Embed Size (px)
Citation preview
http://ajs.sagepub.com/Medicine
The American Journal of Sports
http://ajs.sagepub.com/content/early/2016/02/23/0363546515626538The online version of this article can be found at:
DOI: 10.1177/0363546515626538
published online February 24, 2016Am J Sports MedJoke Schuermans, Damien Van Tiggelen, Lieven Danneels and Erik Witvrouw
Resonance ImagingSusceptibility to Hamstring Injuries in Soccer: A Prospective Study Using Muscle Functional Magnetic
Published by:
http://www.sagepublications.com
On behalf of:
American Orthopaedic Society for Sports Medicine
can be found at:The American Journal of Sports MedicineAdditional services and information for
P<PPublished online February 24, 2016 in advance of the print journal.
http://ajs.sagepub.com/cgi/alertsEmail Alerts:
http://ajs.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- Feb 24, 2016OnlineFirst Version of Record >>
at RMIT University Library on February 25, 2016ajs.sagepub.comDownloaded from at RMIT University Library on February 25, 2016ajs.sagepub.comDownloaded from
Susceptibility to HamstringInjuries in Soccer
A Prospective Study Using MuscleFunctional Magnetic Resonance Imaging
Joke Schuermans,*y MS, Damien Van Tiggelen,y PhD,Lieven Danneels,y PhD, and Erik Witvrouw,yz PhDInvestigation performed at the Department of Rehabilitation Sciences and Physiotherapy,Ghent University, Ghent, Belgium
Background: Running-related hamstring strain injuries remain a delicate issue in several sports such as soccer. Their unremit-tingly high incidence and recurrence rates indicate that the underlying risk has not yet been fully identified. Among other factors,the importance of neuromuscular coordination and the quality of interplay between the different hamstring muscle bellies isthought to be a key determinant within the intrinsic injury risk. Muscle functional magnetic resonance imaging (mfMRI) is oneof the tools that has been proven to be valid for evaluating intermuscular coordination.
Purpose: To investigate the risk of sustaining an index or recurring soccer-related hamstring injury by exploring metabolic musclecharacteristics using mfMRI.
Study Design: Cohort study; Level of evidence, 2.
Methods: A total of 27 healthy male soccer players and 27 soccer players with a history of hamstring injuries underwent stan-dardized mfMRI. The mfMRI protocol consisted of a resting scan, a strenuous bilateral eccentric hamstring exercise, and a post-exercise scan. The exercise-related T2 change, or the signal intensity shift between both scans, was used to detect differences inmetabolic characteristics between (1) the different hamstring muscle bellies and (2) the prospective cohorts based on the (re)oc-currence of hamstring injuries during a follow-up period of 18 months.
Results: The risk of sustaining a first hamstring injury was associated with alterations in the intermuscular hierarchy in terms of themagnitude of the metabolic response after a heavy eccentric effort, with the dominant role of the semitendinosus set aside fora higher contribution of the biceps femoris (P = .017). Receiver operating characteristic (ROC) curve analysis demonstratedthat this variable was significantly able to predict the occurrence of index injuries with a sensitivity of 100% and a specificityof 70% when the metabolic activity of the biceps femoris exceeded 10%. The risk of sustaining a reinjury was associatedwith a substantial deficit in hamstring strength endurance (P = .031). Soccer players who sustained a reinjury were only ableto perform prone leg curls for a mean duration of 146.50 6 76.16 seconds, whereas those with an injury history but no recurrenceduring follow-up were able to continue for a mean of 237.45 6 110.76 seconds (95% CI, 11.9-230.5 seconds; P = .031).
Conclusion: This was the first study to assess the causal relation between the intramuscular recruitment pattern and the risk ofsustaining an index or secondary hamstring strain. Changes in intermuscular interplay seem to significantly increase the risk ofsustaining index hamstring injuries in male amateur soccer players. Inadequate eccentric muscle endurance could be associatedwith an increased risk of sustaining a recurring hamstring injury.
Keywords: hamstring strain injury; etiology; soccer; magnetic resonance imaging
Hamstring strain injuries are the single most commonsports injuries in male soccer players. Given the associatedtime loss and the substantial recurrence rates, these inju-ries have been the subject of research within sports medi-cine for many years.11,19,33,43 In soccer, most commonly,
the biceps femoris (BF) (and to a lesser extent, the semite-ndinosus [ST]) is subject to structural or functionallesions.33,43 These muscles are most likely to sustain inju-ries during explosive running accelerations and kickingactivities because of the high biomechanical demandsplaced on the muscle-tendon unit throughout the frontswing phases in running and kicking.3,6 Next to extensivemuscle stretching and heavy eccentric loading, the impor-tance of intermuscular coordination and cooperationbetween the 3 major biarticular hamstring muscle bellies
The American Journal of Sports Medicine, Vol. XX, No. XDOI: 10.1177/0363546515626538� 2016 The Author(s)
1
AJSM PreView, published on February 24, 2016 as doi:10.1177/0363546515626538
at RMIT University Library on February 25, 2016ajs.sagepub.comDownloaded from

during these eccentric muscle efforts is increasingly beingexplored in current research.20-22,24,36,39 The predominantvulnerability of the BF could possibly be related to its mor-phological characteristics,23 the considerable stretchingand eccentric loading throughout the front swing,6,20 andthe efficiency of intermuscular coordination.20,36 Bearingin mind that the hamstring muscle unit presents a consid-erable vulnerability for both structural and (to an evenhigher extent) functional injuries,10 exploring the role ofneuromuscular coordination in injury susceptibility seemsessential. Previous research has already demonstratedthat the BF, ST, and semimembranosus (SM) are activatedin a specific sequence and with a diverging intensity of con-traction throughout the front swing phase in running.20-22
When the 3 muscle bellies are not capable of engaging insynergistically adequate and economic contractions, thismay cause one of the muscles to fatigue prematurely, ulti-mately resulting in a functional and/or structural injury.36
The exact quantity (spatial distribution of muscle work)and quality (temporal activation characteristics) of inter-muscular interplay within the hamstring unit are sug-gested to be of great importance in hamstring muscleload-bearing capacity and injury vulnerability.36 In a previ-ous study, we already pointed out the value of muscle func-tional magnetic resonance imaging (mfMRI) in assessingthe quantity of intermuscular coordination and the inter-play features within the posterior thigh unit.36 In the priorstudy,36 mfMRI analysis revealed that exercise-inducedmetabolic activity and the exact intermuscular interplaydiffered significantly between soccer players with a (recent)history of hamstring injuries and their matched controls.
Although surface electromyography (EMG) is a valuabletool to measure muscle activity as well, it is less suited todistinguish muscle activity within the same musclegroup,31,32 as it is inevitably subject to cross-talk (in whichneighboring muscles produce a significant amount of theEMG signal that is detected by the local electrode site,challenging the correct evaluation of the isolated activityof each one of the hamstring muscle bellies).11-16 More so,even though EMG measures the amplitude and frequencyof the real-time motor unit discharges within the underly-ing muscle tissue, it is not capable of evaluating the meta-bolic efficacy with which the muscle is able to perform itsimposed task. This is where mfMRI provides an interestingadvantage.§
The T2 relaxation time constant of muscle water, repre-sented by the signal intensity of the muscle tissue capturedin T2 MRI scans, gives an indication of the metabolic stateof the muscle fibers.5,29 Comparing the signal intensity or
the magnitude of the T2 relaxation time constant of themuscle tissue in a scan before and after exercise allowsclinicians and researchers to evaluate to what extent theintended muscle has been activated during that specificexercise. The higher the osmotic and pH changes withinthe loaded muscle unit, the bigger the increase in signalintensity or the more extensive the T2 shift. These physio-logical processes within the muscle tissue are directlyrelated to the amount of muscle work, so the higher theT2 shift, the higher the metabolic muscle activity.
