Embed Size (px)
Citation preview

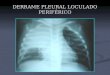
PLEURAL EFFUSIONTHE JUICE, OOZING FROM THE LEAKING
LINGERIE OF LUNGS
DR.RISHIKESAN K.V MD,DNB,
SPECIALIST PHYSICIAN,
VENNIYIL MEDICAL CENTRE, SHARJAH

DEFINITION
•Pleural effusion is an abnormal collection of fluid in the pleural space resulting from excess fluid production or decreased absorption or both.
• It is the most common manifestation of pleural disease.
•Etiologies range from cardiopulmonary disorders to symptomatic inflammatory or
malignant diseases.

BASICS
The pleural space is bordered by the parietal and visceral pleurae.
PARIETAL PLEURA - covers the inner surface of the thoracic cavity, including the mediastinum, diaphragm, and ribs.
VISCERAL PLEURA - envelops all lung surfaces, including the inter lobar fissures.

BASIC ANATOMY•Parietal Pleura Covers the
inner surface of chest wall• Blood supply: intercostal
arteries• Lymphatics drain the pleural
space• Pain fibers are present from
intercostal nerves• Mesothelial cells are
immunoreactive• 5 to 15 mL fluid present in
space• Normally high fluid flux 1Liter
/day• Venous drainage : the superior
vena cava
•Visceral Pleura Envelops entire surface of both lungs• The two pleural cavities
are separate• Composed of
mesothelial cells• Artery Supply: bronchial
arteries• Lymphatics drain the
pulmonary parenchyma• No nerve fibers• The venous drainage is
pulmonary vein
Both linings subject to disease and disorders

PLEURA : VISCERAL AND PARIETAL

BASICS ……
The pleural space plays an important role in respiration by coupling the movement of the chest wall with that of the lungs in 2 ways.
First, a relative vacuum in the space keeps the visceral and parietal pleurae in close proximity.
Second, the small volume of pleural fluid, which has been calculated at 0.13 mL/kg of body weight under
normal circumstances, serves as a lubricant to facilitate movement of the pleural surfaces against each other in the course of respirations

PATHOPHYSIOLOGY
The normal pleural space contains approximately
1 mL of fluid, representing the balance between (1) hydrostatic and oncotic forces in the visceral and parietal pleural vessels and (2) extensive lymphatic drainage.
DISRUPTION
OF BALANCE

PLEURAL EFFUSION
• Fluid in pleural space > 20 mL• Two mechanisms
• Excessive formation• Fluid resorption is disturbed
• Etiology• 40% cardiac causes• 60% other
• Pneumonia (48%)• Malignancy(24%)• Pulmonary embolism (18%)• Cirrhosis (6%)

PLEURAL EFFUSION
• The etiologic spectrum of pleural effusion is extensive.
• Most pleural effusions are caused by congestive heart failure, pneumonia, malignancy, or pulmonary embolism.
an indicator of an
underlying
disease process
May be
pulmonary
or non-
pulmonary
May be
acute or
chronic

PATHOPHYSIOLOGY : MECHANISM
# Altered permeability of the pleural membranes ( inflammation, malignancy, pulmonary embolus)
# Reduction in intravascular oncotic pressure (hypo albuminemia, cirrhosis)
# Increased capillary permeability or vascular disruption ( trauma, malignancy, inflammation, infection, pulmonary infarction, drug hypersensitivity, uremia, pancreatitis , infection, )
# Increased capillary hydrostatic pressure in the systemic and/or pulmonary circulation (congestive heart failure, superior vena cava syndrome)

# Reduction of pressure in the pleural space, preventing full lung expansion (extensive atelectasis, mesothelioma)
# Decreased lymphatic drainage or complete blockage, including thoracic duct obstruction or rupture (malignancy, trauma)
# Increased peritoneal fluid, with migration across the diaphragm via the lymphatics or structural defect (cirrhosis, peritoneal dialysis)
# Movement of fluid from pulmonary edema across the visceral pleura
# Persistent increase in pleural fluid oncotic pressure from an existing pleural effusion, causing further fluid accumulation
THE MECHANISMS…….

