Embed Size (px)
Citation preview

MRI FOR CA RECTUMAdnan Rashid, MD
(Dept of Radiology SIMS/SHL)

THE ROLE OF MRI
To determine:
Diagnosis, location and extent of the tumor
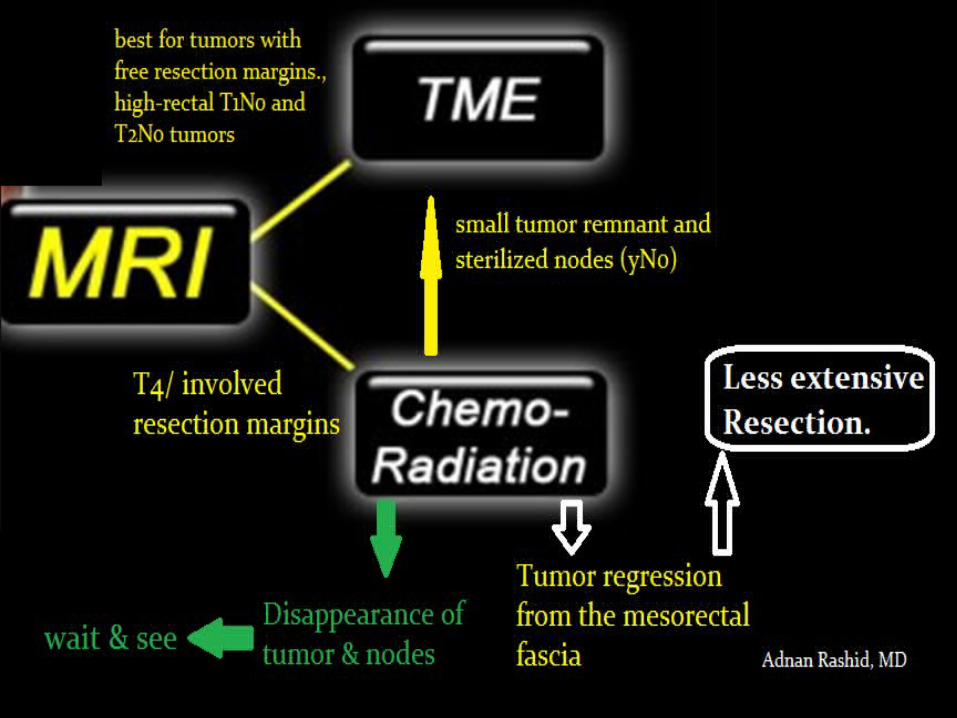
whether Total Mesorectal Excision(TME) is possible or whether there is an advanced tumor that should be down-staged with chemo-radiation and followed by TME at a later stage.

TOTAL MESORECTAL EXCISION(TME)
Completely Remove: Mesorectal compartment rectum mesorectal fat, peri-rectal L.nodesIts envelope, i.e. the mesorectal fascia (the resection plane in TME)
Modern technique for resectable CA

INFORMATION FROM MRI: Location
Length of the tumor
T-stage
N-stage

MRI PROTOCOL:Only FSE (fast spin echo ) T2WIGadolinium NOT neededImages are made in the sagittal, coronal and axial
plane.Field of view (FOV) is L5, to below the anal canal. Use an external coil.
No fat suppression/ bowel preparation needed The use of rectal contrast is not advised Diffusion weighted images can be used in
restaging MRI.High signal on B1000 images indicates incomplete response.

Angulation
Axial images have to be angulated perpendicular to the axis of the tumor to avoid volume averaging.At first the axial images were not properly angulated. This resulted in the false impression, that the MRF was involved on the anterior side (red circle).After proper angulation it was noted, that the MRF was not involved (yellow circle).

1)21) Rectum
2) mesorectal fat (High signal on T1WI & T2WI)
3) Mesorectal fascia appears as a fine line of low signal intensity (red arrows). P: prostate and V: seminal vesicles
The distance between tumor to the mesorectal fascia is the most powerful predictor for local recurrence (⩽1 mm =The mesorectal fascia is involved ) (1-2mm =The mesorectal fascia is threatened )(> 2mm the mesorectal fascia is safe)

LOCATION OF THE TUMOR
Rectum: 15 cm above the anal verge/ anorectal angle
Low rectal cancer:distal border is 0- 5 cm from the anorectal angle
Mid rectal cancer:distal border is 5-10 cm from the anorectal angle
High rectal cancer:distal border is 10-15 cm from the anorectal angle


FOR T3
Circumferential resection margin(CRM);
T3 CRM- : T3-tumor with a wide (> 2mm ) circumferential resection marginT3 CRM+ ; T3-tumor with involved circumferential resection margin (red arrow)The shortest distance from the tumor or lymph nodes to the mesorectal fascia (CRM).