As the most important risk factor for sustaining a ham-string strain injury is presence of an injury history, adequateprimary prevention is essential.33,43 However, consideringthat the risk of sustaining a secondary hamstring injury ismore than twice as high as the risk of sustaining a firstinjury,12 accurate comprehension and acknowledgment ofthe reinjury risk and its implications are even moreimportant.
In our previous study,36 soccer players with a history ofhamstring injuries demonstrated an aberrant and less eco-nomic muscle activation pattern in which the BF partlycompensated for the lack of activation (correspondingwith less metabolic changes) of the (originally eccentricallymore capable) ST. This pattern was associated withweaker strength performance, possibly indicating anincreased risk of sustaining a subsequent injury.
Although we already assessed the retrospective rela-tionship between the intermuscular coordination charac-teristics and soccer-related hamstring injuries, noresearch has attempted to unravel the potential causalassociation between the quality and quantity of activity-induced metabolic changes in the BF, ST, and SM andthe risk of sustaining a future injury. In addition, the exist-ing literature has never explored the nature of the reinjuryrisk profile and its possible disparities with the risk of sus-taining a first hamstring injury.
Therefore, this prospective study intends to explore therelevance of mfMRI for the purpose of identifying thefuture injury risk in male soccer players, making a distinc-tion between the occurrences of first and secondary ham-string strain injuries. In line with the results of previousresearch,36 it was our hypothesis that the risk of hamstringinjuries is associated with an altered pattern of intermus-cular cooperation between the medial and lateral ham-string muscle bellies, with the BF exhibiting more andthe ST exhibiting too little effort compared with whatthey are supposed to produce. The decision to solelyinclude male soccer players was made deliberately, cer-tainly taking into account the recurrence rates, as ham-string injuries are still the single most common type ofinjury within this sport and the financial, personal, andperformance-related stakes are considerable.43§References 1, 2, 5, 7, 10, 13, 19-30, 34, 36, 37.
*Address correspondence to Joke Schuermans, MS, Department of Rehabilitation Sciences and Physiotherapy, Ghent University, De Pintelaan 185,9000 Ghent, Belgium (email: [email protected]).
yDepartment of Rehabilitation Sciences and Physiotherapy, Ghent University, Ghent, Belgium.zDepartment of Physiotherapy, Aspetar, Doha, Qatar.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded by the Agency for Inno-vation by Science and Technology (IWT). This agency provided J.S. with her PhD scholarship.
2 Schuermans et al The American Journal of Sports Medicine
at RMIT University Library on February 25, 2016ajs.sagepub.comDownloaded from
METHODS
mfMRI Protocol
This study was approved by the ethics committee of GhentUniversity Hospital (approval no. EC/2013/118). FromMarch to May 2013, soccer players from 7 recreationalregional soccer clubs (Oost-Vlaanderen, Belgium; commu-nity level) were addressed for participation in this studyby contacting respective trainers, coaches, physical thera-pists, or sports physicians. Potential candidates wereexcluded from the study if they had
� a history of severe knee or hip injuries (eg, anterior cru-ciate ligament or medial collateral ligament ruptures,femoroacetabular impingement, or athletic groin inju-ries requiring surgery);
� a history of lower back complaints or current lower backcomplaints;
� less than 5 years of competitive soccer experience; or� electronic implants, foreign (ferromagnetic) bodies close
to the thigh region, or claustrophobia, which madethem unsuitable for MRI evaluation.
To rule out (subclinical) age-related pathological changes,only soccer players between the age limits of 18 and 35years were considered for inclusion. All participants wererequired to be completely free from injuries and ready toplay at the moment of testing.
Ultimately, 27 male soccer players with a recent historyof hamstring injuries (within the last 2 seasons) and 27matched controls underwent a standardized mfMRI proto-col during the between-season period of July 2013. Soccerplayers in the injury history group had to be recoveredcompletely and have returned to competition. Participantcharacteristics of the formerly injured players and thematched controls are presented in Table 1.
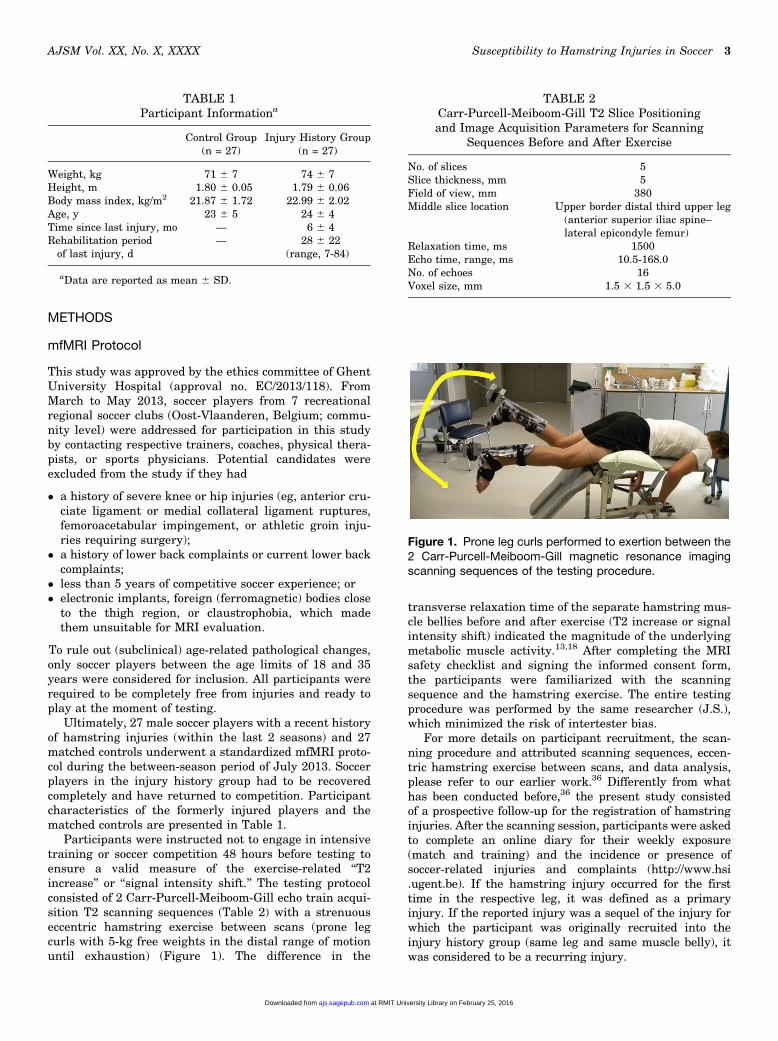
Participants were instructed not to engage in intensivetraining or soccer competition 48 hours before testing toensure a valid measure of the exercise-related ‘‘T2increase’’ or ‘‘signal intensity shift.’’ The testing protocolconsisted of 2 Carr-Purcell-Meiboom-Gill echo train acqui-sition T2 scanning sequences (Table 2) with a strenuouseccentric hamstring exercise between scans (prone legcurls with 5-kg free weights in the distal range of motionuntil exhaustion) (Figure 1). The difference in the
transverse relaxation time of the separate hamstring mus-cle bellies before and after exercise (T2 increase or signalintensity shift) indicated the magnitude of the underlyingmetabolic muscle activity.13,18 After completing the MRIsafety checklist and signing the informed consent form,the participants were familiarized with the scanningsequence and the hamstring exercise. The entire testingprocedure was performed by the same researcher (J.S.),which minimized the risk of intertester bias.