SIGNS AND SYMPTOMS
Common symptoms associated with pleural effusion may include:
• chest pain,
• difficulty breathing,
• painful breathing (pleurisy), and
• cough (either a dry cough or a productive cough).
Deep breathing typically increases the pain.
• Symptoms of fever, chills, and loss of appetite often accompany pleural effusions caused by infectious agents

DIAGNOSIS – PHYSICAL EXAMPHY.EX. in pleural effusion are variable and depend on the volume of the effusion. Generally,
there are no physical findings for effusions <300 mL. With effusions >300 mL, findings may include the following:
Dullness to percussion,
decreased tactile fremitus,
and asymmetrical chest
expansion, with diminished
or delayed expansion on the
side of the effusion – MOST
RELIABLE FINDINGS
Mediastinal shift
away from the
effusion - effusions
of greater than
1000 mL
Diminished
or inaudible
breath
sounds
Egophony - ("e" to
"a" changes) at the
most superior
aspect of the
pleural effusion
Pleural friction
rub

DIAGNOSISCXR: Often the first step identifying a pleural effusion.
Pleural effusions appear on chest X-rays as white space at the base of the lung.
If a pleural effusion is likely, additional X-ray films may be taken while a person lies on his side.
Decubitus X-ray films can show if the fluid flows freely within the chest.
Layering of an effusion on lateral decubitus
films defines a freely flowing effusion .
Effusions of more than 175 mL are usually apparent as blunting of the costophrenic angle on upright posteroanterior chest radiographs.

CHEST X RAY
On supine CXRs, which are commonly used in the intensive care setting, moderate to large pleural effusions may appear as a homogenous increase in density spread over the lower lung fields. Apparent elevation of the hemidiaphragm,
lateral displacement of the dome of the diaphragm, or
increased distance between the apparent left hemidiaphragm and the gastric air bubble
suggests subpulmonic effusions

LEARNING POINTS
Most often, pleural effusions are discovered on imaging tests. Common tests used to identify pleural effusions include: CHEST X RAY

DIAGNOSIS – CT SCAN
Compared to chest X-rays, CT scans produce more detailed information about pleural effusions and other lung abnormalities.

CT BILATERAL PLEURAL EFFUSIONS

LEARNING POINTS
Chest CT scanning with contrast should be performed in all patients with an undiagnosed pleural effusion, to detect
Thickened pleura or
signs of invasion of underlying or adjacent structures.
The two diagnostic imperatives in this situation are pulmonary embolism and tuberculous pleurisy
In both cases, the pleural effusion is a harbinger of potential future morbidity.
CT angiography should be ordered if pulmonary embolism is strongly suggested.

DIAGNOSIS - ULTRASOUND
Ultrasound can help guide drainage; identify whether pleural effusions are free flowing.
USS can aid in the differentiation of transudates from exudates: those with septated and homogenously echogenic patterns are always exudates, whereas hypoechoeic effusions may be either

•Should thoracentesis be
performed?
•If thoracentesis is done•Is the fluid a transudate or exudate?
•If the fluid is an exudate•What is the etiology?
Pleural Effusion Confirmed

DIAGNOSTIC ALGORITHM
WHEN PLEURAL EFFUSION IS DETECTED TWO QUESTIONS NEED TO BE ANSWERED
IS IT A TRANSUDATE ( DUE TO SYSTEMIC DISEASES) OR AN EXUDATE ( DUE TO DISEASE OF PLEURA ITSELF)?
IF THE EFFUSION IS EXUDATE WHAT IS THE DISEASE RESPONSIBLE FOR IT?
EXAMINING THE PLEURAL FLUID MAY GIVE AN ANSWER TO THESE QUESTIONS
NEARLY EVERY PATIENT WITH PLEURAL EFFUSION SHOULD HAVE A DIAGNOSTIC THORACENTESIS

DIAGNOSIS - THORACENTESIS
Should be done in almost all patients who have pleural fluid that is ≥ 10 mm in thickness on CT, ultrasonography, or lateral decubitus x-ray and that is new or of uncertain etiology.
In general, the only patients who do not require thoracentesis are those who have heart failure with symmetric pleural effusions and no chest pain or fever; in these patients, diuresis can be tried, and thoracentesis avoided unless effusions persist for ≥ 3 days.

