Embed Size (px)
Citation preview
Saturday May 16th, 9-11am (MST)Altitude Room; Crowne Plaza, Denver, Colorado
REG Small Airways Study Group Meeting
SASG Meeting Attendees
Lead: Richard Martin
• Keith Allan• Mona Bafadhel• Neil Barnes• Matthias Binek• Sonia Buist• Gene Colice• Glenn Crater• David Evans• Sian Feller• Tom Ferro• Armin Furtwaengler• Jonathan Grigg• Theresa Guilbert• Elliot Israel
• Susan Johnson• Dorothy Keininger• Alberto Papi• Wanda Phipatanakul*• David Price • Dirkje Postma**• Nicolas Roche• Guilherme Safioti• Peter Schweikert• Wim van Aalderen• Elisa Veratelli• Setareh Williams
Bold = confirmed attendance; Blue = SASG Member; *Dial In; **Joining 10-11am

Agenda
Time Item Lead Session type
Part I: Research portfolio overview & future plans
9.00-9.10Brief overview of recently published SASG studies
Richard MartinOpen
9.10-10.10Presentation and discussion of new study ideas
Proposing investigator
Part II: On-going study data review & manuscript discussions
10.10-10.25
On-going study data review• Metabolic effects of small vs large particle ICS
Gene Colice
Closed
10.25-11.00Current Manuscripts• Status review• Detailed discussions
Liz Hillyer
Meeting time: 9.00-11.00 amFormat: Part I: Open to All; Part II: Closed to Collaborators & Supporters
Part I: Recently accepted/published SASG studies• Increased Dose of Inhaled Corticosteroid
vs. Add-On Long-Acting Beta-Agonist for Step-Up Therapy in Asthma1
• Differential effects of inhaled corticosteroids in smokers/ex-smokers and non-smokers with asthma2
• Small-particle inhaled corticosteroid as first-line or step-up controller therapy in childhood asthma3
1Israel E, et al. Ann Am Thorac Soc 2015 Mar 10. [Epub ahead of print]2Roche N, et al. Am J Respir Crit Care Med 2015;191:960-9643Accepted at JACI: In Practice 23 Apr 2015 (van Aalderen WM, et al.)

Increased Dose of Inhaled Corticosteroid vs. Add-On Long-Acting Beta-Agonist for Step-Up
Therapy in Asthma• The odds of asthma control and rates of severe exacerbations
over 1 outcome year were comparable with increased inhaled corticosteroid dose vs. added LABAo Adjusted OR (95% CI) for achieving asthma control with
increased ICS dose vs ICS LABA were 0.99 (0.88, 1.12) for small-particle ICS and 0.85 (0.67, 1.07) for standard-particle ICS
o Adjusted RR (95% CI) for severe exacerbations were 1.04 (0.91, 1.20) for small-particle ICS and 1.18 (0.92, 1.54) for standard-particle ICS
• Increased doses of small- or standard-size particle inhaled corticosteroid is as effective as adding LABA
Israel E, et al. Ann Am Thorac Soc 2015 Mar 10. [Epub ahead of print]Small-particle ICS comparison: n=3036 in each cohort;
Standard-particle ICS comparison: n=809 in each cohort
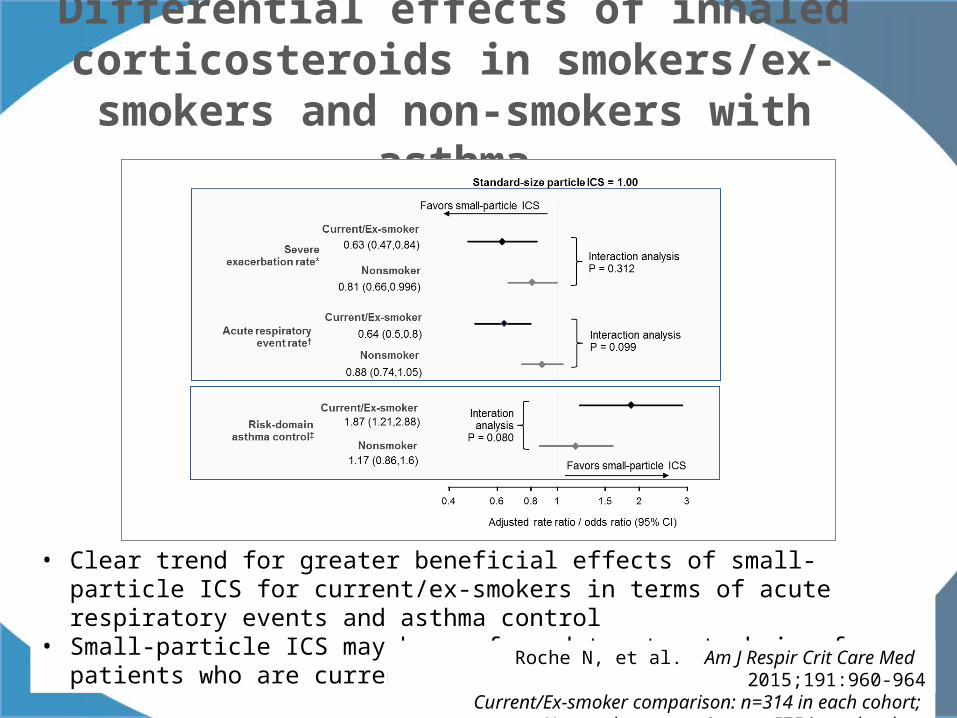
Differential effects of inhaled corticosteroids in smokers/ex-smokers and non-smokers with
asthma
• Clear trend for greater beneficial effects of small-particle ICS for current/ex-smokers in terms of acute respiratory events and asthma control
• Small-particle ICS may be preferred treatment choice for patients who are current or ex-smokers
Roche N, et al. Am J Respir Crit Care Med 2015;191:960-964Current/Ex-smoker comparison: n=314 in each cohort;
Nonsmoker comparison: n=575 in each cohort

Small-particle inhaled corticosteroid as first-line or step-up controller therapy in childhood
asthma• Children initiating or stepping-up with small-particle ICS vs.
standard-size particle ICS experienced:o Greater odds of asthma control
– Initiation population - adjusted OR (95% CI): 1.49 (1.10, 2.02)
– Step-up dose population - adjusted OR (95% CI): 2.22 (1.23, 4.03)
o Lower severe exacerbation rate – Initiation population - adjusted RR (95% CI): 0.56 (0.35,
0.88)– Step-up dose population - adjusted RR (95% CI): 0.49
(0.27, 0.89)• Outcomes were not significantly different for stepped-up small
particle ICS dose vs. ICS/LABA combination
Accepted at JACI: In Practice 23 Apr 2015 (van Aalderen WM, et al.)Initiation population: n=797 in each cohort;
Step-up dose population: n=206 in each cohort;Small particle ICS vs. ICS/LABA combination: n=185 in each cohort

Part I: New Study ProposalsTime Item Lead
Part I: Research portfolio overview & future plans
9.00-9.10Brief overview of recently published SASG studies
Richard Martin
9.10-10.10 Presentation and discussion of new study ideas
9.10-9.25Interaction of particle size and excess weight/obesity and GERD
Nicolas Roche
9.25-9.40Differential role of ICS particle size in ACOS management
Nicolas Roche
9.40-9.55Role of particle size in the management of pre-school asthma(& exploratory study 5-year outcome)
David Price & Gene Colice
10.55-10.05 COPD exacerbation management Richard Martin
10.05-10.10Systematic review of the role of ICS particle size on asthma treatment outcomes
Dirkje Postma

STUDY IDEA
Nicolas Roche
Interaction of particle size and excess weight/obesity and GERD

Background / Rationale
• Concept 1: BMI, GERD and asthmao Studies suggest that high BMI and gastro-esophageal reflux disease
(GERD) are related to poor control of asthma. These observations may be related to:
– BMI: inflammatory mechanisms or lung mechanics impairment
– GERD: pro-inflammatory and neurogenic effects. o Some of these features could (predominantly?) involve small
airways o In addition, there is a well known link between GERD and
overweight
• Concept 2: Distal airway inflammationo EF-particles fractions of inhaled therapies have the potential to
target the distal airwayso Small airways inflammation should be better targeted
by EF ICS than by non-EF ICS

