Embed Size (px)
Citation preview
MRI: techniques for rectal cancer staging and
standardisationGina Brown
Department of RadiologyRoyal Marsden HospitalImperial College, London
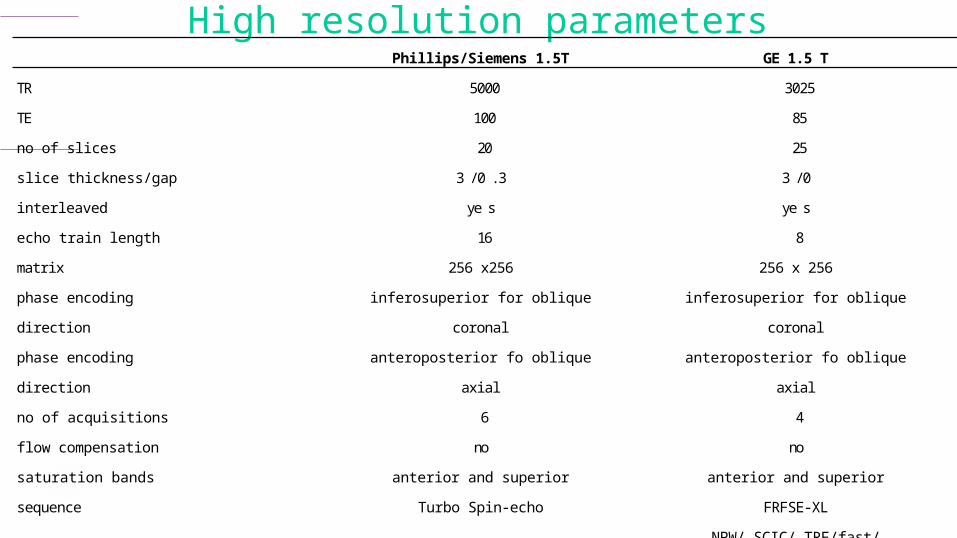
The Royal Marsden High resolution parameters Phillips/Siemens 1.5T GE 1.5 T
TR 5000 3025
TE 100 85
no of slices 20 25
slice thickness/gap 3 /0 .3 3 /0
interleaved ye s ye s
echo train length 16 8
matrix 256 x256 256 x 256
phase encoding inferosuperior for oblique inferosuperior for oblique
direction coronal coronal
phase encoding anteroposterior fo oblique anteroposterior fo oblique
direction axial axial
no of acquisitions 6 4
flow compensation no no
saturation bands anterior and superior anterior and superior
sequence Turbo Spin-echo FRFSE-XL
NPW/ SCIC/ TRF/fast/
options no phase wrap ZIP512
scan duration 7 mins 5 to 7 minutes

The Royal Marsden
Sagittal T2w TSE• FOV 250
• RFOV 100%• 24 slices• 3/.0.4mm• Foldover direction AP• 2 rest slabs anterior & superior• TSE factor 23• TE 125• TR 3961• Matrix 320/512r• Scan % 100• NSA 4• Scan length 6mins
The Royal Marsden
1. Ensure scans are T2 weighted high resolution
• field of view and matrix parameters should not exceed a pixel size of 0.6mm x 0.6mm
Either 200mm x 200mm with 384 x 384 matrix Or 60mm x 160mm with a 256 x 256 matrix
pixel size in mm = field of view/matrixvoxel size mm3 = pixel size x slice thickness

The Royal Marsden
High res vs non high res• the difference
between a high resolution and suboptimal MRI scan. The difference in technique can make a subtantial but entirely preventable difference to staging accuracy.
High res –showing Early T2 tumour
Non-High resSame patient – T stage?
The Royal Marsden
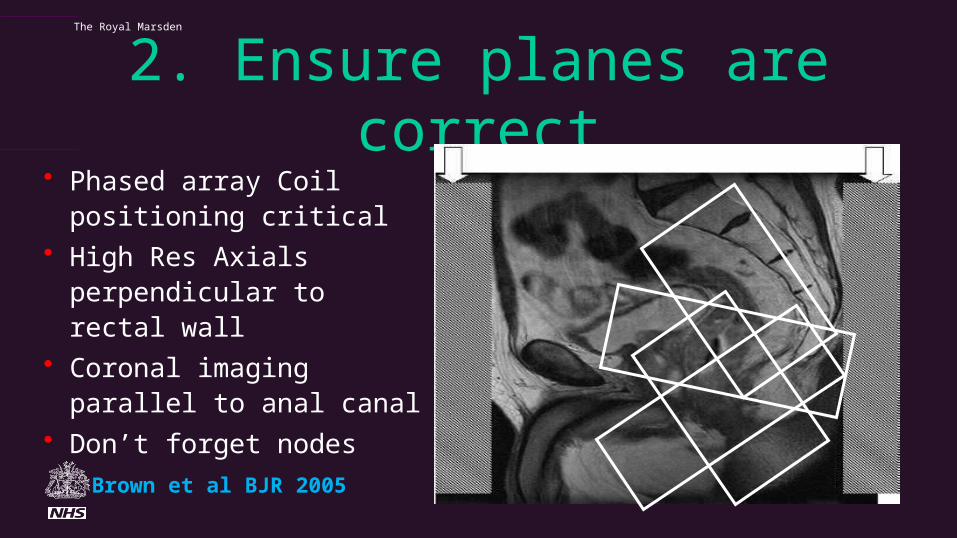
2. Ensure planes are correct• Phased array Coil
positioning critical• High Res Axials
perpendicular to rectal wall• Coronal imaging parallel to
anal canal• Don’t forget nodes
Brown et al BJR 2005

