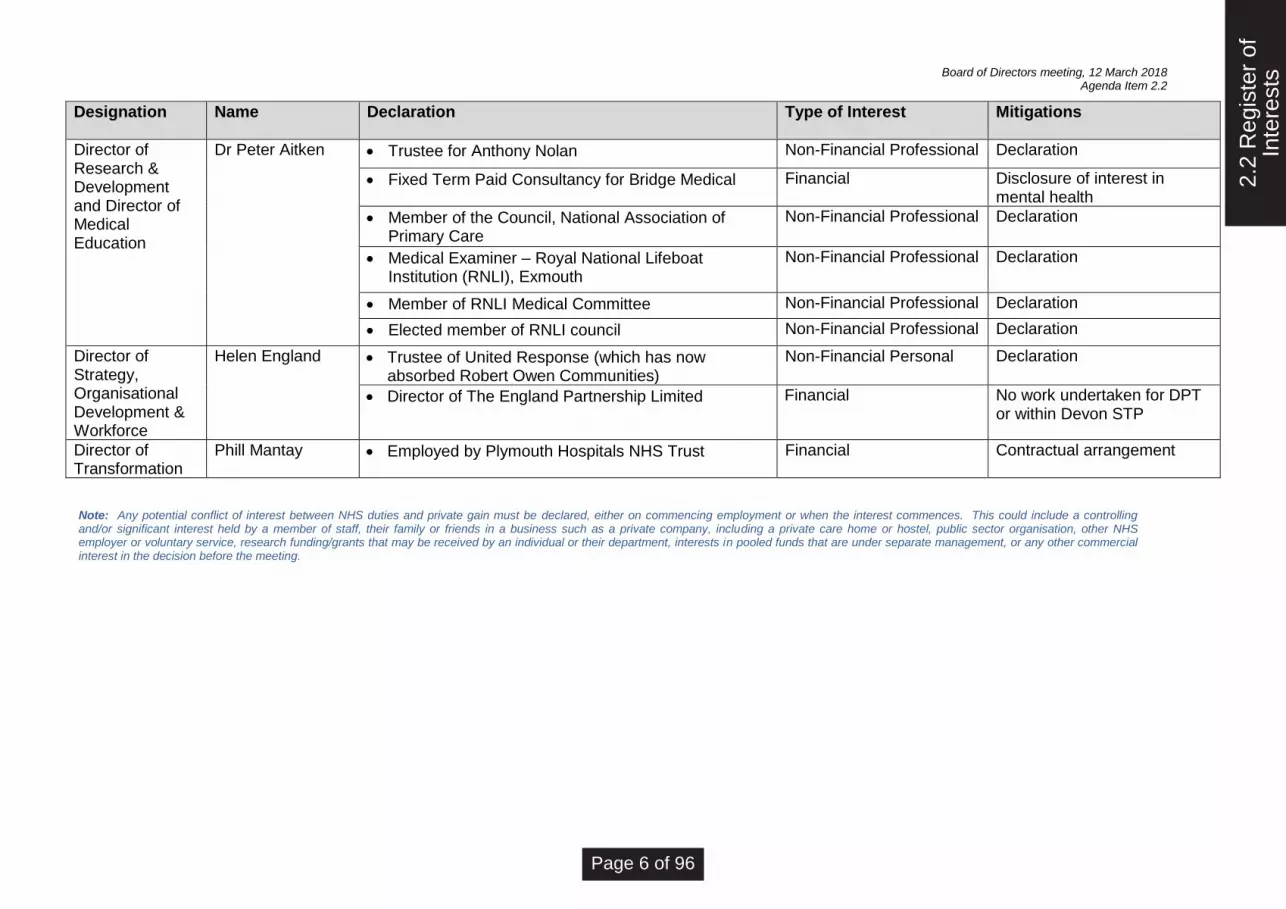
Director of Research & Development and Director of Medical Education
Dr Peter Aitken • Trustee for Anthony Nolan Non-Financial Professional Declaration
• Fixed Term Paid Consultancy for Bridge Medical Financial Disclosure of interest in mental health
• Member of the Council, National Association of Primary Care
Non-Financial Professional Declaration
• Medical Examiner – Royal National Lifeboat Institution (RNLI), Exmouth
Non-Financial Professional Declaration
• Member of RNLI Medical Committee Non-Financial Professional Declaration
• Elected member of RNLI council Non-Financial Professional Declaration
Director of Strategy, Organisational Development & Workforce
Helen England • Trustee of United Response (which has now absorbed Robert Owen Communities)
Non-Financial Personal Declaration
• Director of The England Partnership Limited Financial No work undertaken for DPT or within Devon STP
Director of Transformation
Phill Mantay • Employed by Plymouth Hospitals NHS Trust Financial Contractual arrangement
Note: Any potential conflict of interest between NHS duties and private gain must be declared, either on commencing employment or when the interest commences. This could include a controlling and/or significant interest held by a member of staff, their family or friends in a business such as a private company, including a private care home or hostel, public sector organisation, other NHS employer or voluntary service, research funding/grants that may be received by an individual or their department, interests in pooled funds that are under separate management, or any other commercial interest in the decision before the meeting.
2.2
Reg
iste
r of
Inte
rest
s
Page 6 of 96

Board of Directors Meeting, 12 March 2018 Agenda Item 2.3
1
Meeting of the Board of Directors – Part One
Minutes 8 January 2018
Estuary Room, Darts Farm, Topsham, Exeter
Present: Julie Dent, CBE Chair Liz Childs Non-Executive Director / Vice-Chair Peter Marriner Non-Executive Director Mary Moore Non-Executive Director David Gebbie Non-Executive Director Melanie Walker Chief Executive Dr Helen Smith Medical Director Sarah Brampton Deputy Chief Executive Dr David Somerfield Chief Operating Officer In attendance: Dr Peter Aitken Director of Research and Development Fiona Barr Corporate Governance Advisor Chris Burford Deputy Director of Nursing and Practice Helen England Director of Strategy, Organisational Development and Workforce Secretariat: Natalie Daly Interim Governance Business Assistant 001/18 (Item 1)
Welcome and Apologies for absence The Chair welcomed everyone to the meeting, noting the following apologies:
Professor Clive Ballard Associate Non-Executive Director Paul Keedwell Director of Nursing and Practice Gerry Marshall Non-Executive Director
It was highlighted that Chris Burford, Deputy Director of Nursing and Practice, was in attendance deputising for Paul Keedwell, Director of Nursing and Practice.
The Chair highlighted Professor Ballard, Associate Non-Executive Director, remained committed to supporting the Trust but advised that his current commitments prevented him from attending meetings on Mondays. The Chair, therefore, suggested an alternative day of the week to be identified for future Board meetings to accommodate regular attendance by Professor Ballard. This was agreed.
Action 001/18
Review an alternative day of the week for future Board meetings. Lead: Fiona Barr, Corporate Governance Advisor.
The Chair advised the Board that Helen England, Director of Strategy, Organisational Development and Workforce, had been appointed as Chief Executive Officer of a national charity working in the field of disability and would leave the Trust at the end of March 2018. The Chair led the Board in congratulating Helen on her new role and thanked her for her commitment and contribution to the Trust.
The Chair and the Board welcomed Fiona Barr, temporary Corporate Governance
Advisor, who had joined the Trust to undertake a review of governance processes.
2.3
Min
utes
Page 7 of 96

Board of Directors Meeting, 12 March 2018 Agenda Item 2.3
2
002/18 (Item 2)
Register of Interests and Code of Conduct The Board members received and reviewed the Register of Interests. There were no changes declared.
Resolved Members of the Board resolved to confirm that the information was correct, up to date and approved the Register of Interest and Code of Conduct. It also confirmed the Board’s continued adherence to the NHS Constitution and the NHS Code of Conduct, including the Nolan Principles – The Seven Principles For Public Life.
003/18 (Item 3)
Listening to Experience Chris Burford, Deputy Director of Nursing and Practice, welcomed Tracy Lang to the Board. Tracy Lang is a carer for her 18 year old son who was admitted to Haytor Ward in February 2016 and who has been a regular user of Trust services since then. Tracy shared with the Board her personal experiences of using the Trust’s services from a carer’s perspective. She outlined the frustrations she and her family had encountered, for example, a lack of a consistent psychiatrist, cancelation of appointments, difficulty parking, delays in funding decisions and the need to use services out of area. These frustrations affected her son’s health and caused anxiety to his parents as the principal carers.
Tracy found it difficult to get a response from the Trust regarding her son’s care and felt on many occasions that the Trust was not listening. Tracy wrote a formal complaint to the Trust which was acknowledged and, as a result, Tracy was encouraged to become actively involved with improving services through sharing her experiences as a carer.
As Tracy became more actively involved, her knowledge of the Trust, its staff and the pressures faced began to increase. She recognised that many staff were passionate as well as responsive to feedback and keen to involve service users and their carers’ in decisions about and arrangements for their care. She emphasised the importance of good communication and listening skills when involving service users and carers.
Tracy presented a graphic and powerful diagram which set out the issues of her son’s care ‘at a glance’. Helen Smith, Medical Director, assured Tracy that the diagram had been used within consultant training and development to enable wider learning across the Trust to improve care for other service users.
The Board thanked Tracy for sharing her experience as a carer. Continued active involvement of volunteers to co-design solutions was positively recognised as having a significant potential improving the Trust’s services.
004/18 (Item 4)
Minutes of the Board of Directors meeting held 13 November 2017 The Board members approved the minutes of the previous meeting as a fair and accurate record and authorised the Chair to sign a copy subject to the following amendment of minute 118/17: Register of Interests and Code of Conduct: ‘recoding’ altered to ‘recording’ so that the first paragraph reads: “…Dr Peter Aitken’s entry, recording his fixed…”. The minutes were to be signed by the Chair and not the Vice-Chair as stated in the report.
005/18 (Item 4a)
Matters Arising (Action Log Review) The Board considered the action log and the following updates were highlighted: Action 070/17: Clinical Operations Report, the annual leave policy now underpins the protocol for the Health Roster which will help staff better manage shifts and planned absence. Action 148/17: Quality and Compliance Performance Report, Sarah Brampton, Director
2.3
Min
utes
Page 8 of 96

Board of Directors Meeting, 12 March 2018 Agenda Item 2.3
3
of Finance, reported that progress is being made to renew the format and the latest draft was included in the papers for review. Action 197/19: Dr David Somerfield advised that the work to support Gender Dysphoria was underway, including addressing vacancies and sickness levels. A fuller update would be provided to the next meeting.
006/18 (Item 5)
Chief Executive’s Report Melanie Walker, Chief Executive Officer, presented the report to the Board. Melanie was proud of all the work showcased at the Celebrating Achievements awards in December 2017 which recognised the many achievements of staff across the Trust. There was particular mention of the work by Jay Patel and Lynne Hollis, Care Coordinators, who received the Board award. There were also a number of Lifetime Achievement awards.
The Trust was continuing to encourage vaccinations against flu. The Board welcomed the news that the number of staff vaccinated had increased to 62% since the report was written.
The annual staff survey had now closed but the response rate was the highest ever and Melanie Walker, Chief Executive Officer, was pleased to announce she understood it was the second highest return nationally for a mental health trust.
A letter of thanks had been received from The Open University with positive feedback congratulating the Trust on its work to develop a rigorous process for the recruitment and selection of staff put forward for the programmes of study. The Board recognised the importance of this work in strengthening of the Trust’s partnership with the university.
Care Quality Commission (CQC) service inspections were expected to re-commence in January with the review against the Well Led Framework to commence in the week of 05.02.18 and feedback from inspections to date had been positive.
The Board was pleased to note Dr David Somerfield as the designated Chief Clinical Information Officer recognising how David’s experience and expertise would significantly improve links between the clinical and IT services and how they work together.
The Devon Sustainability and Transformation Partnership (STP) did not appoint to the
role of chief executive officer (CEO) so instead, the STP is seeking an independent chair who will appoint the CEO.
The Trust in partnership with EDP Drug and Alcohol Services (EDP) had been
successful in their bid to deliver drug and alcohol services in communities across Devon and the Board welcomed this announcement.
The Board congratulated Angela Pedder, former Chief Executive at the Royal Devon
and Exeter NHS Foundation Trust (RD&E), on becoming a dame in the New Year’s Honours.
Helen Smith, Medical Director, was pleased to announce that the Trust had won three
awards at the 2017 Training Journal Awards for the Trust’s patient safety programme. The awards were: winners of the best public sector programme, winners of the best operational programme and bronze award in the best training partnership. The Board congratulated the team and recognised the programme underpins the majority of quality and safety work across the Trust.
2.3
Min
utes
Page 9 of 96

Board of Directors Meeting, 12 March 2018 Agenda Item 2.3
4
Mary Moore, Non-Executive Director, requested more information on the EDP partnership but it was highlighted that there would be an update in Part Two of the Board meeting today.
Dr David Somerfield, Chief Operating Officer, discussed the significant impact of delays on the Trust regarding the authorisation of leave from the Ministry of Justice both from a workforce and financial perspective. Delays can take up to 758 days which can also have a serious impact on a service user’s recovery. This had been recognised as a national issue and NHS Improvement and the Royal College of Psychiatry are actively exploring solutions.
The Chair informed the Board that, following the two recent suicides of staff members at SWASFT, the Trust had offered support to affected staff for which SWASFT had formally recorded its thanks for the positive impact it had.
Resolved Members of the Board received and noted the contents of the report.
007/18 (Item 6)
Strategy Development and Implementation Helen England, Director of Strategy, Organisational Development and Workforce, outlined the report, providing an update on the implementation of the Trust’s five year strategy (2016/21). The Board was assured that all corporate plans are aligned to the corporate strategy and objectives. Cost Improvement Plans (CIPs) were being reviewed and the implementation of both annual action plans and progress reports would be reported through the sub-committees.
Using the agreed quality improvement methodology, the plan aimed to embed a culture of continuous improvement to support the Trust in its mission to become a centre of excellence and expertise in mental health and learning disability. The Organisational Development Programme would help to create leaders required for this change.
In addition, a wider review of organisational design and structure would ensure that the organisation’s leadership, infrastructure and systems supported effective delivery of commissioning and provider functions through which the Trust’s governance structure would also be considered.
In closing, the Director of Strategy, Organisational Development and Workforce, informed the Board that the next steps included an annual review of the strategy by the Board and on-going review of progress via the Committees. This approach was welcomed and endorsed by the Board and the Chief Executive suggested that the detailed measures of progress set out in Appendix 1 be added to the Committees’ work plans to ensure visibility of delivery. This was agreed.
Action 007/18
Add the measures of progress set out in Appendix 1 of Delivering Quality, Integration and Recovery – Our Strategy for 2016/21 to the relevant Committee work plans. Lead: Fiona Barr, Corporate Governance Advisor
The Chair thanked Helen England for the report which the Board received and thanked her for her contribution as Director of Strategy, Organisational Development and Workforce.
008/18 (Item 7)
Quality and Safety Committee Report Liz Childs, Non-Executive Director, introduced the Quality and Safety Committee report to the Board. The Committee previously met on 22.12.17 and there were two areas of concern highlighted: ligatures and the prison governance system.
To assure the Board on the action taken to address and remove potential ligature
2.3
Min
utes
Page 10 of 96

Board of Directors Meeting, 12 March 2018 Agenda Item 2.3
5
points, the Board noted that all wards had completed risk assessments and were providing regular reports to the Committee; however this was an area which would continue to be closely monitored by the Quality and Safety Committee.
The Committee had received a report on aspects of the prison service since the Trust had taken responsibility of the prison mental health in April 2017. The Board noted that meetings had been held with the three Devon prisons to resolve the governance issues and that incidents were being recorded on the Trust’s RMS (risk management) system.
A discussion took place on the results from the Royal College of Psychiatrists on the Trust’s Root Cause Analysis investigations. Despite the poor results, the Trust was performing better than other trusts and feedback from the commissioner praised the quality and honesty of the Trust’s reports. The Board noted that the issue was around the capacity to complete the reports rather than a lack of quality or understanding.
Sarah Brampton, Deputy Chief Executive, highlighted that the clinical hubs scheduling has led to improved access for 350 people per a week which was having a significant impact.
The Board discussed the new court video conferencing facilities at Langdon and the positive impact it has made on the experience of both staff and patients.
The Chair thanked the safeguarding team and Penny Rogers, Managing Partner for Safeguarding, for the work on the safeguarding training which had greatly improved.
Resolved The Board received the report.
009/18 (Item 8)
Care Quality Commission Update Chris Burford, Deputy Director of Nursing and Practice, presented the CQC report to the Board updating the Trust’s progress on all the improvement actions being undertaken in response to findings of the CQC’s inspection report from 2016. It was agreed that the Quality and Safety Committee would oversee the delivery of outstanding actions.
He repeated points made earlier in the meeting that there would be further CQC inspections in the run up to the review against the Well Led Framework (which would commence during 05.02.18) though focus groups with staff were scheduled for this week (week commencing 08.01.18). The feedback from the unannounced visits across three services had been positive though preparations continue for the forthcoming inspections.
Resolved The Chair thanked the team for the report and the work they have undertaken on the preparation for the CQC visit and the Board received the report
010/18 (Item 9)
Learning from Deaths and Mortality Review Report In line with national guidance on learning from patient deaths, Helen Smith, Medical Director, presented the report to the Board and thanked the author, Shaun Alexander, Head of Experience, Safety and Risk, for its production though she explained that the Trust had robust systems in place to track and learn from patient deaths for longer than the national requirements. The report was based on figures from April to September 2017 and did not reflect the new Trust’s R21 Learning from Deaths and Mortality Reviews policy. At the next meeting, the Board would receive the report in a format aligned with the new policy and national framework.
She explained the emphasis of working with Coroners to understand the reasons
behind the deaths of detained patients and advised that Dr Adrian James, Consultant Psychiatrist from the Royal College of Psychiatry, was leading work to improve systems and tools to identify avoidable deaths. Training was planned to embed this with staff
2.3
Min
utes
Page 11 of 96

Board of Directors Meeting, 12 March 2018 Agenda Item 2.3
6
and it had generated a high level of interest from the junior doctors.
The Board discussed the Trust’s mortality rates set out in section 3.2 to understand if and the numbers of unexpected deaths were in line with other mental health trusts. Helen Smith explained that there was no national benchmarking data and it would be difficult to compare results with other providers. However she assured the Board of the robust processes followed to understand the reasons behind unexpected deaths and the work being undertaken by the team to identify avoidable factors.
A discussion took place on the recent five suicides in Exeter prison, two of which were receiving treatment from the Trust. The Medical Director agreed to confirm if those figures were included in those in section 3.2 and to confirm how those deaths are investigated and reported if not by the Trust.
Action 010/18a
Advise the Board if the five deaths in custody (Exeter Prison) were included in the Learning from Deaths report to the January Board meeting. Lead: Dr Helen Smith, Medical Director.
Action 010/18b
Confirm where deaths are reported if the Trust is not the lead investigator. Lead: Dr Helen Smith, Medical Director
Melanie Walker, Chief Executive, requested clarification on the incident in section 3.13 which stated that a patient was transferred back to the Emergency Department due to poor health and then subsequently passed away. David Somerfield, Chief Operations Officer, agreed to explore this and report back to the CEO.
Action 010/18c
Brief the CEO on the patient death in the Emergency Department described in section 3.13 of the report on Patient Deaths to the January 2018 Board. Lead: Dr David Somerfield, Chief Operations Officer.
The Board requested that future reports on learning from patient deaths focus on the learning that has arisen and what has changed as a result.
Action 010/18d
Include details of changes which have been made and learning that has arisen from a review of patient deaths in future Learning from Deaths and Mortality Review reports to the Board. Lead: Dr Helen Smith, Medical Director.
Melanie Walker, Chief Executive, requested a report on suicide prevention outlining the challenges in Devon along with the actions being taken by the Trust, future aspirations and partnership opportunities.
Action 010/18e
Report to the Board on the challenges of suicide prevention and include the actions being taken by the Trust, future aspirations and partnership opportunities. Lead: Dr Helen Smith, Medical Director.
Resolved The Chair thanked Helen Smith, Medical Director, and the team for the report. The Board accepted the recommendations though requested that future reports provided greater positive assurance about learning from patient deaths
011/18 (Item 10)
Integrated Performance and Clinical Operations Report Dr David Somerfield, Chief Operations Officer, presented the report to the Board, highlighting the new format though he explained that that further work was required to develop and refine the narrative to support data which would be done through scrutiny at the Directorate Governance Boards. The Chief Executive commended the work done by both the Chief Operations Officer and the Director of Finance on the new
2.3
Min
utes
Page 12 of 96

Board of Directors Meeting, 12 March 2018 Agenda Item 2.3
7
performance dashboard.
Dr David Somerfield, Chief Operations Officer, was pleased to inform the Board that there have been constructive conversations with Lived Well about opening new beds. He also advised that incidences of delayed discharge were subject to internal review and the operational teams currently had a strong focus on reducing waiting times for services.
The Board was informed that Dr Andy Whitaker, Clinical Director (Adult Service), was
stepping down as Clinical Director and returning to full clinical practice; the Board extended its thanks to Andy for all his hard work whilst Clinical Director.
A discussion took place on the underperformance against the national CQUIN for emergency departments for which the Trust may be issued with financial penalties. Dr David Somerfield, Chief Operations Officer, had raised this with the commissioners and was awaiting a response though the Board noted that the achievement of this CQUIN was not fully within the control of the organisation.
The Board discussed the narrative of the reports in the dashboard and requested that future reports provide an historical position to provide greater context and enable trends to be identified.
Action 011/18a
Provide an historical view to the data presented on the performance dashboard to provide greater context and allow better analysis. Lead: Dr David Somerfield, Chief Operations Officer.
The Board noted a downward movement in the results of the Staff Family and Friends Test results over the last three surveys but against a backdrop of considerable improvement over the last two year. Further analysis to understand the variation in the data will therefore be important. The Board noted concerns about the Adult Directorate which had high sickness rates as well as a key gap in leadership with the departure of Andy Whitaker as Clinical Director. Helen England, Director of Strategy, Organisational Development and Workforce, confirmed that sickness levels had increased but that this was in line with last year’s profile over the winter period and was lower than in previous years. The Workforce and Organisational Development Assurance Committee agreed to scrutinise this more fully at its next meeting and report back its findings to the Board.
Action 011/18b
Review in detail sickness absence at the next meeting of the Workforce and Organisational Development Assurance Committee and report back findings to the Board. Lead: Helen England, Director of Strategy, Organisational Development and Workforce
Dr Peter Aitken, Director of Research and Development, outlined the process to source applicants for the Adults Clinical Director post. The Board recognised that other trusts in the South West were finding it difficult to recruit to a number of clinical posts, especially where there was a national shortage.
In response to a recent review of data on prone restraint, the Chief Executive asked for details of prone restraint to be added to the Performance Report as a metric which was regularly reviewed. This was agreed though a separate report would be produced on prone restraint and considered by the Executive before the next meeting of the Board.
Action 011/18c
Include details of instances of prone restraint to the Performance Report. Lead: Dr David Somerfield, Chief Operating Officer.
Resolved The new format of the report was well received by the Board and the Chair thanked all
2.3
Min
utes
Page 13 of 96

Board of Directors Meeting, 12 March 2018 Agenda Item 2.3
8
those involved in its production. The Board received the report.
012/18 (Item 11)
Safer Staffing – Workforce Report Chris Burford, Deputy Director of Nursing and Practice, presented the Safer Staffing report to the Board.
Vacancies in registered nurses in the Additional Support Unit were being managed by flexing the skill mix to make best use of the available resource. It was highlighted that the new Band 4 Trainee Assistant Practitioner programme had been launched which would alleviate some current staffing pressures.
There was a general discussion about the wards’ use of temporary or agency staff and the Board observed that the picture was quite mixed across the Trust. For example, Haytor ward had over-recruited resulting in a low requirement for temporary staff. The Board welcomed the news that the new Bank system had been very successful since it was launched in 2016/17. The Board was advised that there would be a review of ward establishments in line with safer staffing and other guidelines to ensure that the resource and skill mix required on the ward was appropriate to the client group and its care requirements. There needed to be a reconciliation of workforce numbers across the finance (Agresso) and HR (ESR) systems as both used different metrics to measure workforce numbers.
Melanie Walker, Chief Executive, requested that future Safer Staffing reports be reviewed in depth by the Workforce and Organisational Development Assurance Committee before being presented to the Board. This was agreed.
Action 012/18a
Present the Safer Staffing report to the Workforce and Organisational Development Assurance Committee for detailed analysis and review before it is presented to the Board. Lead: Paul Keedwell, Director of Nursing and Practice
The Board noted the high level of leave still to be taken before 31.03.18 and sought assurance from the Executive on how this was being managed. Changes in the way the Health Roster was being used and embedded would help in the planning of leave in the future to ensure a more even spread across the year, though the Executive agreed that action was required immediately to manage the year-end position. To this end, the Executive would report on the measures being taken and the likely year-end outturn to the next meeting of the Workforce and Organisational Development Assurance Committee.
Action 012/18b
Report on the action being taken to manage the year-end leave position at the next meeting of the Workforce and Organisational Development Assurance Committee (March 2018). Lead: Paul Keedwell, Director of Nursing and Practice
Resolved The Chair thanked Chris Burford, Deputy Director of Nursing and Practice, and the Safer Staffing team for the report and the Board received the report.
013/18 (Item 12)
Workforce and Organisational Development Assurance Committee Report Helen England, Director of Strategy, Organisational Development and Workforce, summarised the report. The Committee had looked at the programme of work to improve the Trust’s leadership capacity and capability to achieve its mission to become a centre of excellence and expertise in mental health and learning disability. The Committee had also reviewed recruitment processes and timelines, sickness absence and the actions taken to support the health and well-being of staff, compliance with mandatory and statutory training and apprenticeship programmes.
2.3
Min
utes
Page 14 of 96
Board of Directors Meeting, 12 March 2018 Agenda Item 2.3
9
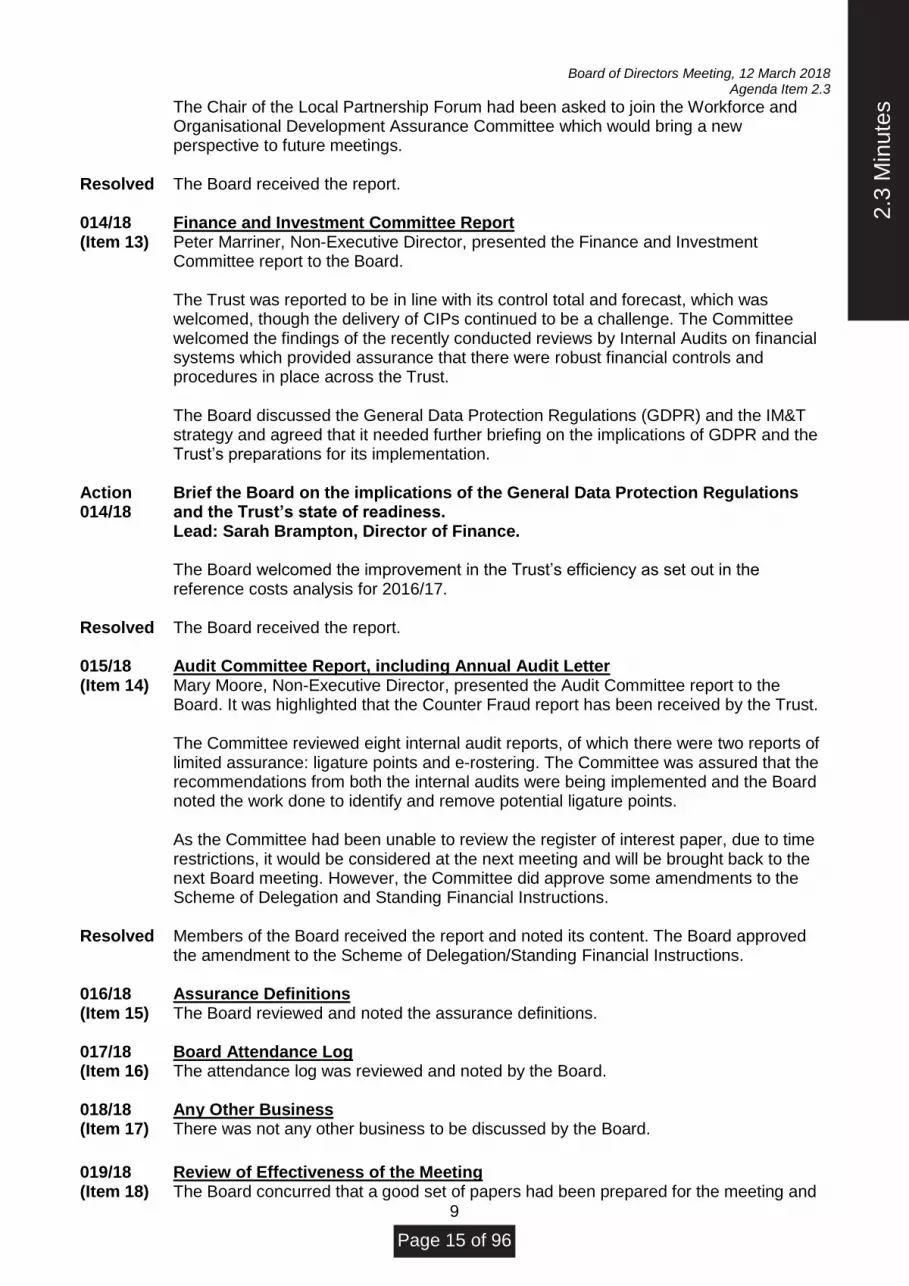
The Chair of the Local Partnership Forum had been asked to join the Workforce and Organisational Development Assurance Committee which would bring a new perspective to future meetings.
Resolved The Board received the report. 014/18 (Item 13)
Finance and Investment Committee Report Peter Marriner, Non-Executive Director, presented the Finance and Investment Committee report to the Board.
The Trust was reported to be in line with its control total and forecast, which was welcomed, though the delivery of CIPs continued to be a challenge. The Committee welcomed the findings of the recently conducted reviews by Internal Audits on financial systems which provided assurance that there were robust financial controls and procedures in place across the Trust.
The Board discussed the General Data Protection Regulations (GDPR) and the IM&T strategy and agreed that it needed further briefing on the implications of GDPR and the Trust’s preparations for its implementation.
Action 014/18
Brief the Board on the implications of the General Data Protection Regulations and the Trust’s state of readiness. Lead: Sarah Brampton, Director of Finance.
The Board welcomed the improvement in the Trust’s efficiency as set out in the
reference costs analysis for 2016/17.
Resolved The Board received the report. 015/18 (Item 14)
Audit Committee Report, including Annual Audit Letter Mary Moore, Non-Executive Director, presented the Audit Committee report to the Board. It was highlighted that the Counter Fraud report has been received by the Trust.
The Committee reviewed eight internal audit reports, of which there were two reports of limited assurance: ligature points and e-rostering. The Committee was assured that the recommendations from both the internal audits were being implemented and the Board noted the work done to identify and remove potential ligature points.
As the Committee had been unable to review the register of interest paper, due to time restrictions, it would be considered at the next meeting and will be brought back to the next Board meeting. However, the Committee did approve some amendments to the Scheme of Delegation and Standing Financial Instructions.
Resolved Members of the Board received the report and noted its content. The Board approved the amendment to the Scheme of Delegation/Standing Financial Instructions.
016/18 (Item 15)
Assurance Definitions The Board reviewed and noted the assurance definitions.
017/18 (Item 16)
Board Attendance Log The attendance log was reviewed and noted by the Board.
018/18 (Item 17)
Any Other Business There was not any other business to be discussed by the Board.
019/18 (Item 18)
Review of Effectiveness of the Meeting The Board concurred that a good set of papers had been prepared for the meeting and
2.3
Min
utes
Page 15 of 96