For more details on participant recruitment, the scan-ning procedure and attributed scanning sequences, eccen-tric hamstring exercise between scans, and data analysis,please refer to our earlier work.36 Differently from whathas been conducted before,36 the present study consistedof a prospective follow-up for the registration of hamstringinjuries. After the scanning session, participants were askedto complete an online diary for their weekly exposure(match and training) and the incidence or presence ofsoccer-related injuries and complaints (http://www.hsi.ugent.be). If the hamstring injury occurred for the firsttime in the respective leg, it was defined as a primaryinjury. If the reported injury was a sequel of the injury forwhich the participant was originally recruited into theinjury history group (same leg and same muscle belly), itwas considered to be a recurring injury.
TABLE 1Participant Informationa
Control Group(n = 27)
Injury History Group(n = 27)
Weight, kg 71 6 7 74 6 7Height, m 1.80 6 0.05 1.79 6 0.06Body mass index, kg/m2 21.87 6 1.72 22.99 6 2.02Age, y 23 6 5 24 6 4Time since last injury, mo — 6 6 4Rehabilitation period
of last injury, d— 28 6 22
(range, 7-84)
aData are reported as mean 6 SD.
TABLE 2Carr-Purcell-Meiboom-Gill T2 Slice Positioningand Image Acquisition Parameters for Scanning
Sequences Before and After Exercise
No. of slices 5Slice thickness, mm 5Field of view, mm 380Middle slice location Upper border distal third upper leg
(anterior superior iliac spine–lateral epicondyle femur)
Relaxation time, ms 1500Echo time, range, ms 10.5-168.0No. of echoes 16Voxel size, mm 1.5 3 1.5 3 5.0
Figure 1. Prone leg curls performed to exertion between the2 Carr-Purcell-Meiboom-Gill magnetic resonance imagingscanning sequences of the testing procedure.
AJSM Vol. XX, No. X, XXXX Susceptibility to Hamstring Injuries in Soccer 3
at RMIT University Library on February 25, 2016ajs.sagepub.comDownloaded from

The participants were asked to complete this surveyevery Monday throughout the entire 2013-2014 season aswell as the first half of the 2014-2015 season, resulting ina follow-up period of 1 and a half seasons. Participants’compliance to this online survey was verified on a weeklybasis. Submission of the entire cohort was checked onTuesday morning, after which the players who did notyet complete their survey were notified by email.
Data Analysis
The end of follow-up was set at the 2014-2015 winterbreak, during which period all participants were contactedagain for a final injury inquiry. After gathering the injurydata during follow-up, the resulting cohort was subdividedinto 4 categories based on the injury incidence duringfollow-up and injury history:
� healthy controls,� players with an injury history but no recurring injury
during follow-up,� players who sustained an index injury during follow-up,
and� players who sustained a reinjury during follow-up.
Analysis of the T2 relaxation times in both the resting andpostexercise scans was performed using T2Processor soft-ware (copyright P. Vandemaele, engineer; Ghent Institutefor Functional and Metabolic Imaging, Ghent UniversityHospital) in Matlab (R2014a; The MathWorks Inc). After-ward, exercise-induced T2 shifts were determined manu-ally for the BF, ST, and SM of both legs in eachparticipant36 (Figures 2 and 3) using the following formula:
T2 shift ¼ T2 postexercise value � T2 pre-exercise value
T2 pre-exercise value:
The relative T2 shift (normalized to the baseline T2 value),rather than the absolute T2 shift, was used for statisticalanalysis as this out ruled potential bias caused bybetween-participant differences in baseline metabolic mus-cle features/activity.
Statistical Analysis
The following variables were subjected to statistical analysis:
1. The T2 shift within each muscle belly, representing theamount of metabolic muscle activity between scansðT2 shift ¼ T2 post�T2 pre
T2 pre Þ.36
2. The proportional activity shares of the biarticularhamstring bellies (long head of the BF, ST, andSM) within the entire hamstring–T2 shift, forwhich the T2 shift per muscle belly was normalizedto the summated shifts of all muscle bellies
ðproportional activity ¼ T2 shift ðBF or ST or SMÞT2 shift ðBF1ST1SMÞ Þ.
36
3. The hamstring strength endurance (time to exertion oneccentric prone leg curls between both scans inseconds).
After the outcome variables on the normality of distributionwere checked, Mann-Whitney U tests and independent-samples t tests were used to compare differences in meta-bolic hamstring activation between groups (index injury vscontrol and no reinjury during follow-up vs reinjury duringfollow-up, respectively). Variables for which the mean val-ues differed significantly between groups were submittedfor logistic regression analysis to verify to what extent theevaluated parameters were able to predict the (re)occurrenceof hamstring injuries during follow-up. Additional receiveroperating characteristic (ROC) curve analyses were per-formed if relevant. Statistical analysis was conducted usingSPSS 22 Statistical Software package (IBM Corp); a wasset at .05. Results were interpreted as being significantwhen statistical inference presented a P value �.05.
RESULTS
Of the 54 soccer players who underwent the mfMRI proce-dure in July 2013, 2 sustained a severe knee injury andhad to end their soccer career, 2 stopped playing because ofacademic priorities, and 6 were lost to follow-up. Ultimately,MRI data of 44 participants could be obtained for prospectiveanalysis: 24 controls and 20 with an injury history. A flow-chart with details regarding the composition of the cohortthroughout testing and follow-up is provided in Figure 4.
Figure 2. Region of interest selection in the T2 map acquiredbefore exercise. (A) Right side: biceps femoris, 1; semitendi-nosus, 2; and semimembranosus, 3. (B) Left side: bicepsfemoris, 4; semitendinosus, 5; and semimembranosus, 6.
Figure 3. Region of interest selection in the T2 map acquiredafter exercise. (A) Right side: biceps femoris, 1; semitendino-sus, 2; and semimembranosus, 3. (B) Left side: biceps fem-oris, 4; semitendinosus, 5; and semimembranosus, 6.