LEARNING BITES : THORACENTESIS
•Most patients should be tapped• Newly recognized effusion
• Two exceptions
• Small Effusions ( < 1 cm on decubitus, US )
• Congestive Heart Failure
• Thoracentesis required only if bilateral
effusions not equal ie ASYMMETRICAL EFFUSION
• Fever
• Pleuritic chest pain
• Impending respiratory failure

ANALYSIS GROSS APPEARANCEGROSS
• BLOODY
• WHITE MILKY
• BLACK
• YELLOW GREEN
• DARK GREEN
• ANCHOVY SAUCE PASTE
• PUS (FETID ODOUR)
• CLEAR
• AMBER COLOR (SMELL OF URINE)
DIAGNOSIS• MALIGNANCY,ASBESTOSIS,PUL.INFARCT
-ION,POST CARD.SURGERY SYNDROME
• CHYLOTHORAX,PSEUDOCHYLOTHORAX
• ASPERGILLUS NIGER
• RA PLEURISY: TEST GLUCOSE
• BILOTHORAX
• AMOEBIC LIVER ABSCESS
• EMPYEMA
• CENTRAL LINE
• URINOTHORAX :CHECK UREA AND CREATINE OF THE PLEURAL FLUID

PLEURAL FLUID ANALYSIS
• Divide the fluid and routinely undertake the following:
• Send one sterile pot and a fluoride tube (for glucose measurement) to biochemistry for protein, lactate dehydrogenase, and glucose
• Send an EDTA vial for a differential white cell count either to cytology or haematology, depending on the local hospital policy
• Send a sterile pot of fluid to microbiology if you suspect pleural infection
• If malignancy is a possibility, send a sterile sample for cytology
• You should measure the pH of pleural fluid whenever you suspect pleural infection

CELLS AND DIFFERENTIAL COUNTS
• Volume 0.2 mL/kg
• Cells/ mm3 1000 – 5000• Mesothelial cells 60%• Monocytes 30%
•Lymphocytes 5%• PMN’s 5%
• Protein 1-2 g/d L
• LDH <50% plasma level
• Glucose plasma level
• pH ≥ plasma level
Cell Count:
PMN predominates in
parapneumonic effusions.
Pleural fluid lymphocytosis,
with values >85% , suggests
TB, CABG, lymphoma,
sarcoidosis, chronic RA
pleurisy, yellow nail
syndrome, and
chylothorax.

PLEURAL FLUID EOSINOPHILIA
Pleural fluid eosinophilia (PFE), with values greater than 10% of nucleated cells, is seen in approximately 10% of effusions.
No correlation with peripheral blood eosinophilia.
PFE is most often caused by air or blood in the pleural space.
PFE may be the result of pulmonary embolism with infarction or benign asbestos pleural effusion.
PFE may be associated with CSS, nonmalignant diseases, including parasitic disease , fungal infection and a variety of medications.

LEARNING BITES
The presence of PFE makes tuberculous pleurisy as well as empyema unlikely.
Mesothelial cells > 5% of total nucleated cells makes a diagnosis of TB less likely.
Markedly increased numbers of mesothelial cells, suggests PE as the cause of effusion.

You see a 68 year old man in clinic who has a three
week history of increasing breathlessness. His chest x ray
shows a large left pleural effusion. You perform a
diagnostic pleural aspiration. The pleural fluid analysis
shows:Protein 50 g/l
Lactate dehydrogenase (LDH) 457 (blood LDH 124)
Glucose 3.8 (blood glucose 4.8)
pH 7.32.
Which of the following statements is correct?
The fluid is an exudate
A pleural fluid protein of 50 g/l is
consistent with an exudative effusion.