Hypothesis & Aim
• Hypothesiso The mechanisms by which high BMI and GERD
impair asthma control could involve increased distal airway inflammation
o Differential effect of EF and standard-size ICS may help exploring this involvement of small airways.
• Objectives 1. Evaluate the comparative effectiveness of EF and
NEF ICS in asthma patients ± GERD ± overweight/obesity
2. Determine the relationship between overweight/obesity and GERD as determinants of poor asthma control
Study DesignSource database: CPRD +/- US database
Study Population:• Patients stepping up or initiating asthma maintenance treatment, as EF or
standard particle (SP) ICSo EF BDP vs SP BDPo EF BDP or ciclesonide vs all SP ICS
• Inclusions:o ≥1 year’s continuous data before and after date of step up (index date)o Physician diagnosed asthma + treatment (≥2 prescriptions in the last
year)
Outcomes• Differences (ORs, forest plots) between EF and SP ICS in terms of:
o Risk-domain asthma controlo Acute respiratory eventso Severe exacerbations
Analysis • Matched cohort analysis• Comparison of “EF/NEF ratio of effectiveness” (to be defined…) between
asthma patients categorized by presence/absence of high BMI and GERD.• Relations between BMI and GERD

STUDY IDEA
Nicolas Roche
Differential role of ICS particle size in ACOS management
Background / Rationale
• Concept 1: asthma, COPD and ACOSo Inflammation and remodeling are known to play key roles in
asthma and COPDo There are many differences in the pathophysiological
mechanisms present in asthma and COPDo These differences could involve small airways. o Asthma & COPD populations are comprised of several clinical
phenotypes. o Some phenotypes share features of asthma and COPD –
“ACOS”
• Concept 2: distal airway inflammationo EF-particles fractions of inhaled therapies have the potential to
target the distal airwayso Small airways inflammation should be better targeted
by EF ICS than by standard particle (SP) ICS
Hypothesis
• The involvement of steroid sensitive distal airway inflammation may differ between:o Asthmao COPDo ACOSo Sub-categories of ACOS (to be explored a posteriori)
• Differential effect of EF and SP ICS may help exploring the involvement of small airways in chronic inflammatory airways diseases and investigating differences between Asthma / COPD / ACOS phenotypes.
Study DesignSource database: CPRD +/- US database
Study Population:• Patients stepping up or initiating asthma, COPD or ACOS maintenance
treatment, as EF or standard particle (SP) ICSo EF BDP vs SP BDPo EF BDP or ciclesonide vs all SP ICS
• Inclusions:o ≥1 year’s continuous data before and after date of step up (index date)o Physician diagnosis (asthma alone, COPD alone, both) + treatment (≥2
prescriptions in the last year)
Outcomes• Differences (ORs, forest plots) between EF and SP ICS in terms of:
o Risk-domain disease controlo Acute respiratory eventso Severe exacerbations
Analysis • Matched cohort analysis• Comparison of “EF/NEF ratio of effectiveness” (to be defined…) between
asthma, COPD, ACOS (=asthma+COPD) patients

Retrospective observational cohort study comparing the effectiveness of common asthma management approaches in pre-school childrenDavid Price & Gene Colice
Comparative effectiveness of EF ICS vs. alternative Step 2 therapies in pre-school wheeze/asthma

Background / Rationale
• Voted REG 2014 Research Pinboard: #1 priority
• The particle size (and delivery characteristics of EF HFA BDP) of the aerosol may be particularly relevant for young children in whom a greater proportion of airways are classified as small (i.e. <2mm in diameter)1 and airways resistance is low.
• There are evidence to suggestion that EF HFA BDP is equivalent to CFC-FP in terms of efficacy and safety in adults and children (5–12 years) with mild-to-moderate asthma.2,3
• Evidence remains lacking as to the role that ICS particle size may play in the management of asthma/wheeze in younger, pre-school (<5 years) children.1. Leach CL, et al. Eur Respir J. 1998;12:1346–1353.
2. Aubier M, et al. Respir Med. 2001;95:212–220.3. Fairfax A, et al. Ann Allergy Asthma Immunol. 2001;86:575–582.

Aims & Objectives
• Aims to improve understanding of the prescribing of guideline recommended management approaches, and their comparative effectiveness, in the routine care of UK children with wheezing illness in their early (pre-school) years.
o Phase I: a descriptive analysis of treatment patterns in children aged ≤5 years with wheezing illness
o Part II: a comparative effectiveness analysis of guideline-recommended treatment options in pre-school children newly initiating Step 2 therapies:
– 3 x 2-way matched comparative effectiveness analysis: EF ICS, NEF ICS and LTRA vs SABA
– Relative benefit of EF ICS vs SABA over alternatives
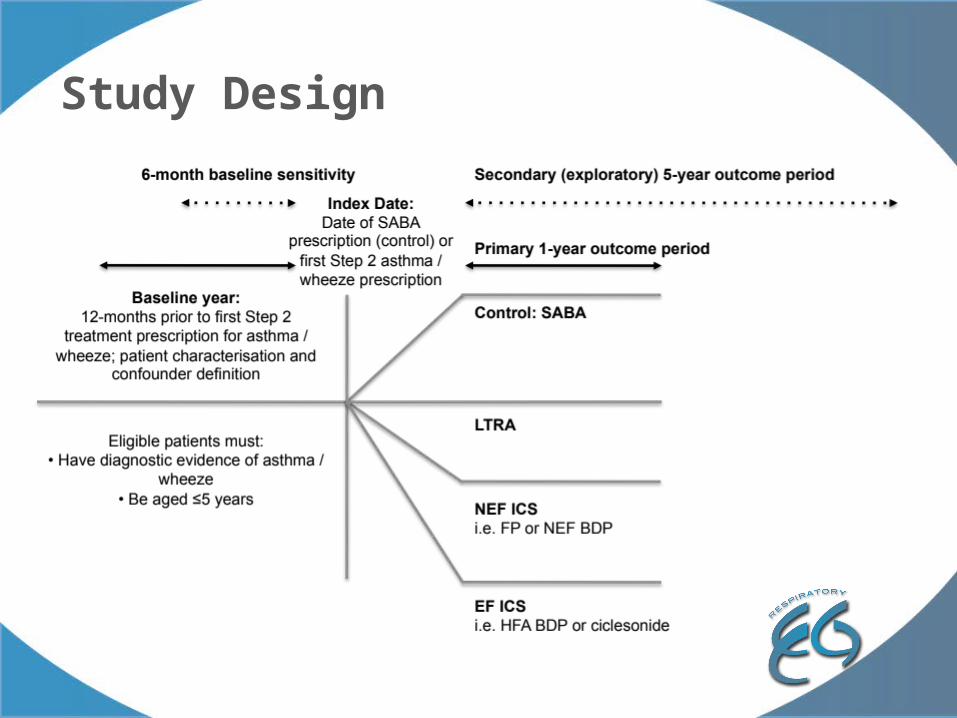
Study Design

21
Inclusion Criteria
Age: ≤5 years of age at the index date (i.e. date of first Step 2 asthma prescription)
Evidence of pre-school wheeze or asthma during the baseline year – defined as either: ≥2 wheezing episodes recorded within their primary care records in the baseline year, or≥2 prescriptions (at two different points in time) during the baseline year for any combination of oral steroids coded for a lower respiratory complaint ± salbutamol
Active treatment during outcome year:Active treatment arms (Step 2 therapy): ≥2 prescriptions (i.e. ≥1 in addition to that prescribed at index date) for any of the Step 2 treatment options (i.e. any ICS or LTRA) Control arm: ≥2 prescriptions for SABA
≥2 years continuous data (≥1 year of baseline plus ≥1 year of outcome data)
Exclusion Criteria
• Physician diagnosis for any chronic respiratory disease, except wheeze or asthma• Received a combination inhaler in addition to a separate ICS inhaler in baseline• Multiple step-up therapies on the same day.
Study Population