T1 AND T2 (GOOD PROGNOSIS)
Rectal tumorcompletely surrounded by the black layer of the muscularis externa. This is a T2 tumor.

T3 MRF-
Infiltration of the mesorectal fat, i.e. T3 (arrow).
There is a wide resection margin
TX: short preoperative course of radiotherapy followed by TME.

T3 MRF+
InfiltratesMesorectal fat with the resection margin on the anterior side
(arrow) Tx: radiotherapy and chemotherapy preoperatively.
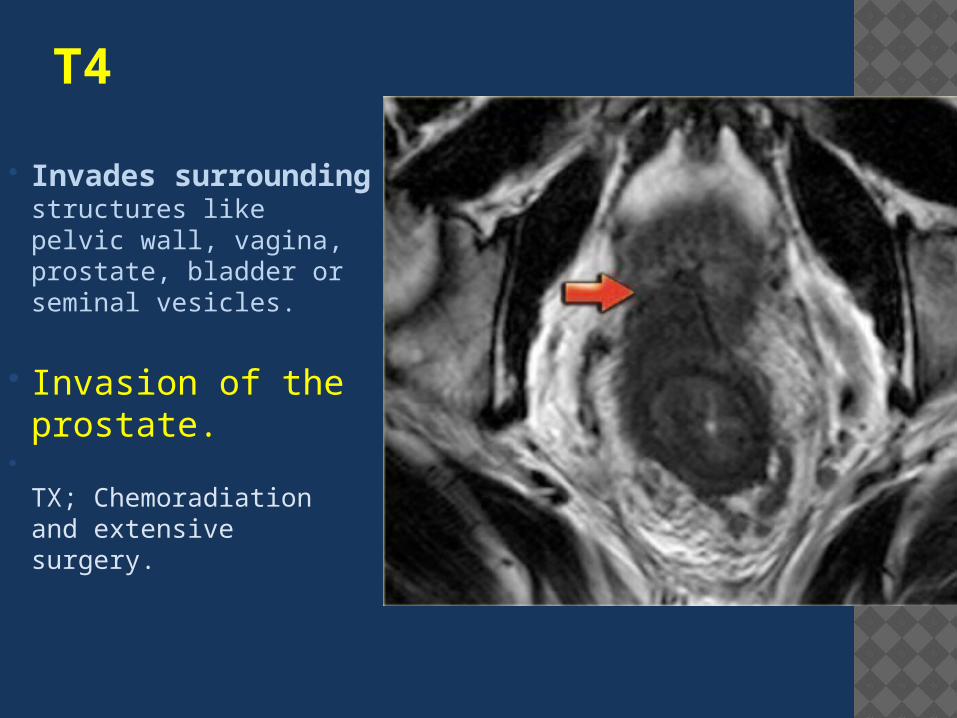
T4 Invades
surrounding structures like pelvic wall, vagina, prostate, bladder or seminal vesicles.
Invasion of the prostate.
TX; Chemoradiation and extensive surgery.
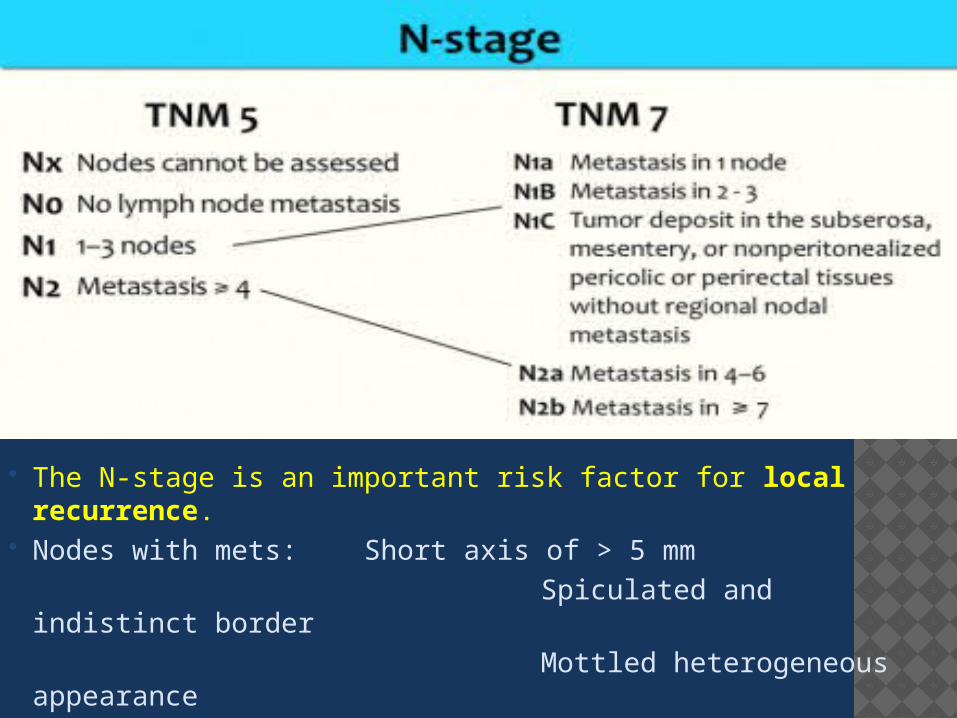
The N-stage is an important risk factor for local recurrence.
Nodes with mets: Short axis of > 5 mm Spiculated and indistinct border Mottled heterogeneous appearance