Board of Directors Meeting, 12 March 2018 Agenda Item 2.3
10
welcomed the fact that the Board pack was shorter than usual though the papers had still covered the main points at issue. The Board welcomed format of the new Integrated Performance and Clinical Operations Report which was clearer to read and easier to follow though more work was required to triangulate the datasets presented and also provide a rich Executive narrative summary to explain current Trust performance. The paper on Strategy Development and Implementation was felt to be well drafted and the Board felt it should be seeking more assurance on the progress being made against the Trust’s strategic aims whilst recognising that a significant amount of work was underway in the Trust.
With there being no further items of business, the Chair closed the meeting.
Date of Next Meeting: 12 March 2018
2.3
Min
utes
Page 16 of 96
Board of Directors, 12 March 2018 Agenda Item 2.4
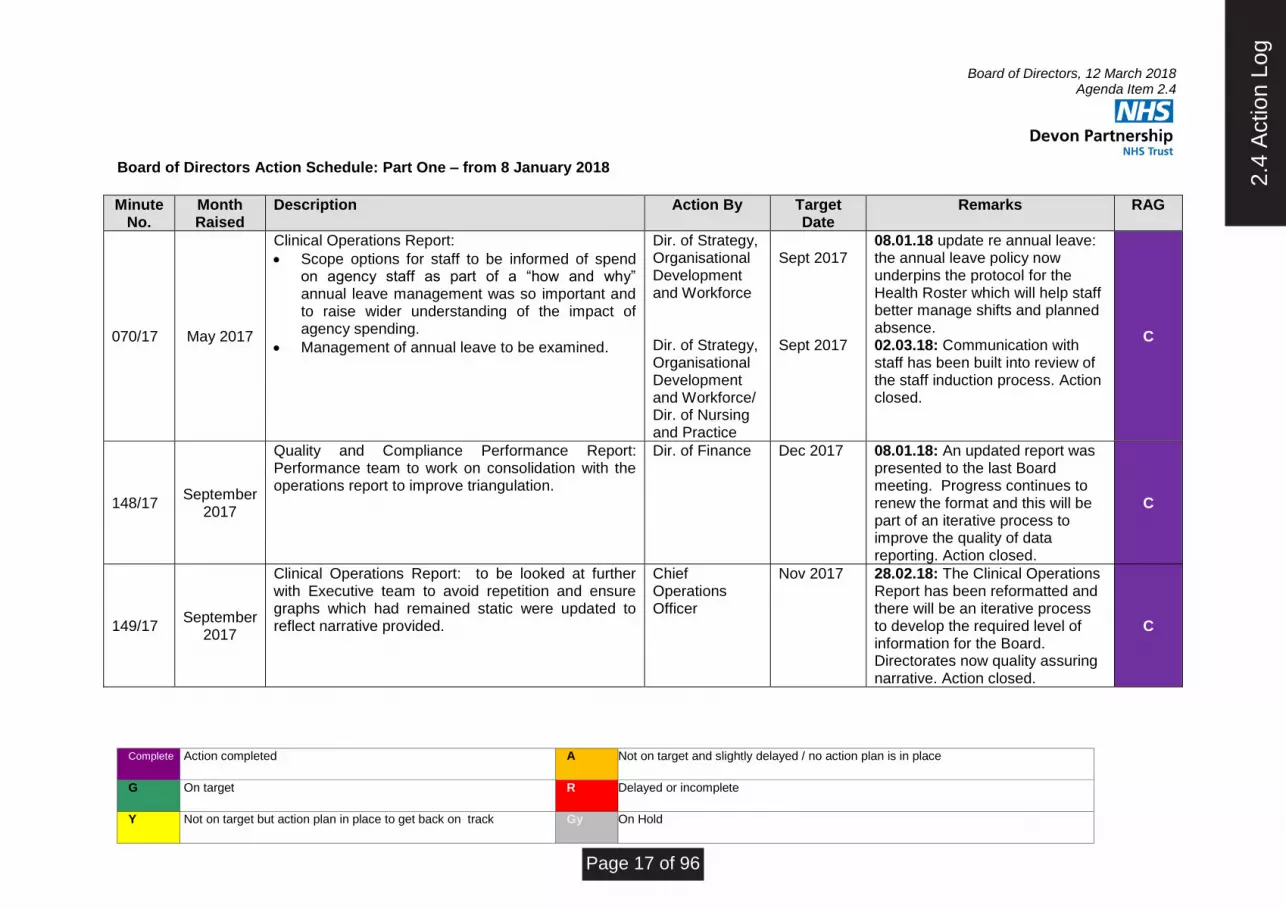
Complete Action completed A Not on target and slightly delayed / no action plan is in place
G On target R Delayed or incomplete
Y Not on target but action plan in place to get back on track Gy On Hold
Board of Directors Action Schedule: Part One – from 8 January 2018
Minute
No. Month Raised
Description Action By Target Date
Remarks RAG
070/17 May 2017
Clinical Operations Report:
• Scope options for staff to be informed of spend on agency staff as part of a “how and why” annual leave management was so important and to raise wider understanding of the impact of agency spending.
• Management of annual leave to be examined.
Dir. of Strategy, Organisational Development and Workforce Dir. of Strategy, Organisational Development and Workforce/ Dir. of Nursing and Practice
Sept 2017 Sept 2017
08.01.18 update re annual leave: the annual leave policy now underpins the protocol for the Health Roster which will help staff better manage shifts and planned absence. 02.03.18: Communication with staff has been built into review of the staff induction process. Action closed.
C
148/17 September
2017
Quality and Compliance Performance Report: Performance team to work on consolidation with the operations report to improve triangulation.
Dir. of Finance Dec 2017 08.01.18: An updated report was presented to the last Board meeting. Progress continues to renew the format and this will be part of an iterative process to improve the quality of data reporting. Action closed.
C
149/17 September
2017
Clinical Operations Report: to be looked at further with Executive team to avoid repetition and ensure graphs which had remained static were updated to reflect narrative provided.
Chief Operations Officer
Nov 2017 28.02.18: The Clinical Operations Report has been reformatted and there will be an iterative process to develop the required level of information for the Board. Directorates now quality assuring narrative. Action closed.
C
2.4
Act
ion
Log
Page 17 of 96
Board of Directors, 12 March 2018 Agenda Item 2.4
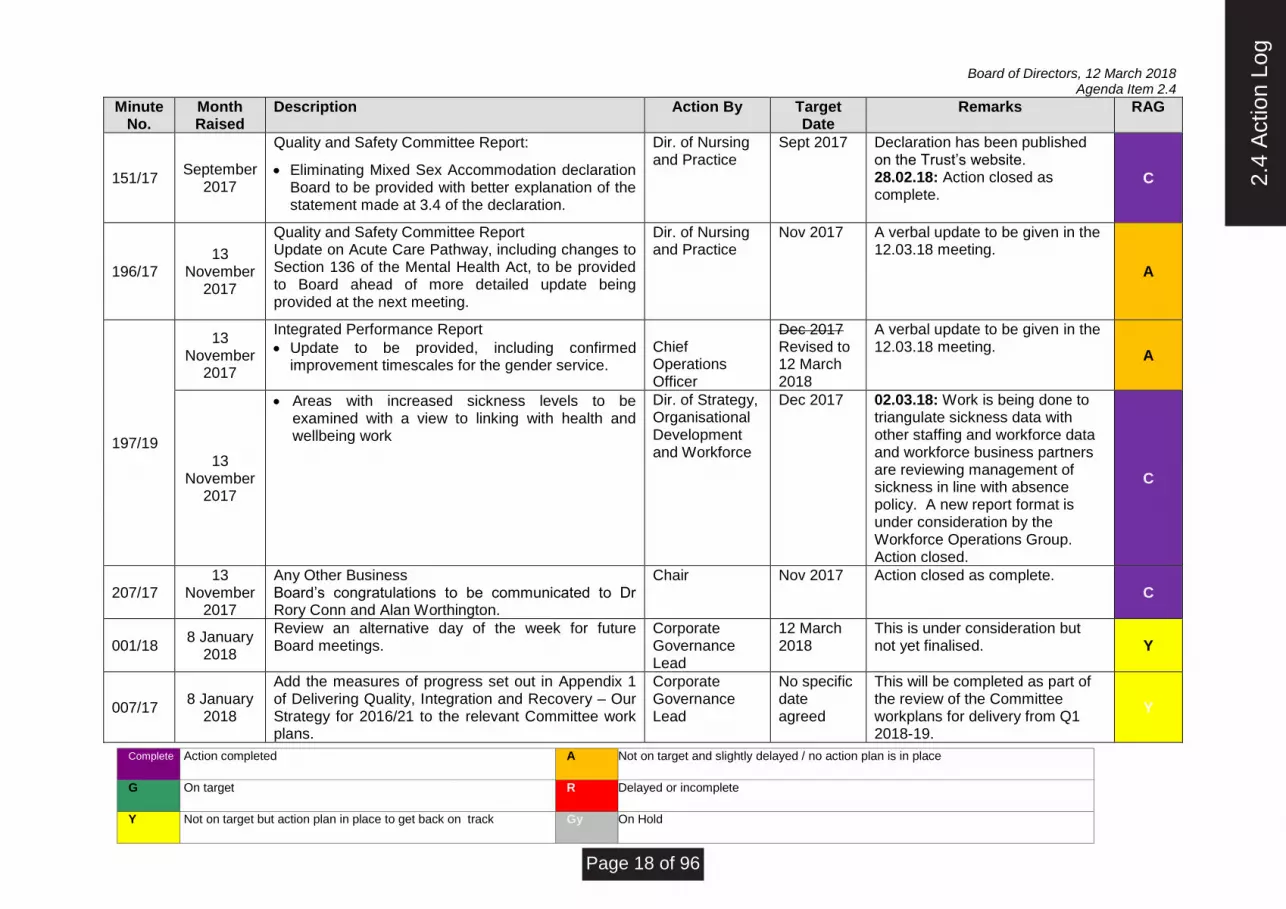
Complete Action completed A Not on target and slightly delayed / no action plan is in place
G On target R Delayed or incomplete
Y Not on target but action plan in place to get back on track Gy On Hold
Minute No.
Month Raised
Description Action By Target Date
Remarks RAG
151/17 September
2017
Quality and Safety Committee Report:
• Eliminating Mixed Sex Accommodation declaration Board to be provided with better explanation of the statement made at 3.4 of the declaration.
Dir. of Nursing and Practice
Sept 2017
Declaration has been published on the Trust’s website. 28.02.18: Action closed as complete.
C
196/17 13
November 2017
Quality and Safety Committee Report Update on Acute Care Pathway, including changes to Section 136 of the Mental Health Act, to be provided to Board ahead of more detailed update being provided at the next meeting.
Dir. of Nursing and Practice
Nov 2017
A verbal update to be given in the 12.03.18 meeting.
A
197/19
13 November
2017
Integrated Performance Report
• Update to be provided, including confirmed improvement timescales for the gender service.
Chief Operations Officer
Dec 2017 Revised to 12 March 2018
A verbal update to be given in the 12.03.18 meeting.
A
13 November
2017
• Areas with increased sickness levels to be examined with a view to linking with health and wellbeing work
Dir. of Strategy, Organisational Development and Workforce
Dec 2017 02.03.18: Work is being done to triangulate sickness data with other staffing and workforce data and workforce business partners are reviewing management of sickness in line with absence policy. A new report format is under consideration by the Workforce Operations Group. Action closed.
C
207/17 13
November 2017
Any Other Business Board’s congratulations to be communicated to Dr Rory Conn and Alan Worthington.
Chair Nov 2017 Action closed as complete. C
001/18 8 January
2018
Review an alternative day of the week for future Board meetings.
Corporate Governance Lead
12 March 2018
This is under consideration but not yet finalised. Y
007/17 8 January
2018
Add the measures of progress set out in Appendix 1 of Delivering Quality, Integration and Recovery – Our Strategy for 2016/21 to the relevant Committee work plans.
Corporate Governance Lead
No specific date agreed
This will be completed as part of the review of the Committee workplans for delivery from Q1 2018-19.
Y
2.4
Act
ion
Log
Page 18 of 96
Board of Directors, 12 March 2018 Agenda Item 2.4
Complete Action completed A Not on target and slightly delayed / no action plan is in place
G On target R Delayed or incomplete
Y Not on target but action plan in place to get back on track Gy On Hold
Minute No.
Month Raised
Description Action By Target Date
Remarks RAG
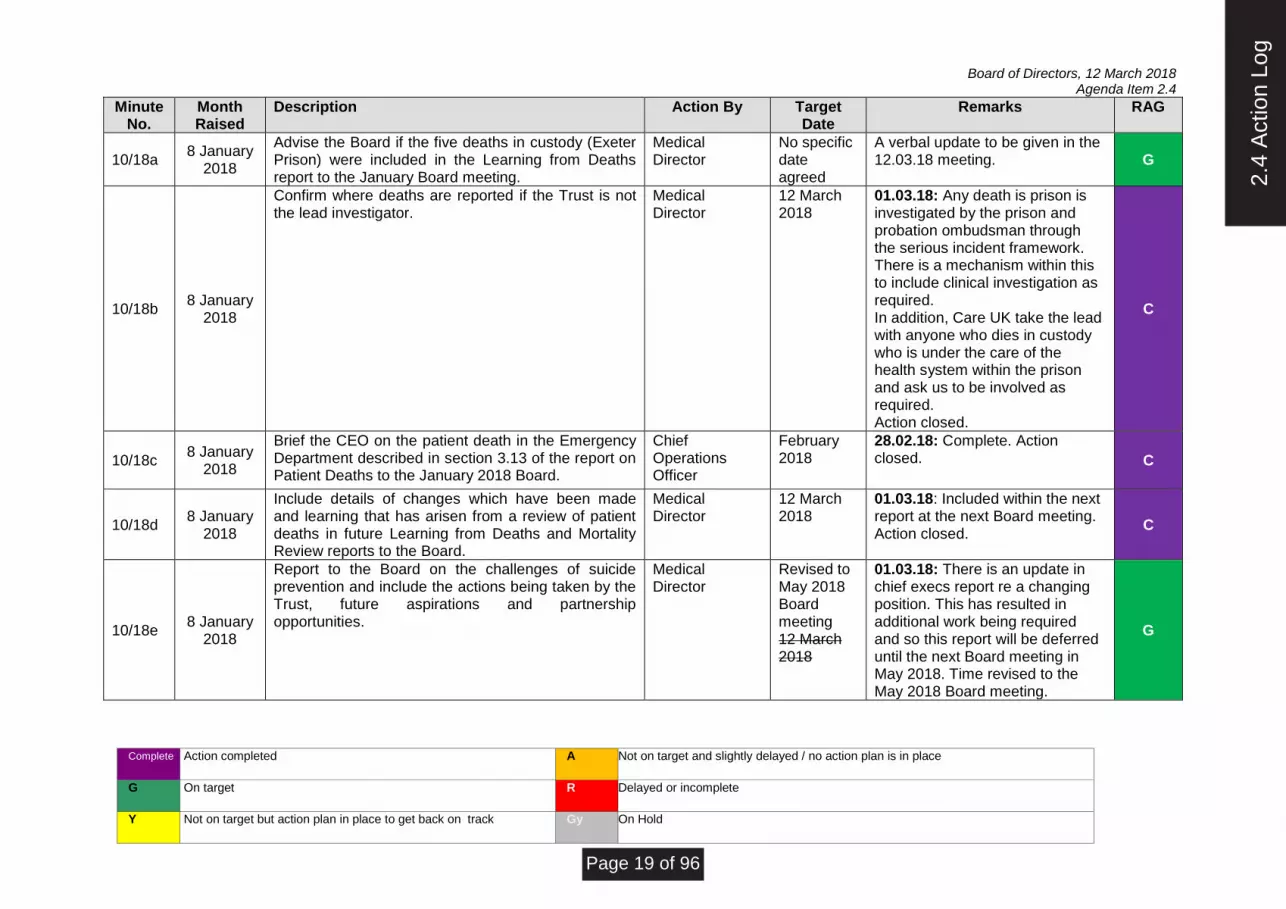
10/18a 8 January
2018
Advise the Board if the five deaths in custody (Exeter Prison) were included in the Learning from Deaths report to the January Board meeting.
Medical Director
No specific date agreed
A verbal update to be given in the 12.03.18 meeting. G
10/18b 8 January
2018
Confirm where deaths are reported if the Trust is not the lead investigator.
Medical Director
12 March 2018
01.03.18: Any death is prison is investigated by the prison and probation ombudsman through the serious incident framework. There is a mechanism within this to include clinical investigation as required. In addition, Care UK take the lead with anyone who dies in custody who is under the care of the health system within the prison and ask us to be involved as required. Action closed.
C
10/18c 8 January
2018
Brief the CEO on the patient death in the Emergency Department described in section 3.13 of the report on Patient Deaths to the January 2018 Board.
Chief Operations Officer
February 2018
28.02.18: Complete. Action closed. C
10/18d 8 January
2018
Include details of changes which have been made and learning that has arisen from a review of patient deaths in future Learning from Deaths and Mortality Review reports to the Board.
Medical Director
12 March 2018
01.03.18: Included within the next report at the next Board meeting. Action closed.
C
10/18e 8 January
2018
Report to the Board on the challenges of suicide prevention and include the actions being taken by the Trust, future aspirations and partnership opportunities.
Medical Director
Revised to May 2018 Board meeting 12 March 2018
01.03.18: There is an update in chief execs report re a changing position. This has resulted in additional work being required and so this report will be deferred until the next Board meeting in May 2018. Time revised to the May 2018 Board meeting.
G
2.4
Act
ion
Log
Page 19 of 96

Board of Directors, 12 March 2018 Agenda Item 2.4
Complete Action completed A Not on target and slightly delayed / no action plan is in place
G On target R Delayed or incomplete
Y Not on target but action plan in place to get back on track Gy On Hold
Minute No.
Month Raised
Description Action By Target Date
Remarks RAG
011/18a 8 January
2018
Provide historical context to the data presented on the performance dashboard to provide greater context and analysis.
Chief Operations Officer
12 March 2018
28.02.18: Included in the IPR narrative. Action closed.
C
011/18b 8 January
2018
Review in detail sickness absence at the next meeting of the Workforce and Organisational Development Assurance Committee and report back findings to the Board.
Dir. of Strategy, Organisational Development and Workforce
Revised to May 2018 1 March 2018
02.03.18: This work is being progressed but has been delayed as the Workforce Information post has been vacant. A new post-holder has now been recruited and this report will be presented to the first Workforce and Organisational Development Assurance Committee in 2018-19 following which it will be reported to the Board.
Y
011/18c 8 January
2018
Include details of instances of prone restraint to the Performance Report.
Chief Operations Officer
12 March 2018
28.02.18: Included in the Clinical Operations report. It is also reported to the Quality and Safety Committee. Action closed.
C
012/18a 8 January
2018
Present the Safer Staffing report to the Workforce and Organisational Development Assurance Committee for detailed analysis and review before it is presented to the Board.
Dir. of Nursing and Practice
12 March 2018
This report was considered. Action complete.
C
012/18b 8 January
2018
Report on the action being taken to manage the year-end leave position at the next meeting of the Workforce and Organisational Development Assurance Committee (March 2018).
Dir. of Nursing and Practice
12 March 2018
A verbal update to be given in the 12.03.18 meeting.
Y
014/18 8 January
2018
Brief the Board on the implications of the General Data Protection Regulations and the Trust’s state of readiness.
Dir. of Finance
12 March 2018
On agenda for 12.03.18 Board meeting. Proposed for closure. C
2.4
Act
ion
Log
Page 20 of 96

Board of Directors Meeting, 12 March 2018 Agenda Item 2.5
Devon Partnership NHS Trust Board of Directors
Chief Executive’s Report
March 2018
2.5
Chi
ef E
xecu
tive'
s R
epor
tM
arch
201
8
Page 21 of 96

Board of Directors Meeting, 12 March 2018 Agenda Item 2.5
2
Staff Survey 2017 The National Staff Survey took place at the end of 2017. We had an excellent response rate of 68%, which was an increase of 5% since 2016 and means that we continue to be one of the best mental health and learning disability trusts in this respect. The results have remained largely unchanged from the previous year with no areas significantly deteriorating. The one area of significant improvement is in staff reporting incidents of violence and aggression which we think may be in response to our Four Step programme. Our staff engagement score has also improved slightly and is in line with the average for our comparator group. Our top five ranking scores were in:
• Staff not feeling that they have to attend work despite feeling unwell
• Reporting incidents of violence
• Support from immediate managers
• Satisfaction with opportunities to work flexibly
• Very low numbers of staff experiencing physical violence from other staff The staff survey scores confirm that further work is needed in the quality of appraisals and training, in staff being satisfied with the quality of work and care that they are able to deliver as well as in our use of feedback from patients and carers. Our Journey events held in 2017 helped to identify the improvements that need to be made in these areas and work is in progress to do this in collaboration with our staff and people who use our services. We will discuss the plans that we need to take in response to this and present an update to the next Board meeting. Staff Retention The Trust has developed a plan focused specifically on measures to improve staff retention as part of its strategic approach to workforce resourcing. Devon Partnership NHS Trust is part of wave 2 of a national programme on improving retention led by NHS Improvement. A site visit to the Trust was held on 9 February by the NHS Improvement team and they reported that they were impressed with the approach to retention adopted by the Trust and the plan itself, as well as the way in which targeted actions were underpinned by analysis of workforce data. PICU Ward Manager Appointed The Adult Directorate is pleased to announce that our new Psychiatric Intensive Care Unit (PICU), The Junipers, now has a Ward Manager. Successful candidate Keri Gilchrist comes from an acute sector background and will start in role in the next couple of months. Keri is very passionate and enthusiastic about the vision for the new PICU and is bringing a number of new of ideas to put into place. We are very much looking forward to welcoming Keri and help her put her plans into place.
2.5
Chi
ef E
xecu
tive'
s R
epor
tM
arch
201
8
Page 22 of 96

Board of Directors Meeting, 12 March 2018 Agenda Item 2.5
3
Care Quality Commission (CQC) - Well-Led Inspection Board members will have seen my note of thanks to everyone for their time and support during February’s CQC’s visit. It appears to have gone well and the inspectors have asked me to thank staff for the warm and open way in which they responded to their questions in the many interviews that took place during the week. The inspectors were also extremely impressed with the passion, enthusiasm and commitment shown by our staff. This has been a regular theme in the CQC’s comments over the last few years and feedback of this kind is always a source of great pride to me and the other members of the Board. As ever, we are always cautious about assuming any significance in the feedback following the inspection and we are not expecting the formal feedback from the CQC until the end of March. We will have an opportunity to check this for factual accuracy before it is published some weeks later. Whatever the CQC’s findings, everyone involved has done a great job and I believe we have demonstrated that we are an organisation well on the way to being. Fit and Proper Persons Following the recent issue of new guidance from NHS Providers and as a result of queries raised during our recent Well Led Inspection, we have been reviewing our compliance against the Fit and Proper Person regulations and we will be updating the Board in part 2. This is a very important regulatory matter and will be inviting CQC colleagues to review the files we hold for our Directors in the next few weeks. Smoke Free The Trust’s Smoke Free pledge was signed at the last Board meeting, with the aim for the Trust to be smoke free from 14 March 2018. The pledge is a clear and visible way for NHS organisations to show their commitment to help smokers quit and provide smokefree environments to support them. We have agreed that from 14 March 2018, the e-burn electronic cigarette can be used on our general adult and older people’s wards in a person’s own bedroom and designated outdoor areas. The vaping devices / e-cigarettes that people can use in areas of lower risk and greater independence is still under consideration. Along with other mental health trusts in the country, we are striving to balance people’s rights and preferences with health considerations and the burden that is placed on our staff in administering the use of e-cigarettes in inpatient environments. Mother and Baby Unit Earthworks on the new Mother and Baby Unit (MBU) started in mid-February and despite a slight delay with last week’s bad weather, the project is continuing with good pace. The Board is considering some papers on the MBU in part 2 of the meeting. Eating Disorders Awareness Staff from the Haldon Unit took the “Sock it to eating disorders” message to visitors to the Royal Devon & Exeter Hospital during the week of 26 February. Team members invited people to show their socks off in support of raising awareness of these misunderstood and often devastating mental illnesses.
2.5
Chi
ef E
xecu
tive'
s R
epor
tM
arch
201
8
Page 23 of 96

Board of Directors Meeting, 12 March 2018 Agenda Item 2.5
4
Adverse Weather The region was affected by some of the worst weather we have seen for a while and whilst the NHS as a whole responded admirably, I am sure the Board will join me in commending our own staff for their diligence and commitment during an incredibly difficult few days. Whilst there is learning to be had across peninsular, there are numerous accounts of our staff going above and beyond to support people within our care. The response was fantastic and ensured that services kept going in some incredibly challenging conditions. National Workforce Strategy Consultation Health Education England is currently consulting on the first national system wide workforce strategy to be developed in 25 years. The final strategy is due to be published in June or July 2018 to coincide with the celebrations of the 70th anniversary of the NHS. The strategy outlines the key interventions that are necessary to address the real workforce challenges facing both the NHS and the wider care sector as well as the transformation needed to ensure that the NHS has the workforce it requires in the future. The actions set out in the strategy will be designed to ensure that the NHS has workforce it needs in the right numbers and with the right skills, values and behaviours to deliver care of a high quality. The Trust already has a comprehensive programme of work on developing its current and future workforce though we will look to the opportunities created by the national strategy to deliver workforce solutions at scale for the NHS and care sector. Our Director of Strategy, Organisational Development and Workforce, Helen England, is coordinating a response to the consultation on behalf of the Devon Sustainability and Transformation Partnership. Mental Health Patients treated far from Home “less likely to recover” The CQC has warned that thousands of people with serious mental health problems are being sent for treatment far away from their homes, and left isolated and less likely to recover. The Guardian reported on a survey published by CQC on 1 March 2018 which found 63% of people with complex psychosis and other serious mental health conditions end up being sent "out of area" for care because the local NHS does not have the beds, staff, or both to treat them. The survey also showed many people are being cared for sometimes many miles away from home, and sometimes for more than three years at a time. This dislocation can mean that people can become isolated from their friends, from their families and from the services that will provide care once they have been discharged. At the Trust, we keep the number of patients who are placed out of area under close review and have constantly strived to reduce numbers and bring these patients back to Devon. Valued Care in Mental Health: Improving for Excellence NHS Improvement plan to publish Valued Care in Mental Health: Improving for Excellence in mid-March 2018. We will receive an embargoed copy soon, and a physical copy will follow. NHS Improvement’s model will be uploaded as an interactive PDF which they will maintain and they hope to gather more case studies from providers. As soon as we receive more briefing, I will advise the Board further.
2.5
Chi
ef E
xecu
tive'
s R
epor
tM
arch
201
8
Page 24 of 96

Board of Directors Meeting, 12 March 2018 Agenda Item 2.5
5
Kirkup Review into Liverpool Community Health An independent review into the widespread failings by Liverpool Community Health NHS Trust from November 2010 to December 2014 has been published by NHS Improvement. The review conducted by Dr Bill Kirkup CBE looks at number of issues with the Trust and the oversight arrangements with NHS Trust Development Authority, NHS England and commissioners. The full report is available here: https://improvement.nhs.uk/news-alerts/independent-review-liverpool-community-health-nhs-trust-published/ The report outlines how cost improvement programmes imposed by the trust in a bid to gain foundation trust status put the safety of patients at risk, and that a culture of bullying meant that staff were scared to speak up or that incidents were ignored or not escalated. The review found that the external overview of the trust failed to identify the services problems for at least four years, and concluded that earlier intervention would have reduced the avoidable harm that occurred. The report makes series of recommendations and we will review any which may apply to the Trust. National Suicide Prevention Alliance On 1 February 2018 Jeremy Hunt announced at the National Suicide Prevention Alliance, his zero suicide ambition for the NHS. He has asked NHS organisations to do more to prevent deaths of patients in NHS care and has already earmarked £25 million within plans for the Five Year Forward View to support this. Sustainable Transformation Partnerships with the highest suicide rates have been invited to bid for money to support their suicide prevention activities and though Devon – which has suicide rates that are higher than the national average has not been invited to bid. Cornwall and the Isles of Scilly has received this invitation and there may be opportunities to benefit indirectly from this funding given our relationships across both counties. Funding for Mental Health Services must reach the Frontline to enact Change The CQC has published ‘Monitoring the Mental Health Act in 2016/17’ which concludes that mental health services are not doing enough to ensure that people whose liberty has been restricted under the Mental Health Act are able to exercise their rights; and that this situation is not improving. Responding to report, NHS Providers has warned that, like other parts of the NHS, mental health trusts are facing major staffing shortages and are struggling to cope with rapidly rising demand. Alongside this, and despite increases in national funding for mental health, providers face a severe funding squeeze. However an independent review of the Mental Health Act, currently underway by Professor Sir Simon Wessely, may ensure that mental health is given the resources it needs to ensure services are both available and most appropriate to meet patients’ needs. We will keep further developments under close review. The full report is available to read here: http://www.cqc.org.uk/publications/major-report/monitoring-mental-health-act-report New Enquiry Report The National Confidential Inquiry into Suicide and Homicide by People with Mental Illness has issued a new report entitled “Safer Care for People with Personality Disorder”. We are considering this report and how it may shape our approach to patients with personality disorder and we will bring a briefing back to the Board in due course. A full copy of the report can be found at: http://research.bmh.manchester.ac.uk/cmhs/research/centreforsuicideprevention/nci/reports/pdreport.pdf
2.5
Chi
ef E
xecu
tive'
s R
epor
tM
arch
201
8
Page 25 of 96

Board of Directors Meeting, 12 March 2018 Agenda Item 2.5
6
Speaking up Culture, Processes and Policies The requirement for all NHS Trusts to have a ‘Freedom to Speak Up’ Guardian Service has been in place since October 2016. The National Guardian’s Office provides leadership, training and advice for Freedom to Speak Up Guardians and works to promote a transparent and open culture across the NHS that enables staff to speak up and ensures that concerns are handled according to best practice. In September 2017 the National Guardian’s Office conducted a review of the speaking up policies, processes and culture at Northern Lincolnshire and Goole NHS Foundation Trust. This was in response to concerns that had been raised with the National Guardian’s Office and the Care Quality Commission from staff that the Trust failed to respond to concerns about patient safety and that a bullying culture existed within the organisation. The review concluded that the Freedom to Speak up culture at the Trust needed improvement. Policies and procedures were not deemed to provide sufficient support to staff to speak up about issues or concerns. Issues raised by staff were not always handled according to good practice. The Guardian Service within the Trust did not have sufficient time and capacity to meet the needs of workers at the Trust. Staff described a bullying culture that existed within parts of the Trust that meant that staff were often afraid to speak up. Twenty three recommendations were made to the Trust on how it could improve its Freedom to Speak up arrangements. One included the reports submitted by the Freedom to Speak Up Guardian to the Trust Board which were considered to lack the necessary detail and content to ensure that the Board had sufficient information about the speaking up policies, procedures and culture at the trust. The independent Guardian Service for Devon Partnership NHS Trust has now been in place for one year. The first year’s worth of data is being analysed by the provider and will form the basis of a ‘valued added report’ which will be submitted for review to the next Workforce and Organisational Development Assurance Committee. The report will consider the recommendations from the review relating to Northern Lincolnshire and Goole NHS Foundation Trust and will consider any lessons that could be applied to the Trust to inform the on-going development of our Freedom to Speak Up arrangements. NHS Planning Guidance: Trust’s Operational Plan for 2018-19 NHS Providers have issued planning guidance as a refresh of plans already prepared under the two-year NHS Operational Planning and Contracting Guidance 2017/19. The briefing sets out detail of how the additional funding from the November 2017 budget will be allocated and the developments in national policy with regards to system level collaboration. In part 2 of today’s Board meeting we will look at the first draft our Operational Plan 2018-19 which we will submit in March before finalising our Plan in April which we will bring back to the May Board meeting.
Compiled by: Janet Morrell, Interim Executive Business Lead Presented by: Melanie Walker, Chief Executive March 2018
2.5
Chi
ef E
xecu
tive'
s R
epor
tM
arch
201
8
Page 26 of 96

Report Summary
Agenda item number: 4.1
Report provided: Agenda
Item: Integrated Performance and Clinical Operations Report
To note:
For assurance: X Report
to: Board of Directors
For approval: X
For information:
Meeting date:
12 March 2018
Integrated Performance and Clinical Operations Report
Accountable Director(s):
Dr David Somerfield, Chief Operating Officer
Presented by:
Dr David Somerfield, Chief Operating Officer
Report author(s):
Dr David Somerfield, Chief Operating Officer
Alignment to the Trust’s strategic aims:
Our aims:
To deliver consistently high quality care and treatment
X To ensure our services are driven by the voices of people who use them
X
To build a reputation as a recognised centre of excellence and expertise
X To attract and retain talented people and to create a great place to work, with a shared sense of pride and ambition
To challenge discrimination and stigma, and to champion recovery, inclusion and wellbeing
X To be an efficient, thriving and successful organisation with a sustainable future
X
Purpose of report:
The report is to provide assurance to the Trust Board of Directors of the Directorate Governance Boards oversight of clinical delivery and performance.
Summary of the key issues:
The report details key achievements and risks
Recommendations:
Members of the Committee are asked to note the contents of the report
Report previously presented to:
Committee/Group: Date: Report title: Outcome/action:
Summary of compliance implications:
Areas of risk have been assessed as appropriate to mitigate the risk of Care Quality Commission (CQC) compliance implications.
Does this report provide assurance in respect of a new / existing risk/s?
Type of risk/s New & Existing Corporate Assurance X Risk Register
Level of Assurance and trend: 1 to 10
Significant Limited None
6
4.1
Inte
grat
ed P
erfo
rman
cean
d C
linic
al O
pera
tions
Rep
ort
Page 27 of 96

Board of Directors, 12 March 2018 Agenda Item 4.1
DEVON PARTNERSHIP NHS TRUST BOARD OF DIRECTORS
Meeting 12 March 2018
CLINICAL OPERATIONAL AND PERFORMANCE REPORT
1. Situation 1.1 To provide the Trusts Board of Directors with an overview of the clinical operational and
performance issues from the Directorate Governance Boards February 2018. 2. Background 2.1 The Directorate Governance Boards meet monthly to review key performance indicators,
quality and financial measures across their services. The Boards report to the monthly Senior Management Board Performance Meeting which in turn reports to Quality and Safety Committee and Trust Board of Directors. The February Directorate Governance Boards reported to the Senior Management Board on 26 February 2018.
3. Assessment 3.1 OPMH Areas of achievement:
• The Directorate continues to improve delayed discharges and have successfully worked on data accuracy of Delayed Transfers of Care (DToC) which has improved the position markedly. Community Support Workers from community teams are now supporting wards to facilitate early discharge.
• Consultant job planning has been completed to move to new model of care under Smart Recovery.
• The Directorate continues to achieve the 10 day assessment target.
• Bristol Dementia and Wellbeing Service continue to meet its targets eg 10 day target 93/85%. The service is participating in 4 research trials and has recruited over 750 patients who can be invited in to research trials.
• Belvedere supervision rate has been rectified and is now 100%.
• Uptake of Flu vaccine is slightly higher at 65% than current Trust average of 64% (with a target of 70%). Belvedere ward have recovered their position from 48% to currently at 65%.
Areas of concern:
• Staffing on Meadow View remains a significant concern, particularly the consultant psychiatrist. Locum consultant psychiatrists are very scarce at present and the current locum leaves at the end of March. The Older Peoples Mental Health (OPMH) and Adult Directorates are currently exploring mutual medical support. Recruitment for other clinical posts remains challenging and is impacting on management and clinical delivery.
• The administration of community clinical teams has been affected by the administration restructure and this is being urgently reviewed by the Directorate.
4.1
Inte
grat
ed P
erfo
rman
cean
d C
linic
al O
pera
tions
Rep
ort
Page 28 of 96

Board of Directors, 12 March 2018 Agenda Item 4.1
• Medical staffing vacancies are impacting on waiting times in the Devon Memory Service. Current Referral to Treatment Times are 5 weeks for Exeter, 5 weeks in North and an improvement from 12 to 10 weeks in South Devon. Unfortunately the new appointment to DMS in South Devon has now declined the post. Mitigations are urgently being explored.
• The rate of falls was within predicted range but there was one significant incident last month. 3.2 Adult Directorate Areas of achievement:
• The Cedars Mental Health Place of Safety refurbishment is currently under way and is due to be completed by April. Funding to enable a substantive staff group for the new 2 bedded Place of Safety has been part of contract discussions.
• The new Rehabilitation model of care has been agreed at the Smart/Acute Care Pathway Programme Board and Senior Management Boards and a business case is now being developed.
• There are now three locality Interim Clinical Directors in place.
• The Directorate is achieving the 95% 12 month CPA review target.
• There has been a continued reduction in Delayed Transfers of Care (DToC).
• The post-discharge seven day follow up target has been met. The 48 hour follow up continues to vary but with all patients being followed up safely.
Areas of concern:
• Recruitment for the Psychiatric Intensive Care Unit (PICU) consultant post has been unsuccessful. A nurse consultant post is being developed as an alternative which is a successful model established elsewhere. There remain significant consultant vacancies which are impacting on operational delivery.
• Short-term sickness has increased and the Directorate sickness rate has increased to 8% from 5.3% the month before.
• Assessment targets continue to remain challenging due to demand and capacity. The Directorate continue to work on addressing these issues. There continue to be vacancies in the assessment service as well as long and short-term sickness.
• The Directorate currently has 70 (66 in September) WTE vacancies with a turnover 12%.
• Out of Area Placements have been particularly high this month which is related to an increase in the level of clinical activity and compounded by the temporary loss of 12 step down beds in South Devon as the provider moves premises. The Directorate continues to manage flow closely, particularly DToC which has been declining over the last few months although have seen a recent increase. The Acute Care Pathway project plan is being reviewed this month after an external review and learning from NHSI.
• The S136 changes in the Mental Health Act came in to force on 11 December. There have been no incidents attributable to these changes.
3.3 Specialist Directorate Area of achievement:
• The PPT waiting lists remains stable despite reallocation of resources to support Adult Directorate pathways.
• Das has maintained excellent recovery rates (South Devon and Torbay 55%, NEW Devon 56.4%).
• Perinatal services received very positive feedback from the Care Quality Commission (CQC) inspection of Torbay Hospital maternity services.
• Health and Neuro-psychology waiting times have significantly reduced at the Royal Devon and Exeter Hospital.
• There are two Liaison clinicians being trained as part of the Flow Academy.
4.1
Inte
grat
ed P
erfo
rman
cean
d C
linic
al O
pera
tions
Rep
ort
Page 29 of 96