4 Schuermans et al The American Journal of Sports Medicine
at RMIT University Library on February 25, 2016ajs.sagepub.comDownloaded from
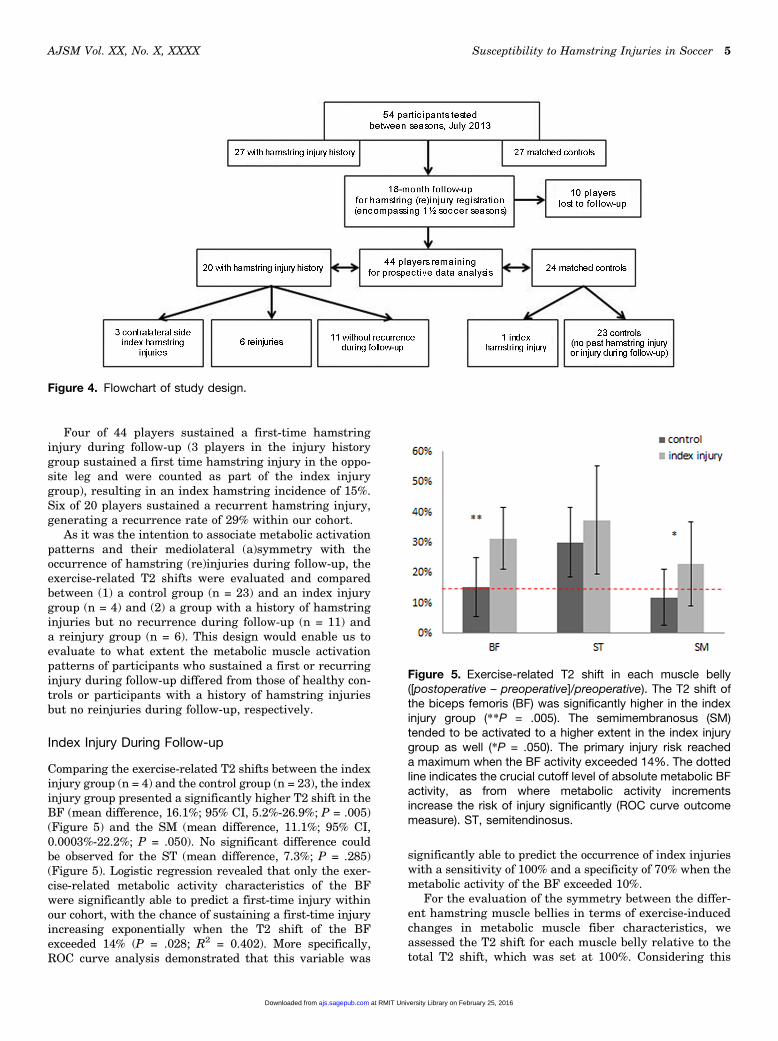
Four of 44 players sustained a first-time hamstringinjury during follow-up (3 players in the injury historygroup sustained a first time hamstring injury in the oppo-site leg and were counted as part of the index injurygroup), resulting in an index hamstring incidence of 15%.Six of 20 players sustained a recurrent hamstring injury,generating a recurrence rate of 29% within our cohort.
As it was the intention to associate metabolic activationpatterns and their mediolateral (a)symmetry with theoccurrence of hamstring (re)injuries during follow-up, theexercise-related T2 shifts were evaluated and comparedbetween (1) a control group (n = 23) and an index injurygroup (n = 4) and (2) a group with a history of hamstringinjuries but no recurrence during follow-up (n = 11) anda reinjury group (n = 6). This design would enable us toevaluate to what extent the metabolic muscle activationpatterns of participants who sustained a first or recurringinjury during follow-up differed from those of healthy con-trols or participants with a history of hamstring injuriesbut no reinjuries during follow-up, respectively.
Index Injury During Follow-up
Comparing the exercise-related T2 shifts between the indexinjury group (n = 4) and the control group (n = 23), the indexinjury group presented a significantly higher T2 shift in theBF (mean difference, 16.1%; 95% CI, 5.2%-26.9%; P = .005)(Figure 5) and the SM (mean difference, 11.1%; 95% CI,0.0003%-22.2%; P = .050). No significant difference couldbe observed for the ST (mean difference, 7.3%; P = .285)(Figure 5). Logistic regression revealed that only the exer-cise-related metabolic activity characteristics of the BFwere significantly able to predict a first-time injury withinour cohort, with the chance of sustaining a first-time injuryincreasing exponentially when the T2 shift of the BFexceeded 14% (P = .028; R2 = 0.402). More specifically,ROC curve analysis demonstrated that this variable was
significantly able to predict the occurrence of index injurieswith a sensitivity of 100% and a specificity of 70% when themetabolic activity of the BF exceeded 10%.
For the evaluation of the symmetry between the differ-ent hamstring muscle bellies in terms of exercise-inducedchanges in metabolic muscle fiber characteristics, weassessed the T2 shift for each muscle belly relative to thetotal T2 shift, which was set at 100%. Considering this
Figure 4. Flowchart of study design.
Figure 5. Exercise-related T2 shift in each muscle belly([postoperative – preoperative]/preoperative). The T2 shift ofthe biceps femoris (BF) was significantly higher in the indexinjury group (**P = .005). The semimembranosus (SM)tended to be activated to a higher extent in the index injurygroup as well (*P = .050). The primary injury risk reacheda maximum when the BF activity exceeded 14%. The dottedline indicates the crucial cutoff level of absolute metabolic BFactivity, as from where metabolic activity incrementsincrease the risk of injury significantly (ROC curve outcomemeasure). ST, semitendinosus.
AJSM Vol. XX, No. X, XXXX Susceptibility to Hamstring Injuries in Soccer 5
at RMIT University Library on February 25, 2016ajs.sagepub.comDownloaded from
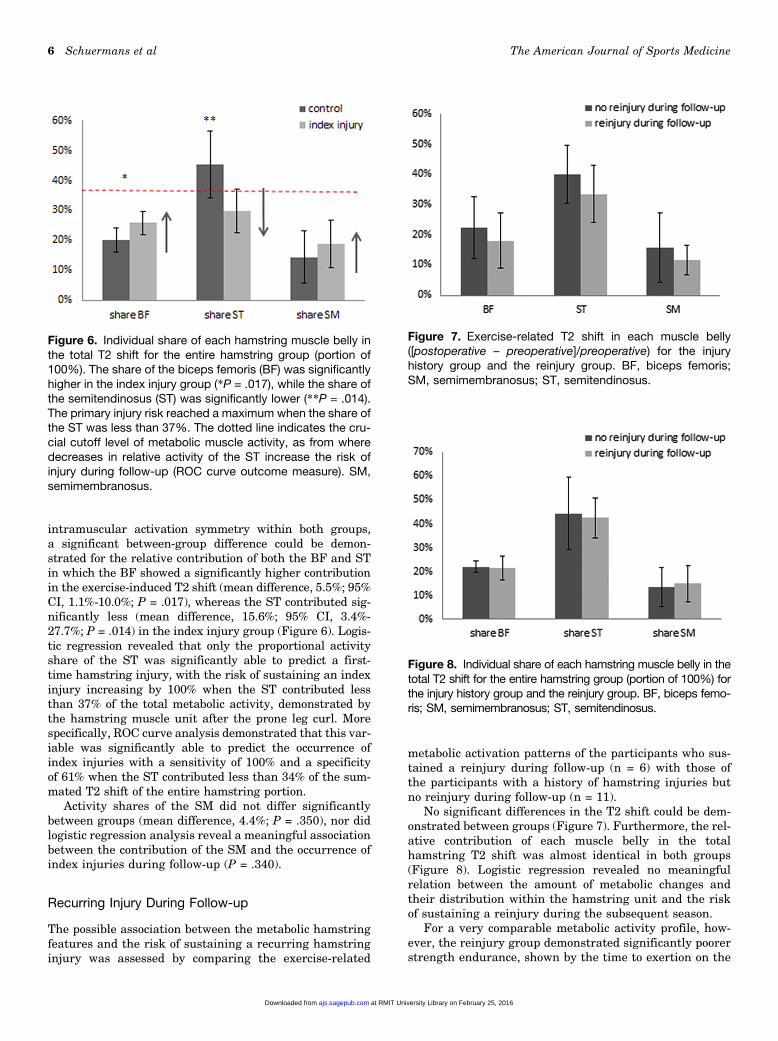
intramuscular activation symmetry within both groups,a significant between-group difference could be demon-strated for the relative contribution of both the BF and STin which the BF showed a significantly higher contributionin the exercise-induced T2 shift (mean difference, 5.5%; 95%CI, 1.1%-10.0%; P = .017), whereas the ST contributed sig-nificantly less (mean difference, 15.6%; 95% CI, 3.4%-27.7%; P = .014) in the index injury group (Figure 6). Logis-tic regression revealed that only the proportional activityshare of the ST was significantly able to predict a first-time hamstring injury, with the risk of sustaining an indexinjury increasing by 100% when the ST contributed lessthan 37% of the total metabolic activity, demonstrated bythe hamstring muscle unit after the prone leg curl. Morespecifically, ROC curve analysis demonstrated that this var-iable was significantly able to predict the occurrence ofindex injuries with a sensitivity of 100% and a specificityof 61% when the ST contributed less than 34% of the sum-mated T2 shift of the entire hamstring portion.