22
Primary Outcomes
Exacerbations (ATS/ERS definition) defined as occurrence of: 1. Asthma-related: Hospital admissions OR A&E attendance; OR2. An acute course of oral steroids (coded for asthma).Exacerbation (ATS/ERS definition sensitivity) defined as occurrence of:3. Asthma-related: Hospital admissions OR A&E attendance; OR4. An acute course of oral steroids with lower respiratory consultation
Secondary Outcomes
Acute respiratory event defined as occurrence of:1. Asthma-related: hospital admissions OR A&E attendance; OR2. An acute course of oral steroids (coded for asthma); OR 3. Antibiotics prescribed with lower respiratory consultation.Acute respiratory event (sensitivity) defined as occurrence of:4. Asthma-related: hospital admissions OR A&E attendance; OR5. An acute course of oral steroids with lower respiratory consultation; OR6. Antibiotics prescribed with lower respiratory consultation.
Risk Domain Asthma Control (RDAC): controlled = absence of the following:absence of the following:1. Asthma-related: Hospital admission AND A&E attendance, AND Out-patient department attendance; AND2. Acute use of oral steroids; AND3. Antibiotics prescribed with lower respiratory consultation.Uncontrolled: all others.Risk Domain Asthma Control (RDAC sensitivity): controlled = absence of the following:4. Asthma-related: Hospital admission AND A&E attendance, AND Out-patient department attendance; AND5. Acute use of oral steroids with lower respiratory consultation; AND6. Antibiotics prescribed with lower respiratory consultation.Uncontrolled: all others.
Outcomes (I)
23
Secondary Outcomes
Overall Asthma Control (OAC) – Risk and Impairment defined as: o Achieved Risk Domain Asthma Control (as defined on previous slide) ANDo Average daily dose of: o UK: ≤200mcg salbutamol / ≤500mcg terbutaline
Treatment Failure defined as RDAC plus no additional or change in therapy
Reliever Usage defined as:
o Average daily SABA dosage during outcome year: Average number of puffs per day/365 x strength (mcg) and categorised as appropriate to data
o Controller-to-Reliever Ratio: Number of controller units/Number of controller units + number of reliever units
• Controllers: ICS and LTRA. For ICS a unit is taken to be one inhaler; for LTRA a unit is one prescription
• Relievers: SABA, with a unit taken to be one inhaler
Outcomes (II)
Potential subgroup & sensitivity analyses
Subgroups: stratification by• Atopy: evidence of personal atopy; No evidence of
personal atopy, but evidence of maternal atopy; No evidence of personal or maternal atopy
• Sex• Age: 1–3 years (at index date); 4–5 years (at index date)• Disease severity: <3 vs ≥3 baseline wheeze episodes
Sensitivity analyses:• 6-month baseline period
Exploratory analyses:• 5-year outcome period…?
Exploratory outcome period: 5-year outcomes
Concept:• Better control of inflammation in the large and small airways with fine
particle ICS compared to standard particle ICS might have long-term consequences in terms of the natural history of the disease.
• Current studies are usually limited to outcomes measured over 1 year or less. Access to large administrative databases allows assessment of asthma outcomes over longer time periods.
Hypothesis: • Treatment with fine particle ICS will result in better long-term outcomes
than treatment with standard particle ICS in young children with asthma Proposed aims/outcomes:• Primary: To demonstrate that EF ICS treatment of small children with
asthma will result in fewer exacerbations over 5 years than treatment with non-EF ICS
• Secondary: To demonstrate that EF ICS treatment of small children with asthma will result in a lower rate of progression of asthma therapy (i.e. either an increase in dose of ICS or addition of other controllers such as montelukast, LABA, omalizumab) over 5 years than treatment with non-EF ICS.
• To explore whether there might be differences in lung function as well.
Additional study arm…?
• Literature suggests that treatment with antibiotics in first year of children’s lives may induce asthma, rhinoconjunctivitis and eczema
• Question – is it feasible to:
o Investigate whether children who receive antibiotics in their first year of life (an additional study arm) have a higher prevalence of asthma at age 5 (compared to the SABA control arm?)
Foliaki S, et al. J Allergy Clin Immunol 2009; 124;982-9

STUDY IDEA raised in prior SASG meetings
Richard Martin
Oral corticosteroid and antibiotic prescription for exacerbations
Concept & Research Questions
• COPD exacerbations are typically managed by either via oral corticosteroids and/or antibiotics
• To guide optimum management of COPD exacerbations, it would be interesting to explore potential drivers and associated outcomes with these real-life prescribing decisions.
Research Questions:• What do these three populations look like:
• Antibiotic treated?• Oral steroid treated?• Antibiotic + oral steroid treated?
• How do they differ in their characteristics?• Do these two populations have the same outcomes?

SYSTEMATIC REVIEW
Dirkje Postma
The role of ICS particle size on asthma treatment outcomes

Concept / Background:• Systematic review and meta-analysis of the effect of
ICS particle size on asthma efficacy and safety presented the 2014 Winter BTS concluded:1
o There are no overall differences in efficacy and no appreciable differences in safety between FP-containing medications and small particle size ICS medications for the treatment of asthma.
o ICS-containing medications with a small particle size do not confer additional clinical benefits over those with a standard particle size.
• These conclusions conflict with (some of) the published literature, including the SASG’s real-life studies
1. Suarez E, et al. Effect of inhaled corticosteroid (ICS) particle size on asthma efficacy and safety outcomes: A systematic literature review. Presented at the British Thoracic Society (BTS) Winter Meeting, London, England, 3–5 December 2014

Effect‘efficacy’ Safety
High ‘internal’ validity feasible in clear-cut trial populations
APPROVAL
Real ‘external’ validity &generalisability by mirroring
real populations and healthcare practices
Medicines won’t work if peoplecan’t or don’t take them
Needs of Regulators
Effectiveness/Outcomes
Device‘to train, or not to train’?
Adherence
CAN IT WORK IN AN IDEAL POPULATION OPTIMALLY MANAGED?
DOES IT WORK IN REAL PATIENTS MANAGED IN ROUTINE CARE
SETTINGS?
Needs of Patients, Physicians, Payers
Efficacy vs Effectiveness

• Studies have shown that efficacy RCTs exclude about 95% of asthma and 90% of COPD routine care populations due to strict inclusion criteria.1
1. Herland K, et al. Respir Med 2005;99:11–19.
Limitations: RCTs inclusions/exclusions
0
100
200
300
400
500
600
700
800
900
1000 Patient RCT eligibility drop-off with sequential application of standard inclusion criteria
Series1N
um
be
r o
f su
bje
cts
100.0%
38.4%
14.3%5.7% 3.7% 2.1% 1.7% 1.3%
COPD
0
200
400
600
800
1000All pat
All pat VAS >7.5 No Co-morbidity FEV1 30-70 S or XS Packy > 15 No Hayfever
Nu
mb
er
of s
ub
ject
s
100.0%
42.1%
15.2%10.1% 9.2% 8.2% 7.2%
Asthma
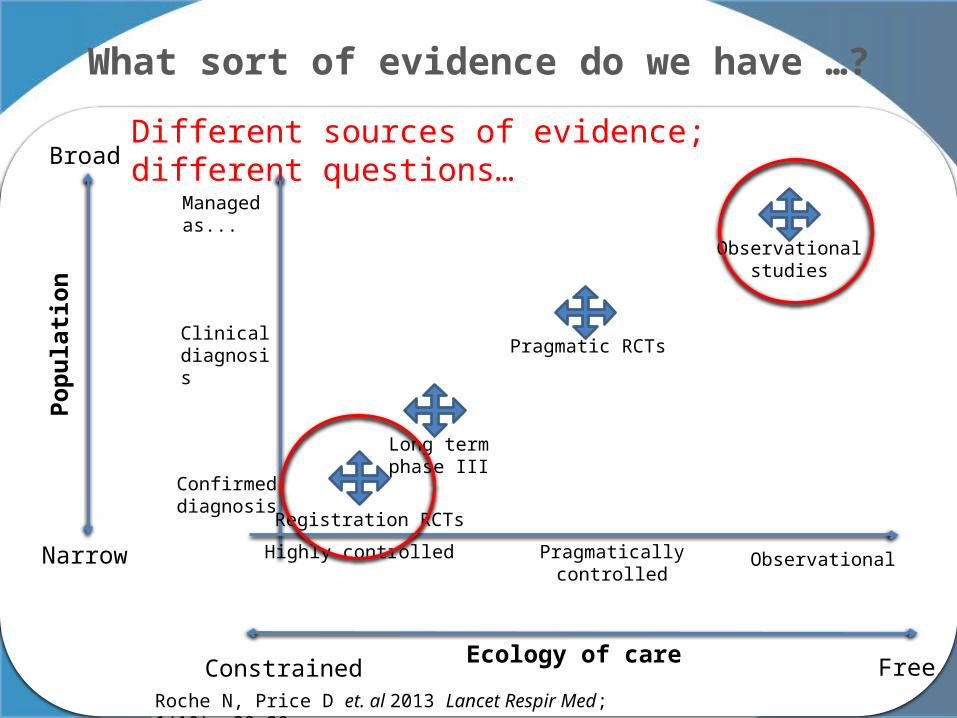
What sort of evidence do we have …?P
op
ula
tio
n
Broad
Narrow
Ecology of care FreeConstrained
Highly controlled Pragmatically controlled
Observational
Managed as...
Clinical diagnosis
Confirmed diagnosis
Registration RCTs
Long term phase III
Pragmatic RCTs
Observational studies
Roche N, Price D et. al 2013 Lancet Respir Med; 1(10):e29-30
Different sources of evidence; different questions…
Improving guidelines: evidence appraisal• Sir Michael Rawlins, the former chairman of the
UK’s National Institute for Health and Care Excellence:1
o Hierarchies of evidence are over-simplistic and offer a pseudoquantitative assessment of the available evidence.
o All forms of evidence should be considered, while taking into account the limitations and strengths of their respective designs
o Differently designed studies should be considered as complementary and should be used in combination by guideline developers to help inform their judgments and recommendations.
1. Rawlins M. De testimonio: on the evidence for decisions about the use of therapeutic interventions. Lancet 2008;372:2152–2161.
Different research questions need different research
approaches to answer them