Classically, if the patient's serum protein is
normal, a pleural fluid protein less than 30 g/l
usually indicates a transudate and a pleural
fluid protein greater than 30 g/l
usually indicates an exudate. Light's
criteria allow a more accurate differentiation
and should be the practical standard. In
practice, the criteria are often used if the
pleural fluid protein is between 25 and 35 g/l.


LIGHT’S CRITERIA
DIFFERENTIATES TRANSUDATES FROM EXUDATESIF ATLEAST ONE OF THE FOLLOWING IS MET, THEN EXUDATETRANSUDATIVE PLEURAL EFFUSION MEETS NONE
PLEURAL FLUID PROTEIN/SERUM PROTEIN >.5PLEURAL FLUID LDH/ SERUM LDH >.6 PLEURAL FLUID LDH > 2/3 THE UPPER LIMITS OF SERUM LDH

SERUM PLEURAL FLUID PROTEIN GRADIENT

TRANSUDATIVE EXUDATIVE EFFUSION
•Congestive Heart Failure.
The most common cause of pleural effusion is LVF
•Nephrotic syndrome
•Cirrhosis
•Meig’s Syndrome
•Hydronephrosis
• Peritoneal Dialysis
• Para pneumonic (The most
common exudative pleural effusion)
• Malignancy
• Pulmonary Embolism (either transudate or exudate)
• Tuberculosis
• Traumatic
• Collagen Vascular Disease(SLE,RA…)
• Drug Induced, Uraemia, Dressler’s Syndrome…….

DIAGNOSIS Transudate - produced through pressure filtration without capillary injuryExudate - "inflammatory fluid" leaking between cells.
Transudative pleural effusions - caused by systemic factors that alter the pleural equilibrium, or Starling forces. The components of the Starling forces–hydrostatic pressure, permeability, oncotic pressure
Exudative pleural effusions - caused by alterations in local factors that influence the formation and absorption of pleural fluid

LDHPROTEIN• MOST TRANSUDATES HAVE A
TOTAL PROTEIN OF <3 GM/DL
• TB PLEURAL EFFUSION GRATER THAN 4GM/DL
• IF THE PROTEIN CONCENTRATION IS > 7-8 GM/DL, CONSIDER THE DIAGNOSIS OF WALDENSTROMS MACROGLUBULINAEMIA OR MULTIPLE MYELOMA
LDH
• ONE OF THE KEY CRITERIA FOR LIGHT’S CRITERIA
• LDH MORE THAN 1000, COMMONLY SEEN IN Empyema, Rheumatoid pleurisy and Malignancy
Pneumocystis jirovecci PLEURAL EFFUSION
PLEURAL FLUID LDH/ SERUM LDH : >1
PLEURAL FLUID PROTEIN/SERUM PROTEIN : < .5

PLEURAL FLUID GLUCOSE• A LOW PLEURAL FLUID GLUCOSE CONCENTRATION <30-50
MG/DL OR PLEURAL FLUID/SERUM GLUCOSE <.5 NARROWS THE DIFFERENTIAL
CAUSES:
• Malignant effusion,
• Tuberculous pleuritis,
• Esophageal rupture, or
• Lupus pleuritis.
A very low pleural glucose concentration (i.e.< 30 mg/d L) further restricts diagnostic possibilities, to rheumatoid pleurisy or empyema

PLEURAL FLUID PH
• Pleural fluid pH is highly correlated with pleural fluid glucose levels
• A pleural fluid pH of less than 7.30 with a normal arterial blood pH level is caused by the same diagnoses as listed above for low pleural fluid glucose.
• In parapneumonic effusions a pleural fluid pH of less than 7.1-7.2 indicates the need for urgent drainage of the effusion,while a pleural fluid pH of more than 7.3 suggests that the effusion may be managed with systemic antibiotics alone.
• In malignant effusions, a pleural fluid pH of less than 7.3 has been associated in some reports with more extensive pleural involvement, higher yield on cytology, decreased success of pleurodesis, and shorter survival times < 30 days