Activity shares of the SM did not differ significantlybetween groups (mean difference, 4.4%; P = .350), nor didlogistic regression analysis reveal a meaningful associationbetween the contribution of the SM and the occurrence ofindex injuries during follow-up (P = .340).
Recurring Injury During Follow-up
The possible association between the metabolic hamstringfeatures and the risk of sustaining a recurring hamstringinjury was assessed by comparing the exercise-related
metabolic activation patterns of the participants who sus-tained a reinjury during follow-up (n = 6) with those ofthe participants with a history of hamstring injuries butno reinjury during follow-up (n = 11).
No significant differences in the T2 shift could be dem-onstrated between groups (Figure 7). Furthermore, the rel-ative contribution of each muscle belly in the totalhamstring T2 shift was almost identical in both groups(Figure 8). Logistic regression revealed no meaningfulrelation between the amount of metabolic changes andtheir distribution within the hamstring unit and the riskof sustaining a reinjury during the subsequent season.
For a very comparable metabolic activity profile, how-ever, the reinjury group demonstrated significantly poorerstrength endurance, shown by the time to exertion on the
Figure 6. Individual share of each hamstring muscle belly inthe total T2 shift for the entire hamstring group (portion of100%). The share of the biceps femoris (BF) was significantlyhigher in the index injury group (*P = .017), while the share ofthe semitendinosus (ST) was significantly lower (**P = .014).The primary injury risk reached a maximum when the share ofthe ST was less than 37%. The dotted line indicates the cru-cial cutoff level of metabolic muscle activity, as from wheredecreases in relative activity of the ST increase the risk ofinjury during follow-up (ROC curve outcome measure). SM,semimembranosus.
Figure 7. Exercise-related T2 shift in each muscle belly([postoperative – preoperative]/preoperative) for the injuryhistory group and the reinjury group. BF, biceps femoris;SM, semimembranosus; ST, semitendinosus.
Figure 8. Individual share of each hamstring muscle belly in thetotal T2 shift for the entire hamstring group (portion of 100%) forthe injury history group and the reinjury group. BF, biceps femo-ris; SM, semimembranosus; ST, semitendinosus.
6 Schuermans et al The American Journal of Sports Medicine
at RMIT University Library on February 25, 2016ajs.sagepub.comDownloaded from
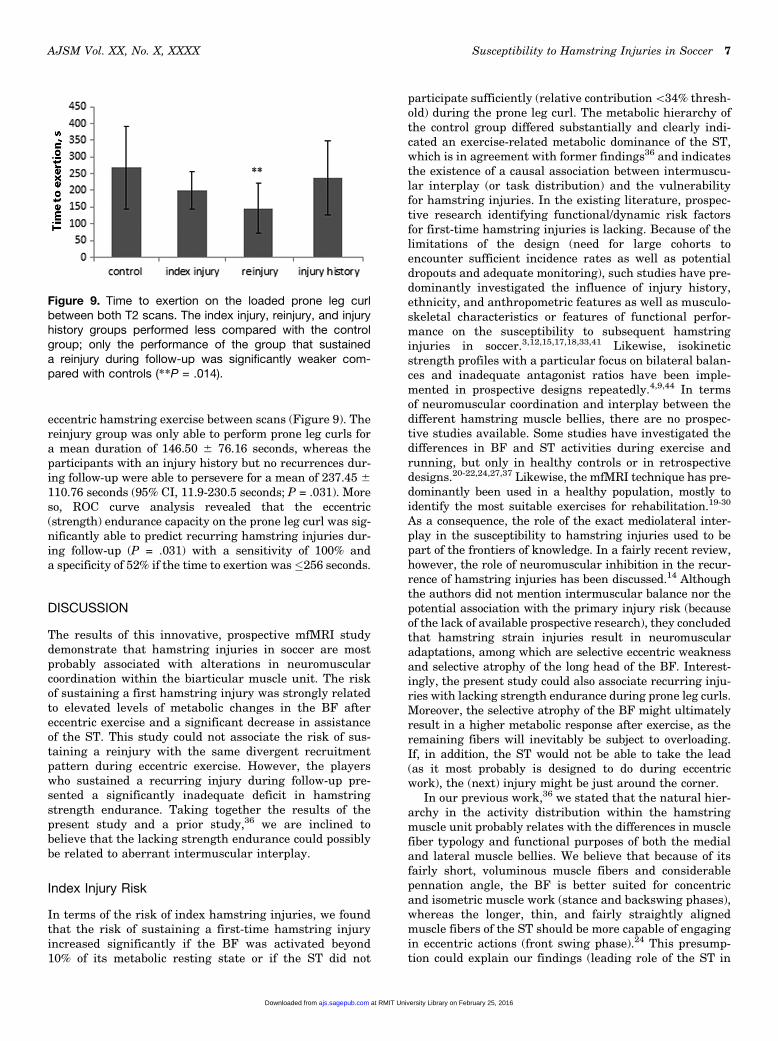
eccentric hamstring exercise between scans (Figure 9). Thereinjury group was only able to perform prone leg curls fora mean duration of 146.50 6 76.16 seconds, whereas theparticipants with an injury history but no recurrences dur-ing follow-up were able to persevere for a mean of 237.45 6
110.76 seconds (95% CI, 11.9-230.5 seconds; P = .031). Moreso, ROC curve analysis revealed that the eccentric(strength) endurance capacity on the prone leg curl was sig-nificantly able to predict recurring hamstring injuries dur-ing follow-up (P = .031) with a sensitivity of 100% anda specificity of 52% if the time to exertion was�256 seconds.
DISCUSSION
The results of this innovative, prospective mfMRI studydemonstrate that hamstring injuries in soccer are mostprobably associated with alterations in neuromuscularcoordination within the biarticular muscle unit. The riskof sustaining a first hamstring injury was strongly relatedto elevated levels of metabolic changes in the BF aftereccentric exercise and a significant decrease in assistanceof the ST. This study could not associate the risk of sus-taining a reinjury with the same divergent recruitmentpattern during eccentric exercise. However, the playerswho sustained a recurring injury during follow-up pre-sented a significantly inadequate deficit in hamstringstrength endurance. Taking together the results of thepresent study and a prior study,36 we are inclined tobelieve that the lacking strength endurance could possiblybe related to aberrant intermuscular interplay.