Systematic review: Aims & Objectives
• Aim, to:
o Summarise the comparative effectiveness of ICS medications of different particle sizes as assessed in real-life studies
o Compare real-life effectiveness and safety outcomes to the RCT systematic review of the efficacy and safety outcomes.
o Identify key similarities / differences between the real-life and RCT evidence
o Consider apparent conflicts in the context of the original research question asked

Systematic review: design / approach
• Literature review – CER literature from the last sixteen years (1 January 1998 to 13 February 2014)* focussing on:o Fluticasone propionate vs EF particle ICS and fine
particle ICS (HFA BDP or ciclesonide) o FP/SAL vs. ICS small particle size combination
comparators (HFA BDP or BDP/FOR HFA)
• Meta-analysis endpoints – consider:o Efficacy & safety points used in the RCT review
(if/where available)o Effectiveness measures: exacerbations; MPR, OCS
prescriptions, asthma consults, LRTI abx*As per RCT review/meta-analysis & extended ~current date

Agenda – Part II – CLOSED
Time Item Lead Session type
Part I: Research portfolio overview & future plans
9.00-9.10Brief overview of recently published SASG studies
Richard MartinOpen
9.10-10.05Presentation and discussion of new study ideas
Proposing investigator
Part II: On-going study data review & manuscript discussions
10.05-10.25
On-going study data review• Metabolic effects of small vs large particle ICS
Gene Colice Closed
10.25-11.00Current Manuscripts• Status review• Detailed discussions
Liz Hillyer Closed

On-going study – Data review
Gene Colice
Metabolic effects of small particle ICS
PART II

Research in Real-Life
Assessing metabolic and other adverse effects of inhaled corticosteroids in relation to their clinical benefit in obstructive lung disease
Study Update, May 2015

• To assess metabolic and other adverse consequences of small particle ICS and large particle ICS* in relation to their clinical benefits in patients with obstructive lung disease
• Specifically to examine:− Incidence of pneumonia− Risk of developing new-onset diabetes − Worsening control of pre-existing diabetes − Change in BMI
• To further explore dose-response relationships
Study Aims
*Note: terminology has recently been updated to use “extrafine” and “fine” in place of small and large particle
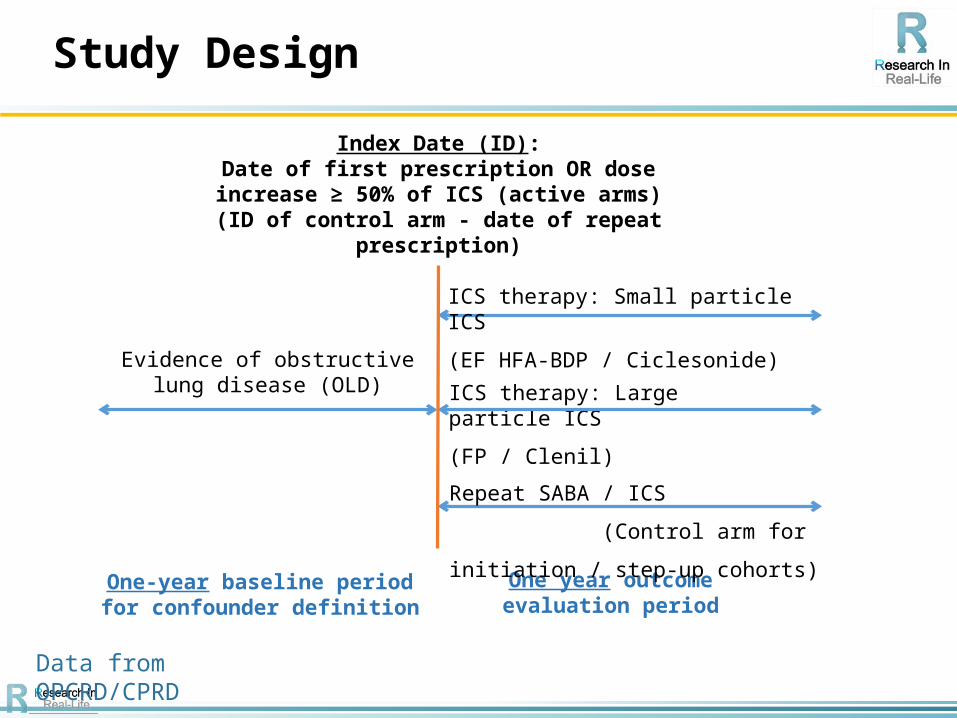
Study Design
Data from OPCRD/CPRD
One-year baseline period for confounder definition
One year outcome evaluation period
Evidence of obstructive lung disease (OLD)
ICS therapy: Small particle ICS
(EF HFA-BDP / Ciclesonide)
ICS therapy: Large particle ICS
(FP / Clenil)
Index Date (ID):Date of first prescription OR dose increase ≥ 50%
of ICS (active arms)(ID of control arm - date of repeat prescription)
Repeat SABA / ICS (Control
arm for initiation / step-up cohorts)

Full adult population
− Inclusion criteria
• Aged 12-80 years at the Index Date
• Evidence of obstructive lung disease (OLD) treatment:− ≥2 prescriptions for respiratory therapy at baseline (for patients in the
ICS step-up cohort, including ≥1 prescription for ICS)
• Continuation of OLD therapy:− ≥2 respiratory prescriptions during the outcome year (i.e. ≥1 in addition to
that prescribed at the Index Date)
• Two years of continuous practice data comprising 1 year baseline data and 1 year of outcome data (up-to-standard data for CPRD patients)
• ICS via a pMDI / BAI at Index Date
− Exclusion criterion
• Any other chronic respiratory disease, at any time
Inclusion / Exclusion Criteria
• Unconfirmed pneumonia
• Confirmed pneumonia
• Severe Asthma Exacerbation (ATS/ERS definition)
• Acute Respiratory Event
• First onset of type 2 diabetes
• Progression of on-going type 2 diabetes to insulin
• Change in HbA1c reading
• Change in antidiabetic medication
• Change in BMI
Study Endpoints

• SASG October 2013:− Presented results for QVAR vs. FP− Recommendations included:
− Increase dataset to compare “large particle” (FP/Clenil) vs “small particle” (QVAR/Ciclesonide);
− Introduce control populations (repeat prescriptions).
• SASG June 2014:− Presented unmatched results for large vs. small particle− Presented matched results for large / small particle ICS step-up vs. control
groups (repeat ICS prescription)− Recommendations included:
− “Per protocol” (no change in drug) “ever after” analysis for progression to insulin & change in HbA1c;
− Look at change in antidiabetic medication;− Look at effect of drug substance & consumed dose on pneumonia results.
• SASG January 2015:− Presented unmatched results for large vs. small particle excluding DPI
patients (including additional analyses above)− Recommended to complete matched analyses (ICS step-up only)
Study history

• ICS Step-up Cohort, pneumonia endpoint−Unmatched analyses−Matched analyses−Publication of results?
• ICS Step-up Cohort, diabetes endpoints−Matched analyses −Unmatched analysis for progression to insulin
Today’s Presentation

