Embed Size (px)
Citation preview

UTS:HEALTH
DETERMINING QUALITY OF LIFE -A NURSING PERSPECTIVE
health.uts.edu.au
Janet Green RN [email protected]@janetagreen
UTS:HEALTHhealth.uts.edu.au
“The special vulnerability of verypremature infants under theassault of modern intensive caretechniques evokes strongresponses: both the desire to
sustain their fragile existence anddoubts about the wisdom of
doing so…” McCormick, M.C. 1994, ‘Survival of very tiny babies –Good news and bad news’, The New England Journal of Medicine, vol. 331, no. 12, Sep 2, pp. 801-803.

UTS:HEALTH
BEFORE WE GET STARTED: 1. How would you define
quality of life (QOL) for you?2. What is the level at which
you think you wouldprefer not to live?
- brain / cognition- ability / disability- taking care of basic needs
health.uts.edu.au

If you have trouble deciding a level of “qualityof life” for you, imagine how hard it would be tobe the parents of an extremely premature babyand being asked to be part of these decisions.
It is essential that parents are part of thedecisions, because those most affected bythese decisions should have a say, however itis impossible for them to project themselvesinto the future.
health.uts.edu.au
UTS:HEALTHhealth.uts.edu.au
Microprem –defined as 24 weeks gestation and less
Although the majority of infants with GAs of ≥24 weeks survive, high rates of morbidity among survivors continue to be observed.Stoll, B.J., Hansen, N.I., Bell, E.F., Shankaran, S., Laptook, A.R., Walsh, M.C., Hale, E.C., Newman, N.S., Schibler, K., Carlo, W.A. and Kennedy, K.A., 2010. Neonatal outcomes of extremely preterm infants from the NICHD Neonatal Research Network. Pediatrics, pp.peds-2009.

UTS:HEALTHhealth.uts.edu.au
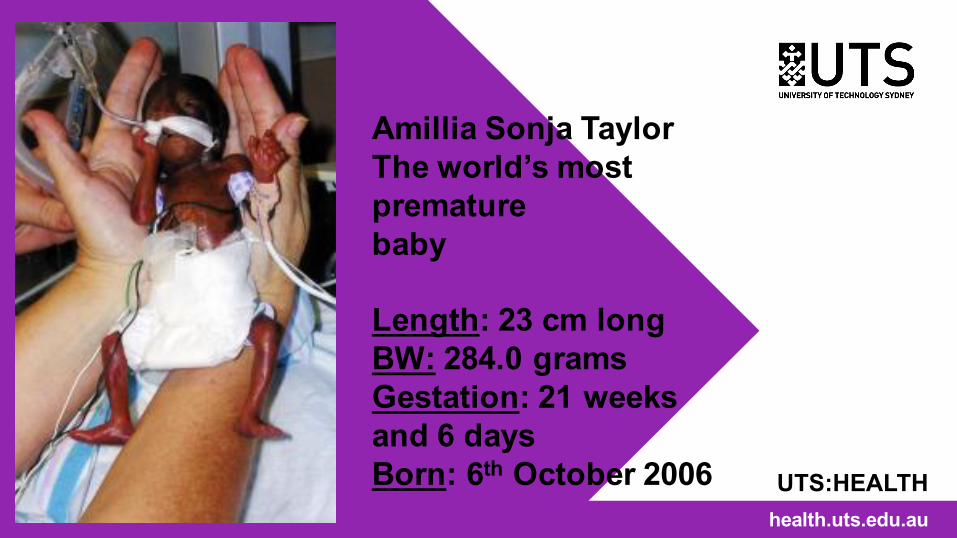
Amillia Sonja TaylorThe world’s most premature baby
Length: 23 cm longBW: 284.0 gramsGestation: 21 weeks and 6 daysBorn: 6th October 2006

THE GROWING BABY
22 weeks 27.8 cm 430 grams
23 weeks 28.9 cm 501 grams
24 weeks 30 cm 600 grams
25 weeks 34.6 cm 660 grams
health.uts.edu.au
LENGTH WEIGHT
http://www.babycenter.com.au/a1004000/average-fetal-length-and-weight-chart
A CASE STUDY - 1• Mother 38 years old• Primigravida – first viable pregnancy but multiple
miscarriages• 23+4 weeks pregnant• Conceived using IVF technologies• Premature / Prolonged rupture of membranes for 3 days
and niggling contractions• Given 2 doses of steroids – enhance lung development• ? urinary tract infection – antibiotics• Visited by the neonatologist and neonatal nurse
health.uts.edu.au