PLEURAL FLUID AMYLASE
•PLEURAL FLUID AMYLASE MORE THAN ULN FOR SERUM AMYLASE
•PLEURAL FLUID AMYLASE/SERUM AMYLASE > 1
DIFFERENTIALS
• CHRONIC PANCREATIC PLEURAL EFFUSION
• ESOPHAGEAL RUPTURE
• ACUTE PANCREATITIS
• MALIGNANCY

ADENOSINE DEAMINASE• High levels of ADA are
commonly seen in tuberculous effusions, but false positives (especially with empyema, rheumatoid effusions, and lymphomas) do occur.
• Routine measurement of ADA is not encouraged in non-endemic areas such as the UK.
In endemic areas, however, a low pleural fluid ADA effectively excludes pleural tuberculosis.
SINCE LESS THAN 40% OF TB PLEURAL EFFUSION
HAVE POSITIVE PLEURAL FLUID CULTURE
ALTERNATIVE MEANS SUCH AS THE LEVEL OF
ADA, GAMMA INTERFERON OR PCR ARE USED
TO ESTABLISH THE DIAGNOSIS

OTHER USEFUL TESTS
•Brain Natriuretric Peptide Normal <1000 p g/mL ; >1000 in CHF
• Triglycerides > 110 mg/d L• Chylothorax
•Microbiology (bacterial and mycobacterial culture)
If clinically indicated, send samples for Gram staining and culture. Inoculation of blood culture bottles may improve yield.
•CytologyRequest cytology if you suspect malignancy - it provides the diagnosis in 60% of all malignant effusions.The diagnostic yield increases with a second sample, but not with further samples

IS IT WORTH DOING ?
Tumour markers
• There is no routine clinical role for these at present.
Rheumatoid factor, antinuclear antibody, complement
• Pleural fluid values mirror serum levels and are of little additional benefit.
Bronchoscopy
• The majority of pleural effusions seen in clinical practice are not associated with a lung parenchymal abnormality as the cause. Bronchoscopy is therefore only advised if the patient has symptoms such as haemoptysis or CT features suggesting endobronchial involvement.

PARAPNEUMONIC EFFUSION
• ANY PLEURAL EFFUSION ASSOCIATED WITH BACTERIAL PNEUMONIA, LUNG ABSCESS , OR BRONCHIECTASIS
• GRAM STAIN AND BACTERIAL CULTURE WILL IDENTIFY INFECTED PLEURAL FLUIDS
• EFFECTIVE ANTIBIOTIC THERAPY IS THE KEY ISSUE FOR CONTROLLING INFECTION
WHEN PLEURAL FLUID ANALYSIS MEETS ANY OF THE FOLLOWING
CRITERIA ICTD SHOULD BE DONE IMMEDIATELY1.EMPYEMA
2.PLEURAL FLUID CULTURE IS POSITIVE
3.PLEURAL FLUID GLUCOSE IS LESS THAN 40 MG%
4.PLEURAL FLUID P H <7.0

TUBERCULOUS PLEURAL EFFUSION
• MOST PATIENTS PRESENT WITH PLEURITC CHEST PAIN
• TUBERCULOSIS TOXIC SYNDROME : DRY COUGH,LOW GRADE FEVER, NIGHT SWEAT AND LOSS OF WEIGHT.
• POSITIVE TUBERCULIN- PPD- TEST, SIGNIFICANTLY HIGH ADA LEVEL IN PLEURAL FLUID (ADA ACTIVITY OF > 43 U/ML)
• EXUDATIVE EFFUSION WITH MARKEDLY ELEVATED PROTEIN LEVEL >50 GM/L.
• IFN GAMMA CONCENTRATION >140 p g/ml SUPPORT THE DIAGNOSIS
• DIFFERENTIAL WHITE CELL COUNT SHOWS > 80% LYMPHOCYTES.
• PLEURAL BIOPSY HAS GOT THE GRATEST UTILITY IN ESTABLISHING THE DIAGNOSIS.
• DEMONSTRATION OF CASEATING GRANULOMA AS WELL AS ACID FAST BACILLI AS THE CONFIRMATORY PROOF