Index Injury Risk
In terms of the risk of index hamstring injuries, we foundthat the risk of sustaining a first-time hamstring injuryincreased significantly if the BF was activated beyond10% of its metabolic resting state or if the ST did not
participate sufficiently (relative contribution\34% thresh-old) during the prone leg curl. The metabolic hierarchy ofthe control group differed substantially and clearly indi-cated an exercise-related metabolic dominance of the ST,which is in agreement with former findings36 and indicatesthe existence of a causal association between intermuscu-lar interplay (or task distribution) and the vulnerabilityfor hamstring injuries. In the existing literature, prospec-tive research identifying functional/dynamic risk factorsfor first-time hamstring injuries is lacking. Because of thelimitations of the design (need for large cohorts toencounter sufficient incidence rates as well as potentialdropouts and adequate monitoring), such studies have pre-dominantly investigated the influence of injury history,ethnicity, and anthropometric features as well as musculo-skeletal characteristics or features of functional perfor-mance on the susceptibility to subsequent hamstringinjuries in soccer.3,12,15,17,18,33,41 Likewise, isokineticstrength profiles with a particular focus on bilateral balan-ces and inadequate antagonist ratios have been imple-mented in prospective designs repeatedly.4,9,44 In termsof neuromuscular coordination and interplay between thedifferent hamstring muscle bellies, there are no prospec-tive studies available. Some studies have investigated thedifferences in BF and ST activities during exercise andrunning, but only in healthy controls or in retrospectivedesigns.20-22,24,27,37 Likewise, the mfMRI technique has pre-dominantly been used in a healthy population, mostly toidentify the most suitable exercises for rehabilitation.19-30
As a consequence, the role of the exact mediolateral inter-play in the susceptibility to hamstring injuries used to bepart of the frontiers of knowledge. In a fairly recent review,however, the role of neuromuscular inhibition in the recur-rence of hamstring injuries has been discussed.14 Althoughthe authors did not mention intermuscular balance nor thepotential association with the primary injury risk (becauseof the lack of available prospective research), they concludedthat hamstring strain injuries result in neuromuscularadaptations, among which are selective eccentric weaknessand selective atrophy of the long head of the BF. Interest-ingly, the present study could also associate recurring inju-ries with lacking strength endurance during prone leg curls.Moreover, the selective atrophy of the BF might ultimatelyresult in a higher metabolic response after exercise, as theremaining fibers will inevitably be subject to overloading.If, in addition, the ST would not be able to take the lead(as it most probably is designed to do during eccentricwork), the (next) injury might be just around the corner.
In our previous work,36 we stated that the natural hier-archy in the activity distribution within the hamstringmuscle unit probably relates with the differences in musclefiber typology and functional purposes of both the medialand lateral muscle bellies. We believe that because of itsfairly short, voluminous muscle fibers and considerablepennation angle, the BF is better suited for concentricand isometric muscle work (stance and backswing phases),whereas the longer, thin, and fairly straightly alignedmuscle fibers of the ST should be more capable of engagingin eccentric actions (front swing phase).24 This presump-tion could explain our findings (leading role of the ST in
Figure 9. Time to exertion on the loaded prone leg curlbetween both T2 scans. The index injury, reinjury, and injuryhistory groups performed less compared with the controlgroup; only the performance of the group that sustaineda reinjury during follow-up was significantly weaker com-pared with controls (**P = .014).
AJSM Vol. XX, No. X, XXXX Susceptibility to Hamstring Injuries in Soccer 7
at RMIT University Library on February 25, 2016ajs.sagepub.comDownloaded from

eccentric muscle effort) and could account for the particu-lar injury vulnerability of the BF in running and kicking.In agreement with this hypothesis, Higashihara and col-leagues20 reported a discrepancy between the onset ofpeak muscle stretch and peak EMG activity in the ham-string muscle unit throughout the explosive front swingphase in sprinting, with the BF reaching peak EMG activ-ity after the onset of peak muscle stretch. The ST, on theother hand, presented peak EMG activity before peakstretch. These findings support our train of thought, asthey indicate that the ST is perfectly able to engage inrapid eccentric contractions, effectively controlling flexionand extension torque generated around the hip and kneejoints, whereas the BF does not seem to be. Consequently,the alterations in absolute and relative metabolic activitieswithin the hamstring muscle unit caused by eccentric exer-cise are most probably partly responsible for an increasedrisk of sustaining a functional or structural injury.
Recurring Injury Risk
In contrast with our original hypothesis, we were not able toassociate this divergent muscle recruitment pattern withthe risk of sustaining a recurring hamstring injury. Inter-estingly and in line with what has previously beenstated,8,14,40 the reinjury group performed strikingly weaklyon prone leg curls, indicating an insufficient hamstringload-bearing capacity and an unjustified return to play.ROC curve analysis demonstrated that the time to exertionon prone leg curls, a parameter for hamstring musclestrength endurance, was able to predict the recurrence ofhamstring injuries within our cohort. This study could notdemonstrate that the intramuscular recruitment patternand interplay are related to the risk of sustaining a recur-ring hamstring injury, as the metabolic activation patternof the participants with a recurring injury during follow-up did not differ from those with a history but no recurrenceduring follow-up. Because the cohort in which this patternwas assessed in relation to the reinjury risk was small (n= 17), these results must be interpreted carefully, as lackingpower might have influenced the outcome. However, inaccordance with the results of the present study, predomi-nantly, the functional muscle output and strength capacityseem to be key for secondary prevention.
Association Between Metabolic Muscle Featuresand Strength Endurance
In agreement with previous research,36 this study revealedsubstantially lower strength endurance in both the indexand reinjury groups, corresponding with a higher anda similar metabolic expense, respectively. This findingonce again indicates that the hamstring muscles of theplayers who sustained a first or recurring injury functionless effectively (probably because of the divergent inter-muscular interplay), which causes them to acidify moreeasily and probably makes them more prone to functionaland structural injuries.10,36
Next to this potentially locally mediated decrease infatigue tolerance (deviated intermuscular hierarchy and
muscle recruitment), central fatigue mechanisms alteringperipheral motor output characteristics might play a roleas well. It has been demonstrated repeatedly that muscleinjuries tend to occur more frequently toward the end ofthe season or the end of a match (later half).10-12,34
Aside from peripheral fatigue mechanisms due to meta-bolic changes in muscle and cardiorespiratory systems,centrally mediated fatigue, caused by changes in the cen-tral nervous system (mostly by alterations in autonomicand hormonal balances), will also cause the muscle to con-tract in a less coordinated manner, subjecting it to func-tional and/or structural injuries.26,28,35,38 As we evaluatedlocal strength endurance by means of a prone leg curl toexertion, we believe that we predominantly verified thecharacteristics of local metabolic muscle functioning ratherthan the fatigue tolerance and load-bearing capacity of thecentral nervous system. Consequently, we cannot discussthe possible influence of centrally mediated fatigue (toler-ance) in the reinjury risk based on the present results. Ifwe had intended to monitor central fatigue and its associ-ation with hamstring (re)injuries during follow-up, weshould have included outcome measures to assess possibleoverreaching/overtraining,28,35 as well as hormonal orautonomic nervous system homeostasis, with additionalfunctional exercise capacity screens (peak VO2 estimation,heart rate at maximum running speed or maximum aero-bic speed,17,42 yo-yo intermittent test,25 etc). We specifi-cally chose to verify the role of local metabolic musclefunction characteristics and their intermuscular coordina-tion in the risk of hamstring injuries in soccer, so the influ-ence of centrally mediated fatigability of the participantsin terms of their injury vulnerability was beyond the scopeof this study. On the basis of what has been demonstratedin this study as well as the results from previous researchassessing peripheral/local and central fatigability,26,28,35,38
we believe that the latter is a considerable risk factor forboth primary and secondary muscle injuries, whereas localfatigability probably predominantly deteriorates in thepresence of a history of muscle injuries because of morpho-logical and functional changes in the previously injuredmuscle unit.14,36 Therefore, the evaluation of local musclestrength endurance (preferably with mfMRI quantifica-tion) seems to be ideally suited for investigating deviatingmuscle function (coordination) after an injury and to verifythe risk of recurrence.