WHAT INFORMATION DID THE NEONATOLOGIST GIVE THE EXPECTANT MOTHER?
• Evidence about clinical management• Evidence about survival and outcome – it is difficult
to separate out the statistics of babies of this gestation
• Possible options – parental choice / wishes / IVF adds to the complexity
AFTER THE DISCUSSION• Mother frightened for her baby• Mother hopeful for a good outcome – “babies all do
well now and survive don’t they?”• Mother hopes that her baby will not be one of the
statisticshealth.uts.edu.au

Extremely low birth weight survival hasimproved with the widespread use ofsurfactant agents, maternal steroids,and advancements in neonataltechnologies.
The minimum age of viability is nowas young as 23 weeks' gestation, withscattered reports of survivors born at21-22 weeks' estimated gestation.
NOTE: Survival is not necessarilyequated with outcome

UTS:HEALTHhealth.uts.edu.au

POSSIBLE OUTCOMEFour factors should be considered in addition to gestational age when determining the likelihood of favorable outcome with intensive care:• Gender - Female gender has the more favorable
outcome• Exposure to antenatal corticosteroids (with
favorable effect)• Single or multiple birth - Single birth has a favorable
effect• Birth weight - Increasing increments of 100g each
add to favorable outcome potential

HOW DO WE INTERPRET THE RESEARCH ON OUTCOMES?
• The most important factor in counselling families is the interpretation of data on survival rates.
• Published data can be confusing – there is wide variation in reported survival rates.
• Different rates of survival – based on geography or single unit institutions – based on cohorts not individual babies – some centres do better than others.
• GOLD STANDARD – population-based studies that report the outcome of all babies alive at the onset of labour (or potential live births) –rates of survival lower (but more accurate) as they use total births
• How is disability defined?
health.uts.edu.au
Smith, L. K., Draper, E. S., & Field, D. (2014, April). Long-term outcome for the tiniest or most immature babies: survival rates. In Seminars in Fetal and Neonatal Medicine (Vol. 19, No. 2, pp. 72-77). WB Saunders.

A CASE STUDY - 2• Cervix 7cm dilated – delivered by vaginal delivery• Full resuscitation – intubated, surfactant, ventilated. • Weight 510 grams• Umbilical vein & artery catheterised and lines inserted• IV fluids• Inotropes• Blood gas measurements• Antibiotics• You either resuscitate fully
or not at all – waiting is not an option – babies can be damaged
health.uts.edu.au

UTS:HEALTHhealth.uts.edu.au
Kimberley Mueller –weighed 10 ounces (283.5g)Born in Hanover Germany
1.bp.blogspot.com/.../bab1BILD2709_468x302.jpg
WHAT TO DO WITH A 23 WEEKER…..• The question of what to do in the case of extreme
prematurity (≤23 weeks' gestation) is a difficult one. • Gestational age, which is typically based on the
mother's recount of her last menstrual period, can differ from the actual gestational age by as much as 2 weeks, even when the latest ultrasonographic technology is used – IVF more accurate
• Most centres do not have minimum birth weight criteria for resuscitation, and often a "trial of life" may be discussed with the parents before the birth so that the infant can be resuscitated and evaluated for viability after birth.
health.uts.edu.au
WHERE THE BABY IS BORN MATTERS• Community medical professionals are doing their best to
provide care to stabilise critical neonates without reducing their chances of survival.
• Increased length of stay and higher rate of retinopathy of prematurity in transported premature babies suggest that differences in medical management during the first few hours of life may adversely affect outcomes.
• The “golden hour” – impacts on the outcome
health.uts.edu.au
Kuo, S., Kimata, C., Akamine, K., Young, B. and Balaraman, V., 2012. Outcomes of inborn and transported extremely premature very-low-birthweight infants in Hawai ‘i. Pediatrics International, 54(3), pp.365-369.
Mohamed, M.A. and Aly, H., 2010. Transport of premature infants is associated with increased risk for intraventricular haemorrhage. Archives of Disease in Childhood-Fetal and Neonatal Edition, 95(6), pp.F403-F407.