Board of Directors, 12 March 2018 Agenda Item 4.1
• There have been very positive compliments received related to transition support in the Learning Disability Service.
• Torbay and North Devon liaison services are achieving the 1 hour waiting time for Emergency Departments but this continues to be a challenge due to significant numbers of patient attendances in Exeter.
Areas of concern:
• Inpatient safer staffing remains challenging due to vacancies and a high sickness rate on the Additional Support Unit (ASU) and the Haldon. ASU continues to require a long term agency nurse to cover shifts. The Directorate continues to work on embedding Positive Behavioural Support on the ASU.
• Delayed discharges remain challenging on both the ASU and Haldon wards due to clinical complexity and high need which is not reflected in onward community non-statutory service provision. The CCG and Devon County Council (DCC) are planning to address the provision of housing and support to people with a learning disability as a Sustainability and Transformation Plan (STP) project stream.
• The Community Eating Disorders Service Pilot is over service capacity. Work is well under way with the CCGs to finalise a business case for a Devon-wide community eating disorder service.
• There remain issues regarding waiting times, waiting lists and sustaining improvements within Gender services. The service will be in a position to finalise clinic trajectories later in March as job planning, training and competency attainment is completed which will define medical capacity. Assessment trajectories include the anticipated additional time required for those patients who have complex presentations and co-morbid mental health and neurodevelopmental conditions which account for around 40% of referrals. Under the proposed new assessment pathway both psychology and psychiatry staff will undertake these assessments to maximise the clinics capacity.
• There are continuing concerns related to the achievability of the National Commissioning for Quality and Innovation (CQUIN) for Emergency Department. Data issues remain in North Devon and South Devon and Torbay General Hospitals. In North Devon this related to a new IT system which means no coding is taking place, in South Devon and Torbay this relates to general engagement in the process which has been compounded by winter pressures.
• Core Depression and Anxiety Service (DAS) services have been affected by the rapid implementation of the IAPT Long Term Conditions service with reduced Step 2 capacity and some increased waits will make achieving access/prevalence targets challenging across both CCGs. The access target remains behind but has improved and there is a mitigation plan in place. Numbers entering LTC are significantly lower than anticipated.
• There are on-going estates issues for teams operating out of acute hospital sites and within Wonford House with team expansion for instance in perinatal services.
3.4 Secure Directorate Areas of achievement
• The Directorate held the first quality Improvement collaborative at Langdon on 1st February 2018. This was an event which saw staff, patients and carers coming together to share and learn about the quality improvement initiatives happening at Langdon. Sessions on the day included an overview of future aspirations for the directorate, a basic introduction to quality improvement tools and world café sessions about each of our key directorate projects. The Directorate finished with patients proudly showing the new admissions video "This is Langdon" which has been co-produced by our patients and staff to give people being admitted to our service an idea of what it is like at Langdon Hospital.
4.1
Inte
grat
ed P
erfo
rman
cean
d C
linic
al O
pera
tions
Rep
ort
Page 30 of 96

Board of Directors, 12 March 2018 Agenda Item 4.1
• The senior leadership team have started a programme of simulation programmes based on learning from incidents feedback.
• Clinic rooms across site have been standardised to support staff which will significantly improve safety and the ability to respond in a timely way. This excess equipment has been centralised which represents a substantial cost saving.
• The Step Care model has now been implemented within the three Devon prisons. Extra support has been provided to the mental health team in HMP Exeter in the form of our experienced prison mental health band 7 nurse who will now be full time within HMP Exeter for a period of 3 months.
• Actual occupancy in January was 98.58%, 0.58% above the internal target of 98% (comprised of a 97% budgeted target and 1% CIP occupancy target). The average occupancy for the period from April 2017 to January 2018 was 98.87%, 1.87% above budgeted occupancy and 0.87% above achieving full occupancy CIP of 98%.
Areas of concern:
• Sue Smith acting Deputy COO and will be spending 2 days a week back at Langdon supporting the Directorate in the absence of a member of the senior management team due to sickness.
• The ligature risk in HMP Exeter is on the Directorate Risk Register and Corporate Assurance Framework with a risk score of 5x4 = 20. There have been no further suicides in Devon prisons since November. A review has been completed of the 5 cases to identify common themes and learning points which has led to a series of work streams including further training for staff and a debrief with an external facilitator. Additional management support has been placed in HMP Exeter for a 3 month period to support the team.
• A number of safeguarding concerns have been raised over the past few months. These have resulted in three section 42 enquires. A systemic review of one service is being undertaken with an external reviewer. The senior leadership team with secure services are working closely with teams to address all immediate concerns.
• Patients and families have raised concerns regarding difficulty with the distances some need to travel to visit. Our patient and careers liaison worker is looking into this to find a sustainable solution.
• Sickness absence increased from 5.72% in December to 6.56% in January, this is just below the Trust average of 6.64%.
All of these areas will be reviewed and improvement plans will be put in place.
4. Prone restraint 4.1 The Trust Board of Directors has requested a report of all Incidents of prone restraint within
this report. Episodes of prone restraint are currently reported to the Quality and Safety Committee. The table below shows the breakdown of Prone Restraint by Department. There has been a review of the existing Prone Restraint incidents to ensure accuracy of the data and an amendment to the Risk Management System to make the reporting of Prone Restraint much clearer. Rather than just having Prone as an intervention there are now two options (Prone –face down) and Prone (face down – seclusion exit). For complete clarity we have also changed the intervention Supine to Supine – Face Up.
Department Total 01/08/2017 01/09/2017 01/10/2017 01/11/2017 01/12/2017 01/01/2018
Ashcombe Ward 8 3 1 2 1 1
Delderfield 7 4 2 1
Coombehaven 5 1 2 2
Haytor 4 1 1 2
Ocean View 4 1 1 2
4.1
Inte
grat
ed P
erfo
rman
cean
d C
linic
al O
pera
tions
Rep
ort
Page 31 of 96

Board of Directors, 12 March 2018 Agenda Item 4.1
Department Total 01/08/2017 01/09/2017 01/10/2017 01/11/2017 01/12/2017 01/01/2018
Moorland View 3 1 2
LD IATT - Exeter & East
1 1
Warren Ward 1 1
Beech Unit 1 1
4.2 Over the last month the Trust has also created a monthly report which is sent to the teams to
check the accuracy of their reporting. The table below shows all Prone Restraint incidents in the last two months and the length of time of prone restraint. This shows that episodes are very brief. There are two incidents that do not have a duration entered and there are no incidents over duration of five minutes. No significant injuries to patients have occurred.
Incident Date Duration Position Start Time End Time Department
29/01/2018 00:02:00 Prone (Face Down) 12:10:00 12:12:00 Warren Ward
17/01/2018 00:01:00 Prone (Face Down) 13:59:00 14:00:00 Beech Unit
09/01/2018 00:01:00 Prone (Face Down) 19:36:00 19:37:00 Ashcombe Ward
09/01/2018 Prone (Face Down) 19:36:00 19:36:00 Ashcombe Ward
06/01/2018 Prone (Face Down) 09:00:00 09:00:00 Ocean View
04/01/2018 00:01:00 Prone (Face Down) 11:00:00 11:01:00 Ocean View
28/12/2017 Prone (Face Down) LD IATT - Exeter & East
25/12/2017 00:01:00 Prone (Face Down) 14:44:00 14:45:00 Coombehaven
08/12/2017 Prone (Face Down) Delderfield
08/12/2017 00:05:00 Prone (Face Down) 14:30:00 14:35:00 Coombehaven
07/12/2017 00:05:00 Prone (Face Down) 14:30:00 14:35:00 Ashcombe Ward
5. Devon-wide Major Incident 1 to 3 March 2018 5.1 A Major Incident was declared Devon-wide on the 1 March due to heavy snow fall, gales and
flooding leading to severe disruption to travel, statutory services and the potential for loss of life. The Trust prepared beforehand enacting its severe weather business continuity plans. All wards, CRHT and liaison services were maintained throughout despite complete travel disruption (other than on foot) and loss of power at Langdon on the 2 March. We had exceptional help from clinical staff and managers (many of whom were stranded overnight at work) and a group of volunteer twenty-one 4x4 drivers who responded to a social media request for assistance. The Trust will be reviewing learning from the incident.
6. Recommendations 6.1 Members of the Trust Board of Directors are requested to note the contents of the report and
the mitigations in place to address current issues. Compiled by: Dr David Somerfield, Chief Operating Officer Presented by: Dr David Somerfield, Chief Operating Officer Date: March 2018
4.1
Inte
grat
ed P
erfo
rman
cean
d C
linic
al O
pera
tions
Rep
ort
Page 32 of 96

Integrated Report
Report as at end of January 2018
1
11
14
21
5
1
3
2
26
10
6
4
4 12 4 10 20
Safe Effective Caring Responsive Well‐Led
1 of 26
4.1
Inte
grat
edP
erfo
rman
ce a
nd
Page 33 of 96

KPI‐253 ‐ Delayed Discharges
PICU ‐ PICU
OOA ‐ Out of Area
KPI‐305 ‐ Routine Referrals ﴾10 Days﴿
KPI‐306 ‐ Urgent Referrals ﴾5 Days﴿
Bed Occ ‐ Bed Occupancy
LoS ‐ Length of Stay
Contacts ‐ Attended Contacts
DNAs ‐ DNAs
KPI‐177 ‐ LD Access to Care
KPI
7.5%
‐
‐
80%
90%
‐
‐
‐
‐
100%
Target
2.6%
11
40
60.8%
19.2%
99.4%
‐
25,453
6.4%
100%
Latest
Page 13
Page 13
Page 13
Page 14
Page 14
Page 15
Page 15
Page 16
Page 16
Page 17
KPI‐363 ‐ Compliments
KPI‐364 ‐ Complaints
FFT ‐ Friends and Family Test
SFFT ‐ Staff that would recomment employment
KPI
‐
‐
85%
‐
Target
57
27
90.5%
‐
Latest
Page 11
Page 11
Page 12
Page 12
KPI‐186 ‐ Accommodation Status
KPI‐187 ‐ Employment Status
KPI‐029 ‐ Gatekeeping
KPI‐399 ‐ CPA Reviews ﴾12 Months﴿
KPI‐452 ‐ EIP Engagement within 2 Weeks
KPI‐453 ‐ Effectiveness of EIP pathway
KPI‐348 ‐ IAPT Recovery Rate
KPI‐374 ‐ IAPT Access Rate
KPI‐434 ‐ IAPT: Treated within 6 weeks
KPI‐435 ‐ IAPT: Treated within 18 weeks
KPI‐416 ‐ Seclusion Incidents
KPI‐427 ‐ Incidents of Restraint
KPI
‐
‐
95%
95%
50%
‐
50%
14.2%
75%
95%
‐
‐
Target
63.7%
6.1%
98.0%
93.2%
42.1%
42.8%
55.5%
12.8%
92.3%
100.0%
31
62
Latest
Page 5
Page 5
Page 6
Page 6
Page 7
Page 7
Page 8
Page 8
Page 9
Page 9
Page 10
Page 10
KPI‐308 ‐ Compulsory Training
KPI‐238 ‐ Supervision in Date
KPI‐239 ‐ Appraisal In Date
KPI‐211 ‐ Sickness Absence
KPI‐414 ‐ Shifts Filled NHS Professionals Against Perm Staff
Fin01 ‐ Capital Expenditure and Disposals ﴾Forecast﴿
Fin02 ‐ Sustainability Risk Ratings YTD
Fin03 ‐ Cash Balance ﴾Current﴿
Fin04 ‐ Cost Improvement Plan Forecast
Fin05 ‐ Performance Against Budget
Fin06 ‐ Pre‐impairment Surplus Performance YTD
Fin07 ‐ Agency Spend YTD
Fin08 ‐ Month by Month Agency Spend
Fin09 ‐ Non‐Framework Agency % ﴾in‐month﴿
Fin10 ‐ Agency Cap ﴾Forecast﴿
Fin11 ‐ Medical Agency Reduction
KPI‐386 ‐ Governance Risk Rating ﴾Monitor﴿
KPI‐165 ‐ Monitor Rating for Finance
CQUIN ‐ CQUIN 2017/18
CCGReq ‐ CCG Contractual Quality Requirements
KPI
90%
90%
90%
5%
‐
£11,447k
1
£16,515k
£8,680k
‐
£2,671k
£2,963k
£296k
0%
£4,056k
£965k
5
1
‐
‐
Target
92.1%
79.1%
78.0%
6.6%
‐
£10,166k
1
£27,069k
£7,852k
‐
£2,671k
£2,787k
£267k
15.7%
£3,383k
£755k
5
1
‐
‐
Latest
Page 18
Page 18
Page 18
Page 19
Page 19
Page 20
Page 20
Page 21
Page 21
Page 22
Page 22
Page 23
Page 23
Page 24
Page 24
Page 25
Page 26
Page 26
Page 26
Page 26
Responsive
Caring
Effective
Well
Safe KPI‐010 ‐ 7 Day Follow Up
KPI‐279 ‐ 48hr Follow Up
KPI‐454 ‐ Meds Reconcilliation in 72hrs
KPI‐446 ‐ Falls
KPI
95%
95%
95%
‐
Target
100.0%
81.3%
92.5%
31
Latest
Page 3
Page 3
Page 4
Page 4
Led
2 of 26
4.1
Inte
grat
edP
erfo
rman
ce a
nd
Page 34 of 96

Safe
Feb‐2017 Mar‐2017 Apr‐2017 May‐2017 Jun‐2017 Jul‐2017 Aug‐2017 Sep‐2017 Oct‐2017 Nov‐2017 Dec‐2017 Jan‐201850 %
60 %
70 %
80 %
90 %
100 %
110 %
Numerator
Denominator
Difference
7 19 12 17 17 11 10 8 13 11 10 13
8 22 13 18 19 11 11 9 13 11 10 13
1 3 1 1 2 0 1 1 0 0 0 0
Feb‐17 Mar‐17 Apr‐17 May‐17 Jun‐17 Jul‐17 Aug‐17 Sep‐17 Oct‐17 Nov‐17 Dec‐17 Jan‐18
KPI‐010 ‐ 7 Day Follow Up
Feb‐2017 Mar‐2017 Apr‐2017 May‐2017 Jun‐2017 Jul‐2017 Aug‐2017 Sep‐2017 Oct‐2017 Nov‐2017 Dec‐2017 Jan‐201850 %
60 %
70 %
80 %
90 %
100 %
Numerator
Denominator
Difference
51 53 40 48 47 45 70 49 52 44 42 53
57 61 52 57 53 53 75 61 55 56 49 65
6 8 12 9 6 8 5 12 3 12 7 12
Feb‐17 Mar‐17 Apr‐17 May‐17 Jun‐17 Jul‐17 Aug‐17 Sep‐17 Oct‐17 Nov‐17 Dec‐17 Jan‐18
KPI‐279 ‐ 48hr Follow Up
Current Year
Target
Previous Year
Current Year
Target
Previous Year
Operational Commentary
Operational CommentaryThere were 12 patients not followed up within the timescales forthe following reasons: ‐ 4 people were not contacted on time due to communicationissues within the teams. Successful contacts were achieved for
both clients after the deadline and within 7 days. ‐ 4 people, third party contact was achieved confirming theirsafety. ‐ 2 people were not contacted on time because they did notanswer their phones. Successful contact was achieved for all theclients after the deadline, confirming their safety. ‐ 2 people were seen on the day of the deadline but slightly late.
3 of 26
4.1
Inte
grat
edP
erfo
rman
ce a
nd
Page 35 of 96

Safe
Feb‐2017 Mar‐2017 Apr‐2017 May‐2017 Jun‐2017 Jul‐2017 Aug‐2017 Sep‐2017 Oct‐2017 Nov‐2017 Dec‐2017 Jan‐201850 %
60 %
70 %
80 %
90 %
100 %
Denominator
Numerator
Difference
84 118 101 108 104 97 105 106 115 95 100 93
77 111 88 98 94 93 99 97 109 93 91 86
7 7 13 10 10 4 6 9 6 2 9 7
Feb‐17 Mar‐17 Apr‐17 May‐17 Jun‐17 Jul‐17 Aug‐17 Sep‐17 Oct‐17 Nov‐17 Dec‐17 Jan‐18
KPI‐454 ‐ Meds Reconcilliation in 72hrs Current Year
Target
Previous Year
Total
Median
UCL
LCL
Operational Commentary
Operational Commentary
Feb‐2017 Mar‐2017 Apr‐2017 May‐2017 Jun‐2017 Jul‐2017 Aug‐2017 Sep‐2017 Oct‐2017 Nov‐2017 Dec‐2017 Jan‐20180
10
20
30
40
50
0 ‐ Near Miss1 ‐ No Harm2 ‐ Minor3 ‐ Moderate4 ‐ Major5 ‐ Catastrophic6 ‐ Expected Death
0 0 0 1 0 0 0 2 0 1 0 010 9 9 11 10 7 16 20 11 11 16 1315 16 5 6 11 20 13 21 17 10 16 161 0 0 1 1 0 1 1 2 0 2 20 0 0 0 0 0 0 0 0 0 0 00 0 0 0 0 0 0 0 0 0 0 00 0 0 0 0 0 0 0 0 0 0 0
Feb‐17 Mar‐17 Apr‐17 May‐17 Jun‐17 Jul‐17 Aug‐17 Sep‐17 Oct‐17 Nov‐17 Dec‐17 Jan‐18
KPI‐446 ‐ Falls
7 cases breached the 72 hour target timescale, all cases werehighlighted with the relevant directorates at the DirectorateGovernance Board meetings.
4 of 26
4.1
Inte
grat
edP
erfo
rman
ce a
nd
Page 36 of 96
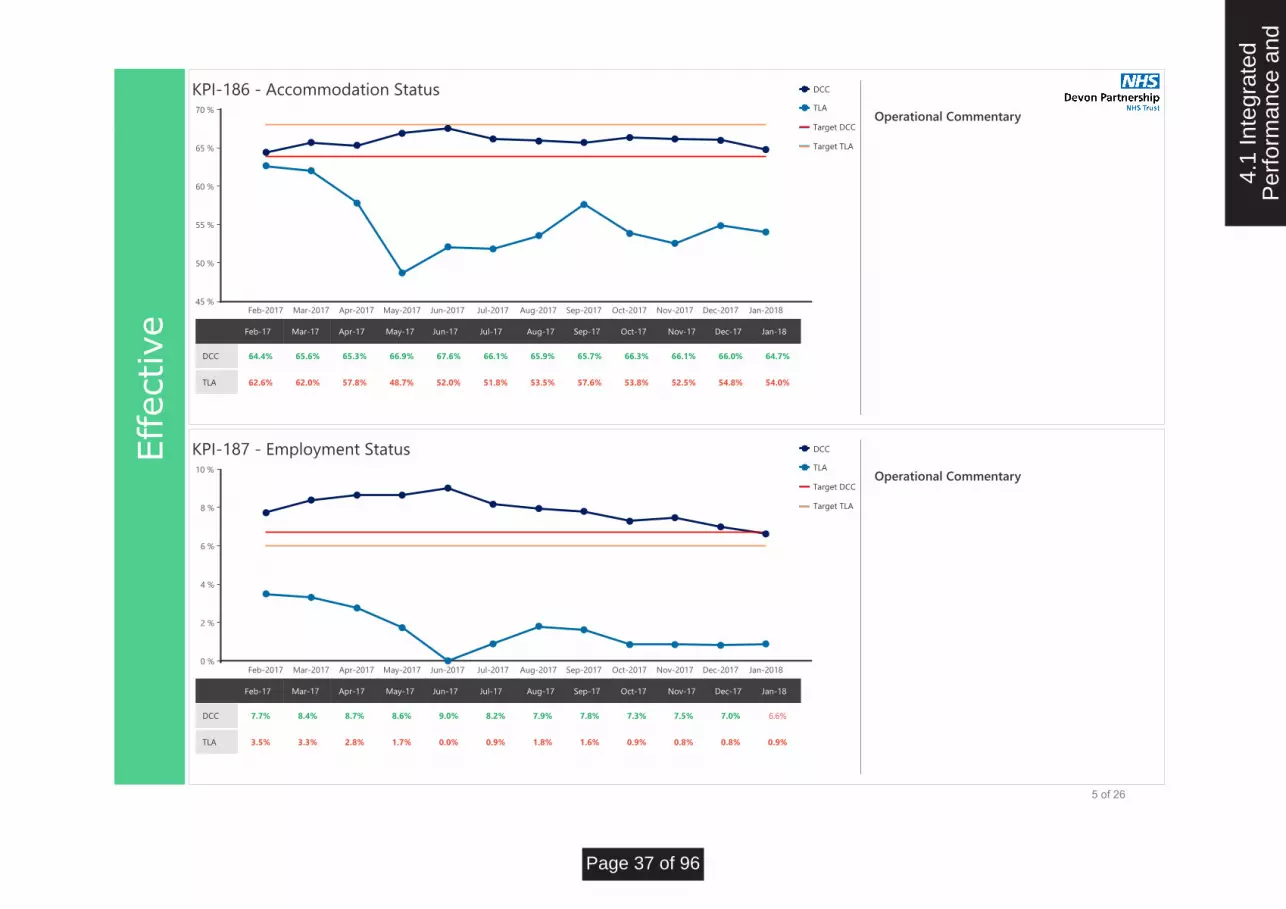
Effective
Feb‐2017 Mar‐2017 Apr‐2017 May‐2017 Jun‐2017 Jul‐2017 Aug‐2017 Sep‐2017 Oct‐2017 Nov‐2017 Dec‐2017 Jan‐201845 %
50 %
55 %
60 %
65 %
70 %
DCC 64.4% 65.6% 65.3% 66.9% 67.6% 66.1% 65.9% 65.7% 66.3% 66.1% 66.0% 64.7%
Feb‐17 Mar‐17 Apr‐17 May‐17 Jun‐17 Jul‐17 Aug‐17 Sep‐17 Oct‐17 Nov‐17 Dec‐17 Jan‐18
KPI‐186 ‐ Accommodation Status
KPI‐187 ‐ Employment Status
DCC
TLA
Target DCC
Target TLA
DCC
TLA
Target DCC
Target TLA
Operational Commentary
Operational Commentary
Feb‐2017 Mar‐2017 Apr‐2017 May‐2017 Jun‐2017 Jul‐2017 Aug‐2017 Sep‐2017 Oct‐2017 Nov‐2017 Dec‐2017 Jan‐20180 %
2 %
4 %
6 %
8 %
10 %
DCC 7.7% 8.4% 8.7% 8.6% 9.0% 8.2% 7.9% 7.8% 7.3% 7.5% 7.0% 6.6%
Feb‐17 Mar‐17 Apr‐17 May‐17 Jun‐17 Jul‐17 Aug‐17 Sep‐17 Oct‐17 Nov‐17 Dec‐17 Jan‐18
TLA 62.6% 62.0% 57.8% 48.7% 52.0% 51.8% 53.5% 57.6% 53.8% 52.5% 54.8% 54.0%
TLA 3.5% 3.3% 2.8% 1.7% 0.0% 0.9% 1.8% 1.6% 0.9% 0.8% 0.8% 0.9%
5 of 26
4.1
Inte
grat
edP
erfo
rman
ce a
nd
Page 37 of 96

Effective
Feb‐2017 Mar‐2017 Apr‐2017 May‐2017 Jun‐2017 Jul‐2017 Aug‐2017 Sep‐2017 Oct‐2017 Nov‐2017 Dec‐2017 Jan‐201880 %
85 %
90 %
95 %
100 %
105 %
Numerator
Denominator
Difference
33 50 49 54 48 46 62 54 55 43 47 48
35 50 50 54 48 48 63 56 55 43 48 49
2 0 1 0 0 2 1 2 0 0 1 1
Feb‐17 Mar‐17 Apr‐17 May‐17 Jun‐17 Jul‐17 Aug‐17 Sep‐17 Oct‐17 Nov‐17 Dec‐17 Jan‐18
KPI‐029 ‐ Gatekeeping
Feb‐2017 Mar‐2017 Apr‐2017 May‐2017 Jun‐2017 Jul‐2017 Aug‐2017 Sep‐2017 Oct‐2017 Nov‐2017 Dec‐2017 Jan‐201875 %
80 %
85 %
90 %
95 %
100 %
Numerator
Denominator
Difference
717 728 742 749 741 742 744 788 803 805 800 771
787 804 828 838 829 822 821 852 864 876 877 827
70 76 86 89 88 80 77 64 61 71 77 56
Feb‐17 Mar‐17 Apr‐17 May‐17 Jun‐17 Jul‐17 Aug‐17 Sep‐17 Oct‐17 Nov‐17 Dec‐17 Jan‐18
KPI‐399 ‐ CPA Reviews ﴾12 Months﴿
Current Year
Target
Previous Year
Current Year
Target
Previous Year
Operational Commentary
Operational CommentaryCPA Reviews – Daily reporting is in place via Informatics Hub,directorate analysts are highlighting cases that are coming up for review with therelevant team managers. The Trust aims to achieve the 95%target by the end of March 2018.
6 of 26
4.1
Inte
grat
edP
erfo
rman
ce a
nd
Page 38 of 96

Effective
Feb‐2017 Mar‐2017 Apr‐2017 May‐2017 Jun‐2017 Jul‐2017 Aug‐2017 Sep‐2017 Oct‐2017 Nov‐2017 Dec‐2017 Jan‐20180 %
20 %
40 %
60 %
80 %
100 %
Numerator
Denominator
Difference
10 16 5 17 17 20 12 18 10 19 10 8
15 25 10 24 19 24 19 24 16 28 15 19
5 9 5 7 2 4 7 6 6 9 5 11
Feb‐17 Mar‐17 Apr‐17 May‐17 Jun‐17 Jul‐17 Aug‐17 Sep‐17 Oct‐17 Nov‐17 Dec‐17 Jan‐18
KPI‐452 ‐ EIP Engagement within 2 Weeks
Feb‐2017 Mar‐2017 Apr‐2017 May‐2017 Jun‐2017 Jul‐2017 Aug‐2017 Sep‐2017 Oct‐2017 Nov‐2017 Dec‐2017 Jan‐20180 %
10 %
20 %
30 %
40 %
50 %
60 %
70 %
80 %
Numerator
Denominator
Difference
252 234 108 117 168 158 167 173 169 127 107 125
550 581 189 200 217 224 233 247 263 277 283 292
298 347 81 83 49 66 66 74 94 150 176 167
Feb‐17 Mar‐17 Apr‐17 May‐17 Jun‐17 Jul‐17 Aug‐17 Sep‐17 Oct‐17 Nov‐17 Dec‐17 Jan‐18
KPI‐453 ‐ Effectiveness of EIP pathway
Current Year
Target
Previous Year
Current Year
Previous Year
Operational Commentary
Operational Commentary
8 out of the 19 clients experiencing first episode psychosis wereallocated to and engaged with an EIP Care Coordinator within 2weeks of referrals being received. 11 clients where not engagedwithin the required timescale because some were out of areahospital admissions that we were unable to see in the timeframe. We also had some DNA'd appointments due to Christmasand we also had trouble organising joint appointments withCAMHS.
7 of 26
4.1
Inte
grat
edP
erfo
rman
ce a
nd
Page 39 of 96

Effective
Feb‐2017 Mar‐2017 Apr‐2017 May‐2017 Jun‐2017 Jul‐2017 Aug‐2017 Sep‐2017 Oct‐2017 Nov‐2017 Dec‐2017 Jan‐201840 %
45 %
50 %
55 %
60 %
Numerator
Denominator
Difference
360 480 306 370 399 352 399 422 358 429 272 522
685 907 591 744 732 687 749 753 714 796 610 941
325 427 285 374 333 335 350 331 356 367 338 419
Feb‐17 Mar‐17 Apr‐17 May‐17 Jun‐17 Jul‐17 Aug‐17 Sep‐17 Oct‐17 Nov‐17 Dec‐17 Jan‐18
KPI‐348 ‐ IAPT Recovery Rate
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar0 %
2 %
4 %
6 %
8 %
10 %
12 %
14 %
16 %
Numerator
Denominator
Difference
883 2,094 3,361 4,657 5,935 7,156 8,619 10,366 11,557 12,974
101,466 101,466 101,466 101,466 101,466 101,466 101,466 101,466 101,466 101,466
100,583 99,372 98,105 96,809 95,531 94,310 92,847 91,100 89,909 88,492
Apr‐17 May‐17 Jun‐17 Jul‐17 Aug‐17 Sep‐17 Oct‐17 Nov‐17 Dec‐17 Jan‐18
KPI‐374 ‐ IAPT Access Rate
Current Year
Target
Previous Year
Previous Year
Current Year
Target
Operational Commentary
Operational CommentaryNew Devon CCG area access rate within January was 1.35%, asignificant increase on the Dec access. The numbers entering treatment within the Long TermConditions team remain below the 170 needed to entertreatment.
This has been discussed within the IAPT Board meeting with theand likely to increase significantly when we can accept referralsoutside of the 3 main areas identified within the bid and implementation of obesity,COPD and diabetes. With agreement from NHSE we haveexpanded into the pain pathway, and following the end of March we will expand into all LTCswithin primary care and move into other specialist pathways within acute physical healthcare.South Devon & Torbay CCG area remains above the year to datetrajectory to meet 15%.
8 of 26
4.1
Inte
grat
edP
erfo
rman
ce a
nd
Page 40 of 96

Effective
Feb‐2017 Mar‐2017 Apr‐2017 May‐2017 Jun‐2017 Jul‐2017 Aug‐2017 Sep‐2017 Oct‐2017 Nov‐2017 Dec‐2017 Jan‐201860 %
65 %
70 %
75 %
80 %
85 %
90 %
95 %
100 %
Numerator
Denominator
Difference
707 938 626 756 754 696 734 730 699 826 589 916
730 957 636 783 783 732 796 801 759 913 643 992
23 19 10 27 29 36 62 71 60 87 54 76
Feb‐17 Mar‐17 Apr‐17 May‐17 Jun‐17 Jul‐17 Aug‐17 Sep‐17 Oct‐17 Nov‐17 Dec‐17 Jan‐18
KPI‐434 ‐ IAPT: Treated within 6 weeks
Feb‐2017 Mar‐2017 Apr‐2017 May‐2017 Jun‐2017 Jul‐2017 Aug‐2017 Sep‐2017 Oct‐2017 Nov‐2017 Dec‐2017 Jan‐201880 %
85 %
90 %
95 %
100 %
105 %
Numerator
Denominator
Difference
729 957 636 783 782 732 796 801 759 912 643 992
730 957 636 783 783 732 796 801 759 913 643 992
1 0 0 0 1 0 0 0 0 1 0 0
Feb‐17 Mar‐17 Apr‐17 May‐17 Jun‐17 Jul‐17 Aug‐17 Sep‐17 Oct‐17 Nov‐17 Dec‐17 Jan‐18
KPI‐435 ‐ IAPT: Treated within 18 weeks
Current Year
Target
Previous Year
Current Year
Target
Previous Year
Operational Commentary
Operational Commentary
9 of 26
4.1
Inte
grat
edP
erfo
rman
ce a
nd
Page 41 of 96

Effective
Feb‐2017 Mar‐2017 Apr‐2017 May‐2017 Jun‐2017 Jul‐2017 Aug‐2017 Sep‐2017 Oct‐2017 Nov‐2017 Dec‐2017 Jan‐20180
10
20
30
40
50
60
Numerator 16 17 9 8 8 13 36 27 31 30 44 31
Feb‐17 Mar‐17 Apr‐17 May‐17 Jun‐17 Jul‐17 Aug‐17 Sep‐17 Oct‐17 Nov‐17 Dec‐17 Jan‐18
KPI‐416 ‐ Seclusion Incidents
Feb‐2017 Mar‐2017 Apr‐2017 May‐2017 Jun‐2017 Jul‐2017 Aug‐2017 Sep‐2017 Oct‐2017 Nov‐2017 Dec‐2017 Jan‐20180
20
40
60
80
100
120
Numerator 40 36 28 17 46 56 60 83 50 48 87 62
Feb‐17 Mar‐17 Apr‐17 May‐17 Jun‐17 Jul‐17 Aug‐17 Sep‐17 Oct‐17 Nov‐17 Dec‐17 Jan‐18
KPI‐427 ‐ Incidents of Restraint
Current Year
Median
Upper Control
Lower Control
Current Year
Median
Upper Control
Lower Control
Operational Commentary
Operational Commentary
10 of 26
4.1
Inte
grat
edP
erfo
rman
ce a
nd
Page 42 of 96

Caring
Feb‐2017 Mar‐2017 Apr‐2017 May‐2017 Jun‐2017 Jul‐2017 Aug‐2017 Sep‐2017 Oct‐2017 Nov‐2017 Dec‐2017 Jan‐20180
20
40
60
80
100
Numerator 43 62 38 44 26 30 69 29 65 87 38 57
Feb‐17 Mar‐17 Apr‐17 May‐17 Jun‐17 Jul‐17 Aug‐17 Sep‐17 Oct‐17 Nov‐17 Dec‐17 Jan‐18
KPI‐363 ‐ Compliments
Feb‐2017 Mar‐2017 Apr‐2017 May‐2017 Jun‐2017 Jul‐2017 Aug‐2017 Sep‐2017 Oct‐2017 Nov‐2017 Dec‐2017 Jan‐20180
5
10
15
20
25
30
35
Numerator 24 27 20 23 22 23 27 17 22 20 12 27
Feb‐17 Mar‐17 Apr‐17 May‐17 Jun‐17 Jul‐17 Aug‐17 Sep‐17 Oct‐17 Nov‐17 Dec‐17 Jan‐18
KPI‐364 ‐ Complaints
Current Year
Previous Year
Current Year
Previous Year
Operational Commentary
Operational Commentary
11 of 26
4.1
Inte
grat
edP
erfo
rman
ce a
nd
Page 43 of 96