Clinical Message
On the basis of the present results, we suggest that thehierarchic shift in the metabolic activity contribution ismost probably (partly) responsible for the first hamstringstrain injury and that this altered pattern of muscle activa-tion is associated with poorer strength endurance.36 Bear-ing this in mind and presuming that a deviated activationpattern could be both a cause and consequence of ham-string strain injuries in soccer, the quality of the recruit-ment pattern should be adequately acknowledged inpreventing first and recurring hamstring injuries.
The findings of this prospective study indicate thata perfectly and functionally balanced out BF-ST unit
8 Schuermans et al The American Journal of Sports Medicine
at RMIT University Library on February 25, 2016ajs.sagepub.comDownloaded from

appears to be of major importance in the prevention ofhamstring (re)injuries and, most probably, in the athlete’sperformance as well. In attempting to protect the BFagainst structural or functional damage, the clinicianshould bear in mind this natural intramuscular hamstringhierarchy and effectively train both the BF and ST plyo-metrically, dominantly addressing the ST during heavyeccentric loading in the distal range of motion. Further-more, prone leg curls with eccentric overloading could beimplemented as an exercise and a test for the purpose ofrehabilitation and determining the readiness for returnto play in community-level soccer players, with a cutoffvalue of 4 minutes and 30 seconds.
Limitations
For the limitations to this study, we partly refer the readerto the previous work as well.36 Because of the prospectivedesign, the distinction between index and recurring inju-ries, and the high costs of the mfMRI protocol, the samplesizes for between-group comparison were small. This low-ers the power of this study considerably, which must beacknowledged when drawing conclusions. Future large-scale prospective research using mfMRI for the assessmentof the importance of intermuscular interplay/coordinationin the risk of hamstring (re)injuries is needed to be ableto affirm or refute the results of this preliminary study.However, this is the very first prospective mfMRI studyto assess metabolic hamstring characteristics and intra-muscular activation features for the purpose of identifyingthe risk of index injuries and reinjuries in soccer.
CONCLUSION
This is the first prospective study using mfMRI to assess theinfluence of metabolic muscle functioning and neuromuscu-lar coordination in the context of identifying the risk of ham-string injuries. The present results indicated that theoccurrence of index hamstring injuries could be associatedwith a hierarchical change in the metabolic activity distri-bution within the hamstring muscle complex after eccentricwork in which the ST is most probably meant to take theleading part, followed by the BF and SM. When the BFincreases its contribution and is activated to a proportionallyhigher extent, the risk of sustaining an index hamstringinjury might increase substantially. This study is also thefirst to assess the risk factors for index and recurring inju-ries, considering both injury entities separately butacknowledging their similarity and interindependence. Sub-jects with reinjuries within our cohort presented a particu-larly weak performance capacity on prone leg curls. Thistype of heavy eccentric exercise or test might be suitablefor determining the athlete’s readiness to return to play.The athlete should be able to perform the standardizedprone leg curl with 5 kg attached to each foot, at a standard-ized pace of 90 Hz for at least 4 minutes and 30 seconds,before safely returning to competition.
ACKNOWLEDGMENT
The authors gratefully acknowledge the assistance of P.Vandemaele, engineer at Ghent University Hospital, forhis assistance in MRI scanning and data processing. Fur-thermore, we thank Steven Heyndrickx, a highly appreci-ated former colleague at the Department of RehabilitationSciences and Physiotherapy, for the assembly of the onlinediary for injury registration during follow-up. Last but notleast, the authors thank the participants of this study, with-out whom this prospective study could have never been com-pleted successfully. For its financial support, the authors’gratitude goes out to the IWT (Brussels, Belgium), whomade this MRI research possible.
REFERENCES
1. Akima H, Kinugasa R, Kuno S. Recruitment of the thigh muscles dur-
ing sprint cycling by muscle functional magnetic resonance imaging.
Int J Sports Med. 2005;26:245-252.
2. Akima H, Takahashi H, Kuno S, et al. Coactivation pattern in human
quadriceps during isokinetic knee-extension by muscle functional
MRI. Eur J Appl Physiol. 2004;91:7-14.
3. Askling CM, Tengvar M, Saartok T, et al. Acute first-time hamstring
strains during high speed running: a longitudinal study including clin-
ical and magnetic resonance imaging findings. Am J Sports Med.
2007;35:197-206.
4. Bennell K, Wajswelner H, Lew P, et al. Isokinetic strength testing
does not predict hamstring injury in Australian rules footballers. Br
J Sports Med. 1998;32(4):309-314.
5. Cagnie B, Elliot J, O’Leary S, et al. Muscle functional MRI as an imag-
ing tool to evaluate muscle activity. J Orthop Sports Phys Ther.
2011;41:896-903.
6. Chumanov ES, Heiderscheit BC, Thelen DG. Hamstring musculoten-
don dynamics during stance and swing phases of high-speed run-
ning. Med Sci Sports Exerc. 2011;43:525-532.
7. Clark BC, Walkowski S, Conatser R, et al. Muscle functional mag-
netic resonance imaging and acute low back pain: a pilot study to
characterize lumbar muscle activity asymmetries and examine the
effects of osteopathic manipulative treatment. Osteopath Med Prim
Care. 2009;3:1-10.
8. Croisier JL, Forthomme B, Namurois MH, Vanderthommen M,
Crielaard JM. Hamstring muscle strain recurrence and strength per-
formance disorders. Am J Sports Med. 2002;30(2):199-203.
9. Croisier JL, Ganteaume S, Binet J, Genty M, Ferret JM. Strength
imbalances and prevention of hamstring injury in professional soccer
players: a prospective study. Am J Sports Med. 2008;36(8):1469-1475.
10. Ekstrand J, Askling C, Magnusson H, et al. Return to play after thigh
muscle injury in elite football players: implementation and validation
of the Munich muscle injury classification. Br J Sports Med.
2013;47(12):769-774.
11. Ekstrand J, Hagglund M, Walden M. Injury incidence and injury pat-
terns in professional football: the UEFA injury study. Br J Sports Med.
2011;45:553-558.