OUTCOME DATA
health.uts.edu.au
http://www.babymed.com/sites/default/files/u160962/preterm-survival-rates_0.jpg

CASE STUDY - 3• Day 2 - Grade III Intraventricular haemorrhage (IVH)
• Day 8 Patent Ductus Arteriosus (PDA) – given indomethacin to close
health.uts.edu.au
http://neuropathologyweb.org/chapter3/chapter3dGmh.html
http://www.chw.org/medical-care/herma-heart-center/conditions/patent-ductus-arteriosus/

CASE STUDY - 4• Day 10 Necrotising Enterocolitis (NEC)
• Day 15 Surgical intervention – removal of part of the small bowel and formation of temporary ileostomy
• Total parenteral nutrition (TPN) – causes liver dysfunctionhealth.uts.edu.au
http://limejournal.co.uk/?p=2767
https://en.wikipedia.org/wiki/Necrotizing_enterocolitis
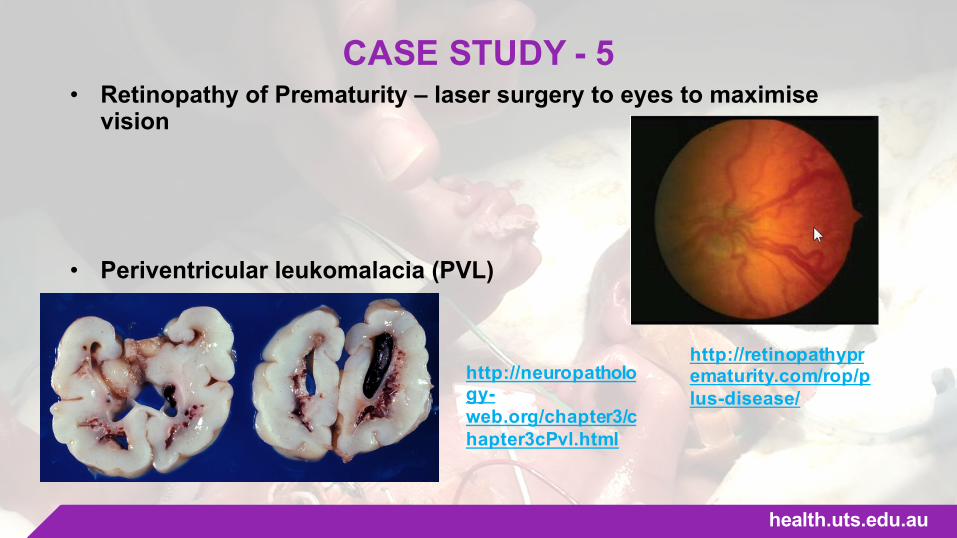
CASE STUDY - 5• Retinopathy of Prematurity – laser surgery to eyes to maximise
vision
• Periventricular leukomalacia (PVL)
health.uts.edu.au
http://retinopathyprematurity.com/rop/plus-disease/
http://neuropathology-web.org/chapter3/chapter3cPvl.html

CASE STUDY - 6
• IVF parents – desperation to be parents• Multiple painful procedures and diagnostic tests• Multiple infections and antibiotics• Multiple blood transfusions• Discussions with family – Quality of life• Discussions with family - Withdrawal of treatment• Outcome? • Uncertainty
health.uts.edu.au

WHAT IS QUALITY OF LIFE?• Use of the term ‘‘quality of life’’ is almost always
controversial. • Diminished quality of life is a frequent consideration in
shaping the boundaries of medical intervention. • Quality of life is one of the most important,
controversial and emotionally charged issues in contemporary clinical bioethics.
• Quality of life is a broad multidimensional concept that usually includes subjective evaluations of both positive and negative aspects of life.
• The purpose of QOL determinations are to decide when a life lacks sufficient quality that it ought not be lived.
health.uts.edu.au
WHAT IS QUALITY OF LIFE?• Quality of life is both objective and subjective, and
one of the major problems with considering QOL is the question of how this is defined and by whom.
• An objective view of someone’s life may be very different to the view of the person who is living that life.
• An extremely premature baby cannot make their own decisions or voice their perceived quality of life status, and their full outcome might not be known for several years.
• Parental input into decisions about treatment withdrawal or continuation frequently involve concerns about the future of the family, as well as the child.
health.uts.edu.au
WHAT IS QUALITY OF LIFE?• Surrogates are required to consider the best interest
of the patient, where the burdens to the patient clearly outweigh the benefits, where suffering is the primary burden and pleasure is the primary benefit.
• There may be some circumstances where an extremely premature baby’s QOL, however defined, is so poor that it should not be maintained even if it is possible to do so.
health.uts.edu.au
WHAT IS QUALITY OF LIFE?• There is ambiguity and confusion in the literature
about what QOL means, therefore there is a lack of agreement about how to define it.
• Many of the definitions of QOL do not offer any understandings of the lived human experience, but rather consider functional abilities and the degree of satisfaction of dissatisfaction, often from the viewpoint of others.
It should be remembered that QOL isnot about making judgements aboutthe value or worth of a particular life.
health.uts.edu.au