Caring
Feb‐2017 Mar‐2017 May‐2017 Jun‐2017 Jul‐2017 Aug‐2017 Sep‐2017 Oct‐2017 Nov‐2017 Dec‐2017 Jan‐201875 %
80 %
85 %
90 %
95 %
100 %
1 ‐ Extremely Likely2 ‐ Likely3 ‐ Neither4 ‐ Unlikely5 ‐ Extremely Unlikely6 ‐ Don't Know
162 95 246 152 231 300 182 208 352 559 28656 17 76 38 61 89 69 91 118 233 1416 1 7 5 11 8 14 9 19 41 182 0 6 4 6 3 3 7 12 10 93 4 4 5 9 8 5 6 4 11 71 4 5 6 4 9 2 10 6 30 11
Feb‐17 Mar‐17 May‐17 Jun‐17 Jul‐17 Aug‐17 Sep‐17 Oct‐17 Nov‐17 Dec‐17 Jan‐18
Mar‐2017 Jun‐2017 Sep‐201760 %
65 %
70 %
75 %
80 %
1 ‐ Extremely Likely2 ‐ Likely3 ‐ Neither likely nor unlikely4 ‐ Unlikely5 ‐ Extremely unlikely6 ‐ Don't Know
72 181 150117 266 27430 66 10510 53 4311 19 222 11 7
Mar‐17 Jun‐17 Sep‐17Recommend Treatment
Current Year
Previous Year
Target
Recommend Employment
Recommend Treatment
Operational Commentary
Operational Commentary
Staff FFT ‐ Would Recommend
1 ‐ Extremely Likely2 ‐ Likely3 ‐ Neither likely nor unlikely4 ‐ Unlikely5 ‐ Extremely unlikely6 ‐ Don't Know
68 157 12498 234 24731 87 10425 62 6620 54 590 2 1
Mar‐17 Jun‐17 Sep‐17Recommend Employment
FTT ‐ Would Recommend
12 of 26
4.1
Inte
grat
edP
erfo
rman
ce a
nd
Page 44 of 96

Responsive Feb‐2017 Mar‐2017 Apr‐2017 May‐2017 Jun‐2017 Jul‐2017 Aug‐2017 Sep‐2017 Oct‐2017 Nov‐2017 Dec‐2017 Jan‐2018
0
200
400
600
800
1,000
1,200
1,400
Numerator
Denominator
Percent
1,159 1,212 970 915 808 743 663 729 758 835 346 208
7,908 8,807 8,466 8,883 8,544 8,793 8,739 8,328 8,613 8,482 8,415 8,851
14.7% 13.8% 11.5% 10.3% 9.5% 8.4% 7.6% 8.8% 8.8% 9.8% 4.1% 2.4%
Feb‐17 Mar‐17 Apr‐17 May‐17 Jun‐17 Jul‐17 Aug‐17 Sep‐17 Oct‐17 Nov‐17 Dec‐17 Jan‐18
KPI‐253 ‐ Delayed Discharges
Feb‐2017 Mar‐2017 Apr‐2017 May‐2017 Jun‐2017 Jul‐2017 Aug‐2017 Sep‐2017 Oct‐2017 Nov‐2017 Dec‐2017 Jan‐20180
10
20
30
40
50
PICU 13 16 13 10 15 8 11 14 14 9 9 11
Feb‐17 Mar‐17 Apr‐17 May‐17 Jun‐17 Jul‐17 Aug‐17 Sep‐17 Oct‐17 Nov‐17 Dec‐17 Jan‐18
Trust
Adult
OPMH
Forensic
Specialist
PICU
Out of Area
Operational Commentary
Operational Commentary
Out of Area 14 17 11 23 12 20 23 28 23 17 22 40
PICU & Out of Area
13 of 26
4.1
Inte
grat
edP
erfo
rman
ce a
nd
Page 45 of 96

Responsive Feb‐2017 Mar‐2017 Apr‐2017 May‐2017 Jun‐2017 Jul‐2017 Aug‐2017 Sep‐2017 Oct‐2017 Nov‐2017 Dec‐2017 Jan‐2018
0 %
20 %
40 %
60 %
80 %
100 %
Numerator
Denominator
Percent
328 201 193 230 285 285 259 299 340 400 266 385
552 523 516 547 530 522 564 576 548 625 467 633
59.4% 38.4% 37.4% 42.0% 53.8% 54.6% 45.9% 51.9% 62.0% 64.0% 57.0% 60.8%
Feb‐17 Mar‐17 Apr‐17 May‐17 Jun‐17 Jul‐17 Aug‐17 Sep‐17 Oct‐17 Nov‐17 Dec‐17 Jan‐18
KPI‐305 ‐ Routine Referrals ﴾10 Days﴿
KPI‐306 ‐ Urgent Referrals ﴾5 Days﴿
Trust
Adult
OPMH
Target
Trust
Adult
OPMH
Target
Operational Commentary
Operational Commentary
Feb‐2017 Mar‐2017 Apr‐2017 May‐2017 Jun‐2017 Jul‐2017 Aug‐2017 Sep‐2017 Oct‐2017 Nov‐2017 Dec‐2017 Jan‐20180 %
20 %
40 %
60 %
80 %
100 %
120 %
Numerator
Denominator
Percent
22 39 29 39 28 41 29 40 48 49 38 5
44 79 55 70 49 77 53 61 64 68 45 26
50.0% 49.4% 52.7% 55.7% 57.1% 53.2% 54.7% 65.6% 75.0% 72.1% 84.4% 19.2%
Feb‐17 Mar‐17 Apr‐17 May‐17 Jun‐17 Jul‐17 Aug‐17 Sep‐17 Oct‐17 Nov‐17 Dec‐17 Jan‐18
We have seen a significant increase in referrals, which impactedon waiting times in January. We have also noticed an increase inDNA’s which means that we then have to rebook and useanother assessment slot so often 2 assessment slots are beingused for one patient. A safeguard is in place where by the CTM/Practice lead willundertake phone triage for all urgent referrals not seen with 5working days and all routine referrals not seen within 20 workingdays. If clinically indicated the appointment will be broughtforward. If the person cannot be contacted a standard letter willbe sent confirming their appointment and advising ofinterim/out of hours options and advising they can contact theMHAT team if required.
Out of the 26 urgent referrals received in January, 5 of them wasoffered appointments within 5 working days. The remaining 21clients missed the target because there were no appointmentsavailable to offer within the 5 working days timescale due tocurrent staffing capacity. All the 21 clients had attended
appointments outside the 5 working day timescale. In all cases,checks were made to ensure the safety and wellbeing of clients.
14 of 26
4.1
Inte
grat
edP
erfo
rman
ce a
nd
Page 46 of 96

Responsive Feb‐2017 Mar‐2017 Apr‐2017 May‐2017 Jun‐2017 Jul‐2017 Aug‐2017 Sep‐2017 Oct‐2017 Nov‐2017 Dec‐2017 Jan‐2018
70 %
80 %
90 %
100 %
110 %
120 %
Trust
Adult
OPMH
Secure
Specialist
101.8% 99.4% 96.8% 99.4% 98.1% 98.1% 97.6% 93.7% 104.1% 100.2% 94.1% 99.4%
110.0% 104.6% 103.3% 107.9% 103.4% 99.0% 97.0% 88.6% 118.9% 106.3% 96.6% 110.7%
100.1% 96.2% 89.9% 91.4% 87.9% 96.3% 98.2% 98.9% 97.4% 95.0% 89.0% 93.3%
99.3% 99.2% 97.4% 98.1% 99.3% 99.1% 98.8% 99.1% 98.6% 99.7% 95.6% 97.8%
77.5% 81.4% 79.6% 87.1% 94.9% 92.4% 91.8% 70.2% 78.9% 87.6% 87.5% 85.2%
Feb‐17 Mar‐17 Apr‐17 May‐17 Jun‐17 Jul‐17 Aug‐17 Sep‐17 Oct‐17 Nov‐17 Dec‐17 Jan‐18
Bed Occupancy
Feb‐2017 Mar‐2017 Apr‐2017 May‐2017 Jun‐2017 Jul‐2017 Aug‐2017 Sep‐2017 Oct‐2017 Nov‐2017 Dec‐2017 Jan‐20180
100
200
300
400
500
Adult Mental Illness
Eating Disorders
Learning Disability
Old Age Psychiatry
Rehabilitation
32 33 33 34 35 36 35 34 32 32 33 33
74 72 69 67 67 76 77 83 82 81 77 77
331 331 335 335 387 459 311 311 311 286 286 186
62 61 61 60 62 66 63 63 62 63 60 59
342 292 286 239 249 237 236 225 190 176 160 136
Feb‐17 Mar‐17 Apr‐17 May‐17 Jun‐17 Jul‐17 Aug‐17 Sep‐17 Oct‐17 Nov‐17 Dec‐17 Jan‐18
Length of Stay
Trust
Adult
OPMH
Secure
Specialist
Adult Mental Illness
Eating Disorders
Learning Disability
Old Age Psychiatry
Rehabilitation
Operational Commentary
Operational Commentary
15 of 26
4.1
Inte
grat
edP
erfo
rman
ce a
nd
Page 47 of 96

Responsive Feb‐2017 Mar‐2017 Apr‐2017 May‐2017 Jun‐2017 Jul‐2017 Aug‐2017 Sep‐2017 Oct‐2017 Nov‐2017 Dec‐2017 Jan‐2018
18K
20K
22K
24K
26K
28K
30K
Numerator 22,179 25,051 20,449 24,492 24,051 23,456 23,581 23,127 25,291 26,270 19,744 25,453
Feb‐17 Mar‐17 Apr‐17 May‐17 Jun‐17 Jul‐17 Aug‐17 Sep‐17 Oct‐17 Nov‐17 Dec‐17 Jan‐18
Contacts
Feb‐2017 Mar‐2017 Apr‐2017 May‐2017 Jun‐2017 Jul‐2017 Aug‐2017 Sep‐2017 Oct‐2017 Nov‐2017 Dec‐2017 Jan‐20185 %
5.5 %
6 %
6.5 %
7 %
7.5 %
Total 6.1% 6.6% 6.9% 6.4% 6.9% 6.4% 6.8% 5.7% 6.3% 6.0% 6.7% 6.4%
Feb‐17 Mar‐17 Apr‐17 May‐17 Jun‐17 Jul‐17 Aug‐17 Sep‐17 Oct‐17 Nov‐17 Dec‐17 Jan‐18
DNAs
Contacts
Median
Upper Control
Lower Control
DNAs
Median
Upper Control
Lower Control
Operational Commentary
Operational Commentary
16 of 26
4.1
Inte
grat
edP
erfo
rman
ce a
nd
Page 48 of 96

Responsive Feb‐2017 Mar‐2017 Apr‐2017 May‐2017 Jun‐2017 Jul‐2017 Aug‐2017 Sep‐2017 Oct‐2017 Nov‐2017 Dec‐2017 Jan‐2018
92 %
94 %
96 %
98 %
100 %
102 %
Total 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0%
Feb‐17 Mar‐17 Apr‐17 May‐17 Jun‐17 Jul‐17 Aug‐17 Sep‐17 Oct‐17 Nov‐17 Dec‐17 Jan‐18
KPI‐177 ‐ LD Access to Care Current Year
Operational Commentary
17 of 26
4.1
Inte
grat
edP
erfo
rman
ce a
nd
Page 49 of 96

Well
Feb‐2017 Mar‐2017 Apr‐2017 May‐2017 Jun‐2017 Jul‐2017 Aug‐2017 Sep‐2017 Oct‐2017 Nov‐2017 Dec‐2017 Jan‐201889 %
90 %
91 %
92 %
93 %
94 %
95 %
96 %
Total 95.1% 95.2% 93.6% 94.6% 94.2% 93.8% 94.4% 93.8% 93.6% 93.3% 93.0% 92.1%
Feb‐17 Mar‐17 Apr‐17 May‐17 Jun‐17 Jul‐17 Aug‐17 Sep‐17 Oct‐17 Nov‐17 Dec‐17 Jan‐18
KPI‐308 ‐ Compulsory Training
Feb‐2017 Mar‐2017 Apr‐2017 May‐2017 Jun‐2017 Jul‐2017 Aug‐2017 Sep‐2017 Oct‐2017 Nov‐2017 Dec‐2017 Jan‐201870 %
75 %
80 %
85 %
90 %
95 %
Supervision 85.5% 82.1% 79.6% 80.9% 84.2% 85.2% 82.0% 77.0% 79.1% 84.5% 79.5% 79.1%
Feb‐17 Mar‐17 Apr‐17 May‐17 Jun‐17 Jul‐17 Aug‐17 Sep‐17 Oct‐17 Nov‐17 Dec‐17 Jan‐18
Trust
Target
Supervision
Target
Appraisal
Operational Commentary
Operational Commentary
Appraisal 84.0% 82.6% 77.9% 78.9% 79.3% 79.7% 78.7% 76.3% 74.6% 72.7% 75.8% 78.0%
Weekly monitoring report is available via the Informatics Hub,the supervision recording system also provides a real timesnapshot of status. Managers are reminded by the HR BusinessPartners and Analysts to continue monitoring progress, some ofthe underreporting is due to the late recording of events which
has been raised and highlighted with the teams, and actionplans are presented at the Directorate Governance Board andTrust Performance Meetings.
Led
KPI‐238 ‐ Supervision in Date and KPI‐239 ‐ Appraisal in Date
18 of 26
4.1
Inte
grat
edP
erfo
rman
ce a
nd
Page 50 of 96

Well
Feb‐2017 Mar‐2017 Apr‐2017 May‐2017 Jun‐2017 Jul‐2017 Aug‐2017 Sep‐2017 Oct‐2017 Nov‐2017 Dec‐2017 Jan‐20180.0 %
1.0 %
2.0 %
3.0 %
4.0 %
5.0 %
6.0 %
7.0 %
Total 4.2% 4.2% 4.3% 3.6% 4.4% 4.7% 4.5% 4.2% 4.6% 5.3% 5.4% 6.6%
Feb‐17 Mar‐17 Apr‐17 May‐17 Jun‐17 Jul‐17 Aug‐17 Sep‐17 Oct‐17 Nov‐17 Dec‐17 Jan‐18
KPI‐211 ‐ Sickness Absence
Jun‐2017 Jul‐2017 Aug‐2017 Sep‐2017 Oct‐2017 Nov‐2017 Dec‐20170 %
5 %
10 %
15 %
20 %
25 %
30 %
35 %
Total 26.3% 26.3% 28.4% 32.7% 24.0% 26.9% 22.6%
Jun‐17 Jul‐17 Aug‐17 Sep‐17 Oct‐17 Nov‐17 Dec‐17
KPI‐414 ‐ Shifts Filled NHS Professionals Against Perm Staff
Trust
Target
Median
Upper Control
Lower Control
Current Year
Previous Year
Operational Commentary
Operational Commentary
The figure has improved since last month, all directorates areworking closely with HR Business Partners to ensure accuratereporting and action plan to address sickness absence relatedissues.
Led
19 of 26
4.1
Inte
grat
edP
erfo
rman
ce a
nd
Page 51 of 96

Well
Capex 2017/18
Disposals ﴾NBV﴿ 2017/18
CRL
14,756 11,447 10,165 ‐1,282 5,194 4,488 ‐706
5,030 0 0 0 0 0 0
9,726 11,447 10,165 ‐1,282 5,194 4,488 ‐706
NHSi Plan Full‐Year
Revised Plan Full‐Year ﴾Internal﴿
Forecast Outturn Variance Revised Profile Spend
Actual Spend YTD
Actual variance
Capital Service Capacity Liquidity I&E measure I&E margin variance Agency Spend Overall rating0
0.5
1
1.5
2
2.5
Plan Rating
Operational Commentary
Operational Commentary
Capital Expenditure and Disposals
Sustainable Risk Ratings ﴾YTD﴿
YTD capital expenditure at M10 was £4.5m. This is behind therevised plan by £0.7m. The Trust has agreed with NHSi it can slip >£1m capitalexpenditure between 2017/18 and 2018/19 and is now reportingforecast expenditure of £10.2m. Due to the spend required inM11 and M12, reporting will be increased to weekly from theend of M11. A revised allocation of £191k for Place of Safety works has nowbeen agreed for work to commence in early Feb and completionin March. The forecast also includes an allocation for MBUenabling works.
At M10 the Trust achieved an overall rating of 1 ﴾highestachievable﴿ shown in the chart which is in line with plan. TheTrust is more prudent with its calculation of Capital ServiceCapacity compared to NHSI, recognising a cost each month forthe loan repayment, whilst NHSi only reflect this in the months
of September and March when loan repayment occurs. The variance in liquidity is due to the cash balances beingsignificantly higher than plan, as explained in the cash section. The Trust is forecasting an overall rating of 1 for the end of thefinancial year.
Led
20 of 26
4.1
Inte
grat
edP
erfo
rman
ce a
nd
Page 52 of 96

Well
Feb‐2016Mar‐2016Apr‐2016May‐2016Jun‐2016Jul‐2016Aug‐2016Sep‐2016Oct‐2016Nov‐2016Dec‐2016Jan‐2017Feb‐2017Mar‐2017Apr‐2017May‐2017Jun‐2017Jul‐2017Aug‐2017Sep‐2017Oct‐2017Nov‐2017Dec‐2017Jan‐2018
0K
5K
10K
15K
20K
25K
30K
Adult Older People Specialist Secure IPP CorporateServices
Procurement SMARTRedesign
SMART ‐Plans
Required
SalarySacrifice
Prior Year‐1,000
‐500
0
500
1,000
1,500
2,000
Recurrent Achieved Non‐Recurrent Achieved Not Achieved CIP Target
Operational Commentary
Operational Commentary
Cash Balances
Cost Improvement Plan Forecast
Actual cash balance Cash balance per NHS Improvement Plan
The cash balance at the end of M10 was £27.1m ﴾net﴿, which is£1.6m lower than the balance at M9. This is ahead of plannedcash by £10.6m which mainly reflects the income received fromNHS England for one month in relation to the new models ofcare for regional secure services from April 2017, against whichno associated expenditure has been made. This is furtherbolstered by circa £1.9m for STF funding received in 2017/18 butpost submission of the plan, and general working capitalmovements in month 10.
CIPs target for 2017/18 is £2.7m, with a stretched target of£8.68m. ‐ At month 10, £1.752m savings achieved against £2.168mpublished target, a £0.416m under‐achievement, and £6.524msavings achieved against stretched target of £7.150m, £0.626m
behind target. ‐ The published target of £2.7m is forecast to be fully delivered.The stretched target of £8.68m is also forecast to be fullydelivered. ‐ Forecast recurrent achievement against the published target of£2.7m is £1.865m, a 69% exit rate, and £3.757m compared to therecurrent stretched target of £6.993m,a 54% exit rate.
Led
21 of 26
4.1
Inte
grat
edP
erfo
rman
ce a
nd
Page 53 of 96

Well
Adults OPMH Specialist Services Secure Services IPP &Commissioning
HQ ManagedServices
Financing & SLAs Medical HQ‐10.0 %
‐5.0 %
0.0 %
5.0 %
10.0 %
15.0 %
20.0 %
Apr‐2017 May‐2017 Jun‐2017 Jul‐2017 Aug‐2017 Sep‐2017 Oct‐2017 Nov‐2017 Dec‐2017 Jan‐20180
500
1,000
1,500
2,000
2,500
3,000
0 %
2 %
4 %
6 %
8 %
Forecast Variance ﴾%﴿ Variance to date ﴾%﴿
Plan Actual Actual EBITDA % Planned EBITDA %
Operational Commentary
Operational Commentary
Performance Against Budget
Pre‐impairment Surplus Performance
For the month 10 2017/18 position: ‐ Notable adverse variance to date across Adult £3.2m, and IPP1.8m. Offset mainly by favourable variances against SpecialistServices ﴾£1m﴿, Secure Services ﴾£0.75m﴿ , HQ Managed Services﴾£0.3m﴿ and OPMH ﴾£0.1m﴿. ‐Noteable forecast adverse variances across Adult £4.2m and IPP£2.1m. Offset mainly by favourable variances against SpecialistServices ﴾£1.24m﴿ and Secure Services ﴾£0.88m﴿.
Pre‐impairment surplus is £2.671m, in line with the year‐to‐dateplan. ‐ EBITDA position is 6.7%, 0.3% behind the year‐to‐date plan. ‐ Income to date is £124m. ‐ Expenditure to date is £116m.
Led
22 of 26
4.1
Inte
grat
edP
erfo
rman
ce a
nd
Page 54 of 96

Well
Adult OPMH Secure Specialist HQ0K
100K
200K
300K
400K
500K
600K
700K
Apr‐2017 May‐2017 Jun‐2017 Jul‐2017 Aug‐2017 Sep‐2017 Oct‐2017 Nov‐2017 Dec‐2017 Jan‐2018 Feb‐2018 Mar‐20180K
50K
100K
150K
200K
250K
300K
350K
Nursing Medical Clerical Other
Year to date Forecast Outrun
Operational Commentary
Operational Commentary
Agency Spend YTD
Month by Month Agency Spend
Month 10 position: ‐ Total expenditure for Agency as at month 10 was £2,787k. Themajority of this spend ﴾£1,843k﴿ was within nursing.
Month by Month spend: ‐ The chart shows the current spend and forecast spend. Theforecast at month 10 has been refined further in line withexpected usage over the next year, and the department will
continue to work with the directorate, safer staffing and medicalteams to ensure an accurate forecast going forward.
Led
23 of 26
4.1
Inte
grat
edP
erfo
rman
ce a
nd
Page 55 of 96

Well
Apr‐2017 May‐2017 Jun‐2017 Jul‐2017 Aug‐2017 Sep‐2017 Oct‐2017 Nov‐2017 Dec‐2017 Jan‐20180
100
200
300
400
500
600
700
800
Adult OPMH Secure Specialist HQ0K
200K
400K
600K
800K
1,000K
1,200K
1,400K
Framework Non‐Framework
Forecast Spend Target
Operational Commentary
Operational Commentary
Framework / Non‐Framework Agency
Agency Cap ﴾Forecast﴿
The chart sets out the Trust’s expenditure relating to frameworkand non‐framework providers by each month. As per the NHS Improvement guidance, the Trust should not beutilising non framework providers. In January 120 shifts werecovered from non‐framework suppliers, compared to 94 inDecember.
Forecast position at month 10 ‐ The Trust is currently forecasting £3.383m, £0.7m below thecap of £4.056m. Work will be ongoing with the directorates toensure that the forecast is accurate and agency usage is
reduced. ‐ A contingency of £0.5m has been retained from the cap,although the cap provided by NHSI remains at £4.056m.
Led
24 of 26
4.1
Inte
grat
edP
erfo
rman
ce a
nd
Page 56 of 96
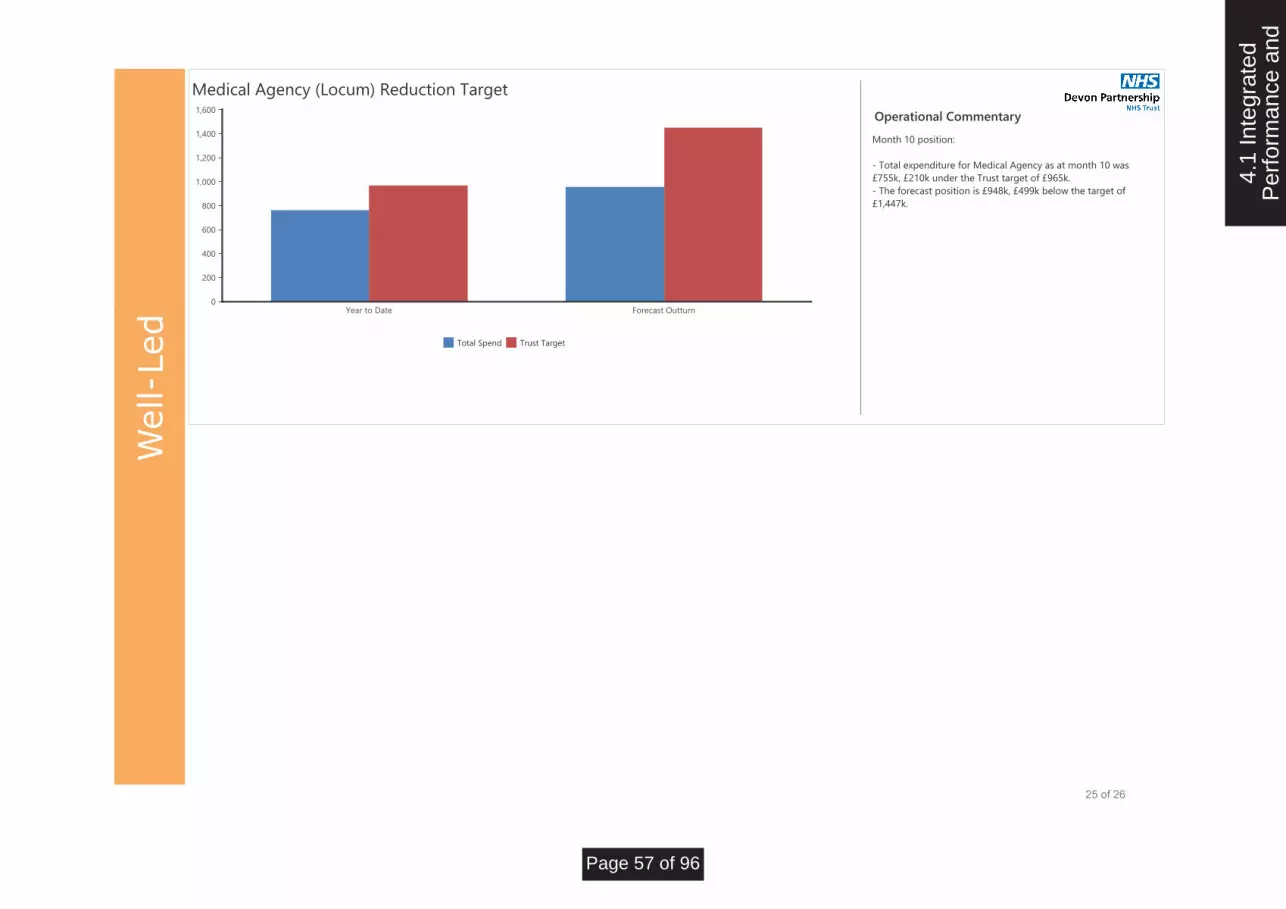
Well
Year to Date Forecast Outturn0
200
400
600
800
1,000
1,200
1,400
1,600
Total Spend Trust Target
Operational Commentary
Medical Agency ﴾Locum﴿ Reduction Target
Month 10 position: ‐ Total expenditure for Medical Agency as at month 10 was£755k, £210k under the Trust target of £965k. ‐ The forecast position is £948k, £499k below the target of£1,447k.
Led
25 of 26
4.1
Inte
grat
edP
erfo
rman
ce a
nd
Page 57 of 96

Well
Operational Commentary
Operational Commentary
KPI‐386 Monitor Risk Rating for Governance
KPI‐165 Monitor overall weighted rating for Finance
Risk Assessment Governance score
Green
Green
Green
CCG Total No ofCQUIN Q1 Q2 Q3
NEW Devon
South Devon& Torbay
NHS Bristol
NHS England
Prison Service
Q4
5
5
1
3
1
Reported byDPT
5 out of 5
5 out of 5
1 out of 1
3 out of 3
1 out of 1
Confirmed byCCG
4 out of 5
4 out of 5
1 out of 1
3 out of 3
1 out of 1
Confirmed byCCG
4 out of 5
1 out of 1
Confirmed byCCG
Confirmed byCCG
CQUIN 2017/18
29 20
Achieved
No. of KPIs ﴾reportedmonthly﴿
Target
10
Bristol WellbeingService
Indicator Group
Performance &Quality
CCG ContractPerformance
4
IAPT
Trust Total
18
11
66%
6
10
CCG Contractual Quality Requirements
KPI‐386 ‐
CQUIN ‐
KPI‐165 ‐
Led
26 of 26
4.1
Inte
grat
edP
erfo
rman
ce a
nd
Page 58 of 96

Report Summary
Report Purpose: Agenda
Item Ref: 5.2
Approval/Decision:
Assurance: X Report to:
Board of Directors
Update
Review Meeting Date:
12 March 2018
Discussion X Steer
GUARDIAN OF SAFE WORKING HOURS REPORT
Presented by:
Dr Helen Smith, Medical Director
Report author(s):
Dr Laurie Windsor, Guardian of Safe Working
Accountable Director: Date Approved:
Dr Helen Smith, Medical Director 1 March 2018
Alignment to the Trust’s strategic aims:
Our aims:
To deliver high quality care and treatment
X To ensure our services are driven by the voices of people who use them
To build a reputation as a recognised centre of excellence and expertise
X To attract and retain talented people and to create a great place to work, with a shared sense of pride and ambition
X
To challenge discrimination and stigma, and to champion recovery, inclusion and wellbeing
To be an efficient, thriving and successful organisation with a sustainable future
Purpose of report:
To provide assurance to the Board that doctors in training are safely rostered and are working hours that are safe and in compliance with their Terms and Conditions.
Summary of the key issues:
• Four exceptions to the safe working practices set out within the Junior Doctor Terms and Conditions have been lodged during the reporting period.
• No fines have been levied during the reporting period.
• Robust systems and processes are in place in relation to reporting and managing exception reports.
• Safe working practices are evidenced within the data provided.
Recommendations:
Members of the Board are requested to receive the report for assurance and discuss the contents.
Report previously presented to:
Committee/Group: Date: Report title: Outcome/action:
Workforce and Organisational Development Committee
01/03/2018 Guardian of Safe Working Hours Report
The report to go to the Board
Summary of compliance implications:
To comply with Guardian for Safe Working requirements. The work of the Guardian is subject to external scrutiny of doctors’ working hours by the Care Quality Commission (CQC) and by the continued scrutiny of the quality of training by Health Education England (HEE). These measures ensure the safety of doctors and therefore of patients.
5.2
Gua
rdia
n of
Saf
e W
orki
ngH
ours
Rep
ort
Page 59 of 96

Board of Directors 12 March 2018 Agenda Item 5.2
Does this report provide assurance in respect of a new / existing risk/s?
Type of risk/s Existing Corporate Assurance Risk Register
Level of Assurance and trend: 1 to 10
Significant Limited None
5.2
Gua
rdia
n of
Saf
e W
orki
ngH
ours
Rep
ort
Page 60 of 96

Board of Directors 12 March 2018 Agenda Item 5.2
BOARD OF DIRECTORS
12 March 2018
GUARDIAN OF SAFE WORKING HOURS REPORT
1. Situation 1.1 The Trust has transitioned 33 doctors in training onto the new Terms and Conditions of
Service for NHS Doctors and Dentists in Training (England) 2016. A further 20 trainees rotate throughout the year from acute Trusts throughout Devon and these are employed by their respective Trusts.
1.2 The purpose of the report is to provide assurance to the Trust that doctors in training are
safely rostered and are working hours that are safe and in compliance with their Terms and Conditions. The report covers the period from 1 July 2017 to October 2017.
2. Background
2.1 The 2016 national contract for junior doctors encourages stronger safeguards to prevent
doctors working excessive hours. The role sits independently from the management structure, with a primary aim to represent and resolve issues related to working hours for the junior doctors employed by it.
2.2 The work of the Guardian is subject to external scrutiny of doctors’ working hours by the Care
Quality Commission (CQC) and by the continued scrutiny of the quality of training by Health Education England (HEE). These measures ensure the safety of doctors and, therefore, of patients.
2.3 The Senior Management Board will receive a quarterly report from the Guardian which will include:
• Aggregated data on exception reports (including outcomes), broken down by categories such as speciality, department and grade.
• Details of fines levied against departments with safety issues.
• Data on rota gaps/staff vacancies/locum usage
• A qualitative narrative highlighting areas of good practice and/or presistent concern 3. Assessment 3.1 Exception reports (with regard to working hours) - Four exception reports have been
created for the time period of this report. These reports were created by one GP trainee in North Devon as well as two Core Trainees and one Foundation Doctor in South Devon. Two of these led to overtime payments, one led to time off in lieu and one is awaiting review. One of these exception reports related to wider possible issues in the junior doctor on call rota in North Devon, which are under review and has been addressed.
3.2 Work schedule reviews – There was one work schedule review that is due to take place. The theme of the work schedule review is related to an increased demand in out of hours work, which has been addressed.
5.2
Gua
rdia
n of
Saf
e W
orki
ngH
ours
Rep
ort
Page 61 of 96

Board of Directors 12 March 2018 Agenda Item 5.2
3.3 Locum Bookings
i) Bank
The table below depicts the total number of locum shifts undertaken by a combination of Specialty Doctors, trainee doctors which include higher trainee doctors and Consultants. This is for the period 1 July 2017 – 31 October 2017.
Locum bookings (bank) by department
Psychiatry Number of shifts
requested
Number of shifts worked
Number of shifts
given to agency
Number of hours
requested
Number of hours
worked
Exeter 31 31 6 - -
South Devon 49 49 3 - -
North Devon 44 44 31 - -
Total 124 124 40 2,295 2,295
• The diagram below demonstrates the number of locum shifts undertaken by junior doctors per month.
• No junior doctor shifts were covered by Consultants.
• The diagram below outlines the reasons for the demand having to be managed. The North Devon rota which has had the highest number of shifts being covered. This was due to some doctors being unable to perform on call and one part-time.
0
10
20
30
40
50
Jul-17 Aug-17 Sep-17 Oct-17
filled by internalmedical staffing JDr(exeter rota)
filled by internalmedical staffing JDr(north rota)
filled internal medicalstaffing JDr (southrota)
5.2
Gua
rdia
n of
Saf
e W
orki
ngH
ours
Rep
ort
Page 62 of 96

Board of Directors 12 March 2018 Agenda Item 5.2
ii) Agency Agencies are unable to supply junior doctors at short notice. Where an agency has been
used, this has been predominately been used to filled vacancies which can be planned in advance. The cost per rota for the quarter is as follows:
• Exeter - £4,136
• South Devon - £2,068
• North Devon - £26,604 The table below outlines the areas of demand and the number of shifts and hours worked.
Locum bookings (agency) by department
Specialty Number of shifts
requested
Number of shifts
worked
Number of hours
requested
Number of hours
worked*
Exeter 6 6 75 75
South Devon 3 3 37.5 37.5
North Devon 35 35 584 584
Total 44 44 696.5 696.5
iii) Locum work carried out by trainees
The table below demonstrates the amount of shifts and hours worked an individual
junior doctor has undertaken across the four month period. These are the highest
number of hours one person has undertaken within each rota. This demonstrates
compliancy with the Junior Doctor Safe Working Hours.
Locum work by trainee
Psychiatry Grade Number of shifts worked
Number of hours worked
Number of hours rostered
per week
Average worked extra
each week
Opted out of WTR?
Exeter ST6 10 123 40 7.7 No
South Devon
Trust Locum
9 96 40 6.0 No
North Devon
Trust locum
10 176 0 - bank 0 No
Total 29 395
0
5
10
15
20
25
30
35
40
45
Exeter rota South Rota North rota
Vacancy
Sickness
Occupational healthadjustments 5.
2 G
uard
ian
of S
afe
Wor
king
Hou
rs R
epor
t
Page 63 of 96