Correct Scan planes•Scans should be obtained perpendicular to the rectal wall, the sagittal MRI scans are used to plan the oblique axial images •Coronal images should be undertaken parallel to the anal canal to visualise the distal anorectum and distal mesorectal plane•High resolution coverage should include at least 5cm above the top of the tumour and to the L5/S1 level for all tumours to ensure that discontinuous tumour deposits are visualised

The Royal Marsden

The Royal Marsden
3. Use of Sat Bands and firm abdominal compression to limit abdominal wall motion
The use of anterior and superior saturation bands reduce image degradation due to abdominal wall motion and hyoscine butylbromide given as an i.m. injection or oral mebeverine reduces small bowel peristalsis respectively
Without Sat Bands With Sat Bands

The Royal MarsdenReduction of physiological motion
• Good lower abdominal compression esp in thin patients
• Use of saturation bands / REST Slabs
If phase AP Swap Phase direction
R-L

The Royal Marsden
Empty bladderUse of anti-spasmodics

The Royal Marsden
Peristalsis – use of antispasmodics

The Royal Marsden
4. Correct Coil Position
The surface phased array coil should be placed correctly over the lower pelvis. For low rectal cancers the distal edge of the coil should lie 10cm below the symphysis pubis to ensure that the distal rectum is in the centre of the image

The Royal Marsden
5. Other Sequences?• T1 weighted imaging, contrast enhanced imaging and fat saturated
sequences do not contribute and worsen staging accuracy and should not be used for primary rectal cancer staging.
• Caution when using diffusion weighted imaging for rectal cancer as it does not improve accuracy when compared with high resolution MRI techniques.
• The prolonged examination time caused by additional non-contributory sequences reduce the overall quality of the examination as well as prolonging patient discomfort.

The Royal Marsden
DWI has insufficient resolution to distinguish tumour from fibrosis
bа с d

The Royal Marsden
Fat Saturation and Contrast Enhancement Does not improve accuracy
Tumour and normal anatomy both enhance
and are not distinguished

The Royal Marsden
MDT choices and making best use of high resolution MRI
MRI based Selectionof patientsFor range treatments
Local excision
MRI and PET surveillanceDeferral of surgery
ChemoradiotherapyRestage:Timing of surgery
after CRT6 vs 12?
Biological agents and neoadjuvant chemotherapy for MRI EMVI
Further Therapy/Extended surgery
for mrCRM/low rectal
MRI T1/T2 NxEMS /TEMS
pre/post operative CRTMRI surveillance…
MRI Low rectal Stage 3 or 4
Post CRTyMRI TRG 1-2
MRI T3a/T3b N anyLow rectal stage 1/2 Primary TME Surgery: open v laparoscopic
MRI T3c/T3d N anyEMVI positive CRM safe
potential CRM unsafe

Reporting Minimum StandardsBaseline assessment of Rectal cancer MRI report Primary tumour The primary tumour is demonstrated as an [ Annular | Semi-annular | Ulcerating | | Polypoidal | Mucinous] mass with a [nodular / smooth] infiltrating border. The distal edge of the luminal tumour arises at a height of [ ] mm from anal verge: The distal edge of the tumour lies [ ]mm [Above,at, below] the top of the puborectalis sling The tumour extends craniocaudally over a distance of [ ] mm The proximal edge of tumour lies [above at below] the peritoneal reflection Invading edge of tumour extends from [ to ] O’clock Tumour is [confined to] [extends through] the muscularis propria: Extramural spread is [ ] mm mrT stage: [T1 ] [ T2 ] [ T3a] [ T3b ] [ T3c] [ T3d ] [T4visceral ] [T4 peritoneal] Tumour is [present] [not present] the level of the puborectalis sling at this level: [Tumour is confined to the submucosal layer/part thickness of muscularis propria indicating that the intersphincteric plane/mesorectal plane is safe and intersphincteric APE or ultra low TME is possible] [Tumour extends through the full thickness of the muscularis propria : intersphincteric plane/mesorectal plane is unsafe, Extralevator APE. is indicated for radial clearance] [Tumour extends into the intersphincteric plane : intersphincteric plane/mesorectal plane is unsafe, therefore an extralevator APE. is indicated for radial clearance] [Tumour extends into the external sphincter : intersphincteric plane/mesorectal plane is unsafe.] [ Tumour extends into adjacent [prostate/vagina/bladder/sacrum] : exenterative procedure will be required Additional comments: .
Lymph node assessment Only benign reactive and no suspicious nodes shown [N0] [ ] mixed signal/irregular border nodes [N1/N2] Extramural venous invasion: [ No evidence ] [ Evidence] [ ] Small [ ]Medium [ ]Large vein invasion is present CRM The closest circumferential resection margin is at o’clock The closest CRM is from [Direct spread of tumour] [Extramural venous invasion] [Tumour deposit] Minimum tumour distance to mesorectal fascia: mm [CRM clear ] [CRM involved] Peritoneal deposits: [ No evidence] [ Evidence] Pelvic side wall lymph nodes: [ None] [ Benign] [ Malignant mixed signal/irreg border] Location: [Obturator fossa • R •L ] . [External Iliac Nodes • R •L] .[ Internal iliac • R •L ] Summary: MRI Overall stage: T N M [CRM clear] , [ CRM involved ] , [ EMVI positive] [EMVI negative],[PSW positive ] [PSW negative] No adverse features eligible for primary surgery High risk safe margins for preoperative therapy : eligible for Serenade, Marvel Poor prognosis unsafe margins eligible for preoperative chemoradiotherapy: eligible for 6 vs 12 trial Low Rectal <6cm – eligible for the Low Rectal Study.