12. Engebretsen AH, Myklebust G, Holme I, Engebretsen L, Bahr R. Intrin-
sic risk factors for hamstring injuries among male soccer players:
a prospective cohort study. Am J Sports Med. 2010;38(6):1147-1153.
13. Fisher MJ, Meyer RA, Adams GR, et al. Direct relationship between
proton T2 and exercise intensity in skeletal muscle MR images. Invest
Radiol. 1990;25:480-485.
14. Fyfe JJ, Opar DA, Williams MD, Shield AJ. The role of neuromuscular
inhibition in hamstring strain injury recurrence. J Electromyogr Kine-
siol. 2013;23(3):523-530.
15. Gabbe BJ, Bennell KL, Finch CF, Wajswelner H, Orchard JW. Predic-
tors of hamstring injury at the elite level of Australian football. Scand J
Med Sci Sports. 2006;16(1):7-13.
AJSM Vol. XX, No. X, XXXX Susceptibility to Hamstring Injuries in Soccer 9
at RMIT University Library on February 25, 2016ajs.sagepub.comDownloaded from

16. Gabbe BJ, Finch CF, Bennell KL, Wajswelner H. Risk factors for ham-
string injuries in community level Australian football. Br J Sports Med.
2005;39(2):106-110.
17. Gonzalez-Mohıno Mayoralas F, Gonzalez-Rave JM, Juarez D, de Asıs
F, Barragan Castellanos R, Newton RU. Effects of continuous and
interval training on running economy, maximal aerobic speed and
gait kinematics in recreational runners [published online September
3, 2015]. J Strength Cond Res. doi:10.1519/JSC.0000000000001174.
18. Henderson G, Barnes CA, Portas MD. Factors associated with
increased propensity for hamstring injury in English Premier League
soccer players. J Sci Med Sport. 2010;13(4):397-402.
19. Hicke J, Shield AJ, Williams MD, et al. The financial cost of hamstring
strain injuries in the Australian football league. Br J Sports Med.
2014;48:729-730.
20. Higashihara A, Nagano Y, Ono T, et al. Relationship between the
peak time of hamstring stretch and activation during sprinting. Eur
J Sport Sci. 2014;31:1-6.
21. Higashihara A, Ono T, Kubota J, et al. Functional differences in the
activity of the hamstring muscles with increasing running speed.
J Sports Sci. 2010;28:1085-1092.
22. Higashihara A, Ono T, Kubota J, et al. Functional differences
between individual hamstring muscles at different running speeds.
Med Sci Sports Exerc. 2010;42:404-410.
23. Kellis E, Galanis N, Kapetanos G, et al. Architectural differences
between the hamstring muscles. J Electromyogr Kinesiol. 2012;
22:520-526.
24. Kubota J, Ono T, Araki M, et al. Non-uniform changes in magnetic
resonance measurements of the semitendinosus muscle following
intensive eccentric exercise. Eur J Appl Physiol. 2007;101:713-
720.
25. Macpherson TW, Weston M. The effect of low-volume sprint interval
training on the development and subsequent maintenance of aerobic
fitness in soccer players. Int J Sports Physiol Perform. 2015;10(3):
332-338.
26. Marshall PW, Lovell R, Jeppessen GK, Andersen K, Siegler JC. Ham-
string muscle fatigue and central motor output during a simulated
soccer match. PLoS One. 2014;9(7):e102753.
27. McAllister MJ, Hammond KG, Schilling BK, et al. Muscle activation
during various hamstring exercises. J Strength Cond Res.
2014;28:1573-1580.
28. Meeusen R, Duclos M, Foster C, et al. Prevention, diagnosis, and
treatment of the overtraining syndrome: joint consensus statement
of the European College of Sports Science and the American College
of Sports Medicine. Med Sci Sports Exerc. 2013;54(1):186-205.
29. Mendiguchia J, Garrues MA, Croninc JB, et al. Nonuniform changes
in MRI measurements of the thigh muscles after two hamstring
strengthening exercises. J Strength Cond Res. 2013;27:574-581.
30. Mendiguchia J, Los Arcos A, Garrues MA, et al. The use of MRI to
evaluate posterior thigh muscle activity and damage during Nordic
hamstring exercise. J Strength Cond Res. 2013;27:3426-3435.
31. Oliver G, Dougherty C. Comparison of hamstring and gluteus
muscles electromyographic activity while performing the razor curl
vs. the traditional prone hamstring curl. J Strength Cond Res.
2009;23:2250-2255.
32. Onishi H, Yagi R, Oyama M, et al. EMG-angle relationship of the
hamstring muscle during knee flexion. J Electromyogr Kinesiol.
2002;12:399-406.
33. Opar D, Williams MD, Shield AJ. Hamstring injuries: factors that lead
to injury and re-injury. Sports Med. 2012;42:209-226.
34. Pattyn EP, Verdonk A, Steyaert D, et al. Muscle functional MRI to
evaluate quadriceps dysfunction in patellofemoral pain. Med Sci
Sports Exerc. 2013;45:1023-1029.
35. Piacentini MF, Meeusen R. An online training monitoring system to
prevent non-functional overreaching. Int J Sports Physiol Perf.
2015;10(4):524-527.
36. Schuermans J, Van Tiggelen D, Danneels L, et al. Biceps femoris and
semitendinosus: team mates of competitors? New insights into ham-
string injury mechanisms in male football players: a muscle functional
MRI study. Br J Sports Med. 2014;48:1599-1606.
37. Segal RL. Use of imaging to assess normal and adaptive muscle
function. Phys Ther. 2007;87:704-718.
38. Small K, McNaughton LR, Greig M, Lohkamp M, Lovell R. Soccer
fatigue, sprinting and hamstring injury risk. Int J Sports Med.
2009;30(8):573-578.
39. Sole G, Milosavljevic S, Nicholson H, et al. Altered muscle activation
following hamstring injuries. Br J Sports Med. 2012;46:118-123.
40. Tol JL, Hamilton B, Eirale C, Muxart P, Jacobsen P, Whiteley R. At
return to play following hamstring injury the majority of professional
football players have residual isokinetic deficits. Br J Sports Med.
2014;48(18):1364-1369.
41. Verrall GM, Slavotinek JP, Barnes PG, Fon GT, Spriggins AJ. Clinical
risk factors for hamstring muscle strain injury: a prospective study
with correlation of injury by magnetic resonance imaging. Br J Sports
Med. 2001;35(6):435-439.
42. Vesterinen V, Nummela A, Ayramo S, et al. Monitoring training adap-
tation with a submaximal running test in field conditions [published
online August 26, 2015]. Int J Sports Physiol Perform. doi:10.1123/
ijspp.2015-0366.
43. Woods C, Hawkins RD, Maltby S, et al. The Football Association Med-
ical Research Programme: an audit of injuries in professional football.
Analysis of hamstring injuries. Br J Sports Med. 2004;38:36-41.
44. Yeung SS, Suen AM, Yeung EW. A prospective cohort study of ham-
string injuries in competitive sprinters: preseason muscle imbalance
as a possible risk factor. Br J Sports Med. 2009;43(8):589-594.
For reprints and permission queries, please visit SAGE’s Web site at http://www.sagepub.com/journalsPermissions.nav.
10 Schuermans et al The American Journal of Sports Medicine
at RMIT University Library on February 25, 2016ajs.sagepub.comDownloaded from





