WHY DO WE TREAT TB EFFUSION?
Tuberculous pleuritis is typically self-limited. If not treated the effusion will resolve but pulmonary or extra pulmonary tuberculosis subsequently develops in >65% of patients within five years.
Empiric ATT is the option, pending culture results when sufficient clinical suspicion is present, such as an unexplained exudative or lymphocytic effusion in a patient with a positive PPD finding

MANAGEMENT OF TUBERCULOUS PLEURAL EFFUSION• ATT : ADEQUATE THERAPY IS NINE MONTHS TREATMENT
WITH RIFAMPICIN AND INH DAILY
• PERFORMANCE OF THERAPEUTIC THORACENTESIS IS HIGHLY RECOMMENDED
• HIGHLY SYMPTOMATIC PATIENTS SHOLUD BE PUT ON PEDNISOLONE 40MG.DAILY AND THEN GRADUALLY TAPERED OVER SEVERAL WEEKS
• THE ADMINISTRATION OF CORTICOSTEROIDS WILL RAPIDLY RELEIVE THE SYMPTOMS OF FEVER,CHEST PAIN AND MALAISE.
• IT DOESN’T DISSEMINATE THE DISEASE

DRESSLER’S SYNDROME
• POST CARDIAC INJURY SYNDROMES .
•POST CABG EFFUSIONS ARE COMMON.
• EXAGGERATED IMMUNE RESPONSE TO CARDIACANTIGENS
•PLEURITIC CHEST PAIN ,FEVER,HIGH ESR, LEUCOCYTOSIS, ANTI MYOCARDIAL ANTIBODIES.
• PMN LEUCOCYTOSIS <30 DAYS;LATER LYMPHOCYTOSIS
•NSAIDS AND STEROIDS AS TREATMENT• 1-12 MONTHS AFTER SURGERY, AVERAGE 3 WEEKS

MALIGNANT PLEURAL EFFUSIONMALIGNANT PLEURAL EFFUSIONS SIGNIFY INCURABLE DISEASE .
THE SECOND MOST COMMON TYPE OF EXUDATIVE EFFUSION.
THE 3 TUMORS THAT CAUSE approx. 75% OF MALIGNANT EFFUSIONS ARE LUNG, BREAST & LYMPHOMA
MEAN SURVIVAL < 1 YEAR.
RECURRENT MASSIVE EFFUSIONS MAY NEED REPEATED THORACENTESIS, PLEURODESIS OR PLACEMENT OF INDWELLING TUNNELED CATHETERS WHICH
PROVIDES GOOD PALLIATION

HEART FAILURE WITH ASYMMETRICAL EFFUSION
A 78 year old woman presents with a 3 week h/o increasing breathlessness, orthopnoea, and peripheral oedema. She had an AWMI 2 months ago.
Her CXR shows venous congestion and bilateral pleural effusions, with the right sided effusion larger than the left. What would you do?
•Start therapy for heart failure and observe
• This woman gives a typical history of heart failure, which you should treat before you perform further investigations.
Asymmetrical pleural effusions are recognised in heart failure. You should only attempt a pleural aspiration if the patient fails to respond to treatment for the heart failure.

IDIOPATHIC EXUDATIVE EFFUSIONS
• DESPITE REPEATED DIAGNOSTIC THORACENTESES APPROX. 20% OF EXUDATIVE EFFUSIONS REMAIN UNDIAGNOSED.
• MAY BE BENIGN ASBESTOSIS ( EXPOSURE TO ASBESTOSE 10-20 YEARS BACK)
• DRUG INDUCED ( NITROFURANTOIN, AMIODARONE,PHENYTOIN,METHOTREXATE )
• DRUG INDUCED LUPUS OR
• HEPATIC HYDROTHORAX WITH MINIMAL OR UNDETECTABLE ASCITES.
In practice, many patients with undiagnosed effusions turn out to have malignancy.