Board of Directors 12 March 2018 Agenda Item 5.2
iv) Vacancies
The table below outlines the number of vacancies within the junior doctor rotas due to vacant slots. These vacancies exist due to a number of reasons, such as allocation of part time trainees, allocation of trainee doctors by HEESW, inability to perform out of hour duties for health reasons and moving within the Trust into Specialty doctor roles.
Psychiatry July Aug Sept Oct Total gaps Number of shifts
uncovered
Exeter 1.6 0 0 0 30 0
South Devon 3 0 0 0 19 0
North Devon 1 0 0 0 41 0
Total 5.6 0 0 0 90 0
v) Fines
• There were no fines levied during this quarter or the last quarter.
Fines (cumulative)
Balance at end of last quarter
Fines this quarter Disbursements this quarter
Balance at end of this quarter
1,010.40 £0 £0 £1,010.40
• Qualitative information Feedback from the junior doctor forum indicates that overall trainees are satisfied that they are working safe hours. The junior doctors have feedback several suggestions of how they feel the money created by fines would be best spent through the Junior Doctor Forum and with the Director of Medical Education, Dr Peter Aitken.
• Summary On the basis of the information provided to me, I am reassured that they are working safe hours. I have no current concerns about specific departments. I am reassured that the junior doctor forum is working well. All junior doctors have the ability to exception report. There have been four exception reports, one outstanding work schedule review and no fines for the time period that this report covers.
4. Recommendations
Members of the Board of Directors are asked to receive the report, and consider and discuss the key points as identified.
Compiled by: Dr Laurie Windsor, Guardian of Safe Working Presented by: Dr Helen Smith, Medical Director Date: 12 March 2018
5.2
Gua
rdia
n of
Saf
e W
orki
ngH
ours
Rep
ort
Page 64 of 96

Report Summary
Safer Staffing - Workforce Report
Presented by:
Paul Keedwell, Director of Nursing and Practice
Report author(s):
Chris Burford, Deputy Director of Nursing and Practice, with the Safer Staffing Team
Accountable Director: Date Approved:
Paul Keedwell, Executive Director of Nursing and Practice
5 March 2018
Alignment to the Trust’s strategic aims:
Our aims:
To deliver high quality care and treatment
x To ensure our services are driven by the voices of people who use them
x
To build a reputation as a recognised centre of excellence and expertise
x To attract and retain talented people and to create a great place to work, with a shared sense of pride and ambition
x
To challenge discrimination and stigma, and to champion recovery, inclusion and wellbeing
x To be an efficient, thriving and successful organisation with a sustainable future
x
Purpose of report:
The Trust is required to report on inpatient staffing levels on a monthly basis – both externally, through the NHS Choices website and internally to the Board.
Summary of the key issues:
Vacancy factor for Whole Time Equivalents
Incidents of staff teams working under established shift numbers
Ward staffing numbers working above establishment
Trust usage of Bank, Agency and overtime
Inclusion of the Bank v Agency shift fill figures for January 2018
Recommendations:
Assurance that inpatient wards are safely staffed at all times, that when breaches with skill mix are identified, they will be mitigated with a ratio of increased unregistered staff. The breaches of skill mix are noted in Section 3.2. Assurance of the containment of agency expenditure over the two year period from November 2015 to January 2018 as illustrated in Appendix C. Assurance the continued controls implemented by the Safe Staffing Team, including validation of agency requests, agency negotiation and rostering. To support the development of a ward based Dashboard tool to support the rationale of assuring safely staffed inpatient wards.
Report Purpose: Agenda
Item Ref: 5.3
Approval/Decision: x
Assurance: x Report
to: Board of Directors
Update x
Review x Meeting
Date: 12 March 2018
Discussion
x Steer
5.3
Saf
er S
taffi
ng -
Wor
kfor
ceR
epor
t
Page 65 of 96
Board of Directors, 12 March 2018 Agenda Item 5.3
Report previously presented to:
Committee/Group: Date: Report title: Outcome/action:
Senior Management Boar Quality & Safety Committee
22/02/18 1/03/18
Safer Staffing - Workforce Report
Paper Acknowledged
Summary of compliance implications:
Meeting agency spending cap and National Quality Board requirements
Does this report provide assurance in respect of a new / existing risk/s?
Type of risk/s Existing Corporate Assurance x Risk Register x
Level of Assurance and trend: 1 to 10
Significant Limited None
8
5.3
Saf
er S
taffi
ng -
Wor
kfor
ceR
epor
t
Page 66 of 96

Board of Directors, 12 March 2018 Agenda Item 5.3
DEVON PARTNERSHIP NHS TRUST BOARD OF DIRECTORS
12 March 2018
SAFER STAFFING – WORKFORCE REPORT
1. Situation 1.1 The Trust is required to report on inpatient staffing levels on a monthly basis – both
externally, through the NHS Choices website and internally to the Board. This has been a requirement since June 2014.
1.2 This report is reflective of the National Quality Board guidance published July 2016:
“Staffing Guidance any Guidance applicable to the Services in relation to Staff numbers or
skill-mix, including the National Quality Board publication Supporting NHS providers to
deliver the right staff, with the right skills, in the right place at the right time, available at
https://www.england.nhs.uk/wp-content/uploads/2013/04/nqb-guidance.pdf
2. Background 2.1 The data presented on this report is obtained through the following reports/systems:
• ORBIT – Workforce Report Inpatient Staffing
Planned hours, Total Hours worked, Overtime, Bank and Agency
• ESR – NHS Absence Management Analysis - organisation absence record
annual leave, study leave, other planned leave, sickness, other unplanned
leave.
• AGRESSO – AD Vacancy Report
Full-time equivalent establishment, actual, vacancies, pending new starters.
3. Assessment 3.1 Appendix A illustrates the vacancies for Registered Mental Health Nursing (RMHN) staff
within inpatient wards have decreased from 60.27 Full Time Equivalent (FTE) (Reported
January 2018) to 56.41FTE – this includes the inclusion of the Mother and Baby Unit that
has not been fully recruited too.
3.2 Appendix B Currently Mental Health Practitioners (MHPs) comprising Occupational
Therapists and Social Workers are employed onto wards as a second professional within the
new ward establishments to support the Qualified Nursing Staff. There are 3 MHPs working
in this capacity, primarily on the Langdon site, providing quality support for the Nursing team.
This initiative will be used across all wards with positive recruitment to these posts expected
during 2018.
3.3 Appendix C Support staff posts are 271.80FTE for Band 3 Healthcare Assistants, with an
actual requirement for 163.91FTE as agreed within the current establishment review. This is
a current over establishment of 107.89FTE currently in post. Band 4 Assistant Practitioners
posts are established at 112.73FTE, with a current establishment of 17.60FTE in post. This
is a shortfall of 95.13FTE for the Band 4 Assistant Practitioner role. Therefore the Band 3
5.3
Saf
er S
taffi
ng -
Wor
kfor
ceR
epor
t
Page 67 of 96
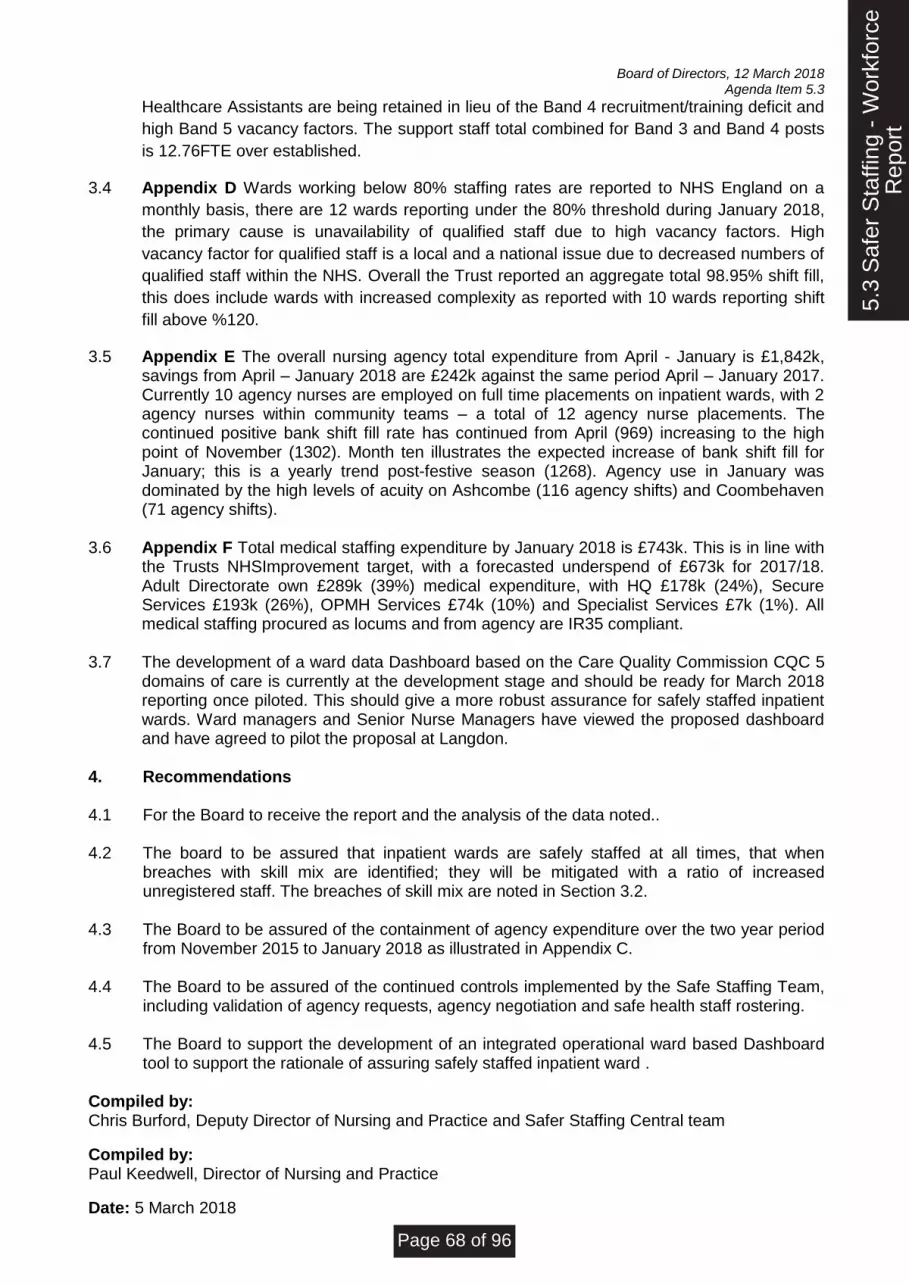
Board of Directors, 12 March 2018 Agenda Item 5.3
Healthcare Assistants are being retained in lieu of the Band 4 recruitment/training deficit and
high Band 5 vacancy factors. The support staff total combined for Band 3 and Band 4 posts
is 12.76FTE over established.
3.4 Appendix D Wards working below 80% staffing rates are reported to NHS England on a
monthly basis, there are 12 wards reporting under the 80% threshold during January 2018,
the primary cause is unavailability of qualified staff due to high vacancy factors. High
vacancy factor for qualified staff is a local and a national issue due to decreased numbers of
qualified staff within the NHS. Overall the Trust reported an aggregate total 98.95% shift fill,
this does include wards with increased complexity as reported with 10 wards reporting shift
fill above %120.
3.5 Appendix E The overall nursing agency total expenditure from April - January is £1,842k, savings from April – January 2018 are £242k against the same period April – January 2017. Currently 10 agency nurses are employed on full time placements on inpatient wards, with 2 agency nurses within community teams – a total of 12 agency nurse placements. The continued positive bank shift fill rate has continued from April (969) increasing to the high point of November (1302). Month ten illustrates the expected increase of bank shift fill for January; this is a yearly trend post-festive season (1268). Agency use in January was dominated by the high levels of acuity on Ashcombe (116 agency shifts) and Coombehaven (71 agency shifts).
3.6 Appendix F Total medical staffing expenditure by January 2018 is £743k. This is in line with
the Trusts NHSImprovement target, with a forecasted underspend of £673k for 2017/18. Adult Directorate own £289k (39%) medical expenditure, with HQ £178k (24%), Secure Services £193k (26%), OPMH Services £74k (10%) and Specialist Services £7k (1%). All medical staffing procured as locums and from agency are IR35 compliant.
3.7 The development of a ward data Dashboard based on the Care Quality Commission CQC 5
domains of care is currently at the development stage and should be ready for March 2018 reporting once piloted. This should give a more robust assurance for safely staffed inpatient wards. Ward managers and Senior Nurse Managers have viewed the proposed dashboard and have agreed to pilot the proposal at Langdon.
4. Recommendations 4.1 For the Board to receive the report and the analysis of the data noted.. 4.2 The board to be assured that inpatient wards are safely staffed at all times, that when
breaches with skill mix are identified; they will be mitigated with a ratio of increased unregistered staff. The breaches of skill mix are noted in Section 3.2.
4.3 The Board to be assured of the containment of agency expenditure over the two year period
from November 2015 to January 2018 as illustrated in Appendix C. 4.4 The Board to be assured of the continued controls implemented by the Safe Staffing Team,
including validation of agency requests, agency negotiation and safe health staff rostering. 4.5 The Board to support the development of an integrated operational ward based Dashboard
tool to support the rationale of assuring safely staffed inpatient ward . Compiled by: Chris Burford, Deputy Director of Nursing and Practice and Safer Staffing Central team
Compiled by: Paul Keedwell, Director of Nursing and Practice
Date: 5 March 2018
5.3
Saf
er S
taffi
ng -
Wor
kfor
ceR
epor
t
Page 68 of 96

Board of Directors, 12 March 2018 Agenda Item 5.3
Appendix A
Band 5 and Band 6 Vacancy Tables 310118
Directorate Team
Sum of
Establishment
Band 5 FTE
adjusted
Sum of Actual
Band 5 FTE
Sum of Band 5
FTE Vacant
Sum of Band
5 FTE
Vacancy %
Sum of
Establishment
Band 6 FTE
adjusted
Sum of Actual
Band 6 FTE
Sum of Band 6
FTE Vacant
Sum of Band
6 FTE
Vacancy %
Total Establishment
Band 5 & Band 6
FTE adjusted
Sum of Actual
Band 5 &
Band 6 FTE
Sum of Band
5 & Band 6
FTE Vacant
Sum of
Band 5 &
Band 6 FTE
Vacancy %
369 Adult Mental Health
Services Directorate 369 Coombehaven 9.66 3.40 6.26 64.80% 2.00 1.80 0.20 10.00% 11.66 5.20 6.46 55.40%
369 Delderfield 9.66 7.03 2.63 27.26% 2.00 2.80 -0.80 -40.00% 11.66 9.83 1.83 15.72%
369 Haytor 9.91 6.40 3.51 35.42% 2.00 2.00 0.00 0.00% 11.91 8.40 3.51 29.47%
369 Moorland View 8.40 5.60 2.80 33.33% 2.00 1.00 1.00 50.00% 10.40 6.60 3.80 36.54%
369 Ocean View 8.40 7.80 0.60 7.14% 2.00 2.00 0.00 0.00% 10.40 9.80 0.60 5.77%
369 Russell Clinic 7.14 7.20 -0.06 -0.84% 2.00 2.00 0.00 0.00% 9.14 9.20 -0.06 -0.66%
369 Adult Mental Health Services Directorate Total 53.17 37.43 15.74 29.61% 12.00 11.60 0.40 3.33% 65.17 49.03 16.14 24.77%
369 Older Peoples Mental
Health Services 369 Beech Unit 9.91 7.80 2.11 21.29% 2.00 2.00 0.00 0.00% 11.91 9.80 2.11 17.72%
369 Belvedere 8.66 6.00 2.66 30.72% 2.00 2.00 0.00 0.00% 10.66 8.00 2.66 24.95%
369 Meadow View 9.66 4.52 5.14 53.21% 2.00 0.80 1.20 60.00% 11.66 5.32 6.34 54.37%
369 Rougemont 10.16 9.30 0.86 8.46% 2.00 2.00 0.00 0.00% 12.16 11.30 0.86 7.07%
369 Older Peoples Mental Health Services Total 38.39 27.62 10.77 28.05% 8.00 6.80 1.20 15.00% 46.39 34.42 11.97 25.80%
369 Secure Services 369 Ashcombe 7.13 5.00 2.13 29.87% 4.53 1.00 3.53 77.92% 11.66 6.00 5.66 48.54%
369 Avon House 6.34 4.40 1.94 30.60% 3.00 4.00 -1.00 -33.33% 9.34 8.40 0.94 10.06%
369 Chichester House 5.54 3.00 2.54 45.85% 4.00 3.96 0.04 1.00% 9.54 6.96 2.58 27.04%
369 Cofton 7.14 3.44 3.70 51.82% 2.00 3.80 -1.80 -90.00% 9.14 7.24 1.90 20.79%
369 Holcombe 8.06 3.00 5.06 62.78% 4.00 4.00 0.00 0.00% 12.06 7.00 5.06 41.96%
369 Owen House 6.34 5.60 0.74 11.67% 3.00 3.00 0.00 0.00% 9.34 8.60 0.74 7.92%
369 Warren 8.86 3.80 5.06 57.11% 3.00 3.00 0.00 0.00% 11.86 6.80 5.06 42.66%
369 Secure Services Total 49.41 28.24 21.17 42.85% 23.53 22.76 0.77 3.27% 72.94 51.00 21.94 30.08%
369 Specialist Services 369 Haldon Service 8.06 6.60 1.46 18.11% 3.00 3.00 0.00 0.00% 11.06 9.60 1.46 13.20%
369 LD Inpatient - ASU 9.66 6.00 3.66 37.89% 2.00 1.50 0.50 25.00% 11.66 7.50 4.16 35.68%
369 Mother and Baby Unit - 4 Bed 5.64 5.00 0.64 11.35% 1.70 1.60 0.10 5.88% 7.34 6.60 0.74 10.08%
369 Specialist Services Total 23.36 17.60 5.76 24.66% 6.70 6.10 0.60 8.96% 30.06 23.70 6.36 21.16%
Grand Total 164.33 110.89 53.44 32.52% 50.23 47.26 2.97 5.91% 214.56 158.15 56.41 26.29%
Data - Band 5 & Band 6 vacancies January 2018
5.3
Saf
er S
taffi
ng -
Wor
kfor
ce R
epor
t
Page 69 of 96

Board of Directors, 12 March 2018 Agenda Item 5.3
Appendix B
Band 5 Inpatient Mental Health Practitioners
Band 5 Mental Health Practitioners Vacancies for Wards as at 31/01/2018
Directorate Team Sum of Establishment Fte adjusted Sum of Actual Fte Sum of FTE Vacant Sum of FTE Vacancy %
369 Adult Mental Health Services Directorate 369 Coombehaven 1.00 0.00 1.00 100.00%
369 Delderfield 1.00 0.00 1.00 100.00%
369 Adult Mental Health Services Directorate Total 2.00 0.00 2.00 100.00%
369 Secure Services 369 Ashcombe 0.00 1.00 -1.00 -100.00%
369 Avon House 0.00 1.00 -1.00 -100.00%
369 Chichester House 0.00 1.00 -1.00 -100.00%
369 Connelly House 1.00 0.00 1.00 100.00%
369 Secure Services Total 1.00 3.00 -2.00 -200.00%
369 Specialist Services 369 Mother and Baby Unit - 4 Bed 0.30 0.00 0.30 100.00%
369 Specialist Services Total 0.30 0.00 0.30 100.00%
Grand Total 3.30 3.00 0.30 9.09%
5.3
Saf
er S
taffi
ng -
Wor
kfor
ce R
epor
t
Page 70 of 96

Board of Directors, 12 March 2018 Agenda Item 5.3
Appendix C
Band 3 and Band 4 Vacancy Tables 310118
Directorate Team
Sum of
Establishment
Band 3 FTE
adjusted
Sum of Actual
Band 3 FTE
Sum of Band 3
FTE Vacant
Sum of Band 3
FTE Vacant %
Sum of
Establishment
Band 4 FTE
adjusted
Sum of Actual
Band 4 FTE
Sum of Band 4
FTE Vacant
Sum of Band 4
FTE Vacant %
Sum of
Establishment
Band 3 & Band 4
FTE adjusted
Sum of Band
3 & Band 4
Actual FTE
Sum of Band 3
& Band 4 FTE
Vacant
Sum of Band
3 & Band 4
FTE Vacancy
%
369 Adult Mental Health
Services Directorate 369 Coombehaven 7.58 17.16 -9.58 -126.39% 5.29 0.00 5.29 100.00% 12.87 17.16 -4.29 -33.33%
369 Delderfield 7.58 12.20 -4.62 -60.95% 5.29 0.00 5.29 100.00% 12.87 12.20 0.67 5.21%
369 Haytor 7.58 16.29 -8.71 -114.95% 5.29 0.00 5.29 100.00% 12.87 16.29 -3.42 -26.60%
369 Moorland View 8.84 12.04 -3.20 -36.20% 5.29 1.00 4.29 81.10% 14.13 13.04 1.09 7.71%
369 Ocean View 8.85 13.64 -4.79 -54.12% 5.29 0.00 5.29 100.00% 14.14 13.64 0.50 3.54%
369 Russell Clinic 3.45 8.70 -5.25 -152.17% 5.29 0.00 5.29 100.00% 8.74 8.70 0.04 0.46%
369 Adult Mental Health Services Directorate Total 43.88 80.03 -36.15 -82.39% 31.74 1.00 30.74 96.85% 75.62 81.03 -5.41 -7.16%
369 Older Peoples Mental
Health Services 369 Beech Unit 7.08 12.20 -5.12 -72.32% 5.29 0.00 5.29 100.00% 12.37 12.20 0.17 1.37%
369 Belvedere 11.03 15.68 -4.65 -42.16% 5.29 1.60 3.69 69.75% 16.32 17.28 -0.96 -5.88%
369 Meadow View 7.58 16.55 -8.97 -118.29% 5.29 0.00 5.29 100.00% 12.87 16.55 -3.68 -28.57%
369 Rougemont 7.58 11.20 -3.62 -47.76% 5.29 0.00 5.29 100.00% 12.87 11.20 1.67 12.98%
369 Older Peoples Mental Health Services Total 33.27 55.63 -22.36 -67.20% 21.16 1.60 19.56 92.44% 54.43 57.23 -2.80 -5.14%
369 Secure Services 369 Ashcombe 12.97 20.88 -7.91 -60.99% 10.77 1.00 9.77 90.71% 23.74 21.88 1.86 7.83%
369 Avon House 4.13 12.00 -7.87 -190.56% 5.98 3.00 2.98 49.83% 10.11 15.00 -4.89 -48.37%
369 Chichester House 5.78 10.24 -4.46 -77.16% 5.48 1.64 3.84 70.07% 11.26 11.88 -0.62 -5.51%
369 Cofton 4.13 13.20 -9.07 -219.61% 5.98 0.96 5.02 83.95% 10.11 14.16 -4.05 -40.06%
369 Connelly House 6.00 4.80 1.20 20.00% 6.00 1.00 5.00 83.33% 12.00 5.80 6.20 51.67%
369 Holcombe 13.33 16.00 -2.67 -20.03% 6.90 2.00 4.90 71.01% 20.23 18.00 2.23 11.02%
369 Owen House 11.26 11.32 -0.06 -0.51% 0.00 0.40 -0.40 -100.00% 11.26 11.72 -0.46 -4.07%
369 Warren 4.13 12.60 -8.47 -205.08% 5.98 1.00 4.98 83.28% 10.11 13.60 -3.49 -34.52%
369 Secure Services Total 61.73 101.04 -39.31 -63.68% 47.09 11.00 36.09 76.64% 108.82 112.04 -3.22 -2.96%
369 Specialist Services 369 Haldon Service 6.78 12.70 -5.92 -87.32% 5.29 0.00 5.29 100.00% 12.07 12.70 -0.63 -5.22%
369 LD Inpatient - ASU 13.56 19.40 -5.84 -43.07% 2.76 0.00 2.76 100.00% 16.32 19.40 -3.08 -18.87%
369 Mother and Baby Unit - 4 Bed 4.69 3.00 1.69 36.03% 4.69 4.00 0.69 14.71% 9.38 7.00 2.38 25.37%
369 Specialist Services Total 25.03 35.10 -10.07 -40.23% 12.74 4.00 8.74 68.60% 37.77 39.10 -1.33 -3.52%
Grand Total 163.91 271.80 -107.89 -65.82% 112.73 17.60 95.13 84.39% 276.64 289.40 -12.76 -4.61%
Band 3 and 4 Support Worker Vacancies as at 31/01/2018
5.3
Saf
er S
taffi
ng -
Wor
kfor
ce R
epor
t
Page 71 of 96

Board of Directors, 12 March 2018 Agenda Item 5.3
Appendix D
Summary of Total Hours Worked for Nursing Registered and Support StaffPeriod : 01/01/2018 to 31/01/2018
Registered Registered Support Support
Worked Planned Worked Planned
369 Coombehaven 805.25 930 86.59% 1408.75 1162.5 121.18% 2:1 Supportive Observations
369 Delderfield 832.5 930 89.52% 1380 1534.5 89.93%
369 Haytor 809 930 86.99% 1181.5 1162.5 101.63%
369 Moorland View 856.5 930 92.10% 936 1162.5 80.52%
369 Ocean View 1103 930 118.60% 852 1162.5 73.29% RMN covering/HCAs on nights
369 Russell Clinic 864.5 930 92.96% 812 930 87.31%
369 Beech Unit 922.5 930 99.19% 1307 1162.5 112.43% Twilight shift
369 Belvedere 661.5 930 71.13% 2077 2092.5 99.26% RMN Vacancies
369 Meadow View 887 930 95.38% 1305.5 1162.5 112.30%
369 Rougemont 917.5 930 98.66% 926.5 930 99.62%
369 Ashcombe 817.5 744 109.88% 2219 2092.5 106.05%
369 Avon House 682 930 73.33% 948.5 930 101.99% RMN Vacancies
369 Chichester House 568.5 837 67.92% 1131 837 135.13% RMN Vacancies/HCA cover
369 Cofton 763.5 930 82.10% 840 930 90.32%
369 Connelly 540 465 116.13% 428.5 465 92.15%
369 Holcombe 615 930 66.13% 1546 1860 83.12% RMN Vacancies
369 Owen 552 930 59.35% 969 930 104.19% RMN Vacancies
369 Warren 805.5 930 86.61% 1082.5 930 116.40%
369 Haldon Service 959 1162.5 82.49% 1394.5 1162.5 119.96%
369 LD Inpatient - ASU 783.25 930 84.22% 1812.25 2092.5 86.61%
Total 15745.5 18088.5 87.05% 24557.5 24691.5 99.46%
Registered Registered Support Support
Worked Planned Worked Planned
369 Coombehaven 532.5 682 78.08% 1113 682 163.20% RMN Vacancies/HCA cover
369 Delderfield 648.5 682 95.09% 922 682 135.19% Escalation Level 3 Obs
369 Haytor 484 682 70.97% 891 682 130.65% RMN Vacancies/HCA cover
369 Moorland View 385 511.5 75.27% 979 852.5 114.84% RMN Vacancies/HCA cover
369 Ocean View 341 511.5 66.67% 1001 852.5 117.42% RMN Vacancies/HCA cover
369 Russell Clinic 396 372 106.45% 672 372 180.65% Escalation Level 3 Obs
369 Beech Unit 341 341 100.00% 759 1023 74.19% 1 x Twilight HCA/2 x HCA nights
369 Belvedere 372 511.5 72.73% 1342.5 852.5 157.48% RMN Vacancies/HCA cover
369 Meadow View 341 341 100.00% 990 1023 96.77%
369 Rougemont 382 511.5 74.68% 671 511.5 131.18% RMN Vacancies/HCA cover
369 Ashcombe 407 341 119.35% 2486 1364 182.26% Escalation Level 3 Obs
369 Avon House 372 372 100.00% 682 682 100.00%
369 Chichester House 372 372 100.00% 744 744 100.00%
369 Cofton 341 341 100.00% 682 682 100.00%
369 Connelly 0 0 #DIV/0! 744 744 100.00%
369 Holcombe 372 372 100.00% 1353 1364 99.19%
369 Owen 372 372 100.00% 744 744 100.00%
369 Warren 341 682 50.00% 693 682 101.61% Budget 2 x RMN Nights
369 Haldon Service 372 372 100.00% 1046.5 372 281.32% Escalation Level 3 Obs
369 LD Inpatient - ASU 374 372 100.54% 1083 1023 105.87%
Total 7546 8742 86.32% 19598 15934 122.99%
Secure Services
Specialist
Services
Adult Mental
Health Services
Comments% Fill Rate
Night
Comments% Fill Rate
Day
% Fill Rate
Older Peoples
Mental Health
Services
Adult Mental
Health Services
Older Peoples
Mental Health
Services
Secure Services
Specialist
Services
% Fill Rate
5.3
Saf
er S
taffi
ng -
Wor
kfor
ceR
epor
t
Page 72 of 96
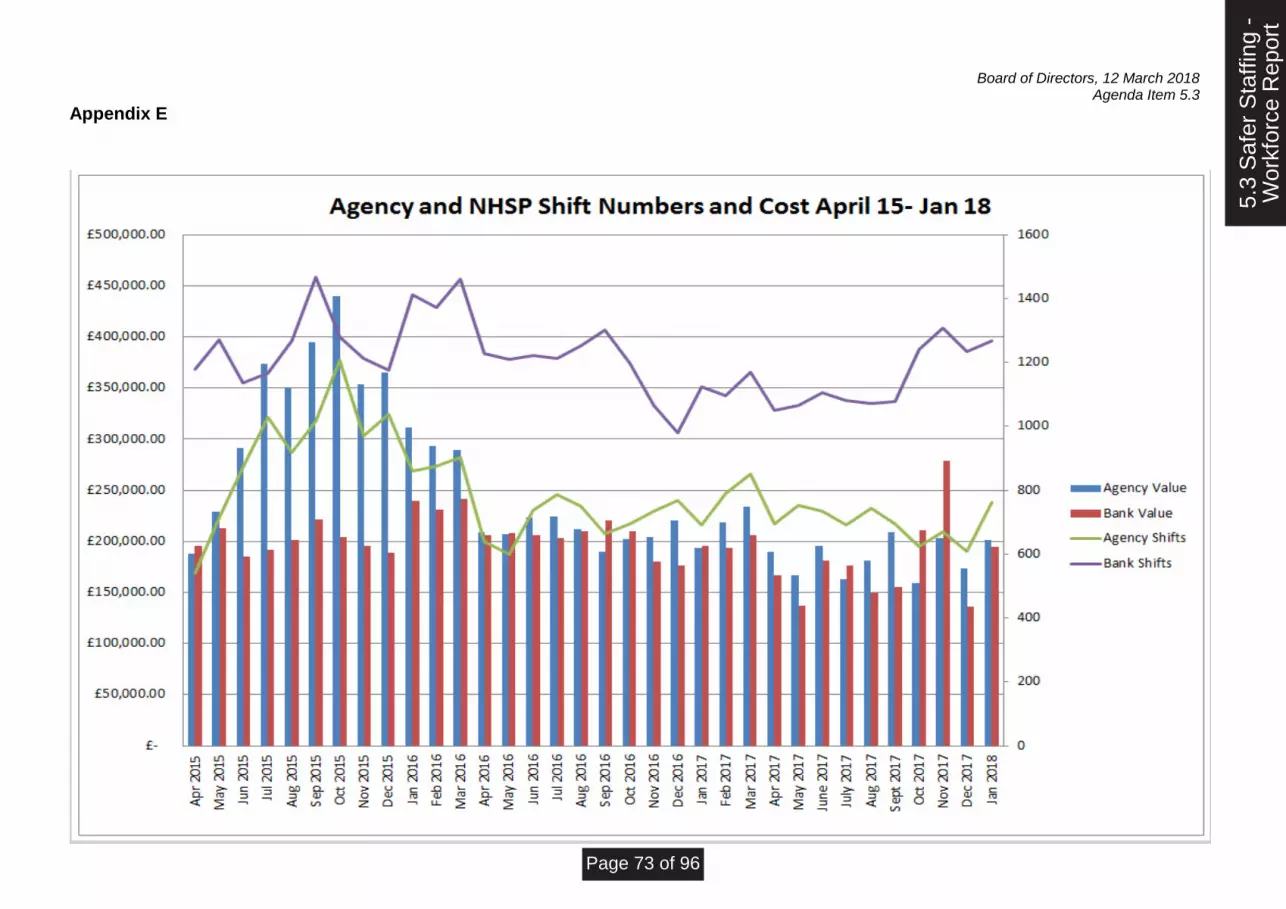
Board of Directors, 12 March 2018 Agenda Item 5.3
Appendix E
5.3
Saf
er S
taffi
ng -
Wor
kfor
ce R
epor
t
Page 73 of 96

Board of Directors, 12 March 2018 Agenda Item 5.3
Appendix F: Agency Reduction Group - January 2017 Data
Produced by Katie Bridle, Finance
Summary:
• Total forecast spend £3,383k by end of year – this assumes an increase on straight line forecast of £39k.
• Current forecast sees us under the Trust target by £673k.
• Trust cap for 17/18 is the same as 16/17. The locum cap of £225k notified by NHSI has been confirmed as medical agency only, and is within the trust cap, rather than reducing it.
• Specialist have breached the cap set at month 2 by £10k.
• HQ have breached the cap set at month 2 by £153k. Trust Wide Agency Spend to Date The below chart splits the agency spend to date by area. Nursing (qualified and unqualified)
is the largest spend, with medical second. Other comprises of various professions including
psychologists, occupational therapists and hotel services staff. Trust medical locums include
doctors paid through the IR35 method through payroll.
Directorate Caps
The above table demonstrates the actual position for each directorate, and compares to their
individual caps.
The directorate caps have been revised at month 2. A £500k contingency has been
removed from the total trust cap, and the remaining balance has been split between the
Spend to Date Forecast Spend Target
Over/(Under)
Target
Adult 940,953 1,137,051 1,245,175 (108,124)
OPMH 437,940 517,989 588,500 (70,511)
Secure 747,119 884,136 1,040,675 (156,539)
Specialist 231,349 284,783 275,193 9,590
HQ 429,246 558,985 406,457 152,528
Contingency - - 500,000 (500,000)
2,786,608 3,382,944 4,056,000 (673,056)
5.3
Saf
er S
taffi
ng -
Wor
kfor
ceR
epor
t
Page 74 of 96