UTS:HEALTHhealth.uts.edu.au
An exploration of the ethical issues experienced by neonatal nurses concerning the care and management of babies 24 weeks gestation and less
All publications available free on ResearchGatehttps://www.researchgate.net/profile/Janet_Green2

Please remember that I am speaking about babies of 24
weeks gestation and less only. This research is not
generalisable to any other premature babies!!!!!
Neonatal nurses are beginning to question the value of aggressive
neonatal intensive care for babies of marginal viability in light of
recent outcome studies that show that these babies have a very real
prospect for disability.

WHY THE RESEARCH?
• Nurses should enter the debate aboutsaving tiny babies.• Nurses could contribute, but historically
have not had a voice.• Nurses constitute the largest population
of staff in the NICU.
health.uts.edu.au

THE RESEARCH
• Questionnaire to all members ofAustralian Neonatal Nurses Association
• Ethics approval from Flinders UniversitySth Australia
Q/A addressed issues related to:- feelings / attitudes / beliefs- ethical issues- social issues- legal issues- technology of the future
health.uts.edu.au
THE RESEARCH• SPSS analysis• Major issues discovered from analysis
of questionnaires (414 = 54% responserate)
• 14 Interviews with 24 neonatal nurses– single / focus group- Perinatal / tertiary centres (11) - Neonatal retrieval team (1)- Surgical centres (3)• Every large centre in New South Wales
health.uts.edu.au
UTS:HEALTHhealth.uts.edu.au
Amillia Sonja TaylorThe world’s most premature baby
Length: 23 cm longBW: 284.0 gramsGestation: 21 weeks and 6 daysBorn: 6th October 2006

AMILLIA SONJA TAYLOR
• The “poster girl” for extreme prematurity• Born: 6th October 2006• Name typed into Google on 29/3/2016 -
about 12,700 results• Google images – latest photo is when
she was 2 years old.• Websites say her parents want to keep
her out of the spotlight.• 2016 – her outcome?
health.uts.edu.au
http://www.growingyourbaby.com/2008/10/25/amillia-taylor-turns-2/

Questionnaire data
Frequency Percent
Disagree 8 2.0
Agree 374 93.5
Neutral 18 4.5
Total 400 100.0
health.uts.edu.au
“When making decisions for infants of 24 weeks gestation and less, quality of life must be a critical factor to be considered”.
• The results showed that 374 out of 400 or 93.5% of respondents believed that quality of life should be considered when making decisions for extremely premature babies.
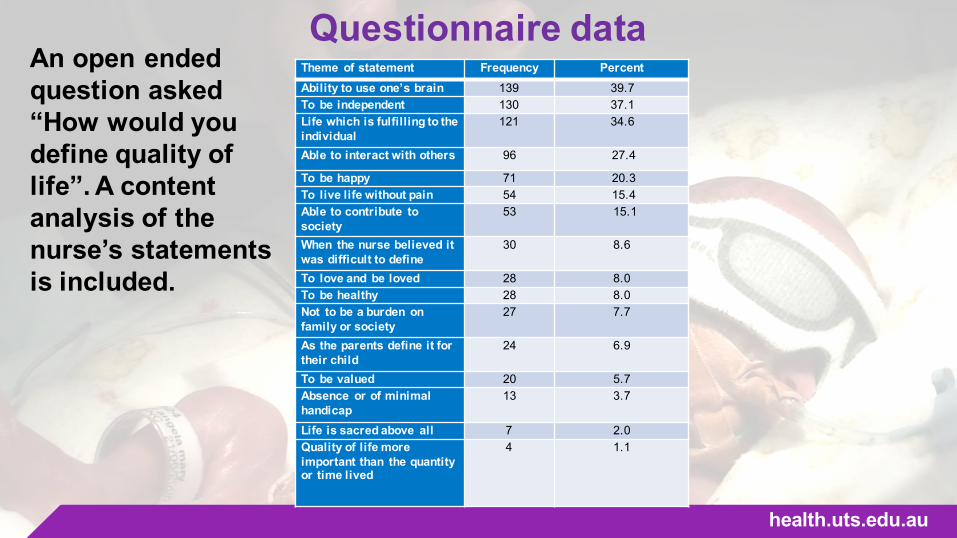
Questionnaire data
health.uts.edu.au
Theme of statement Frequency PercentAbility to use one’s brain 139 39.7To be independent 130 37.1Life which is fulfilling to the individual
121 34.6
Able to interact with others 96 27.4
To be happy 71 20.3To live life without pain 54 15.4Able to contribute to society
53 15.1
When the nurse believed it was difficult to define
30 8.6
To love and be loved 28 8.0To be healthy 28 8.0Not to be a burden on family or society
27 7.7
As the parents define it for their child
24 6.9
To be valued 20 5.7Absence or of minimal handicap
13 3.7
Life is sacred above all 7 2.0Quality of life more important than the quantity or time lived
4 1.1
An open ended question asked “How would you define quality of life”. A content analysis of the nurse’s statements is included.
QUALITY OF LIFE“I think if you’ve got a baby that’s going to never grow, never feed, never know anything of life other than more pain – that is not quality of life. But a child that is at least going to be able to receive something, hear something or see something, touch, taste, feel something. Have some of his five senses . . he can receive something. He’s going to have an amount of quality of life. If you take all of those away, what have you got? Just a body! And that’s not quality of life.” (Nurse 9)
health.uts.edu.au
Green, J., Darbyshire, P., Adams, A., & Jackson, D. (2016). Quality versus quantity: The complexities of quality of life determinations for neonatal nurses.Nursing Ethics, 0969733015625367