NO FURTHER EVALUATION IF….
•PATIENT CLINICALLY STABLE
•NO WEIGHT LOSS
•ADA AS WELL AS PPD NORMAL
•NO FEVER
•THE EFFUSION OCCUPIES LESS THAN 50% OF THE HEMITHORAX
ONE SHOULDN’T BE TOO AGGRESSIVE IF THE PATIENT IMPROVING CLINICALLY

MANAGEMENT OF PLEURAL EFFUSION
Medical Management:
Antibiotics
Analgesics
Diuretics
Cardiotonic Drugs
Thoracentesis
CTT
Pleurodesis

Thoracentesis
aspiration of fluid or air from the pleural cavity.
instillation of medication into the pleural space
MEDICAL/SURGICAL MANAGEMENT, DRUGS, AND TREATMENT

If mesothelioma is likely, you should
tattoo the site of aspiration with Indian ink.
This will enable prophylactic radiotherapy
to be given if the diagnosis is confirmed.
Repeated aspiration attempts are not
recommended, but if more than one
pleural puncture is made, you need to
mark both sites.

You are told to remove "a good litre or so" of pleural fluid
from a stoical 82 year old man who has presented to clinic
with a large pleural effusion. During the procedure, after
you have removed 900 ml, he develops chest discomfort
but says he can bear it. What would you do?
Stop the procedure You should stop the procedure if a patient develops chest
discomfort or a cough, or if resistance to the aspiration is
felt. These may indicate the development of re-expansion
pulmonary oedema. Aspiration of 900 ml should achieve
symptomatic relief, and so it would be appropriate to stop.

RE EXPANSION PULMONARY EDEMA
It is serious and can be fatal.
The exact pathophysiology is not fully understood.
Alteration of endothelial permeability and disruption of the alveolar-capillary membrane, are probably involved.
Re-expansion pulmonary oedema may either resolve spontaneously or result in hypoxic respiratory failure with catastrophic circulatory collapse.
Draining a large amount of fluid (usually more than 1.5 l)
too rapidly, especially if the lung has been
collapsed for several weeks, may lead to
re-expansion pulmonary oedema.

NURSING MANAGEMENT-THORACENTESIS
Verify a signed informed consent
Assist client to an appropriate position
Instruct client not to move during the procedure including no coughing or deep breathing.
Provide comfort
Maintain asepsis
Monitor vital signs during the procedure – also monitor pulse oximetry if client is connected to it

@Apply a dressing over a puncture and position the client on the unaffected side. Instruct the client to stay in this position for at least 1 hour.
@During the first several hours after thoracentesis frequently assess and document vital signs, oxygen saturation, respiratory status including respiratory excursion, lung sounds, cough and hemoptysis and puncture site for bleeding or crepitus.
@Obtain a chest x-ray
NURSING MANAGEMENT –Thoracentesis

On the ward round, you see a 55 year old man with COPD was
admitted with an AECB three days ago. He continues to have
fevers and raised inflammatory markers following treatment. His
CXR shows a small to moderate pleural effusion. You request an
USG pleural aspiration. The aspirate yields frank pus, which is sent
for microscopy and culture. How would you manage him?
Continue with antibiotics and arrange for a
guided chest drain insertion He requires drainage of the pleural fluid with ongoing
antimicrobial treatment. The addition of anaerobic cover
is appropriate, if not already started. As he has an
underlying lung disease and a small collection, this should
be done under imaging guidance.

Done to drain fluid, blood and air from the space around the lungs. Whether the accumulation is the result of rapid traumatic filling or insidious malignant seepage, placement of a chest tube allows for continuous, large volume drainage until the underlying pathology can be more formally addressed.
CHEST TUBE THORACOSTOMY

TRIANGLE OF SAFETY
• The British Thoracic Society guidelines define a triangle of safety for needle insertion, bordered by:
• The anterior border of latissimus dorsi
• The lateral border of pectoralis major muscle and
• The line superior to the horizontal level of the nipple with the apex based within the axilla.