Board of Directors, 12 March 2018 Agenda Item 5.3
Appendix F: Agency Reduction Group - January 2017 Data
Produced by Katie Bridle, Finance
directorates based on their forecast at month 2 (17/18). At month 9, Specialist and HQ are
forecasting to breach the cap.
The below charts demonstrate the overall Trust position against NHS Improvement caps.
5.3
Saf
er S
taffi
ng -
Wor
kfor
ceR
epor
t
Page 75 of 96
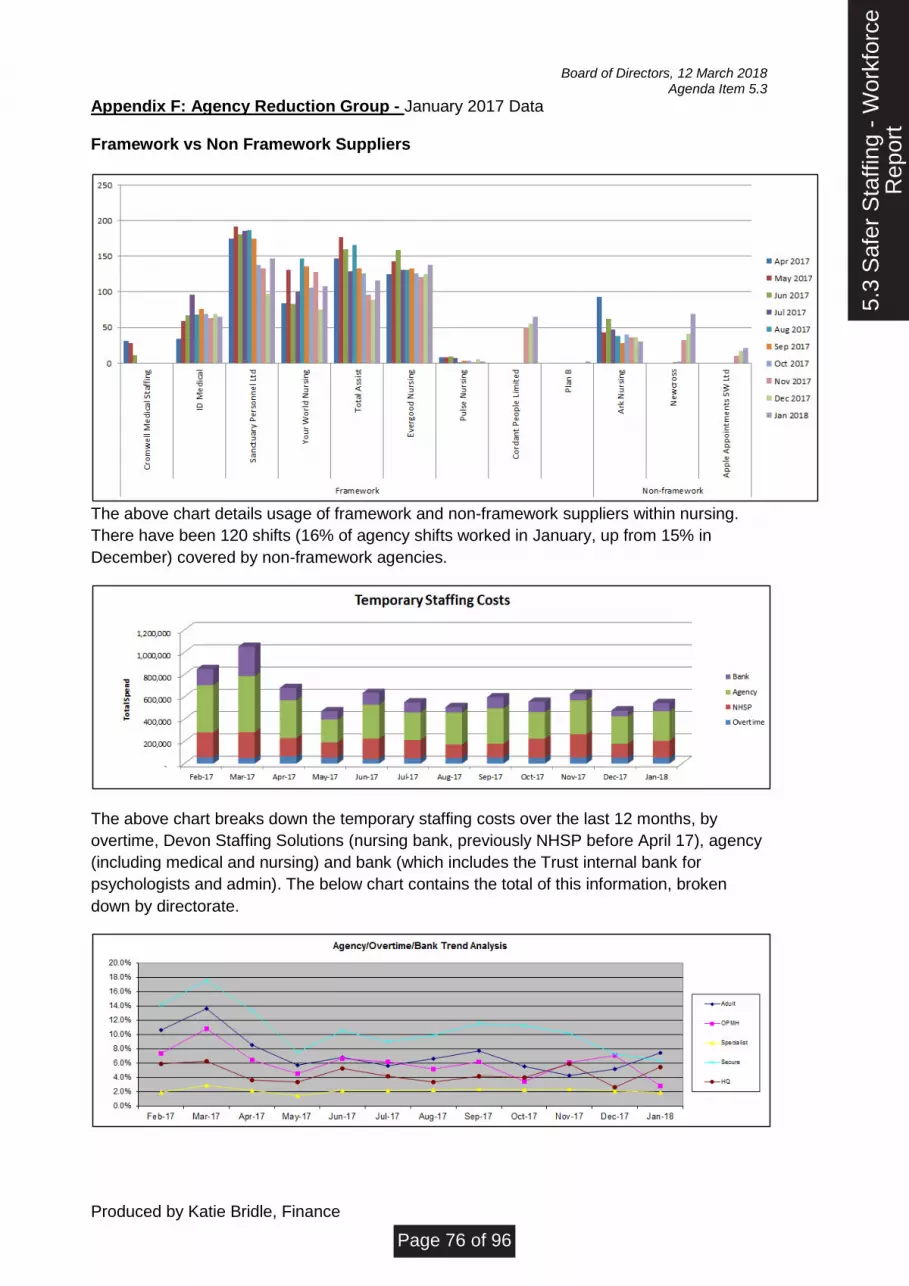
Board of Directors, 12 March 2018 Agenda Item 5.3
Appendix F: Agency Reduction Group - January 2017 Data
Produced by Katie Bridle, Finance
Framework vs Non Framework Suppliers
The above chart details usage of framework and non-framework suppliers within nursing.
There have been 120 shifts (16% of agency shifts worked in January, up from 15% in
December) covered by non-framework agencies.
The above chart breaks down the temporary staffing costs over the last 12 months, by
overtime, Devon Staffing Solutions (nursing bank, previously NHSP before April 17), agency
(including medical and nursing) and bank (which includes the Trust internal bank for
psychologists and admin). The below chart contains the total of this information, broken
down by directorate.
5.3
Saf
er S
taffi
ng -
Wor
kfor
ceR
epor
t
Page 76 of 96

Board of Directors, 12 March 2018 Agenda Item 5.3
Appendix F: Agency Reduction Group - January 2017 Data
Produced by Katie Bridle, Finance
Breakdown of Spend The Medical Agency spend compares the amount spent on medical agency by directorate by
month.
5.3
Saf
er S
taffi
ng -
Wor
kfor
ceR
epor
t
Page 77 of 96

1
Report Purpose: Agenda
Item Ref: 5.4
Approval/Decision:
Assurance: Report
to: Trust Board
Update
Review Meeting
Date: 12 March 2018
Discussion
Steer
Equality, Diversity and Inclusion - Gender Pay Gap Report
Presented by:
Paul Keedwell, Director of Nursing and Practice
Report author(s):
Laura Hobbs, Head of CQC Compliance, Nursing Executive Support and Equality, Diversity & Inclusion Katy Tatman, Nursing and Professions Business Manager
Accountable Director: Date Approved:
Paul Keedwell, Director of Nursing and Practice March 2018
Alignment to the Trust’s strategic aims:
Our aims:
To deliver high quality care and treatment
To ensure our services are driven by the voices of people who use them
To build a reputation as a recognised centre of excellence and expertise
To attract and retain talented people and to create a great place to work, with a shared sense of pride and ambition
To challenge discrimination and stigma, and to champion recovery, inclusion and wellbeing
To be an efficient, thriving and successful organisation with a sustainable future
Purpose of report:
To approve and sign off the Gender Pay Gap report for mandatory publication on Trust website and government website.
Summary of the key issues:
This report provides gender pay gap analysis of our workforce data as at the snapshot date of 31 March 2017. Mandatory reporting of the findings as required nationally, with Trust information to be published by 30 March 2018 on both the government website and the Trust’s public facing website.
Recommendations:
Members of Trust Board are asked to:
• approve the Trust Gender Pay Gap as at snapshot date 31st March 2017 for publication on the government website and Trust website.
• approve the development of a responsive action plan through the Workforce and Organisational Development Assurance Committee.
Report previously presented to:
Committee/Group: Date: Report title: Outcome/action:
Senior Management Board (Workforce)
22 February 2018
Equality, Diversity and Inclusion - Gender Pay Gap Report
Recommended for onward approval – Approved
Workforce and Organisational Development Assurance Committee
1 March 2018
Equality, Diversity and Inclusion - Gender Pay Gap Report
Recommended for onward approval – NOT APPROVED. Report amended in response to feedback
Summary of compliance implications:
5.4
Gen
der
Pay
Gap
Rep
ort
Page 78 of 96

Board of Directors, 12 March 2018 Agenda Item 5.4
Does this report provide assurance in respect of a new / existing risk/s?
Type of risk/s New Corporate Assurance Risk Register
Level of Assurance and trend: 1 to 10
Significant Limited None
7
5.4
Gen
der
Pay
Gap
Rep
ort
Page 79 of 96

Board of Directors, 12 March 2018 Agenda Item 5.4
1
DEVON PARTNERSHIP NHS TRUST BOARD OF DIRECTORS
Meeting 12 March 2018
EQUALITY, DIVERSITY AND INCLUSION - GENDER PAY GAP REPORT (Data Snapshot Date - 31 March 2018)
1. Situation Devon Partnership NHS Trust is required by law to undertake Gender Pay Reporting under the
Equality Act 2010 (Specific Duties & Public Authorities) Regulations 2017. The requirement to
publish specific gender pay gap information became an annual activity as of April 2017,
requiring employers with more than 250 employees to publish the following statutory
calculations:
• The difference between the mean hourly rate of pay for male and female employees
• The difference between the median hourly rate of pay for male and female employees
• The difference between the mean bonus pay for male and female employees
• The difference between the median bonus pay for male and female employees
• Proportions of male and female employees who were paid a bonus
• The proportions of male and female employees in the four quartile pay bands (lower, lower
middle, upper middle and upper)
The gender pay gap shows the difference in average hourly pay between all men and women in
the workforce. If a workforce has a particularly high gender pay gap, this can indicate there may
be issues that need to be dealt with and the detailed calculations may help to identify what
those issues are.
Throughout the report detail following, percentage difference between male and female hourly
rates is shown. Positive percentage pay gaps are used to indicate men are the higher earners
and negative percentage pay gaps are where women earn more on average.
One of Devon Partnership NHS Trust’s six strategic aims is ‘Challenging discrimination and
stigma and to champion recovery, inclusion and wellbeing.’ We have analysed workforce
race equality for the past two years and commence workforce disability equality analysis this
year.
Undertaking the gender pay gap analysis in response to the national requirement supports our
strategic aim and forms part of a wider piece of work we are focusing on in the coming year - to
review our workforce data across all protected characteristics as defined under the Equality Act
2010.
As part of our wider Equality, Diversity and Inclusion portfolio, an action plan will be developed
in response to the findings of the Gender Pay Gap audit and agreed through our Workforce and
Organisational Development Assurance Committee.
5.4
Gen
der
Pay
Gap
Rep
ort
Page 80 of 96
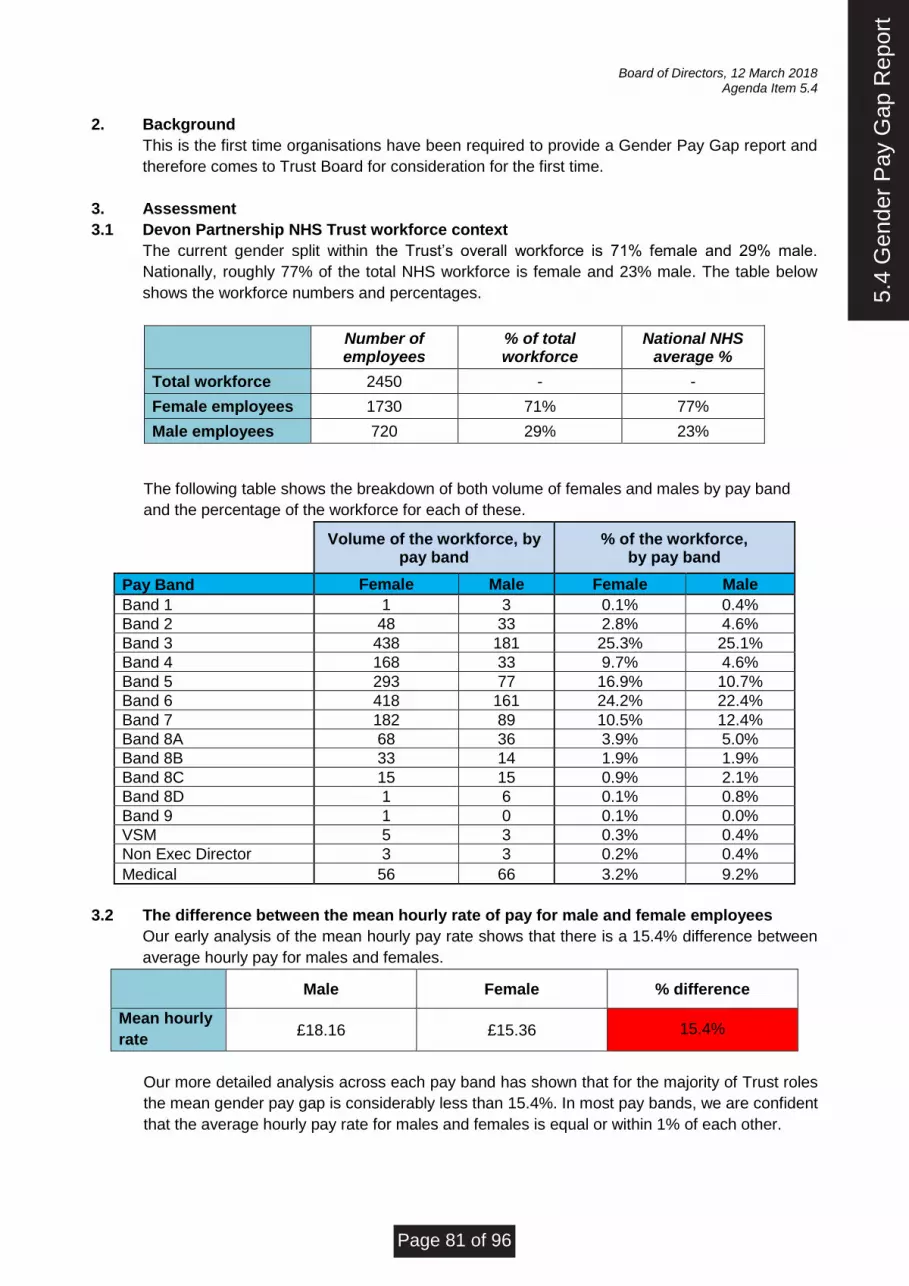
Board of Directors, 12 March 2018 Agenda Item 5.4
2. Background
This is the first time organisations have been required to provide a Gender Pay Gap report and
therefore comes to Trust Board for consideration for the first time.
3. Assessment
3.1 Devon Partnership NHS Trust workforce context
The current gender split within the Trust’s overall workforce is 71% female and 29% male.
Nationally, roughly 77% of the total NHS workforce is female and 23% male. The table below
shows the workforce numbers and percentages.
Number of employees
% of total workforce
National NHS average %
Total workforce 2450 - -
Female employees 1730 71% 77%
Male employees 720 29% 23%
The following table shows the breakdown of both volume of females and males by pay band
and the percentage of the workforce for each of these.
Volume of the workforce, by pay band
% of the workforce, by pay band
Pay Band Female Male Female Male
Band 1 1 3 0.1% 0.4%
Band 2 48 33 2.8% 4.6%
Band 3 438 181 25.3% 25.1%
Band 4 168 33 9.7% 4.6%
Band 5 293 77 16.9% 10.7%
Band 6 418 161 24.2% 22.4%
Band 7 182 89 10.5% 12.4%
Band 8A 68 36 3.9% 5.0%
Band 8B 33 14 1.9% 1.9%
Band 8C 15 15 0.9% 2.1%
Band 8D 1 6 0.1% 0.8%
Band 9 1 0 0.1% 0.0%
VSM 5 3 0.3% 0.4%
Non Exec Director 3 3 0.2% 0.4%
Medical 56 66 3.2% 9.2%
3.2 The difference between the mean hourly rate of pay for male and female employees
Our early analysis of the mean hourly pay rate shows that there is a 15.4% difference between
average hourly pay for males and females.
Male Female % difference
Mean hourly
rate £18.16 £15.36 15.4%
Our more detailed analysis across each pay band has shown that for the majority of Trust roles
the mean gender pay gap is considerably less than 15.4%. In most pay bands, we are confident
that the average hourly pay rate for males and females is equal or within 1% of each other.
5.4
Gen
der
Pay
Gap
Rep
ort
Page 81 of 96

Board of Directors, 12 March 2018 Agenda Item 5.4
3.3 The difference between the median hourly rate of pay for male and female employees
Our early analysis of the median hourly pay rate shows that for the Trust overall there is a 7.6%
difference between hourly pay for male staff and female staff.
Male Female % difference
Median
hourly rate £14.74 £13.62 7.6%
There are more than double the amounts of female employees working in the Trust than males,
with a higher number of women working in the lower pay bands than men. This therefore plots
the median value at a lower hourly rate for females than for males.
3.4 The difference between the mean bonus pay for male and female employees
All analysis undertaken with regard to bonus payments only includes consultants who are
eligible to receive a Clinical Excellence Award and excludes all roles across the workforce that
are not eligible for bonus payments of any kind. There are only 30 staff in the Trust who were
paid this award as at 31 March 2017; 18 men and 12 women.
Our early analysis of bonus pay (CEAs) shows that there is an 11.5% difference between the
mean bonus payments for male consultants and female consultants in receipt of Clinical
Excellence Awards.
Male (Consultants) Female (Consultants) % difference
Mean bonus
payment £14063.55 £12441.66 11.5%
58
3.5 The difference between the median bonus pay for male and female employees
Our early analysis of bonus pay (CEAs) shows that there is a 16.7% difference between the
median bonus payments for male consultants and female consultants in receipt of Clinical
Excellence Awards.
Male (Consultants) Female (Consultants) % difference
Median bonus payment
£8958.00 £7465.00 16.7%
Both the mean and median gender pay gaps for bonus pay can largely be attributed to the fact
that no female consultants are in receipt of higher national awards (silver and above).
3.6 Proportion of male and female employees who were paid a bonus
Our early analysis of proportions of male and female (eligible) consultants receiving bonus pay
(CEAs) shows that there are 58 consultants eligible for CEAs currently employed by the Trust
of which 30 (45%) are in receipt of a CEA. This is shown in the table on page 4.
5.4
Gen
der
Pay
Gap
Rep
ort
Page 82 of 96
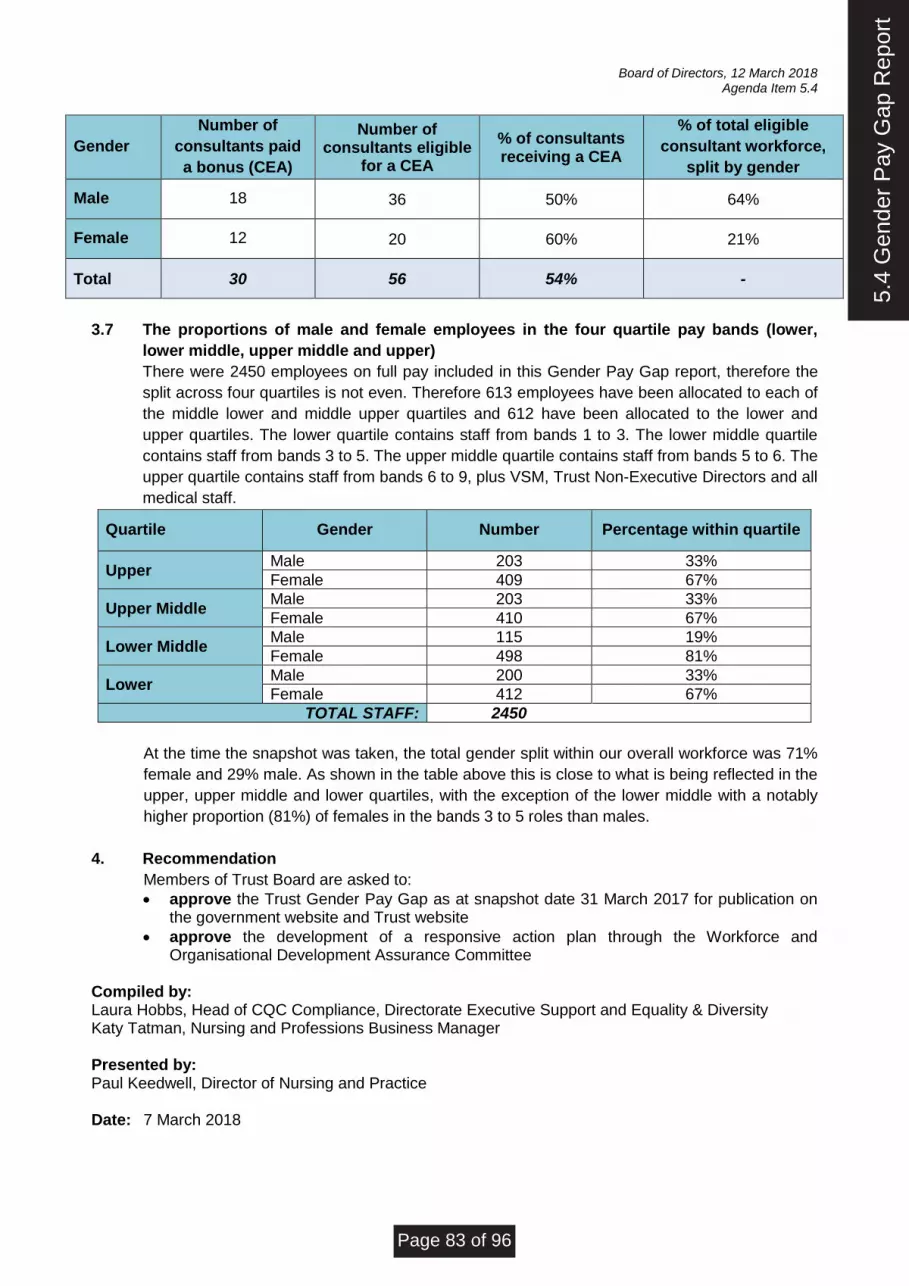
Board of Directors, 12 March 2018 Agenda Item 5.4
Gender
Number of
consultants paid
a bonus (CEA)
Number of consultants eligible
for a CEA
% of consultants receiving a CEA
% of total eligible
consultant workforce,
split by gender
Male 18 36 50% 64%
Female 12 20 60% 21%
Total 30 56 54% -
3.7 The proportions of male and female employees in the four quartile pay bands (lower,
lower middle, upper middle and upper)
There were 2450 employees on full pay included in this Gender Pay Gap report, therefore the
split across four quartiles is not even. Therefore 613 employees have been allocated to each of
the middle lower and middle upper quartiles and 612 have been allocated to the lower and
upper quartiles. The lower quartile contains staff from bands 1 to 3. The lower middle quartile
contains staff from bands 3 to 5. The upper middle quartile contains staff from bands 5 to 6. The
upper quartile contains staff from bands 6 to 9, plus VSM, Trust Non-Executive Directors and all
medical staff.
Quartile Gender Number Percentage within quartile
Upper Male 203 33%
Female 409 67%
Upper Middle Male 203 33%
Female 410 67%
Lower Middle Male 115 19%
Female 498 81%
Lower Male 200 33%
Female 412 67%
TOTAL STAFF: 2450
At the time the snapshot was taken, the total gender split within our overall workforce was 71%
female and 29% male. As shown in the table above this is close to what is being reflected in the
upper, upper middle and lower quartiles, with the exception of the lower middle with a notably
higher proportion (81%) of females in the bands 3 to 5 roles than males.
4. Recommendation
Members of Trust Board are asked to:
• approve the Trust Gender Pay Gap as at snapshot date 31 March 2017 for publication on the government website and Trust website
• approve the development of a responsive action plan through the Workforce and Organisational Development Assurance Committee
Compiled by: Laura Hobbs, Head of CQC Compliance, Directorate Executive Support and Equality & Diversity Katy Tatman, Nursing and Professions Business Manager Presented by: Paul Keedwell, Director of Nursing and Practice Date: 7 March 2018
5.4
Gen
der
Pay
Gap
Rep
ort
Page 83 of 96

Report provided: Agenda
Item: 6.2
To note:
For assurance: x Report
to: Board of Directors
For approval:
For information:
Meeting date:
12 March 2018
General Data Protection Regulations Briefing
Accountable Director(s):
Sarah Brampton, Finance Director
Presented by:
Mark A. Jones, Acting Chief Information Officer
Report author(s):
Sue Banham, Information Governance Manager, Mark A. Jones, Acting Chief Information Officer
Alignment to the Trust’s strategic aims:
Our aims:
To deliver consistently high quality care and treatment
x To ensure our services are driven by the voices of people who use them
To build a reputation as a recognised centre of excellence and expertise
x To attract and retain talented people and to create a great place to work, with a shared sense of pride and ambition
To challenge discrimination and stigma, and to champion recovery, inclusion and wellbeing
To be an efficient, thriving and successful organisation with a sustainable future
x
Purpose of report:
The purpose of this report is to provide significant assurance that the Trust will meet its obligations in being ready for the EU General Data Protection Regulation (GDPR) from 25 May 2018 and beyond.
Summary of the key issues:
The EU General Data Protection Regulation (GDPR) will become directly applicable as law in the UK from 25 May 2018. The current Data Protection Bill, which will become the Data Protection Act 2018 (DPA 2018) will fill in the gaps within the GDPR and address areas in which flexibility and derogations are permitted. The board requires assurance that the Trust will be compliant by 25 May 2018.
Recommendations:
4.1 Accept and note the contents of this report and the significant assurance. 4.2 Support the review of information assets and information flows and DPIAs as a matter of priority within the Trust, including that all systems being approved by the IM&T Strategy Group. 4.3 Recognise that resources have been made available on the basis of current assessment which may be subject to change as implementation of the plan progresses.
Report previously presented to:
Committee/Group: Date: Report title: Outcome/action:
Summary of compliance implications:
If the Trust is not compliant with the new GDPR legislation there is a risk that it will receive significant fines and associated reputational damage.
Does this report provide assurance in respect of a new / existing risk/s?
Type of risk/s Existing Corporate Assurance Risk Register
Level of Assurance and trend: 1 to 10
Significant Limited None
x
6.2
Gen
eral
Dat
a P
rote
ctio
nR
egul
atio
ns B
riefin
g
Page 84 of 96

Board of Directors, 12 March 2018 Agenda Item 6.2
Authors: Susan Banham, Information Governance Manager, Mark A. Jones, Acting CIO
DEVON PARTNERSHIP NHS TRUST BOARD OF DIRECTORS
12 March 2018
GENERAL DATA PROTECTION REGULATIONS (GDPR) BRIEFING
1. Situation 1.1
The purpose of this SBAR is to provide significant assurance that the Trust will meet its obligations in being ready for the EU General Data Protection Regulation (GDPR) from 25 May 2018 and beyond.
1.2 The EU General Data Protection Regulation (GDPR) will become directly applicable as law in the UK from 25 May 2018. The current Data Protection Bill, which will become the Data Protection Act 2018 (DPA 2018) will fill in the gaps within the GDPR and address areas in which flexibility and derogations are permitted. Whilst GDPR will not be directly applicable in the UK post Brexit it is expected that the DPA 18 will ensure continuity and maintain a data protection regime in the UK equivalent to that introduced by the GDPR which will continue to be applicable throughout EU member states.
2. Background 2.1
IM&T and in particular the Safer Information Team have been working on generating a gap analysis and planning for GDPR compliance since October 2017. A detailed plan is in place and dedicated resource has been allocated to GDPR.
2.2 There have been delays in the publication of specific guidance but additional guidance is now becoming available through the Information Governance Alliance (IGA) and will continue to be provided from March.
2.3 The Acting Chief Information Officer for the Trust attended the Information Governance NHS Summit 2018 on 23 February 2018, with the focus of the summit being on ‘Ensuring Compliance with GDPR in Health and Social Care’. The Summit provided significant assurance as to the actual requirements and confirmed Devon Partnership NHS Trust was ahead of schedule in comparison to other attendees. This was due to Devon Partnership Trust showing significant adherence the existing Data Protection Act through its compliance with the IG toolkit that has achieved level two on all requirements for a number of years
3. Assessment 3.1 At the Information Governance NHS Summit 2018, Dawn Monaghan, Chair of the
Health and Social Care Working Group on GDPR and Head of Data Sharing and Privacy at NHS England made the following statements that can provide DPT with significant assurance.
• Any organisation that is meeting the Data Protection Act today, particularly those that have been doing the IG toolkit for many years, will already be 70-75% complete.
6.2
Gen
eral
Dat
a P
rote
ctio
nR
egul
atio
ns B
riefin
g
Page 85 of 96

Board of Directors, 12 March 2018 Agenda Item 6.2
Authors: Susan Banham, Information Governance Manager, Mark A. Jones, Acting CIO
4. Recommendations 4.1
Accept and note the contents of this report and the significant assurance provided from the 2018 Information Governance NHS Summit and work already undertaken by IM&T and specifically Safer Information.
4.2 Support the review of information assets and information flows and DPIAs as a matter of priority within the Trust, including that all procured and developed systems are approved by the IM&T Strategy Group.
4.3 Recognise that resources have been made available on the basis of current assessment which may be subject to change as implementation of the plan progresses.
Compiled by: Susan Banham, Information Governance Manager Mark A. Jones, Acting Chief Information Officer Presented by: Mark A. Jones, Acting Chief Information Officer Date: 6 March 2018
• Any organisation already adhering to existing Information Commissioner Office codes will be a further 10-15% compliant.
• “There will not be a fleet of drones swooping to every health and social care organisation on May 25th to ensure compliance. If any organisation is visited by the ICO and they have a gap analysis and a plan to ensure compliance from May 25th and over the following 12-18 months; they will be fine.”
3.2 Devon Partnership Trust meets the existing Data Protection Act, adheres to the ICO codes and has a gap analysis and plan for compliance. The Safer Information team are now concentrating on the remaining 15% of work that needs to be done for May 25th and the next 18 months.
3.3 3.4 3.5
The fundamental principles around Data Protection are not new and the new legislative framework builds on existing requirements. The headline impacts, response and planned actions are detailed in Appendix A. To provide further assurance, two audits are planned and have specific references to GDPR compliance:
• In March 2018, Internal Audit will audit the IG Toolkit.
• In May 2018, A voluntary Information Commissioners Office (ICO) audit will be undertaken.
GDPR compliance will continue to be monitored through the IM&T Strategy Group, SMB and FIC.
6.2
Gen
eral
Dat
a P
rote
ctio
nR
egul
atio
ns B
riefin
g
Page 86 of 96

Board of Directors, 12 March 2018 Agenda Item 6.2
Authors: Susan Banham, Information Governance Manager, Mark A. Jones, Acting CIO
Appendix A – GDPR Headline Impacts and Actions
Headline Impact Response
By 25 May 2018
From 25 May 2018
Organisation obliged to demonstrate that they comply with the new law
The Trust has demonstrated compliance with the Data Protection Act 1998 with the IG toolkit and has achieved level two on all requirements for a number of years. The toolkit is to be replaced by a new ‘Data Security and Protection toolkit’ (DSPT) from April 2018 and the Trust is working towards compliance with the new standards which will reflect the changes arising from the new legislation.
The Trust has a detailed plan and gap analysis.
The gap will be met through the actions planned over the next 18 months.
Significantly increased penalties possible for any breach of the Regulation – not just data breaches.
Failure to comply with the new legislation can lead to significant financial penalties. The broadcast fines of between 2% and 4% of global turnover (up to 20m Euros) is only for private businesses. The ICO has not yet decided if this will apply to health and social care organisations. There are proposed higher fines for incidents involving: · P1 fair and lawful · Consent · Misuse of special category data · Data subjects rights · Transfer to 3rd Countries DPT have never received an improvement notice or a fine in regard to any incident related to the above, so the overall risk is low.
Continue best practice.
Monitor compliance and continue best practice.
Legal requirement for security breach notification
GDPR includes a specific requirement about prompt reporting of incidents. The Trust has robust processes already in place and it is not anticipated that there will be any significant changes necessary.
Continue best practice.
Monitor compliance and continue best practice.
Requirement to keep records of data processing activities
As part of compliance with the IG Toolkit, DPT currently maintains an asset register that contains details of systems and Information Asset Owner details. This register is currently being updated to contain the required extra information for GDPR.
Amend existing Asset Register and populate
Update and review Asset Register on a regular basis
Appointment of Data Protection Officer mandatory for all public authorities
Under the new legislation it will be mandatory for the Trust to have an appointed Data Protection Officer (DPO) with a specific role and associated responsibilities. Whilst the Chief Information Officer is currently nominated in Trust policy as DPO, the appropriateness of this will require review following further guidance. This will be the subject of a separate specific paper to be presented at a future meeting.
A DPO will be formally appointed.
DPO to perform duties and report through the Trust, up to the board.
Data Protection Impact Assessment required for high risk processing
All systems should employ privacy by design and privacy by default. To ensure on-going compliance the Trust will need to update and implement processes around implementation of any changes to the ways in which information is used. There will need to be a robust system for ensuring that any new information systems implemented are reviewed by the DPO and Data Protection Impact Assessments (DPIAs) (The replacement for the Privacy Impact Assessment) carried out. Highly complex DPIAs must be signed off by the ICO. This is the area of work that is being concentrated on for compliance by the 25th May 2018 and work is currently underway to inform the Information Asset Owners of their responsibility in this regard. Any existing or newly procured system or system change, along with any in-house developments will need to have a DPIA. A recommendation is for SMB and the Trust Board to agree to the measure that all systems require approval from the IM&T Strategy Group before proceeding.
All DPIAs complete for all existing systems and those in development will be reviewed by the IM&T Strategy Group and signed off by the DPO with any that are highly complex going to the ICO for sign-off.
All new systems (procured or developed) will have a DPIA and it be reviewed by the IM&T Strategy and signed off by the DPO with any that are highly complex being sent to the ICO for sign-off.
Data The new legislation requires that there be a lawful basis for processing of personal data Data mapping Plan met to
6.2
Gen
eral
Dat
a P
rote
ctio
nR
egul
atio
ns B
riefin
g
Page 87 of 96

Board of Directors, 12 March 2018 Agenda Item 6.2
Authors: Susan Banham, Information Governance Manager, Mark A. Jones, Acting CIO
protection issues must be addressed in all information processes
and this lawful basis is required to be documented. The requirement is not new and mirrors the previous requirement to satisfy one of the ‘conditions for processing’ under the Data Protection Act 1998. The difference is that the GDPR places more emphasis on being accountable for and transparent about the lawful basis for processing. It will be necessary to check and update existing records and map all data flows to ensure that a lawful basis is identified for each. This is the most significant piece of work identified as being necessary for the Trust in terms of the scope of the review, the resource required and also in terms of timescale. It is worth noting that DPT are one of only 3 organisations present at the IG NHS Summit to have already started this exercise. We will also review contractual arrangements with system providers to ensure that they are compliant with GDPR and identify any gaps or risks. Safer Information will work with Procurement on this exercise and provide the appropriate clauses when given by the ICO/IGA Additional resources have been made available to Safer Information to ensure GDPR compliance.
exercise started and aligned to asset register. All new contracts will have GDPR compliant elements in place. Renewal of contracts will also have the appropriate clauses.
record all information flows over the next 18 months. All existing contracts will be amended to ensure the appropriate clauses are contained.
Specific requirements for transparency and fair processing
The Trust must inform people in advance about the lawful basis for processing their data. There are already processes in place to ensure that people are informed about the ways their information is used. The Trust privacy notice as per the “Your information” leaflet will be updated and the changes publicised. This cannot be finalised until the lawful basis is confirmed. Safer Information will be working with communications and specific teams/functions on this element as guidance becomes available. Mandatory IG training and induction is being amended to ensure all staff know about the required changes and ensure compliance. The new legislation brings changes to Subject Access Requests (SARs). The right to request access to their own information is already available to any individuals and the Trust has robust processes to ensure compliance. The timescales for compliance are reduced under the GDPR from 40 days to 30, although Department of Health recommendations are to process requests limited to health records within 21 days. Review of the overall process is required to reduce the administrative burden of printing and checking records and thus improve compliance times. In addition the options for scanning of archived paper health records are being considered.
Privacy notices and other communications will be provided to patients, service users and staff as required. Training will be updated and provided. Opportunities to reduce the SAR process will be identified and implemented.
Communications will continue and follow any further guidance in actual application of the law. Mandatory training rates will be improved with a particular focus on bank staff and assigned staff whose compliance rates have been historically low.
Tighter rules where consent is the basis for processing.
The main message that was repeated through the IG NHS Summit was to move away from consent for the use and flow of information as it creates many more issues with the increased rights of the data subject. The main being the “ability to demonstrate consent” and the right to withdraw consent being “as easy to withdraw as to give”. This will create a significant administrative and costly burden on trusts and would be extremely difficult to actually implement. GDPR allows for the easier sharing of information through new articles 6 and 9 and these are revised conditions for processing data and for processing non-special personal data: •Contract •Legal obligation •Vital interest of data subject •Public interest/task •Legitimate interest (can no longer be used by public authorities) •(Consent) (not recommended to be used). Conditions specific to health & social care: Art 9(2)(h): Processing necessary for purposes of preventive or occupational medicine, for assessment of working capacity of the employee, medical diagnosis, the provision of health or social care or treatment or the management of health or social care systems and services on the basis of Union or Member State law or pursuant to contract with a health professional and subject to the conditions and safeguards referred to in paragraph 3 [obligations of secrecy]
Identify consent for data processing and remove all instances and replace with appropriate clause.
Continue to monitor compliance.
6.2
Gen
eral
Dat
a P
rote
ctio
nR
egul
atio
ns B
riefin
g
Page 88 of 96