Post Treatment Assessment MRI Rectal Cancer Comparison is made with the previous examination of: • The treated tumour: shows no fibrosis,TRG5 • Less than <25% fibrosis, predominant tumour signal, TRG4 • 50% tumour/fibrosis, TRG 3 •>75% fibrosis, minimal tumour signal intensity,TRG2 •low signal fibrosis only no intermediate tumour signal TRG1 The distal edge of the luminal tumour arises at a height of [ ] mm from anal verge: The distal edge of the tumour lies [ ]mm [Above, at, below] the top of the puborectalis sling compared with []mm previously The tumour extends craniocaudally over a distance of [ ] mm compared with [ ]mm previously The proximal edge of tumour lies [above at below] the peritoneal reflection The invading edge of treated tumour extends from [ to ] O’clock Tumour signal is [Confined to / Extends through the muscularis propria.] Fibrotic signal is [ Confined to / Extends through muscularis propria.] Extramural spread: [ ]mm for tumour signal [ ]for fibrotic stroma yMR T stage: • T1 • T2 • T3a • T3b • T3c • T3d •T4 visceral •T4 peritoneal Treated tumour [is/ is not] present at or below the puborectalis sling • tumour signal/fibrosis extends into the submucosal layer/part thickness of muscularis propria : intersphincteric plane/mesorectal plane is safe intersphincteric APE or ultra low TME possible, CRM is safe • tumour signal/fibrosis extends through the full thickness of muscularis propria : intersphincteric plane/mesorectal plane is unsafe, for extralevator APE. • tumour signal/fibrosis extends into external sphincter : intersphincteric plane/mesorectal plane is unsafe:for extralevator APE •tumour signal/fibrosis extends into beyond external sphincter into [prostate/vagina ] : intersphincteric plane / mesorectal plane is unsafe, for extralevator APE.
Lymph nodes: • None /Only benign reactive [N0] • Present number mixed signal/irregular border [N1/N2] Extramural venous invasion: [• No evidence • Evidence] [• Small • Medium • Large] CRM Closest circumferential resection margin: [ ]O’clock Closest CRM is from [ Direct spread of tumour • Extramural venous invasion • Tumour deposit] Minimum tumour distance to mesorectal fascia: [ ]mm [ • CRM clear • CRM involved] Peritoneal deposits: [• No evidence • Evidence ] Pelvic side wall lymph nodes: • None • Benign • Malignant [Location: Obturator fossa • R •L . External Iliac Nodes •R •L. Inf Hypogastric •R •L ] Summary: y MRI Overall stage ymrT ymr N M , TRG • Low/intermediate risk, CRM clear, TRG 1-2, EMVI negative • High prognosis, CRM pos or TRG4/5 or EMVI positive TRG1-2 low tumour – eligible for consideration for deferral of surgery
Reporting Template Post Treatment

The Royal Marsden
Technique Summary of Essentials
• Scan duration = quality 7mins average length of each sequence• 4-6 NSA/NEX and T2- FSE / TSE /FRFSE• 0.6mm x 0.6mm x 3mm = 1.1mm3 voxel• Adequate coverage – 5cm above top of tumour• Perpendicular to the rectal wall• Low rectal cancer – parallel to anal canal• Ensure discontinuous deposits are covered on high res• Buscopan• Saturation Bands• Firm coil placement with secure abdominal compression

The Royal Marsden
Key Bioimaging markers for poor outcome at baseline and post CRT
• CRM involvement on MRI• Depth of extramural spread >5mm• Presence of MRI detected venous invasion• MRI detected mucinous tumours• Tumour spread into or beyond the intersphincteric
plane• MRI TRG status

10th – 11th March 2016, London, UK Intensive Hands On 2 Day Workshop How to perform Rectal MRI staging and restaging accurately and consistentlyHANDS ON WORKSTATION PRACTICE CASES CASE DISCUSSIONSTIPS AND TRICKS FOR : REPORTING AND MDT BASED WORKING
Email:[email protected] receive further details





