POSITIONA suggested position is
SEMI-DECUBITUS ON THE BED AT 45 degrees WITH THE ARM BEHIND THE HEAD SO AS TO EXPOSE THE AXILLARY AREA.
The drain should ideally be inserted in the SAFE TRIANGLE which is delineated by the lateral border of the pectoralis major , the anterior border of the latissimus dorsi and a line horizontal with the nipple. Most clinicians insert the tube via an incision at this space in the ANTERIOR AXILLARY or 4th or 5th
intercostal MIDAXILLARY LINE

Ensure a signed consent for chest tube insertion
Position as indicated for the procedure
Assist with chest tube insertion as needed
Assist respiratory status at least every 4 hours.
Maintain a closed system.
Ensure tubing with no kinks or not compressed
Check the water seal frequently.
Palpate the area around the chest tube sitefor subcutaneous emphysema or crepitus.
Encourage client for coughing and deep breathing
Assist with frequent position changes ,sitting and ambulation as allowed
NURSING MANAGEMENT – CLOSED TUBE THORACOSTOMY

LEARNING BITES
Your consultant asks you to perform a therapeutic pleural aspiration on a woman who is taking warfarin for atrial fibrillation.
She has presented with a large right pleural effusion on her chest x ray and is increasingly distressed as a result of her breathlessness. Her INR is 2.0.

GUIDELINES
•Aspirate 1 litre of fluid for symptomatic relief and diagnostic purposes
• This common clinical scenario often raises difficult management questions. There are no published data to suggest an increased risk of bleeding following a pleural aspiration or insertion of a chest drain in patients with an underlying coagulopathy or thrombocytopenia In clinical
practice, therapeutic and diagnostic pleural aspiration are generally performed when the INR is less than or equal to 2.
• For elective insertion of a chest drain, the British Thoracic Society guidelines recommend that time is given for the anticoagulation effects to resolve.
• Guidelines suggest that percutaneous lung or pleural biopsies are not performed with an INR greater than 1.4.

Pleurodesis is performed to prevent recurrence of pneumothorax or recurrent pleural effusion also known as Pleural Sclerosis.Involves instilling an irritant into the pleural space to cause inflammatory changes that result in bridging fibrosis between the visceral and parietal pleural surfaces.
PLEURODESIS

Ensure informed consent
Record baseline vital signs
Consider the use of pre medication
Position patient comfortably
An existing effusion should be completely drained before the procedure
Ensure a recent chest x-ray
Observe for excessive pain and breathlessness
Patient ambulation is possibly helpful to ensure good spread of the slurry
NURSING MANAGEMENT – PLEURODESIS

Q AND A•Cytological analysis of two separate samples of pleural fluid from a man with an undiagnosed exudative pleural effusion, who presented with worsening dyspnoea in the absence of other symptoms, reveals no malignant cells.
• Initial Gram and Ziehl-Nielsen stains are
negative. What would you do next ?

………….THORACOSCOPY•Medical thoracoscopy would be an appropriate next step.
•This would allow pleural biopsies to be taken under direct vision and therapeutic drainage of pleural fluid.
•If appearances suggested pleural malignancy, pleurodesis with talc poudrage could be done.

TAKE HOME MESSAGE
ASYMPTOMATIC OR MILDLY SYMPTOMATIC EFFUSIONS MAY JUST BE LEFT AND OBSERVED.
A LARGE PLEURAL EFFUSION THAT MAKES YOU BREATHLESS CAN BE DRAINED.
UNLESS THE UNDERLYING CAUSE CAN BE TREATED, AN EFFUSION IS LIKELY TO RETURN.
REPEATED DRAINING, PERMANENT ICTD, PLEUROPERITONEAL SHUNT, AND PLEURECTOMY ARE DIFFERENT OPTIONS FOR RECURRENT EFFUSIONS.
PLEURODESIS IS MOST OFTEN USED IN THE TREATMENT OF REPEATED EFFUSIONS CAUSED BY CANCER.

THANK YOU……
ANY QUESTIONS??????????