QUALITY OF LIFEQuality of life for the family is important
“I think as they [baby] become more that person, they gain more right to life. I think down this end of the spectrum, the family has more right to their life than that baby does. Sure it’s a life, but the life that that family has . . The siblings and everyone, they’ve got a life, they’ve got expectations and plans. They’ve got a right to that, more than the baby has.” (Nurse 14)
health.uts.edu.au
Green, J., Darbyshire, P., Adams, A., & Jackson, D. (2016). Quality versus quantity: The complexities of quality of life determinations for neonatal nurses.Nursing Ethics, 0969733015625367

QUALITY OF LIFEQuality of life for the family is important
“They’re [parents] going to have to look after the child. It’s easy for me to turn around and say ‘Oh you should have the child no matter what’. But I’m not going to clothe it, I’m not going to feed it, I’m not going to be the one who’s going to have to pay for the special schooling or the physiotherapy or the special shoes or the glasses.” (Nurse 12)
health.uts.edu.au
Green, J., Darbyshire, P., Adams, A., & Jackson, D. (2016). Quality versus quantity: The complexities of quality of life determinations for neonatal nurses.Nursing Ethics, 0969733015625367
QUALITY OF LIFE• Imagining the baby’s future was common.
“You can just see it lying there, and you wonder how is this kid going to be. Is he going to end up lying in bed all day, not doing anything or in a wheelchair. Is he going to get something out of his life?” (Nurse 17)
health.uts.edu.au
Green, J., Darbyshire, P., Adams, A., & Jackson, D. (2016). Quality versus quantity: The complexities of quality of life determinations for neonatal nurses.Nursing Ethics, 0969733015625367

QUALITY OF LIFE• Imagining the baby’s future was common.
“I think most of our perceptions of babies of this gestation are that they face so many problems and such a stormy path if they do survive, that the outlook is extremely bleak. I think there are an awful lot of negatives. I think a lot of nurses have trouble getting past that.” (Nurse 4)
health.uts.edu.au
Green, J., Darbyshire, P., Adams, A., & Jackson, D. (2016). Quality versus quantity: The complexities of quality of life determinations for neonatal nurses.Nursing Ethics, 0969733015625367
CONCLUSION• Neonatal nurses believed that quality of life was an important
consideration, yet they experienced inner conflict and uncertainty when asked to suggest specific elements of quality of life, or to suggest how it might be determined.
• It was even more difficult for the nurses to say when an extremely premature baby’s life possessed or lacked quality.
• Their previous clinical and personal experiences led the nurses to believe that the quality of the family’s life was important, and possibly more so than the quality of life of the surviving baby.
• This finding contrasts markedly with much of the existing literature in this field.
• As is the case in ethics - I should leave you with more questions than answers
health.uts.edu.au





