Board of Directors, 12 March 2018 Agenda Item 6.2
Authors: Susan Banham, Information Governance Manager, Mark A. Jones, Acting CIO
The Safer Information team are looking for where any current models of consent for the processing of data apply and will remove and replace these alongside other departments with the appropriate application of articles 6 and 9.
6.2
Gen
eral
Dat
a P
rote
ctio
nR
egul
atio
ns B
riefin
g
Page 89 of 96

Report Summary
Agenda item number: 7.2
Report provided: Agenda
Item: Corporate Assurance Framework
To note:
For assurance: X Report
to: Board of Directors
For approval:
For information: Meeting
date: 12 March 2018
CORPORATE ASSURANCE FRAMEWORK
Accountable Director(s):
Melanie Walker, Chief Executive
Presented by:
Fiona Barr, Corporate Governance Advisor
Report author(s):
Fiona Barr, Corporate Governance Advisor
Alignment to the Trust’s strategic aims:
Our aims:
To deliver consistently high quality care and treatment
X To ensure our services are driven by the voices of people who use them
X
To build a reputation as a recognised centre of excellence and expertise
X To attract and retain talented people and to create a great place to work, with a shared sense of pride and ambition
X
To challenge discrimination and stigma, and to champion recovery, inclusion and wellbeing
X To be an efficient, thriving and successful organisation with a sustainable future
X
Purpose of report:
The purpose of the report is to provide an update on the Corporate Assurance Framework (CAF) to the Board of Directors.
Summary of the key issues:
The CAF is a working document which is subject to regular review. In February, the Executive Leads reviewed the controls, controls assurance and risk scoring for each risk on the CAF and updated risks were presented to the assuring Committees in March 2018. As a result, one of the risks (S32: IF the Trust does not review and comply with best practice guidelines (NICE) THEN patients may not receive quality health care, as required by commissioners) was removed from the CAF as the Quality & Safety Committee was sufficiently assured the information presented in the Clinical Effectiveness and Assurance Group Report which indicated that this no longer presented a risk. Twenty risks remain on the CAF; seven risks are rated as significant (9-12) post mitigation and the remainder moderate or low. There are no risks rated high (15-25) post mitigation. The top risks on the CAF are highlighted in yellow below. Broadly they relate to workforce, delivery of change programmes, under-commissioned services and some specific issues relating to services or estates.
Ref Risk Theme Type of Risk
Residual Risk Score
S35 Staffing levels Workforce Significant
S37 Gender Services – access for patients
Operational Significant
7.2
Cor
pora
te A
ssur
ance
Fra
mew
ork
Page 90 of 96

Board of Directors, 12 March 2018 Agenda Item 7.2
SU35 Workforce skillmix Workforce Significant
SU36 Staff recruitment and retention Workforce Significant
SU37 Achievement of 2017-18 cost improvement plans and knock-on impact to 2018-19
Financial Significant
SU41 Construction of Mother & Baby Unit Operational Significant
AS Dual diagnosis of mental illness and substance abuse
Operational Significant
S25 Deprivation of Liberty Operational Moderate
S33 Demand (admission to adult & older patient wards)
Operational Moderate
S34 Staff health & wellbeing Workforce Moderate
S36 Provision of Eating Disorder Service Operational Moderate
S38 Gender Services – governance arrangements
Operational Moderate
S39 Ligature reduced cells for prisoners Operational Moderate
SU38 SMART programme and impact on delivery of 2017-18 cost improvement targets
Financial Moderate
SU39 Achievement of 2017-18 financial plan
Financial Moderate
SU42 Demand (admissions to High Dependency in patient services)
Operational Moderate
SU43 Demand (Psychiatric Intensive Care Unit)
Operational Moderate
T1 Patients held on waiting lists Operational Moderate
SU44 Implementation of General Data Protection Regulations
Operational Low
ES36 Outsourcing arrangements (collapse of Carillion)
Operational Low
In the Trust’s drive to constantly review and improve its processes, the CAF is currently the subject of an expert external review and revised principal risk register will be presented to the Board in May 2018 following discussion at the Audit Committee.
Recommendations:
The Board should be assured that risks on the Committee are driving the agenda of the Board (GDPR briefing) and Committees (Clinical Effectiveness and Assurance Group Report to Quality & Safety Committee) and the Trust’s risk profile is changing as a result.
Report previously presented to:
Committee Review: Date:
Finance & Investment Committee, Workforce and Organisational Development Assurance Committee, Quality & Safety Committee, Audit Committee
March 2018
Summary of compliance implications:
The Corporate Assurance Framework is updated on a regularly and forms part of the Trust’s system of internal control and risk management.
Does this report provide assurance in respect of a new / existing risk/s?
Type of risk/s Existing Corporate Assurance X Risk Register
Level of Assurance and Trend: 1 to 10
Significant Limited None
7.2
Cor
pora
te A
ssur
ance
Fra
mew
ork
Page 91 of 96

ID Activity/Objective/
Risk Description
Contributory issue Source of risk Exec Risk
Type
Prev Month's
Risk
Inherent
Risk (risk if
no controls
were in
place, ie
pre-
mitigating
actions)
Residual Risk
(risk that
remains after
controls are
taken into
account, ie
post-
mitigating
actions)
Current Assurance
(Evidence of effective actions)
Gaps in Assurance
(Where evidence is inadequate
of our control and systems)
Current Controls
(Actions being taken to mitigate risks)
Gaps in Control
(Where systems of control are
inadequate)
Committee Action Plan
(Evidence of action to address control/assurance gaps)
S25 Added July 2015
IF DoLS assessments from
the Supervisory Body
DoLS team are delayed
THEN patients who lack
capacity may be deprived
of their liberty on inpatient
units whilst awaiting
assessment.
RISK APPETITE -
AVERSE
1. Recent Supreme Court ruling on
what constitutes a deprivation of
liberty; patients on inpatient units that
lack capacity are now deprived of
their liberty and require DoLS to
safeguard their rights.
2. Local Authority DoLS do not have
sufficient number of DoLS assessors
to manage the demand.
Paul Keedwell
(Carole Camps)
O/C Significant
(4x3=12)
Significant
(4x3=12)
Moderate
(4x2=8)
1. MHA office is aware of patients who have urgent DoLS
authorisation and liaises with ward and DoLS team.
2. MHA office offers training for ward managers and those
completing DoLS urgent authorisation, ensuring immediate
situation described; especially distress/agitation from patients
who want to leave
3. Expiry dates are monitored.
4. RMS report is submitted for patients that do not have a DoLS
assessment in the 14 day period and are subject to unauthorised
deprivation of liberty.
5. MHA office updates list of patients on DoLS list and advises
DoLS team.
6. CCG guidance on DoLS circulated to inpatient teams.
7. Assistant Director of Social Services triage assessment tool
sent to Responsible Clinicians to aid completion of urgent
authorisation.
8. Weekly information sent to all patients.
1. The Supervisory Body
manages workload for DoLS
assessments and although
psychiatric inpatient units are
prioritised there are insufficient
DoLS assessors to cope with the
demand.
1. On-going communication between MHA office and DoLS
team regarding individual patients on waiting list.
1. The Supervisory Body is
responsible for managing DoLS
assessments.
1. Q&S
2. SMB
3. SC
1. Contact made with responsible body if person needs increase in accordance with the DoLS triage
system. Target date: Completed.
**Timescale to achieve residual risk: Jan 2016, Apr 2018 (significant impact will not be made until
planned legislative change comes into effect. Law Commission published proposed legislative changes
13/03/17, proposing that no individual in a mental health bed should be subject to LPS but detained under
MHA. Implications of changes in legislation unlikely to come into effect until 2019/20).
Key milestones:
1. Regular meetings with DoLS team to plan and prioritise. Ongoing.
2. MHA office to maintain updated lists of patients subject to delayed DoLS applications. Ongoing.
S33 Added November 2016
(S17 incorporated in July
2017)
IF we are unable to meet
the demand for
admissions to acute adult
and older peoples wards
THEN patients may suffer
harm/delay in treatment
(particularly out of hours
care or may not be able to
access elements of the
urgent care pathway in
local area).
RISK APPETITE -
CAUTIOUS
1. Insufficient inpatient capacity
(externally validated by PenChord,
University of Exeter) leading to high
occupancy and Out of Area
Placements
2. Insufficient 24 hour home
treatment capacity.
3. Alternatives to admission such as
Crises Houses and Step-up and -
down facilities across Devon
4. CRHT home treatment capacity is
insufficient due to high volume of
referral for assessments (80% of
CRHT capacity) with low conversion
rates to home treatment (20%)
5. Delays in accessing panel funding
(delayed discharge of care).
6. System cannot be flexed quickly
to open additional beds (unable to
source additional qualified staff).
7. National availability of beds and
local challenges associated with
patient flow.
8. Lack of investment and gaps in
service compared to best in class.
1. Reduction of DPT beds due to
quality and safety concerns,
difficulties with recruitment and
retention of staff
2. Patients morbidity and acuity
increased due to use of of illict
substances
3. Increase in self-injurous and high
risk behaviours associated with
personality disorders.
4. Number of delayed discharges high
across acute and older peoples'
wards which negatively affects length
of stay and bed availability.
5. Limited investment and whole
acute care pathway commissioning in
NEW Devon CCG area.
David
Somerfield
(Karl Vile)
S/C/O/F High
(5x4=20)
High
(5x4=20)
Moderate
(4x2=8)
1. Flow and capacity analysis (PenCHORD and NHSI) completed
whihc has informed ACP project plan.
2. System blockages escalated to senior management for
authorisation for urgent funding eg for external beds or supported
accommodation
3. CQC improvement to 'Good' for ACP service.
4. CCGs invenstment of £1m 17/18 now funding OAPs, fully
engaged in the Acute Care Programme, have agreed and
seeking more inpatient capacity is required and seeking
investment for alternatives to admission
5. Panel processes have been reviewed and re-engineered to
enable better flow. Reduction in DToC
6. Crisis concordat signed.
7. Additional investment has enabled each adult and older adult
ward to have a Discharge Co-ordinator with subsequent reduction
in delayed discharges and DToC.
8. SMART ACP Programme governance structure includes
Social Care and commissioner representation.
9.Prioritised ACP project programme of work underway.
10. STP ACP workstream in place.
11. Bed Stock analysis to ACP Board and Devon A&E Board
2017
12. STP developing outline Business Case for First Response
Service. Draft paper presented (Sep 2017).
1. Home treatment capacity
continues to be limited.
2. No increase in crisis and step
down facilities across Devon.
3. Lack of demand management
at primary care interface.
4. Fragmented discharge
pathways involving external
organisations.
5. Continuing high occupancy
rates and no reduction in OAPs
6. Funding for expanding Torbay
CRHT's operating hours
withdrawn. As at Oct 2017, North
Devon expanded hours (to 22:30)
and Exeter recruited staff to
expand until midnight. Expansion
will form part of a wider CRHT
redesign project.
1. Monthly SMART ACP Programme Board in place.
2. Monthly Devon A&E Delivery Board in place.
3. ACP project plan in train.
4. STP MH Steering Group and ACP project stream in place.
5. Directorate Delivery Group in place.
6. Acute Care Pathway Group developed action plan to
support development of clear and robust care pathway.
7. Executive oversight to hold Directorate to account.
8. Daily bed management calls and ward reviews.
9. Focus on active management of discharges and delayed
discharges.
10. Multi-agency workplan - Devon MH Steering Group (CCG
chaired).
11. Reviewing panel processes to expedite discharge.
12. Recruitment of additional CRHT staff and Discharge Co-
ordinators.
13. Projects for step-down and redesign of long term
rehabilitation services being considered in Directorate delivery
plans. 14. 14.
Single Point of Access Business Case agreed. Phase 1 of
SPA operational by May 2018.
1. Organisation of other urgent
care services where the Trust has
no influence or control, such as
ED, Emergency Social Services
Duty Teams.
2. Lower control over LoS and
discharge coordination in third
sector providers / out of area
placements (tendency to result in
longer LoS and cost). Improved
partnership working identified.
3. Onward care and Social Care
packages causing delays and
pressure on beds.
4. Lack of clear financial envelope
for Acute Care Pathway linked to
aim of becoming recognised
Centre of Excellence and CQC
'Outstanding' organisation.
5. Concern over level of
Directorate resource allocated to
deliver change at pace.
1. Q&S
2. SMB
3. Q&S
4. Devon A&E
Delivery Board
5. SMART
ACP
1. Daily focus on active and delayed discharges. Target date: Complete
2. Multiagency Monthly DPT SMART ACP Programme Board. Target date: Complete
3. Bed Stock paper Target date: complete (Aug 2017). Steering Group actively exploring options to
increase bed capacity within Devon. Met with Livewell Jan 18. Expansion within Plymouth excluded.
Meeting with alternative acute inpatient provider to be scheduled Feb 18
4. Discharge Co-ordinator posts approved (Aug 2017) and in post. DTOC reduced to 8%. Target date:
Complete.
5. SPA Business Case approved Target Date; Complete. SPA will help reduce CRHT assessment
demand tough more effective triage. SPA Project iunderway. Aim to have Phase 1 of SPA operational by
May 2018. This is a complex multi-streamed piece of work to ensure mitigations are in place to risk stratify
patient access. Target date: Dec 2018 to be fully operational.
6. Agreement at SMART ACP Board that STP lead on developing Outline Business Case for First
Response Service. Target Date: Complete. Awaiting authorisation form STP to develop full buisness case.
8. Exeter Mental Health Place of Safety refurbishment due to commence Feb 18. Target Date: March 18.
Refurbishment of the Cedars Ward paper for presented at SMB (Dec 2017). Further options appraisal to
be developed. Target date: April 2018
**Timescale to achieve residual risk: Dec 2018
Key milestones - as above
S34 Added March 2017
(previously S12)
IF the Trust does not take
effective action to promote
the health and wellbeing of
our staff THEN this could
adversely affect sickness
levels and our ability to
deliver high quality care
and treatment.
Additionally, the experience
of staff across the
organisation will impact our
work to achieve the aim of
attracting and retaining
talented people and
ensuring that DPT is a
great place for people to
work.
RISK APPETITE - OPEN
1. Increasing demand for Trust
services at a time when we are
carrying vacancies as well as
working to an agency use cap. This
creates pressures for current staff
and if this is not managed well then it
could impact on staff health and
wellbeing.
1. Large scale change across the
Trust due to external and internal
strategic drivers. New ways of
working are required to ensure the
Trust's services are sustainable. Our
staff engagement approach needs to
involve, motivate and support staff
and harness their support for
implementing the Trust Strategy.
2. Cross referenced to SU33 (now
complete/archived).
Helen England
(Jess Hobbs)
S/C/O Significant
(3x4=12)
Significant
(3x4=12)
Moderate
(3x2=6)
1. DGB sickness monitoring.
2. Revised Employee Assistance Programme (EAP) service
specification. Awarded CIC new EAP contract.
3. Promotion of OH service, physiotherapy services etc.
4. CQUIN action plan.
5. Corporate Health & Wellbeing Programme Board formed
supported by an advisory and delivery group.
6. Partnership with LPF - staff health and well-being is an agreed
priority for partnership working.
7. Use of HWB survey results and National Staff Survey results.
8. Piloting use of stay interviews to improve retention which may
identify health and well-being themes
9. Use of Exit Interview data.
10. Use of ESR Business Intelligence. Link Exit Interviews to ESR
to improve robustness.
11. Use of Directorate Action Plans.
12. Dashboard being developed to monitor sickness.
13. Triangulate OH, EAP and ESR following new EAP contract.
14. 'Our Journey' Staff Roadshows 2017 included Health and
Wellbeing theme.
1. Implementation of Trust Absence Policy.
2. Regular review of plans, monitoring and exception
reporting.
3. Quarterly CQUIN reports and programme reports to
WODAC and SMB.
4. Staff Health and Wellbeing Programme governance
structure.
1. Reporting system that uses
appropriate data to measure
improvement in staff health and
well-being
1. WODAC
2. SMB
1. Review Health and Wellbeing Programme 2017. Target date: May 2017, Aug 2017. Programme
endorsed by SMB (Sep 2017). Completed.
2. Implementation of Staff Health and Wellbeing Programme, overseen by Health and Wellbeing
Programme Board. Agreed membership for Programme Board (Nov 2017). Completed. A Health and
Wellbeing Champions meeting held on 24 Nov 2017 engaged cross section of staff and explored how the
role could be utilised to support the delivery of the programme. Completed. 4. Mediation, De-briefing and
Team Support model is in development. Target date: March 2018 5. Pathways for staff needing acute
mental health support or psychological therapy are being developed in partnership with occupational
health. Target Date April 2018 6. Work is in progress to develop programme measures to monitor
improvement. Target date April 2018
**Timescale to achieve residual risk: Apr 2018
S35 Added May 2017,
redefined September
2017
IF the inadequate levels of
staffing for nursing and
medical staff within
inpatient units are not
resolved THEN this will
negatively affect the safety
and quality of the services
provided. Additionally, this
may result in a temporary
suspension of services.
RISK APPETITE -
AVERSE
1. Recruitment of Consultant
Psychiatrists national issue.
2. Recruitement of registered nurses
national issue.
3. Geographic location of Trust
services.
4. Limited agency cover available.
1. DGB review and escalation.
2. Meadowview.
3. Haldon.
4. Cedars.
5. Langdon.
David
Somerfield
(Sue Smith)
C/O
High
(3x5=15)
High
(3x5=15)
Significant
(3x3=9)
1. Escalated through DGB and Executive Team.
2. Job reprofiling.
3. Recrutiment initiatives.
4. Substantive staff on Trust Bank and substantive and locum
consultants in place
5. Commisoners aware of challenges - discussing options.
1. Major difficulty in sourcing staff
despite a number of actions and
initiatives.
1. Senior management and Executive oversight of staff rotas.
2. Business Manger B6 post, freeing up clinical time - pilot
and review.
3. Centralised recruitment to ensure applicants above the line
are recruited.
1. National shortage of key roles,
including nursing and medical.
1. DGB
2. SMB
3. Q&S
1. Recruitment and Retention Strategy in place with regular progress updates received through SMB,
WODAC and Executive Team meetings. Target date: reviewed monthly.
2. Planned OPMH medical staffing reconfiguration has not achieved resolution of north Devon inpatient
post but locum currently in place.
**Timescale to achieve residual risk: Dec 2018
Key milestones - as above
CORPORATE RISK REGISTER AND ASSURANCE FRAMEWORK - JANUARY 2018
Ref: Combined Assurance Framework Corporate Risk Register Page 1 of 5
7.2
Cor
pora
teA
ssur
ance
Page 92 of 96

ID Activity/Objective/
Risk Description
Contributory issue Source of risk Exec Risk
Type
Prev Month's
Risk
Inherent
Risk (risk if
no controls
were in
place, ie
pre-
mitigating
actions)
Residual Risk
(risk that
remains after
controls are
taken into
account, ie
post-
mitigating
actions)
Current Assurance
(Evidence of effective actions)
Gaps in Assurance
(Where evidence is inadequate
of our control and systems)
Current Controls
(Actions being taken to mitigate risks)
Gaps in Control
(Where systems of control are
inadequate)
Committee Action Plan
(Evidence of action to address control/assurance gaps)
S36 Added May 2017
IF there is not a significant
investment into the
development of a
Community Eating
Disorder Service THEN
this could negatively affect
individuals' health,
wellbeing and safety,
leading to inappropriate
admissions and
readmissions to acute
general and mental health
services.
RISK APPETITE -
AVERSE
1. Lack of investment in Community
Eating Disorder Services and
demand and capacity mismatch in
adult community teams.
2. Lack of appropriate care
pathways, realistic to the needs of
the local population.
3. High number of local university
students whose needs cannot be
fully met.
4. Over reliance on specialist
inpatient beds.
1. HSO report into historic death of a
person using our services (2010).
2. Directorate Risk Register.
David
Somerfield
(Ann Richards)
C/O/F High
(4x4=16)
High
(4x4=16)
Moderate
(4x2=8)
1. Provision of a limited consultation and advice service to mental
health teams from Haldon team to provide advice and guidance
to CMHTs, acute hospitals and GPs
2. Evaluation of the Community Eating Disorder consultation
advice service which has been presented to SMB.
3. Establised pathways in Exeter/Torbay for admission to acute
hospitals for those with acute physical health presentations.
4. Adult Mental Health Care Co-ordinators managing a significant
number of individuals within the community.
5. Training for Adult Mental Health teams across Devon.
6. Trust Executive have fromally raised the risk of an insufficient
community eating disorders service with CCGs.
1. Adult Mental Health Care Co-
ordinators managing significant
number of individuals within the
community setting. Care Co-
ordinators feel inequipped and
limited in skills set.
2. Limited specialist community
provision restricted to consultation
and advice.
3. Increased demand for
community provision as evidenced
through referral data to
community service.
4. Readmission rates to Haldon of
Devon clients.
1. Incident reporting will highlight emerging risk trends
2. Adult Mental Health services working with a significant
number of patients with eating disorders
3. Establishment of psychological therapy pathway for
individuals discharged from Haldon.
4. Risk management and assessment process.
5. Training delivery of physical complications of eating
disorders, signs and management.
6. Advice and consultation via CEDS service.
1. Effectiveness of interventions
provided by Adult Mental Health
Services. Some GP practices now
refusing to share care.
2. Access to psychological therapy
for individuals managed in
community.
3. Restricted access to specialist
eating disorder services.
4. Lack of day programme/group
work provision.
1. DGB
2. SMB
3. Q&S
1. Ongoing provision of a limited eating disorder service. Target date: Complete
2. Develop Business Case for fully funded Community Eating Disorder Service. Business Case presented
at Business Development Board and SMB in Nov 2017. Target date: Nov 2017. Complete.
3. Review new NICE Guidance and undertake Provider Compliance Assessment to identify areas that
require development and share assessment with CCGs. Target date: Feb 2018.
4. CCG developing a business case inconjuntion with DPT and Livewell with stated intention of
commissioning an eating disorders community service 2018. Target date: Mar 2018
**Target date to achieve residual risk: December 2018
Key milestones:
1. Deliver a fully funded Community Eating Disorder Service - December 2018.
S37 Added July 2017
IF people cannot access
gender identity services in
a timely way THEN people
may experience
psychological distress and
have a poor experience of
the services.
RISK APPETITE-
CAUTIOUS
1. High levels of referral to a lmited
number of GICs nationally.
Substantial waiting lists in all clniics.
1. Long waiting list for accessing the
service (>900 people).
2. Once in service there are delays for
medical assessment due to available
staff resource.
David
Somerfield
(Ann Richards)
C/O High
(4x4=16)
High
(4x4=16)
Significant
(4x3=12)
1. National specification released on 11 Jul 2017 which clearly
describes what the service should deliver.
2. The DPT care pathway redesign and recovery plan in place
following full review.
3. New senior service manager in post overseeing recovery plan.
4. Waiting list review and projections in place
5. New substantive posts have been recruited to.
1. Improve the waiting list position
and resolve any governance
concerns.
1. Senior operational view of productivity.
2. Senior psychiatric input into team meetings.
1. Psychiatric medical capacity 1. DGB
2. SMB
3. Q&S
1. Consideration being given to managing a single waiting list. Target date: Mar 2018.
2. Recruitment to Care Navigator posts in line with new service specification. Target date: Oct 2017, Dec
2017.
3. Action plan following internal review in place. Review Action Plan Mar 2018. Target date: Mar 2018.
**Timescale to achieve residual risk: Mar 2018
Key milestones :
1. Reduction in internal waits.
2. Recruitment to posts.
S38 Added July 2017
IF the inadequate gender
governance arrangements
are not addressed THEN
the Trust may not be
assured that it is delivering
a high quality and safe
service.
RISK APPETITE-
CAUTIOUS
1. Concerns raised about governance
of the service through a
whistleblowing concern.
David
Somerfield
(Ann Richards)
C/O Significant
(4x3=12)
Significant
(4x3=12)
Moderate
(3x2=6)
1. Investigation into governance raised through whistleblowing.
Investigation completed - feedback to staff ongoing and actions
from review to be taken forward via implementation plan.
2. Service governance meeting established.
3. Risk assessment training for all staff timetabled.
4. New care navigator roles recruited to.
5. Engagement event held with staff relating to psychiatrist role.
1. Investigation to report clarity on
any potential issues.
2. Implementation plan to be
actioned.
1. New service governance meeting. 1. Review effectiveness of new
service governance meeting.
1. DGB
2. SMB
3. Q&S
1. Risk assessment training for all staff timetabled. One training session completed. Target date: Oct
2017. Completed.
2. Implementation plan to be progressed. Target date: Dec 2017.
**Timescale to achieve residual risk: Mar 2018
Key milestones :
1. Outcome of investigation and next steps.
2. Delivering of training.
3. New staff in post.
AD Added January 2018 If the
Trust does not ensure that
patients with a dual
diagnosis of mental illness
and substance abuse do
not receive care in line with
good practice, there may
be serious incidents.
1. The Trust has developed good
practice pathways for patients with a
dual diagnosis but there is limited
evidence that these are being
followed in practice.
2. NHS England required assurance
by Janury 28th 2018 that the Trust
has taken action to improve its care
of paient swith a dual diagnosis.
1. An independent homicide review by
the Health And Social Care Advisory
Service is shortly to be published
which finds that a patient who has
been convicted of homicide did not
receive care that met NICE guidelines
for schizopenai or substance abuse.
2. 2017's annual audit of dual
diagnosis found that joint working is
happening between the services but
could be developed further and more
consistently.There were
inconsistencies with the amount of
evidence documented of joint care
planning between the services and
service users, joint agency reviews
with service users, the sharing of risk
assessments and joint agency
reviews of the initial risk assessments.
Paul Keedwell/
dr Gavin
Garman
(Robin Scoville
and Cath Kean)
C/O High (4x4=16) High
(4x4=16)
significant
(4x3=12)
The governance structure around Dual Diagnosis and joint
working with other agencies is established and in place. A joint
dual diagnosis meeting, chaired by the NEW Devon lead
commissioner occurs once a month between DPT adult services,
RISE and the (DPT) Torbay drug and alcohol service. These are
attended by service managers from all adult community teams.
They oversee the implementation of action plans, develop audits
and consider any RCA investigations with any dual diagnosis
issues. The commissioner has recently indicated that he is
satisfied with working arrangements and that the frequency of
meetings can be reduced.
Locality dual diagnosis meetings with local providers are up and
running in each area. The meetings include a joint review of
caseloads and reviews of service design.
An audit takes place once a year of clients open to DPT teams
and drug and alcohol services. This year’s (planned for April) will
include service user feedback for the first time. Previous audits
were based on best practice and the findings from RCAs. This
year’s will also include standards drawn from NICE guidelines.
A protocol on joint working with RISE and the Torbay drug and
alcohol services has been ratified. Three pathways are detailed in
the protocol which are shown below. Pathway one follows from a
GP referral and details separate assessments by DPT and drug
and alcohol services but joint arrangements are put in place
around care planning, information sharing and reviews. Pathway
two follows from a drug and alcohol service referring a patient
into DPT.
• The Training Needs Analysis
became a component of the
Learning and Development
Review being completed by
Workforce rather than a specific
and detailed analysis in relation to
dual diagnosis.
• It is not clear that dual diagnosis
patients can now be readily
reported on reliably from care
notes by their cluster, diagnosis or
fields on alcohol and drug use in
their assessments. Or that
adherence to the pathway is
routinely checked for individual
patients.
• The 2017 audit did not include a
patient survey as planned.
A task and finish group is meeting fortnightly to take forward
the actions that need to be completed by the 28th January
when NHS England will next meet to consider the HASCAS
investigation report. The timetable is tight but the actions are
on track. A workshop is taking place on the 24th of January
which will include a presentation from service users, an outline
of local DD pathways, the recent audit report, case
presentations of good and less good practice and problem
solving by function and locality to fix areas identified in the
audit report. On line e-learning has been created and sent to
the training department to be uploaded to Daisy. This will be
mandatory for all clinical staff in the adult directorate. Service
managers are identifying CMHT staff to spend time
shadowing drug and alcohol workers. It has been agreed to
offer joint assessments to all relevant routine referrals and
feedback from the drug and alcohol service is that this has
improved, figures on how many have been conducted have
been requested. Joint working with the non-Trust Drug and
alcohol services – currently run by Rise, may be effected in
April as the service has recently been tendered and Rise were
unsuccessful, so a changeover will take place at this time.
Care notes has been altered to allow easier identification of
patients with a dual diagnosis for staff to check that the
pathways are being followed in supervision. A clinical bundle
on dual diagnosis has been distributed and all staff asked to
sign that they have read it. Service Managers have been
asked to report back on the number of signed forms returned
so far. Guidance has been drafted on how best to support
accommodation providers with dual diagnosis clients and this
will be added to the bundle. An SBAR on the results of last
No wide scale additional training
has yet taken place. There does
not appear to be a clear strategy
that details who needs training on
what and how this will be delivered
long term across the organisation.
• The option of seconding CMHT
staff into drug and alcohol services
to improve their skills has not been
explored.
• An information sharing protocol
with RISE is not in place.
• Joint assessments have not been
rolled out and are not routine
practice in the teams where they
were piloted
SMB Q&S
\\DPTDATA\BarrF$\Fiona\CAF\Jan 18 Review\PK\Dual
Diagnosis Task and Finish Group Action Plan 29 01 18.docx
Ref: Combined Assurance Framework Corporate Risk Register Page 2 of 5
7.2
Cor
pora
teA
ssur
ance
Page 93 of 96