ICS STEP-UP COHORT
PNEUMONIA ENDPOINTUnmatched analyses

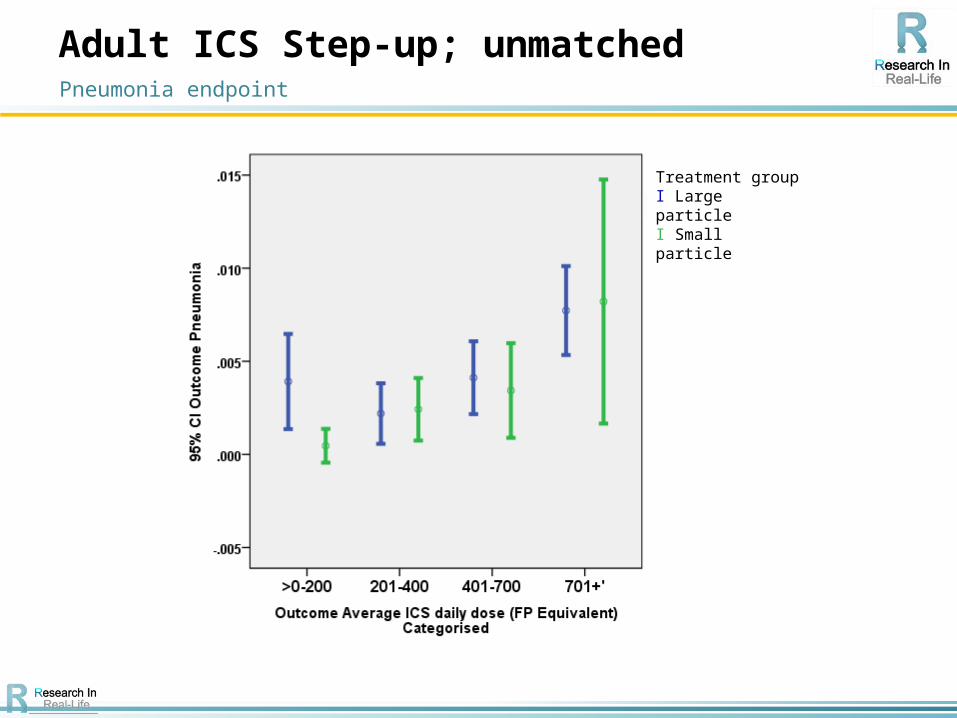
Adult ICS Step-up; unmatched
*Mann Whitney ^ Chi Square Ω FP Equivalent
Pneumonia endpoint
Baseline Characteristics
Particle SizeTotal
(n=23013)P valueLarge
(n=14788)Small
(n=8225)
Age (in years) Median (IQR) 46 (33, 57) 45 (31, 57) 46 (32, 57) 0.018*
Gender, n (%) female 9046 (61.2) 4871 (59.2) 13917 (60.5) 0.004^
Year of IPD Median (IQR)2002
(1998, 2006.5)2006
(2003, 2008)2003
(2000, 2007)<0.001*
Acute Oral steroids, n (%)
0 10335 (69.9) 6560 (79.8) 16895 (73.4)
<0.001^1 2608 (17.6) 1167 (14.2) 3775 (16.4)
2+ 1845 (12.5) 498 (6.1) 2343 (10.2)
Pneumonia, n (%) Yes 82 (0.6) 33 (0.4) 115 (0.5) 0.044^
Diabetes &/or therapy, n (%) Yes 872 (5.9) 592 (7.2) 1464 (6.4) <0.001*
COPD Diagnosis (ever), n (%) Yes 3098 (20.9) 940 (11.4) 4038 (17.5) <0.001*
ICS Dose at IPD Median (IQR)Ω 1000 (500, 1000) 400 (200, 400) 500 (400, 1000) <0.001*
Average ICS daily dose Median (IQR) Ω
213.7 (82.2, 438.4)
109.6 (54.8, 219.2)
164.4 (82.2, 356.2)
<0.001*

Adult ICS Step-up; unmatched
^ Adjusted for: Baseline coding for pneumonia (Y/N), diabetes dx &/or therapy at baseline (Y/N) & COPD dx (ever) (Y/N).*Fisher’s Exact 2-sided test
Pneumonia endpoint
Patients stepping up their ICS therapy as small particle ICS are significantly less likely to be coded for pneumonia compared with patients stepping up as large particle ICS
Pneumonia Diagnosis in outcome
Particle SizeTotal
(n=23013)P value*Large
(n=14788)Small
(n=8225)
Yes, n (%) 73 (0.5) 22 (0.3) 95 (0.4)0.011
No, n (%) 14715 (99.5) 8203 (99.7) 22918 (99.6)
Odds Ratio (95% CI) adjusted for baseline confounders^
1.000.60
(0.37, 0.97)
Adult ICS Step-up; unmatchedPneumonia endpoint
Treatment group I Large particleI Small particle
Adult ICS Step-up; unmatched
* Adjusted for: Baseline coding for pneumonia (Y/N), diabetes dx &/or therapy at baseline (Y/N) and COPD dx (ever) (Y/N).^ Chi Square test
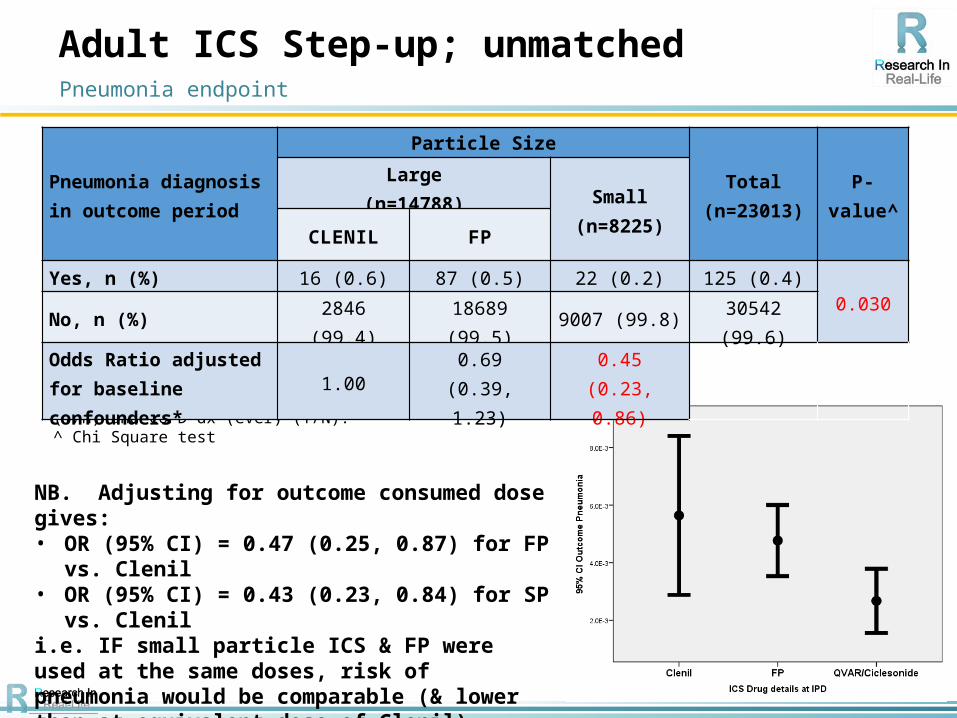
NB. Adjusting for outcome consumed dose gives: • OR (95% CI) = 0.47 (0.25, 0.87) for FP vs. Clenil• OR (95% CI) = 0.43 (0.23, 0.84) for SP vs. Clenili.e. IF small particle ICS & FP were used at the same doses, risk of pneumonia would be comparable (& lower than at equivalent dose of Clenil)
Pneumonia endpoint
Pneumonia diagnosis in outcome period
Particle Size
Total(n=23013)
P-value^
Large(n=14788) Small
(n=8225)CLENIL FP
Yes, n (%) 16 (0.6) 87 (0.5) 22 (0.2) 125 (0.4)0.030
No, n (%) 2846 (99.4) 18689 (99.5) 9007 (99.8) 30542 (99.6)
Odds Ratio adjusted for baseline confounders*
1.000.69
(0.39, 1.23)0.45
(0.23, 0.86)
Adult ICS Step-up; by consumed dose
* Adjusted for: Baseline diagnosis for pneumonia (Y/N), diabetes diagnosis or therapy at baseline (Y/N) and COPD diagnosis (ever) (Y/N).^ Chi Square test
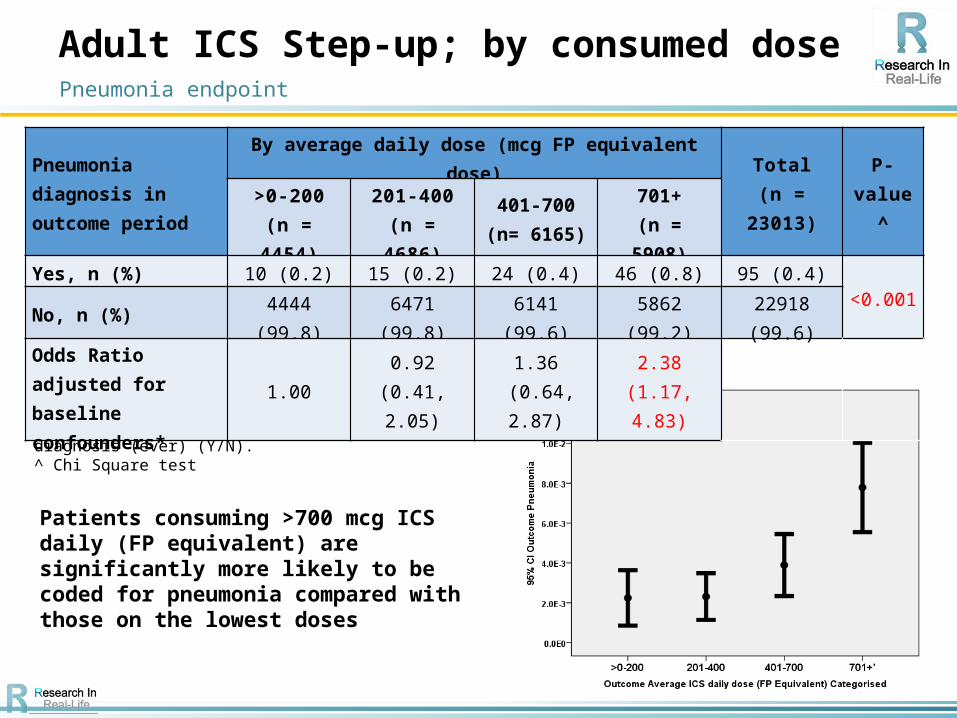
Pneumonia endpoint
Patients consuming >700 mcg ICS daily (FP equivalent) are significantly more likely to be coded for pneumonia compared with those on the lowest doses
Pneumonia diagnosis in outcome period
By average daily dose (mcg FP equivalent dose)
Total(n = 23013)
P-value^>0-200
(n = 4454)201-400
(n = 4686)401-700
(n= 6165)701+
(n = 5908)
Yes, n (%) 10 (0.2) 15 (0.2) 24 (0.4) 46 (0.8) 95 (0.4)<0.001
No, n (%) 4444 (99.8) 6471 (99.8) 6141 (99.6) 5862 (99.2) 22918 (99.6)
Odds Ratio adjusted for baseline confounders*
1.000.92
(0.41, 2.05)1.36
(0.64, 2.87)2.38
(1.17, 4.83)

Adult ICS Step-up; by consumed dose
The interaction between consumed dose and particle size is not significant (at the 5% level: p =0.257)
Pneumonia endpoint
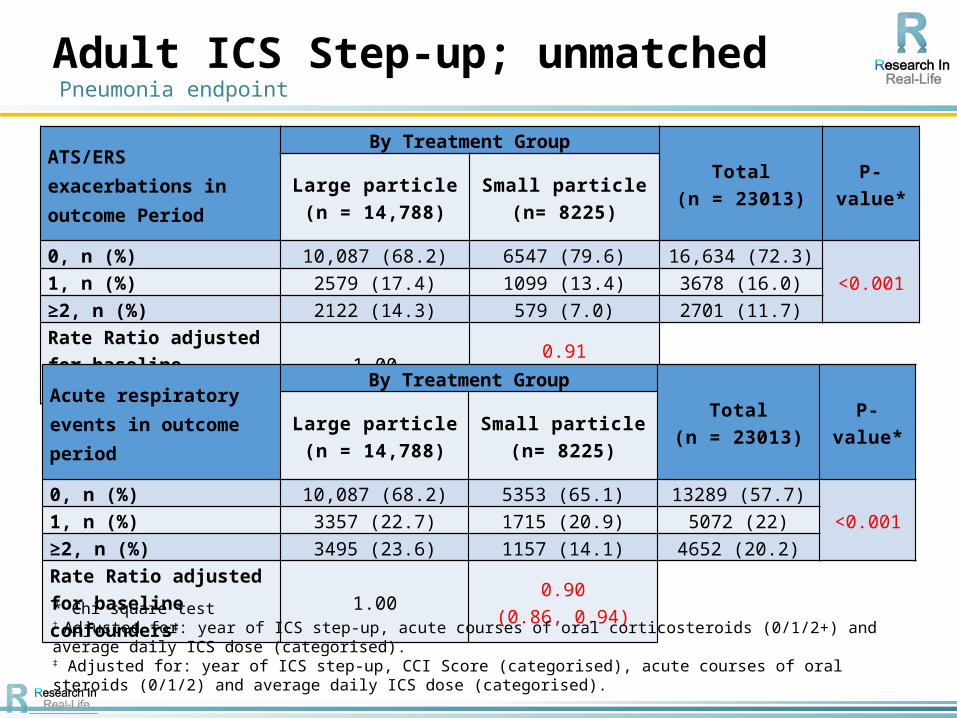
Adult ICS Step-up; unmatched
ATS/ERS exacerbations in outcome Period
By Treatment GroupTotal
(n = 23013) P-value*Large particle(n = 14,788)
Small particle(n= 8225)
0, n (%) 10,087 (68.2) 6547 (79.6) 16,634 (72.3)<0.0011, n (%) 2579 (17.4) 1099 (13.4) 3678 (16.0)
≥2, n (%) 2122 (14.3) 579 (7.0) 2701 (11.7)
Rate Ratio adjusted for baseline confounders† 1.00
0.91(0.85, 0.97)
Acute respiratory events in outcome period
By Treatment GroupTotal
(n = 23013) P-value*Large particle(n = 14,788)
Small particle(n= 8225)
0, n (%) 10,087 (68.2) 5353 (65.1) 13289 (57.7)<0.0011, n (%) 3357 (22.7) 1715 (20.9) 5072 (22)
≥2, n (%) 3495 (23.6) 1157 (14.1) 4652 (20.2)
Rate Ratio adjusted for baseline confounders‡
1.000.90
(0.86, 0.94)
* Chi square test† Adjusted for: year of ICS step-up, acute courses of oral corticosteroids (0/1/2+) and average daily ICS dose (categorised).‡ Adjusted for: year of ICS step-up, CCI Score (categorised), acute courses of oral steroids (0/1/2) and average daily ICS dose (categorised).
Pneumonia endpoint
PNEUMONIA ENDPOINTMatched analyses

Patients were matched on:− Sex (M/F)− Age (± 5 years)− Baseline coding for pneumonia (Y/N)− Smoking status (non-smoker / current smoker / ex-smoker)− Number of acute courses of oral corticosteroids (0/1/2+)− Number of prescriptions for antibiotics (0/1/2+)− Average daily ICS dose at baseline (1-200/201-400/401-
800/801+mcg; FP equivalent dose)− Year of ICS step-up (± 3 years)
Adult ICS Step-up; matchedPneumonia endpoint

Adult ICS Step-up; matched
Baseline Characteristics
Particle SizeTotal
(n=13272)P value*Large
(n=6636)Small
(n=6636)
Age (in years) Median (IQR) 44 (30, 57) 44 (30, 57) 44 (30, 57) 0.060
Gender, n (%) female 3936 (59.3) 3936 (59.3) 7872 (59.3) N/A
Year of IPD Median (IQR)2006
(2002, 2008)2006
(2003, 2008)2006
(2002, 2008)<0.001
Acute Oral steroids n (%)
0 4899 (73.8) 4899 (73.8) 9798 (73.8)
N/A1 1099 (16.6) 1099 (16.6) 2198 (16.6)
2+ 638 (9.6) 638 (9.6) 1276 (9.6)
Pneumonia, n (%) Yes 3 (0) 3 (0) 6 (0) N/A
Diabetes &/or therapy, n (%) Yes 444 (6.7) 453 (6.8) 897 (6.8) 0.751
COPD Diagnosis (ever), n (%) Yes 834 (12.6) 746 (11.2) 1580 (11.9) 0.007
ICS Dose at IPD Median (IQR)Ω 500 (250, 1000) 400 (200, 400) 400 (200, 500) <0.001
Average ICS daily dose Median (IQR) Ω
115.1(54.8, 219.2)
109.6 (54.8, 219.2)
109.6 (54.8, 219.2)
0.007
*Conditional Logistic Regression Ω FP Equivalent
Pneumonia endpoint
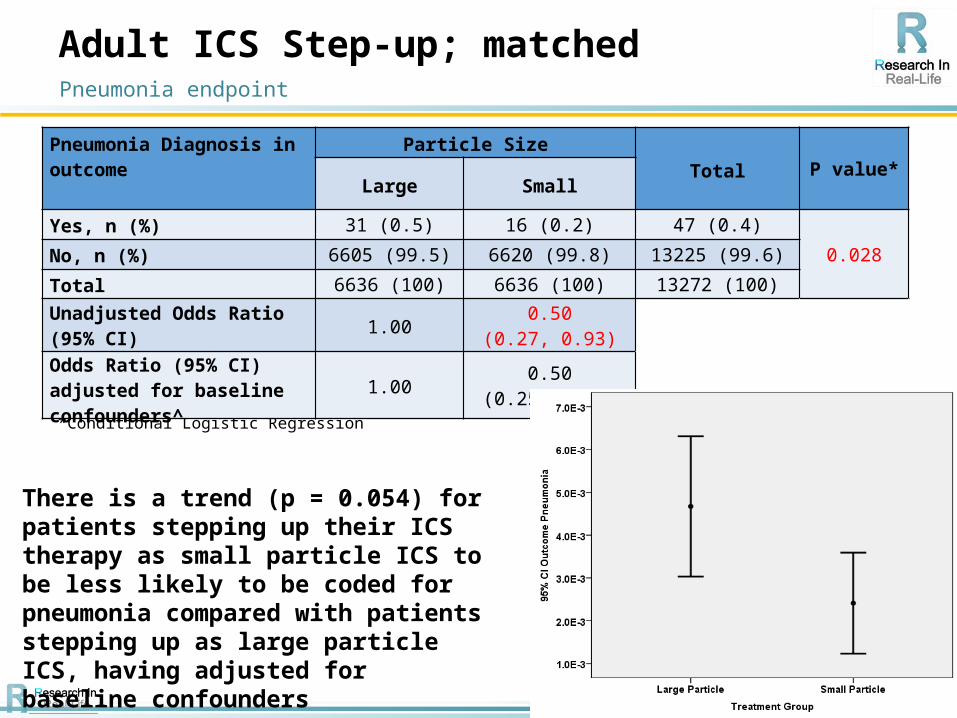
Adult ICS Step-up; matched
^Adjusted for: COPD diagnosis (ever) (Y/N)*Conditional Logistic Regression
Pneumonia Diagnosis in outcome
Particle Size
Total P value*Large Small
Yes, n (%) 31 (0.5) 16 (0.2) 47 (0.4)
0.028No, n (%) 6605 (99.5) 6620 (99.8) 13225 (99.6)
Total 6636 (100) 6636 (100) 13272 (100)
Unadjusted Odds Ratio (95% CI) 1.00
0.50(0.27, 0.93)
Odds Ratio (95% CI) adjusted for baseline confounders^
1.000.50
(0.25, 1.01)
Pneumonia endpoint
There is a trend (p = 0.054) for patients stepping up their ICS therapy as small particle ICS to be less likely to be coded for pneumonia compared with patients stepping up as large particle ICS, having adjusted for baseline confounders