ID Activity/Objective/
Risk Description
Contributory issue Source of risk Exec Risk
Type
Prev Month's
Risk
Inherent
Risk (risk if
no controls
were in
place, ie
pre-
mitigating
actions)
Residual Risk
(risk that
remains after
controls are
taken into
account, ie
post-
mitigating
actions)
Current Assurance
(Evidence of effective actions)
Gaps in Assurance
(Where evidence is inadequate
of our control and systems)
Current Controls
(Actions being taken to mitigate risks)
Gaps in Control
(Where systems of control are
inadequate)
Committee Action Plan
(Evidence of action to address control/assurance gaps)
S39 Added December 2017
IF ligature reduced cells
are not available for
prisoners who are at high
risk of suicide THEN the
risk of completed suicide is
high.
RISK APPETITE - AVOID
1. In HMP Exeter there are two safe
cells and two gated cells for a
population of 533. HMP Exeter is a
Category B remand prison which
presents a higher risk of suicide.
There have been 5 suicides by
ligature in the past 6 months. Rates
of prison suicides are a national
issue.
1. Incident Reports / RCA Reports
within Devon prison health services
David
Somerfield
(Brian
Darnley/Sam
Churchward)
C/O N/A High
(4x5=20)
Moderate
(1x5=5)
1. Monitoring of incident reports of serious incidents or near
misses.
2. Review paper submitted to Q&S Committee every two months.
None. 1. Risk assessments to determine those at highest risk of
suicide.
2. Placing on 'Constant Watch' those assessed as being at
highest risk.
3. The use of the ACCT process to safeguard individuals
assessed at high risk. This is a multi-agency process of
enhanced observation.
1. Risk assessments not
consistently completed, resulting in
over or under management of risk.
2. Information not being made
available which would highlight
additional risks. Risk assessment
is not an exact predictor of risk.
1. DGB
2. LDU
Governance
3. Q&S
1. Letter reagrding DPT concerns sent from Melanie Walker, CEO, to Governor of HMP Exeter. Target
date: Nov 2017. Completed.
2. Process to be developed for anyone placed on a constant watch to have a high level risk assessment by
a Consultant Psychiatrist. Target date: Nov 2017. Completed.
3. Training of staff to carry out processes more consistently to improve safety of services - care planning.
Training delivered to 7 staff on 20/21 Nov 2017. Training planned for 6 staff on 11/12 Dec 2017. 4 staff to
receive training on 12 Jan 2018. Target date: Jan 2018.
4. Training of staff to carry out processes more consistently to improve safety of services - triage
assessment. Target date: Feb 2017.
5. Quality review of records to be implemented to improve standards of documentation. First 3 standards
produced by team ready for next quality records cycle from 18 Dec 2017 - 1. triage assessment, 2. care
plans and 3. casework (progress notes). Target date: Dec 2017.
6. Melanie Walker, CEO, to meet with the Governor of HMP Exeter to discuss the provision of ligature free
cells and to see how we can assist in moving the issue forward to HMP's. Target date: Complete
7. MH Team to receive ASIST Suicide Prevention Training to ensure that they are aware of the risk factors
pertinent to suicide in the prison population. The ASIST approach enables practitioners to manage suicide
ideation through longer term care planning. Target date: Apr 2018.
**Target date to achieve residual risk: July 2018
Key milestones: as above.
SU35 Added March 2017
(previously SU21)
IF the Trust is unable to
effectively re-profile the
workforce given the
national shortage of staff in
specific professional
groups THEN we will find it
increasingly difficult to
ensure there is sufficient
workforce supply to
resource services. The
resulting gaps could have
an adverse impact on the
provision of care.
RISK APPETITE -
HUNGRY
1. Nationally there is a shortage of
qualified nurses and there are low
numbers of newly qualified nurses,
with no immediate prospect of early
resolution. This may affect the quality
and safety of services provided by
the Trust.
2. Internally some newly qualified
staff frequently leave inpatient areas
to work in community settings.
3. Emerging new services that may
be provided by the Trust or other
providers (e.g. PICU, Cygnet) can
prove attractive to staff and
exacerbate workforce gaps in
current services.
Recruitment
1. National shortage of suitable
qualified nurses.
2. Number of suitably
qualified/experienced applicants for
key posts is often low.
3. High demand and low supply.
4. Age profile of Trust nursing staff will
result in further turnover in the next 3
to 5 years.
5. Geographic location makes
recruitment more challenging -
particularly in some parts of Devon.
Retention
1. Staff leave inpatient units to work in
community settings.
Helen England
(Alison Dean)
S/C/O High
(4x4=16)
High
(4x4=16)
Significant
(4x3=12)
1. Workforce remodelling to adapt skills mix.
2. Higher Education England (HEE) supporting development of
workforce strategies across the Devon STP.
3. Trainee Assistant Practitioner recruitment and training
programme in place.
4. Devon-wide pilot of Associate Nurse role in place.
5. Project established to optimise opportunities through
apprenticeship levy.
6. Dedicated resource in place for practice education and
development.
7. Bi-monthly reporting to SMB and WODAC.
8. Recruitment of preceptors to Trust-wide programme (working
group established).
9. Participation in national workforce planning.
1. Assurance on training pipeline
and the likely numbers of qualified
staff this will create in the South
West
1. Workforce plans integrated with finance and business
planning.
2. Development of workforce plans at Directorate level to
include training and development.
3. Participation in national and STP workforce planning.
4. Bi-monthly reporting to SMB and WODAC.
5. Review of Workforce Business Partner role to release
capacity for enhanced contribution to strategic workforce
planning at directorate level.
1. Development of workforce
planning expertise and systems in
Directorates.
2. Translate workforce plans into
capacity and resourcing plans so
that recruitment and development
are delivered in a timely way.
3. Operational managers need
support in thinking about the use of
different/new roles.
1. SMB
2. WODAC
3. DGB
1. Apprenticeship Project monitoring through Workforce Project Board. Levy in place and plan for
apprenticeship levels developed. Finance SMB approved the procurement of training suppliers. Tender
completed Nov 2017 with three preferred providers. Target date: Mar 2018
2. Development of bridging reports for SMB and WODAC with capacity/resourcing plans. Enhanced SMB
reports approved and reaching Directorates through the Workforce Business Partners. Resourcing plan
taken routinely to WODAC. Target date: Aug 2017. Completed.
3. Workforce planning templates developed with workshops supporting implementation. Templates and
guidance circulated to all Workforce Business Partners (Oct 2017) to be used in planning round (starting
Feb 2018). Target date: Completed.
4. Career pathways to be developed for support posts and preceptorships linked to training programmes
rather than posts. Scoping work commenced and market research results presented, informing the revised
preceptorship programme. Options for recruitment to training posts for B5 nurses presented to SMB (Dec
2017). Target date: Mar 2018. 5. Enhance
leadership capacity for Practice Education Team. Target date: Mar 2018
**Target date to achieve residual risk: Apr 2018
Key milestones
1. Plan for apprenticehip levy to be fully utilised – Mar 2018.
2. Development of a scheme for career pathways, both clinical and non-clinical – Mar 2018.
3. Revision of preceptorship programme – Dec 2018.
4. Support staff recruited to training programmes – Mar 2018.
5. Workforce planning templates, guidance and training available to operational managers. Completed.
SU36 Added March 2017
(previously SU33)
IF the Trust is unable to
recruit and retain sufficient
numbers of clinical staff
THEN this could impact on
our ability to deliver
services and to build a
reputation as a recognised
Centre of Excellence.
RISK APPETITE - OPEN
1. Shortfalls in workforce supply
have led to significant competition for
staff across health providers.
1. Known national and local shortages
of mental health clinicians, particularly
psychiatrists and B5 nurses.
2. A number of staff choose to retire
early and some still have mental
health officer status which enables
this.
3. The Trust has to adhere to NHS
Improvement caps on the use of
agency staff.
Helen England O/F/S High
(4x4=16)
High
(4x4=16)
Significant
(4x3=12)
1. Revised process for conducting staff exit interviews.
2. Workforce Resourcing Framework and Action Plan to monitor
key actions.
3. Participation in STP resourcing group to foster collaborative
approaches.
4. Vacancy authorisation process expedites clinical roles to
external recruitment.
5. Monthly performance management of workforce resourcing
projects through the Action Group (WRAG)
6. Development of bespoke plan to improve retention - supported
by NHS Improvement National Programme
7. Intelligence, influence and actions derived from the
participation, strengthening our domestic supply through regional
workshops.
1. Evidence a causal link between
actions and impact.
1. Monthly monitoring of vacancies, recruitment activity and
performance and Workforce Resourcing Action Plan
2. Reporting to Workforce SMB and WODAC
3. Workforce metrics and reporting.
4. STP Workforce Strategy Group has Devon workstream on
recruitment through which partners can ensure recruitment
initiatives complement each other and maximise resources.
5. Ensure Workforce Resourcing Action Group agrees short
and mid-term priorities with each Directorate as part of
business planning process.
6. WRAG Action Plan (10 priority areas) reviewed monthly.
7. Review of reward as part of DPT 'Our Offer' to staff.
8. Identification of key factors that shape retention.
9.Performance Improvement Project on Recruitment Process
1. Escalation process for skills mix
decisions being addressed by
SMB. 2. Performance data on
recruitment process
1. SMB
2. WODAC
1. Resourcing workshop with key stakeholders and Directorates (Mar 2017): ten priority areas identified;
monthly review process in place and workstreams progressed. Highlights include: 'Our Offer' booklet for
staff; review of preceptorship offer, recruitment fairs and centralised recruitment test of change.
Completed.
2. Digital recruitment microsite and digital recruitment campaign - signed-off by Workforce Resourcing
Action Group and implementation underway. Development of personas for nurses and doctors, films and
photography completed and channels identified to target on social media for the recruitment campaign.
Site completed on plan by Dec 2017 with integration of NHS Jobs into the microsite to follow. Campaign
now underway and to be timed to begin end Jan/early Feb 2018 for set period of time to be agreed.
Target date: Jun 2017, Dec 2017 for microsite completed. Campaign commenced.
3. Pilot to centrally coordinate recruitment process across Bands 3-7 clinical posts, to commence Aug
2017. Assessment centre took place 6 Oct 2017. Process reviewed and improvements identifed. Target
date: Nov 2017. Completed.
Marketing expertise and capacity now required to improve presentation of job descriptions. Target date to
have resource in place: April 2018. Project to improve accomodation, travel and re-location assistance for
staff to be scoped by April 2018.
**Timescale to achieve residual risk: Mar 2018
SU37 Added April 2017
IF the 2017/18 CIPs
programme is not achieved
recurrently THEN this will
result in a cost pressure in
2018/19.
RISK APPETITE -
MODERATE
1. Operational delivery of CIPs. Sarah
Brampton
F High
(4x4=16)
High
(4x4=16)
Significant
(3x4=12)
1. First cut budget and CIPs approved by Board
2. Monthly and extraordinary meetings with Directorates to
establish CIPs have taken place.
3. Further mitigation planning taken place throughout year
4. DGBs monthly review of CIPs control and financial
performance.
5. Mandatory financial budget training has taken place (Feb
2017).
6. Q&S Committee - sign off of Quality Impact Assessment of all
CIPs
7. FIC and Q&S Committee review and approval.
1. Evaluate value of CIPs - further
CIP meetings being arranged to
develop mitigations. Completed
2. SLA contract to be agreed with
CCG. Completed
3. Monitor and evaluate delivery
through SMB, FIC and Q&S.
1. DoF led meetings with all Directors to finalise plans.
2. FIC and Q&S Committee to review and approval.
3. SMB and Directorate performance management.
4. Continuation of budget holder programme to develop
budget management skills across the Trust.
5. Meetings continue with Directorates throughout the year to
monitor delivery.
1. FIC
2. SMB
3. DGB
1. CIP plans with Directorates reviewed on monthly basis at DGBs. Target date: reviewed monthly.
2. CIP plans received by Q&S Committee to review quality impact assessments. Target date: end April,
May 2017. Presented at Audit Committee (8 June 2017). Completed.
3. DoF working with CCG to finalise contract. Target date: Apr 2017, May 2017, Jun 2017, Aug 2017,
Sep 2017, Oct 2017. Contract finalised Oct 2017 and signed Nov 2017. Completed.
**Timescale to achieve residual risk: Sep 2017, Jan 2019. SMB have agreed to review all non-
recurrrent CIPs forecast to be achieved this year with a view to making them recurrent where operationally
and clinically safe to do so. This work is being led by Deputy COO and will report back in Dec 2017 and
then in Feb 2018. This will reduce cost pressure going into 2018/19.
Key milestones:
1. Monthly reports of achievement against the profiled plan to SMB, FIC and BoD – review 31 Mar 2018.
Ref: Combined Assurance Framework Corporate Risk Register Page 3 of 5
7.2
Cor
pora
teA
ssur
ance
Page 94 of 96

ID Activity/Objective/
Risk Description
Contributory issue Source of risk Exec Risk
Type
Prev Month's
Risk
Inherent
Risk (risk if
no controls
were in
place, ie
pre-
mitigating
actions)
Residual Risk
(risk that
remains after
controls are
taken into
account, ie
post-
mitigating
actions)
Current Assurance
(Evidence of effective actions)
Gaps in Assurance
(Where evidence is inadequate
of our control and systems)
Current Controls
(Actions being taken to mitigate risks)
Gaps in Control
(Where systems of control are
inadequate)
Committee Action Plan
(Evidence of action to address control/assurance gaps)
SU38 Added April 2017
IF the SMART Recovery
Programme is not fully
implemented THEN this
may not deliver revenue
CIPs 2017/18.
RISK APPETITE -
MODERATE
1. Implementation of SMART
pathway and new ways of working.
Sarah
Brampton
(Kevin Grady)
F Significant
(4x3=12)
High
(5x3 =15) Moderate
(5x2=10)
1. Updated PMO structure to support SMART.
2. SMART implementation plans reviewed and refreshed by the
Executive Team (Mar 2017). SMART discussed weekly at
Executive Team meeting.
3. Executive action plan developed (Jun 2017) with timeframes to
drive forward programme challenges.
4. Tiverton Assessment Hub operational (Jun 2017) and North
Devon Wellbeing Hub operational (May 2017).
5. Agreed continuation with the sale of Riverside and Quay in
Barnstaple to release £600k capital and £120k revenue.
6. Operational transitional plan in place in Adult Directorate.
7. Additional management capacity being sought to support
senior team to embed changes.
8. OPMH workforce and medical staff plan developed.
9. Clinic scheduling framework in place.
1. Gaps in plans to achieve
2017/18 CIP target.
2. Directorate does not have a
plan to transition staff into new
roles to support SMART plan.
1. Weekly SMART group monitoring project delivery.
2. Weekly clinical assurance group.
3. Fortnightly finance meeting review plans.
4. Strengthened governance arrangements in place.
5. Monthly SMART Board meetings.
6. Weekly clinical assurance meetings.
7. Operational management plan in place to embed changes
in practice.
1. New workforce models not yet
owned by Directorates.
1. FIC
2. EXEC
3. SMART
4. DGB
1. Core Care Pathway (phased implementation plan) developed with Adult Directorate. Rollout Jan 2017–
Jun 2017. Target date: Jul 2017, Nov 2017 so the Executive action plan around Consultant input and
NMP can be implemented. Meeting held between medical staffing and consultants from EEM to discuss
options for developing a robust roster to civer the hub clinic in Wonford House 52 weeks per year - two
options worked up (Nov 2017).
2. SMART Dashboards to be used to measure improvement in productivity (approval through
Performance, SMB and DGBs and with staff training). Target date: Oct 2017, Nov 2017 as awaiting
Dashboard sign-off.
3. Adult Directorate workforce re-design (CIPs) to start in Aug 2017 led by Cath Keane. Target date: Apr
2018
4. OPMH PMO supported programme plan and PMO resource aligned to support the delivery of key
projects that support the delivery of CIPs. Target date: Mar 2018
5. SPA Business Case signed off through SMB and Transformation Board (project to run from Oct 2017 to
Jun 2018). Target date: Completed.
6. SMART Programme Plan revised through to Mar 2018. Target date: Completed.
**Timescale to achieve residual risk: Mar 2016, Jun 2017, Oct 2017, Dec 2017, Apr 2018 to ensure
SMHP training can be delivered to support psychologically informed practice and productivity gains and
CIP target being met. Agree through cross-directorate meeting to allow additional time for psychologically
informed practice training.
Key milestones:
1. OPMH workforce and medical staffing plan to be redefined.
2. Adult Directorate workforce redesign (CIPs).
3. Full utilisation of SMART Dashboards.
SU39 Added April 2017
IF the Trust does not meet
its financial plans and if
there are major unforeseen
events THEN there is a risk
that the Trust may not be
able to deliver a minimum
RAF rating of 2 in 2017/18.
RISK APPETITE -
MODERATE
1. Capital sales programme (timing
and value), reduced income, non-
delivery of CIPs, non-payment of
debtors and increased non-pay
costs.
2. Non-performance against
contract.
3. Increased risk - IPP pressures, out
of area beds and agency costs.
4. Planning assumptions - CQUIN.
5. Non-delivery of Secure
repatriations in line with delivery
plans.
1. Slippage on disposal plans and/or
failure to deliver CIPs could impact on
cash balances leading to reduced
liquidity and possible RAF of 2.
2. Adult and PICU bed pressures -
overspend.
3. Premises insurance self
assessment - possible costs
associated.
4. Inabaility to secure contract
settlement from CCG.
Sarah
Brampton
F
Significant
(5x2=10)
Significant
(5x2=10)
Moderate
(5x1=5)
1. Financial planning process through SMB.
2. Review and scrutiny at FIC.
3. Review by NHS improvement.
4. Cash mitigation plans continuously through FIC.
5. Sustained healthy liquidity ratio during 2016/17
6. First cut budget and CIP plan approved by Board.
7. Monthly returns and control totals in place.
8. Capital program reviews in place.
1. Further work against a plan to
minimise the possibility of
reaching a RAF of 2.
1. Detailed review of options by SMB.
2. Review and scrutiny by FIC.
3. FIC review and approval.
4. SMB and Directorate on-going performance management.
5. Continuation of budget holder program.
1. FIC
2. SMB
1. Monthly review of RAF and performance against all financial targets. Target date: reviewed monthly.
2. Mitigating plans will be brought into force as and when appropriate. Target date: Ongoing.
3. CIP plans with Directorates reviewed on a monthly basis. Target date: reviewed monthly.
4. Quality performance meetings chaired by COO in place. Target date: completed.
**Timescale to achieve residual risk level: Mar 2018
Key milestones:
1. Monthly reports of achievement against the profiled plan to SMB, FIC and Board.
SU41 Added July 2017
IF the Mother and Baby
Unit cannot be built and
opened by the end of
March 2019, THEN there is
a risk that the capital
funding will not be
available.
RISK APPETITE-
CAUTIOUS
1. Procurement route may take
longer than planned.
2. Other unforeseen delays occur.
3. Issues with Interim MBU solution
due to the extent of the
refurbishment works needed. The
unit will be operational Mar 2018.
4. Capital costs could exceed the
budget and add to the programme.
1. Conversations with NHS England
about capital funding post 2018/19.
Helen England
(Ralph
Hayward)
F/S High
(5x3 =15)
High
(5x3 =15)
Significant
(5x2=10)
1. Project Board managing timeline.
2. CEO met with Exeter City Council re planning permission.
3. Procurement work prioritised to ensure timelines met.
4. Signed contract with NHS England and formal notification on
availability of capital funding.
5. Received capital for total project (Aug 2017).
6. Interim MBU to be in place by Mar 2018.
7. Refurbishment works tendered - contract awarded.
8. Signed interim MBU NHS England contract.
9. Planning permission in place.
1. Project Board in place.
2. Ongoing conversations with NHS England and Exeter City
Council.
3. Executive Team oversight.
4. Appointed architects to developed design and planning
permission confirmed subject to conditions
1. FIC
2. SMB
1. Planning Application submitted in Sep 2017 and decision expected at end of Dec 2017 Target date:
Dec 2017.
2. Interim contract with NHS England. Target date: Aug 2017. Completed.
3. Appoint architects and submit planning application. Target date: Sep 2017. Completed
4. Interim MBU refurbishment works in place by 2017/18. Target date: Dec 2017, Mar 2018.
5. Principal supply chain partner to be selected. Letter issues to Interserve Target date: Nov 2017.
Completed.
6. Supplier interviews 1 Nov 2017 through Framework 22. Target date: Nov 2017.
7. Approval of Full Business Case by Board. Target date: Feb 2018. Now March 2018 due to GMP
timeline
**Timescale to achieve residual risk: Dec 2017, March 2018 linked to issues with interim MBU and
securing GMP to finalise business case for new unit.
Key milestones:
1. Approval of full Business Case by Board - by March 2018.
2. Planning permission - received.
3. Construction to commence- by end Mar 2018.
4. Delivery of interim MBU - by March 2018.
SU42 Added July 2017
IF the number of new
admissions to High
Dependency Inpatient
Services continues to
exceed the forecasted plan
THEN this will affect the
IPP Directorate's delivery
of the Financial Plan
(2017/18.)
RISK APPETITE -
CAUTIOUS
Elective Care
1. New referrals in excess of plan
(High Dependency Inpatient
Rehabilitation - locked).
2. Delayed transfer of care (funding
approval, identification of appropriate
step down placements, timely MoJ
approval).
3. Responsible commissioner
handover delays.
4. Delayed care pathway
developments (PD).
5. Timing of Local Authority uplifts.
6.No HDIR units in Devon (Russell
Clinic is not a locked facility).
1. Delayed discharge calls &
information from delayed transfers of
care
2. Weekly IPP clinical reviews and
new panel applications for approval.
3. IPP Panel Minutes.
4. Monthly IPAM report.
5. Directorate's performance review -
DGB.
Peter Aitken
(Shawn Tait)
F High
(4x4=16)
High
(4x4=16)
Moderate
(4x2=8)
1. Monthly IPAM reports to CCG's.
2. Monthly SBAR to SMB, DGB, FIC and Exec.
3. Monthly assurance reports and scrutiny at IPP, DGB and x 3
weekly meetings with Adult Directorate.
4. Robust prevention and repatriation plans and processes.
5. Outcome based commissioning.
6. Collaborative working with Secure and Adult Directorates.
7. Finance mitigation plan agreed.
8. IPP attendance at monthly PD and Psychosis hubs to advise,
guide, consult and scrutinise all new referrals.
9. Working in partnership with the Acute Care Pathway to
improve flow and capacity.
10. Deep dive new patients to understand the increase in
referrals for Specialist OOA placements, shared with Directorates
via SMB.
11. Contract and performance monitoring with providers. 12.
Post investment reviews into PD and Psychosis pathways.
1. Lack of specific service model
of care (including role/function of
Russell Clinic).
2. Incomplete evidence based
integrated PD care pathway.
3. Incomplete evidence based
integrated Psychosis Care
Pathway.
4. Effective Psychosis clinical hub
(gatekeeping only).
5. Lack of local HDIR services -
working with independent sector
through MOU to develop services
in Devon.
1. Regular meetings to scrutinise work through FIC, SMB &
IPP Directorate performance management.
2. IPP budget management through DGB to SMB to FIC to
board.
3. Weekly directorate leadership review and scrutiny of the
IPP Focus List.
4. Joined New Care Models Core Group interrogating spend,
capcity, quality care pathways and barriers
5. Implementation of inetgrated clinical quality and
management system BRIDGE IPP.
6. Program of deep dives - findings and learning shared with
Directorates.
1. Frequency and speed of
decision making from Social Care
Panels.
2. Incomplete care pathways -
ACP, PD, Psychosis (with
substance misuse).
3. Lack of agreed single s117
policy with agreed funding matrix
for joint social care and health.
1. SMB
2. DGB
3. CRM -
CCGs
4. FIC
1. Social work re-design program led by Sarah Adams that will establish three social care panels able to
work in a timely way with the IPP agenda March 2018
2.Business Case Business cases in support of HDIR for PD & Psychosis pathways, faciltitated by Program
Management Office (PMO). Cross Directorate working group established facilitated by the PMO to pull
together a single enhanced recovery and rehabilitation work stream. Target date: March 2018
3. Consultation on an agreed S117 between DCC and DPT to report by March2018
**Timescale to achieve residual risk: Apr 2018
Key milestones
1. Social care panel redesign March 2018.
2. Business cases in support of HDIR for PD & Psychosis pathways. March 2018
3. SII7 joint protocol March 2018.
SU43 Added October 2017
IF the PICU activity
continues to exceed the
forecasted plan THEN this
will affect the delivery of
the 2017/18 Financial Plan.
RISK APPETITE -
CAUTIOUS
Urgent & Emergency Care (PICU)
1. Lack of Devon PICU provision.
2. Activity greater than agreed.
3. Delayed transfer of care (secure
and acute).
4. Delayed service redesign - Acute
Care Pathway
1. Delayed discharge calls.
2. Outliers report (daily).
3. Twice weekly PICU call.
3. IPP Panel Minutes.
4. Monthly IPAM report.
5. Directorate's performance review -
DGB.
Peter Aitken
(Shawn Tait)
TBC High
(4x4=16)
High
(4x4=16)
Moderate
(4x2=8)
1. Risk escalated to FIC and SMB.
2. Monthly IPAM reports to CCG's and SBAR to SMB, DGB, FIC
and Executive Team.
3. Devonwide PICU - project board.
4. Monthly assurance reports and scrutiny at IPP, DGB, x3
weekly meetings with Adult Directorate.
5. Collaborative working with Secure and Adult Directorates.
6. Finance mitigation plan agreed.
7. IPP attending PICU Clinical Reference Group Meetings.
8. PICU co-ordinator overseeing PICU/ acute admissions to
ensure timely repatriation (x2 weekly calls and weekly unit visits).
9. 12 month block arrangement with Cygnet Healthcare
10. PICU activity/performance reports, contract and performance
monitoring
11. Working with Acute Care Pathway workstream to improve
flow and capacity.
12. Block contract with Cygnet Healthcare to increase acute bed
capacity.
13. Internal Service Level Agreement between IPP and Adult
Directorate. IPP to fund PICU block (additional beds to be funded
by the Adult Directorate).
1. Lack of attendance by Adult
Directorate at x2 weekly PICU
calls.
2. Evidence based integrated PD
care pathway.
3. Lack of acute bed capacity to
ensure timely repatriation from
PICU.
4. Effective Psychosis clinical hub
(gatekeeping only).
1. Regular meetings to scrutinise work through FIC.
2. SMB & IPP Directorate performance management.
3. IPP budget management within IPP Directorate with clear
accountability to Board and reviewed regularly through
performance meetings.
4. x2 weekly PICU conference calls.
5. Weekly minimum contact with PICU providers via UEC Co-
ordinator.
6. Risk share agreement with Adult Directorate for 12th PICU
bed.
7. Improved information from Secure New Models of Care
(NHS England) - step down plans for secure placed
individual.
8. IPP, as commissioners, involved in PICU Project Board
and PICU end users group.
9. Currently Bed capacity team coordinate PICU activity and
have a repatriation clinician who manages the patient
pathway
1. Lack of a Devon PICU.
2. Lack of attendance by Adult
Directorate at x2 weekly PICU call.
1. SMB
2. DGB
3. CRM -
CCGs
4. FIC
5. PICU
1. Build and commission Devon PICU. Target date: Jan 2019
2. Agree PICU Commissioning Strategy for 2018/19. Options paper to be completed and presented to
SMB for decision. Target date: Nov 2017. Completed.
**Timescale to achieve residual risk: Apr 2018
Key milestones
1. Business case for local PICU. Target date: Completed
2. Commission Devonwide PICU. Target date: Jan 2019
3. Agree Commissioning Strategy for 2018-19. Target date: Nov 2017. Completed.
Ref: Combined Assurance Framework Corporate Risk Register Page 4 of 5
7.2
Cor
pora
teA
ssur
ance
Page 95 of 96

ID Activity/Objective/
Risk Description
Contributory issue Source of risk Exec Risk
Type
Prev Month's
Risk
Inherent
Risk (risk if
no controls
were in
place, ie
pre-
mitigating
actions)
Residual Risk
(risk that
remains after
controls are
taken into
account, ie
post-
mitigating
actions)
Current Assurance
(Evidence of effective actions)
Gaps in Assurance
(Where evidence is inadequate
of our control and systems)
Current Controls
(Actions being taken to mitigate risks)
Gaps in Control
(Where systems of control are
inadequate)
Committee Action Plan
(Evidence of action to address control/assurance gaps)
SU44 Added December 2017
IF the Trust does not meet
compliance standards of
Data Protection Act 2017
(General Data Protection
Regulations - GDPR)
THEN there is a risk of
Investigation by the
Information
Commissioner's Office
(ICO) leading to possible
enforcement action,
including monetary penalty
of up to €10m or 2% of the
organisation’s turnover.
RISK APPETITE -
AVERSE
1. Limited resources to progress with
preparation for implementation of the
new standards.
1. New GDPR legislation. Sarah
Brampton
(Mark Jones)
IM&T/ F N/A High
(4x4=16)
Low
(2x2=4)
1. Compliance with current legislation and Information
Governance Toolkit.
1. Detailed action plan not yet
complete.
1. High level actions identified in accordance with national
guidance.
2. Ongoing work to meet the new standards of the Data
Protection and Security Toolkit.
1. Not yet appointed Data
Protection Officer.
2. Policies and procedures to be
reviewed.
3. Assessment and allocation of
resources needed.
4. Development and
implementation of detailed action
plan.
1. FIC
2. SMB
3. IM&T
Strategy
1. Initial resource allocation to Safer Information Team to free IG Manager in order to focus on planning
and compliance (Susan Banham). Progress: Job description complete and approved by HR.
Advertisement to commence w/c 4 Dec 2017. Target Date: Dec 2017.
2. Action plan and detailed risks to be reviewed/monitored via FIC, IM&T Strategy Group and SMB (Susan
Banham). Target Date: Ongoing.
3. Task and finish group to be set up to review and progress the action plan and report to committee as
required (Mark Jones). First meeting in Dec 2017 being set up. Consideration being given to Non-
Executive Director input to group. Target Date: Dec 2017.
**Timescale to achieve residual risk May 18
Key milestones:
1. Collate detailed action plan including review of resources required (Susan Banham). Progress: Initial
requirements compiled. Work proceeding on detailed planning. Target Date: Dec 2017. Start Date:
01/09/17
Action: Collate detailed action plan by 15.12.17 including review of resources required.
Owner: Susan Banham
Target Date: 15/12/2017 02/02/18
Completed:
Progress: Initial requirements compiled. Work has been undertaken for detailed planning, target
has been delayed due to illness within the team and IG Officer joining department on 08/01/17.
Action to be completed w/e 02/02/18 through dedicated workshop on 31st January 2018.Start Date:
19/12/17
Action: Action plan and detailed risks to be reviewed/monitored via IM&T strategy group and SMB
Owner: Susan Banham
Target Date: 01/05/2018
Completed:
Progress: Update to be provided at IM&T Strategy Group on 06/02/18
T1 Added September 2010
and redefined October
2014
IF individuals remain held
on a waiting list for
recovery co-ordination
THEN this may affect their
wellbeing and their
pathway to recovery and
ultimately their safety.
RISK APPETITE -
CAUTIOUS
1. National shortage of mental health
professionals creating capacity
issues within community teams
2. Sickness rates compound
community team capacity.
1. Trust wide Board level risk
assessment.
2. Incident reports.
3. Local risk registers.
4. Directorate performance review
meetings or DGBs.
David
Somerfield
(Robin
Scoville/Sarah
Hughes)
C/O Significant
(5x2=10)
Significant
(5x2=10)
Moderate
(5x1=5)
1. Monthly performance data (referral to assessment date).
2. Monthly Board reporting scorecard.
3. Monthly Adult CD exception reporting.
4. Review of Provider Compliance Assessments.
5. Reports to Q&S, Exec and Board across last 3 months.
6. All waiting lists for treatment and care co-ordination analysed
and RAG rated.
7. Triage standards in place.
8. Monthly meetings with performance team.
9. ORBIT and referral redesign project plans.
10. Link to rollout agreed CQUIN target over 2 year period.
11. Central referral management across Adult Directorate.
12. Demand and capacity plan being implemented.
13. Capacity in respect of actions re AMH prioritised within the
Improvement Academy.
14. Reduction in waiting list project.
15. SMB agreed task and finish group with monthly reporting.
1. Generalised gaps as detailed
within the reduction in waiting list
project.
1. Monthly monitoring at team level through performance and
Directorate meetings.
2. Capacity directed at agreed priorities.
3. Monitoring of compliance against individualised targets.
4. On-going service redesign and skills mix.
5. Inter-Directorate communication through Community
Effectiveness Group.
6. Consistency checks through RiO/CareNotes.
7. Review timeliness of data with performance.
8. Development of PBR linked clinical pathways.
9. Review of waiting list protocol.
10. Development of escalation matrix.
11. Team by team engagement re waiting list and discharge
planning - led by two senior staff.
12. Risk assessment of all referrals and waiting lists (RAG
rated for priority).
13. On-going review and reporting against reduction in waiting
list project. Reporting into Adult Directorate governance
system, community redesign, Board and SMB.
1. Capacity along the pathway to
meet treatment or interventions
identified.
2. Variations in current service
specifications and identification of
priority client groups leading to
gaps in service provision.
1. Q&S 1. Introduction to Cognitive Behavioral Therapy and Behavioural Activation 2 day course to be delivered to
all community Band 5/6 clinicians to support their effective practice on the initial interventions programme.
Target Date: Jan 2018 (last course date).
2. Pathways information training to be delivered to all teams referring to Community Mental Health Teams.
Target date: last training day booked for 29 Mar 2018
3. Conference calls commenced Sep 2017 to accelerate implementation of clinic rotas. Target date:
Completed.
**Timescale to achieve residual risk: Feb 2018
Key milestones:
1. Achievement of agreed waiting list trajectories within the national agreed targets. Waiting list trajectories
remain positive, though variable through LDUs, with some areas continuing to exceed the referral to
treatment target.
2. PD change training delivered to all Band 5/6 community clinicians.
3. CBT and Behavioural Activation training booked for all Band 5 and 6 community clinicians.
4. Planned Care Dashboard launch to offer contemporary monitoring of clinical efficiency and flow.
ES36 Added Jan 18
If the Trust does not review
the impact on other
contracting companies
following Carillion entering
liquidation then the Trust
may find this has a impacts
on Interserve who are the
Trust's PSCP for the two
new build projects. This may
have an adverse affect on
the Trust project
programmes and introduce a
financial risk.
The collapse of Carillion PLC has the
potential to adversely affect other
contracting companies and the Trust is
relying on Interserve as their PSCP to
procure two buildings that have a
reputational and financial risk.
Carillion entering liquidation Sarah Brampton O N/A Moderate
(4x2 =8)
Low
(4x1=4)
1) The Trust has written to Interserve to seek assurance that the
collapse of Carillion PLC would not impact on the existing Psychiatric
Intensive Care Unit P21+ and Mother and Baby P22 new
development projects currently being undertaken by the Trust.
2) Andy Mitchell of the DH has been asked to provide some evidence
to support Interserves financial position.
3) Interserve Group have provided assurance on their commitment to
Interserve construction following a recapitalisation exercise which
provided a significant equity injection.
1) We are still awaiting a response
from the local Interserve construction
company.
1) We will ask interserve to consider the impact the Carillion
collapse my have on any sub-contractors that they employ to work
on either of the new build projects.
2) Regular meetings with interserve will take place to monitor sub-
contractors delivery.
3) Continue to monitor the discussions taking place within the
construction industry.
1) We have not commissioned an
independent review of the financial
stability of Interserve.
1) Estates
Strategy and
Capital Group.
2) SMB
1. Further press the local Interserve construction company for a response to the local impact
2. A further review of the construction industry impact to the collapse of Carillion PCL will take place and the
findings share with the Trust.
S32 Added July 2016
IF the Trust does not
review and comply with
best practice guidelines
(NICE) THEN patients may
not receive quality health
care, as required by
commissioners.
RISK APPETITE -
AVERSE
1. Audit report - DPT32/16 1. Clinical Audit of NICE
implementation.
Helen Smith
(James
Rooney)
S/C/O Significant
(3x3=9)
Significant
(3x3=9)
Moderate
(3x2=6)
1. The Clinical Effectiveness and Assurance Group (CEAG) meet
monthly with new ToR/Membership.
2. Regular reporting to SMB, Q&S and DGBs as part of the bi-
monthly EScR report.
3. CEAG agreed that a new sub group, the ‘CEAG Clinical
Group’, would review future guidance for relevance to reduce
delay in reviews and enable a clearer Trust position.
4. NICE Guidelines in relation to Physical Healthcare to be
reviewed by Physical Healthcare Steering Group.
5. New QI/Clinical Audit policy ratified at CEAG (Jun 2017).
6. Revised NICE Policy ratified at CEAG (Jun 2017).
7. Actions from internal audit report 2016 checked and signed off
by CEAG (Jun 2017).
8. Clinical Audit/NICE lead established in each Directorate.
1. CEAG meetings re-established
but need to ensure full attendance
by members, in particular
representatives from operational
services.
2. New process for completing
NICE compliance assessments is
being rolled out and is new for
many being asked to complete.
3. Regular consideration of NICE
at DGBs within reporting to SMB.
1. Review of action plan at CEAG to ensure progress.
2. Support to leads completing compliance assessments
available from the Clinical Audit Team.
3. Senior Management engagement incl. Medical Director
who chairs CEAG.
4. Regular reporting of progress to SMB, Q&S and DGBs.
1. Regular consideration of NICE
at DGBs within reporting to SMB.
1. CEAG
2. Q&S
1. From May 2017, CEAG will operate to its ToR (meetings held monthly). Revised template issued to
group members for completion and consideration. As at Oct 2017, meeting quoracy achieved only 50% as
one Directorate did not send a representative (in 5/6 meetings three Directorates attended). ToR and
quoracy on the agenda for the CEAG meeting on 30 Nov 2017. QI/Audit programme is established,
covering appropriate national audits, CQUINs and local QI/audits. The programme for QI/Audit established
this year will roll on into 2018/19. Target date: Dec 2017.
2. CEAG has requested Directorates nominate deputies to attend if the designated person is unable to.
Target date: Dec 17. Review attendance Apr 2018.
3: Dr Smith as chair of the group to write to all CD/MO to ask that they send a member to this group to
represent them. Target date: Jan 2018. COMPLETE
4. Visit from national NICE team ( Jan 20180 with positive feedback about current processes and useful
advice about on going improvement to process.
**Timescale to achieve residual risk: Nov 2016, Dec 2017
Key milestones:
1. Audit and NICE Policies for review in Nov 2017. Placed on CEAG agenda for Dec 2017.
2. ToR/Attendance will be reviewed in Nov 2017. Reviewed at CEAG in Nov 2017. Quorate on only 50%
of occasions since Apr 2017 (all 4 directorates should atttend) although 3 of 4 directorates attended 5 of
the last 6 meetings. 3 consequetive meetings need to be quorate to ensure embeddedness. Quoracy not
acheived in January. (75%)
3. PMO QI leads meeting Directorate leads to progress QI/Audit programme for 2017/18 and prepare
2018/19 programme. 30 audits ongoing in Dec 2017, including National and CQUIN audit.
RISK BELOW REMOVED FROM CAF DUE TO ASSURANCES PROVIDED AT QSC.01.03.18
Ref: Combined Assurance Framework Corporate Risk Register Page 5 of 5
7.2
Cor
pora
teA
ssur
ance
Page 96 of 96





