Adult ICS Step-up; matched
ATS/ERS Exacerbations in Outcome Period
By Treatment GroupTotal P-value^
Large Particle Small Particle
0, n (%) 5112 (77.0) 5319 (80.2) 10431 (78.6)
<0.0011, n (%) 966 (14.6) 861 (13.0) 1827 (13.8)
2+, n (%) 558 (8.4) 456 (6.9) 1014 (7.6)
Total, n (%) 6636 (100) 6636 (100) 13272 (100)
Rate Ratio adjusted for baseline confounders*
1.000.90
(0.84, 0.97)
Acute Respiratory Events in Outcome
By Treatment GroupTotal P-value^
Large Particle Small Particle
0, n (%) 4094 (61.7) 4366 (65.8) 8460 (63.7)
<0.0011, n (%) 1475 (22.2) 1360 (20.5) 2835 (21.4)2+, n (%) 1067 (16.1) 910 (13.7) 1977 (14.9)Total, n (%) 6636 (100) 6636 (100) 13272 (100)
Rate Ratio adjusted for baseline confounders*
1.000.90
(0.86, 0.95)
^Conditional logistic regression*Adjusted for: rhinitis diagnosis &/or therapy (Y/N), COPD diagnosis (ever) (Y/N) and number of prescriptions for SABA (categorised)
Pneumonia endpoint
Conclusions
• At the ICS doses consumed in real life, patients prescribed small particle ICS:
− Are less likely to be coded for pneumonia; and− Record significantly lower relative rates of Exacerbations /
Acute Respiratory Events compared with patients prescribed large particle ICS
• This may be due to the lower doses consumed as small particle ICS compared with large particle ICS but
• Lower exacerbation risk AND lower pneumonia risk are achieved at these lower doses
• Matched analyses confirm these results
Pneumonia endpoint
FIRST ONSET OF TYPE 2 DIABETES
Matched analyses

Patients were matched on:− Sex (M/F)− Age (± 5 years)− Smoking status (non-smoker / current smoker / ex-smoker)− Number of acute courses of oral corticosteroids (0/1/2+)− Last ICS dose prior to step-up (1-100 / 101-200 /
201+mcg; FP equivalent dose)− Year of ICS step-up (± 3 years)
Adult ICS Step-up; matched1st onset of type 2 diabetes

Adult ICS step-up; matched
Diabetes diagnosis &/or therapy in outcomeParticle Size
Total P value*Large Small
Yes, n (%) 85 (1.6) 109 (2.0) 194 (1.8)
0.005No, n (%) 5318 (98.4) 5294 (98.0) 10612 (98.2)
Total 5403 (100) 5403 (100) 10806 (100)
Odds Ratio (95% CI) adjusted for baseline confounders^
1.001.34
(0.99, 1.82)
*Chi-square test ** Mann Whitney U test
^ Adjusted for: Beta blockers (Y/N) and number of primary care consultations (categorised).
There is a trend (p = 0.059) for patients prescribed small particle ICS to be more likely to develop type 2 diabetes compared with patients prescribed large particle ICS, having adjusted for baseline confounders
Average Daily ICS Dose in Outcome: Median (IQR) (mcg)
328.8 (164.4, 657.5)
301.4(164.4, 438.4)
328.8 (164.4, 493.2) <0.001**
1st onset of type 2 diabetes
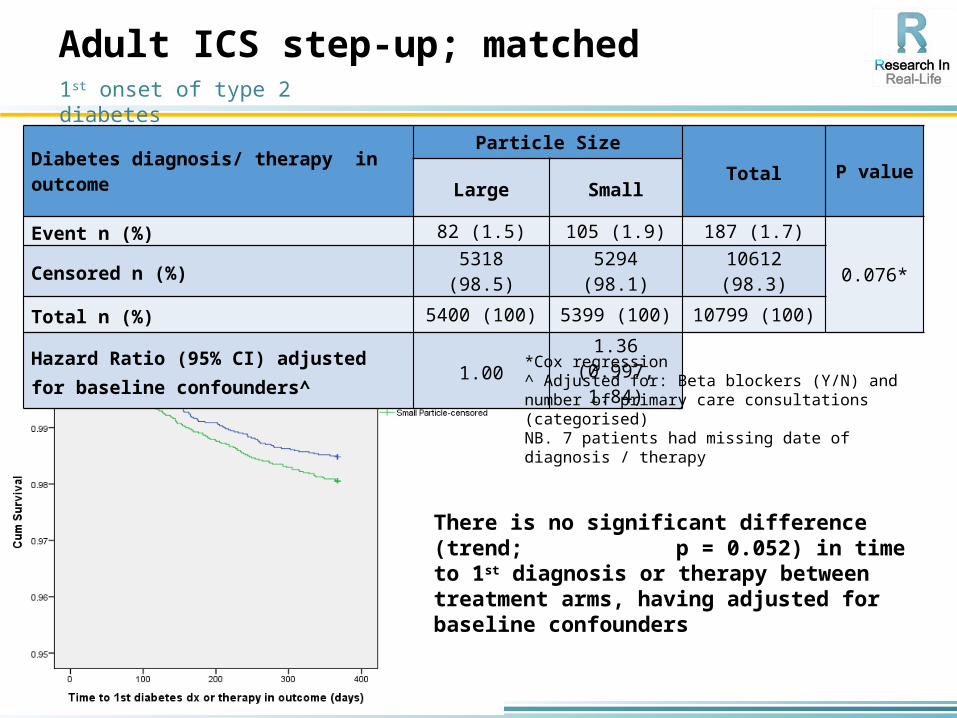
Adult ICS step-up; matched
Diabetes diagnosis/ therapy in outcomeParticle Size
Total P valueLarge Small
Event n (%) 82 (1.5) 105 (1.9) 187 (1.7)
0.076*Censored n (%) 5318 (98.5) 5294 (98.1) 10612 (98.3)
Total n (%) 5400 (100) 5399 (100) 10799 (100)
Hazard Ratio (95% CI) adjusted for baseline confounders^
1.001.36
(0.997, 1.84)
*Cox regression^ Adjusted for: Beta blockers (Y/N) and number of primary care consultations (categorised)NB. 7 patients had missing date of diagnosis / therapy
There is no significant difference (trend; p = 0.052) in time to 1st diagnosis or therapy between treatment arms, having adjusted for baseline confounders
1st onset of type 2 diabetes

Adult ICS step-up; matched
Diabetes diagnosis/ therapy ever after$Particle Size
Total P valueLarge Small
Event, n (%) 497 (9.2) 513 (9.5) 1010 (9.3)
0.031*Censored, n (%) 4906 (90.8) 4890 (90.5) 9796 (90.7)
Total, n (%) 5403 (100) 5403 (100) 10806 (100)
Hazard Ratio (95% CI) adjusted for baseline confounders^
1.001.19
(1.00, 1.41)
*Cox regression^Adjusted for: Year of ICS step-up, Respiratory diagnosis (None / Asthma only / COPD only / ACOS), CCI Score (categorised) and number of primary care consultations (categorised).$ Censored at end of records or any change in ICS drugNB Unadjusted HR (95% CI) = 1.19 (1.02, 1.41)
There is no significant difference (trend; p = 0.085) in time to 1st diagnosis or therapy between treatment arms, having adjusted for baseline confounders
1st onset of type 2 diabetes
PROGRESSION OF ONGOING TYPE 2 DIABETES TO INSULIN
Unmatched analyses

Insulin Prescription ever after$Particle Size
Total P value*Large Small
Event, n (%) 68 (4.5) 19 (3.8) 87 (7.1)0.030Censored, n (%) 651 (90.5) 481 (96.2) 1132 (92.9)
Total, n (%) 719 (100) 500 (100) 1219 (100)
Unadjusted Hazard Ratio (95% CI) 1.000.50
(0.30, 0.86)
Adjusted Hazard Ratio^ (95% CI) 1.000.57
(0.34, 0.95)
Adult ICS step-up; unmatched
*Log rank test^Adjusted for: Rhinitis diagnosis (Y/N), Statins scripts (Y/N), CCI Score (categorised) & number of acute courses of oral steroids (0/1/2+)$Censored at end of records or any change in ICS drug
Progression to Insulin
In the unmatched cohort, diabetic patients stepping up their ICS therapy as large particle ICS progress to insulin significantly more quickly compared with patients stepping up as small particle ICS
An analysis by consumed dose does not suggest this result is dose-related
PROGRESSION OF ONGOING TYPE 2 DIABETES TO INSULIN
Matched analyses
• Patients were matched on:− Sex (M/F)− Age (± 5 years)− Number of acute courses of oral corticosteroids (0/1/2+)− Last ICS dose prior to step-up (1-100 / 101-200 /
201+mcg; FP equivalent dose)− Year of ICS step-up (± 3 years)
Adult ICS Step-up; matchedProgression to Insulin

*Conditional Logistic Regression
There is no significant difference between treatment groups in the odds of progressing to insulin
Insulin scripts in outcomeParticle Size
Total P valueLarge Small
Yes, n (%) 7 (2.2) 9 (2.8) 16 (2.5)
0.618*No, n (%) 309 (97.8) 307 (97.2) 616 (97.5)
Total 316 (100) 316 (100) 632 (100)
Unadjusted Odds Ratio (95% CI)
1.001.29
(0.48, 3.45)
Adult ICS step-up; matchedProgression to Insulin

Insulin Prescription ever after$Particle Size
Total P value*Large Small
Event, n (%) 23 (7.3) 14 (4.4) 37 (5.9)
0.113Censored, n (%) 293 (92.7) 302 (95.6) 595 (94.1)
Total, n (%) 316 (100) 316 (100) 632 (100)
Unadjusted Hazard Ratio (95% CI) 1.000.69
(0.32, 1.48)
Adjusted Hazard Ratio^ (95% CI) 1.000.61
(0.27, 1.39)
Adult ICS step-up; matched
*Conditional Logistic Regression^Adjusted for paracetamol prescriptions (Y/N)$Censored at end of records or any change in ICS drug
There is no significant difference between treatment groups in the time to progression to insulin
Progression to Insulin

CHANGE IN HBA1C READINGSMatched analyses

• Patients were matched on:− Sex (M/F)− Age (± 5 years)− Number of acute courses of oral corticosteroids (0/1/2+)− Average daily ICS dose (1-200 / 201+mcg; FP
equivalent dose)− Insulin use at baseline (Y/N)− HbA1c reading at baseline (±1%)
Adult ICS Step-up; matchedChange in HbA1c

Adult ICS step-up; matched
Change in HbA1c from baseline to 1st reading ever after index date
Particle Size
Total P valueLarge Small
N (% non-missing) 210 (100) 210 (100) 420 (100)
0.094*Mean (SD) 2.96 (13.04) 0.98 (13.5) 1.97 (13.29)
Median (IQR) 2.2 (-2.2, 7.7) 1.1 (-4.4, 5.5) 1.1 (-3.3, 6.6)
Adjusted^ difference in means (95% CI) 0.00
-1.25(-3.39, 0.89)
*Conditional Logistic Regression^Adjusted for: OCS use in the 60 days prior to outcome HbA1c reading (Y/N) and time from Index date to outcome HbA1c reading (logged)
There is no significant difference between treatment groups in the change in HbA1c, having adjusted for confounders
Change in HbA1c

Adult ICS step-up; matched
Dose Response Curve
Change in HbA1c vs. total consumed ICS dose prior to outcome reading
Change in HbA1c
Conclusions
• There was a trend in the matched comparison of small particle vs. large particle ICS step-up, for:
− Higher odds of 1st onset of type 2 diabetes; and− Shorter times to 1st onset of type 2 diabetes
for patients stepping up with small particle ICS compared with patients stepping up with large particle ICS
• However, unmatched analyses indicate a significantly quicker progression to insulin treatment amongst diabetic patients prescribed large particle versus small particle ICS
• Other results were unconvincing, likely due to small sample sizes and low event rates
Diabetes Endpoints
Part II: ManuscriptsTime Item Lead
10.15-11.00 Current ManuscriptsUpdate
Liz Hillyer & Group Discussion
As requiredUpdate: Comparative cost-effectiveness analysis Qvar step-up vs ICS/LABA
Discussion / Review
As requiredPharmo analyses x 2
-ciclesonide vs. fine-particle-extrafine-particle vs. fine-particle ICS
As required Spacer vs no spacer
As required ICS step-up: FDC vs. separate inhaler
As required Dose response
As required Letter to ERJ: terminology

Manuscripts & journals
• Comparative cost-effectiveness analysis Qvar step-up vs ICS/LABA was submitted to PharmacoEconomics on April 23rd
o Current status as of May 9th: “Under review”, thus appears to be in peer review
• PHARMO analysis: ciclesonide vs. fine-particle ICS (FP + non-EF-BDP)o Readied for submission to Eur Respir Jo Pending several author forms (all are required
at first submission)

Manuscripts in internal review
• PHARMO analysis: Extrafine-particle ICS (Qvar + ciclesonide) vs. fine-particle ICS (FP + non-EF-BDP)o Target journal: BMC Pulmonary Medicine
• Spacer vs. no spacer (Qvar and FP, intracohort comparisons)o Target journal: Chesto Lead author: Gene Colice

Manuscripts in drafting phase
• ICS step-up: FDC vs. separate inhalero This had been on hold until acceptance of the
ICS step-up vs. FDC paper – now restarted
• Dose response papero A short report is under considerationo Possible journals: Ann Allergy, Respir Med,
Respir Res, npjPrim Care Respir Medo Leads: Gene Colice & Elliot Israel
Particle size terminology: denoting ICS particle size
• The consensus is to use extrafine vs. fine:• Extrafine for ICS with particle MMAD <2
microns (thus Qvar and ciclesonide)• Fine for ICS with particle MMAD <5 microns
but ≥2 microns (thus FP/non-extrafine BDP etc.)
Particle size terminology: Invited editorial for ERJ
• Proposed title:o Labeling the size of inhaler-delivered
particles: need for a consensus• Just ICS or all inhaled particles?• 1500-word & 30-reference limits; include 1 figure
and 1 table

Particle size: Invited editorial for ERJ - outline
• Both aerosol-related and patient-related factors determine inhaled drug deposition in the airways
• Particle size is the most important of the aerosol-related factors
• Basic background on how particle size influences deposition: oropharynx, central/intermediate airways, small airwayso FIGURE

Possible figure: from ERS/ISAM Task Force Report

Particle size: Invited editorial for ERJ – outline (cont.)• The need for consensus on particle
nomenclature• Terms used in the published literature:
o Extrafine, ultrafine, small versuso Large, standard-size, coarse
• Rationale for choosing the termso Based on ERS/ISAM Task Force Report: ERJ 2011o “Fine-particle fraction” or “fine-particle dose” are well-
accepted terms – = mass of drug consisting of particles <5µm

Particle size: Invited editorial for ERJ – outline (cont.)
• Rationale for choosing the terms (cont.)o ERS-ISAM consensus paper clearly denotes Qvar
and ciclesonide as being “extrafine.”
• Table ideas?o Drugs and particle sizes?
• Conclusions





