low rectal cancer with multiple nodes in the perirectal fat on the posterior side.
MRF+ and N+
Low rectal cancer higher local
recurrence rate.The distal tapering of the mesorectal fat implies that low rectal cancer more easily invades the surrounding structures Tx; Neoadjuvant chemo-radiation

Extramesorectal nodes are important, because they can be a cause of local recurrence.When they are detected by MR, the radiation and surgical planning has to be adapted.

RECAP

INITIAL MRI: Location :low, mid or high rectum (Distance from the anorectal
junction ) Circular or semi-circular within the wall Length of the tumor
T-stage:T1 / T2: tumor limited to the bowel wallT3: perirectal fat invasion. mesorectal fascia involvement
(tumor/nodes<2 mm)T4: invasion of surrounding structures.
N-stage: # of nodes inside & outside mesorectum .

B. RESTAGING AFTER NEOADJUVANT TREATMENT Restaging is done in the same way as the
primary staging, except that the prefix y is added to the stage.For instance YT3 means, that the patient neoadjuvant therapy and there is remaining tumor with depositis in the mesorectum.

REFERENCES: Recurrence and survival after total mesorectal excision for rectal cancer.
Heald RJ, Ryall RD. Lancet 1986; 1:1479- 1482.
The mesorectum in rectal cancer surgery: the clue to pelvic recurrence?by R. J. Heald, E. M. Husband, R. D. H. RyallBritish Journal of Surgery Volume 69, Issue 10, pages 613-616, October 1982
Surgical management of locally recurrent rectal cancer.by Sagar PM, Pemberton JH Br J Surg 83:293-304, 1996
Rectal Cancer: Review with Emphasis on MR Imagingby Regina Beets-Tan and Geerard BeetsAugust 2004 Radiology, 232, 335-346.
Accuracy of magnetic resonance imaging in prediction of tumour-free resection margin in rectal cancer surgery.by Beets-Tan RG, Beets GL, Vliegen RF, et al Lancet 357:497-504, 2001
Rectal Cancer: Local Staging and Assessment of Lymph Node Involvement with Endoluminal US, CT, and MR Imaging; A Meta-Analysisby Bipat S, Glas AS, Slors FJ, Zwinderman AH, Bossuyt PM, Stoker J Radiology 232:773-783, 2004

Morphologic Predictors of Lymph Node Status in Rectal Cancer with Use of High-Spatial-Resolution MR Imaging with Histopathologic ComparisonBrown G, Richards CJ, Bourne MW, et al Radiology 227:371-377, 2003
High-resolution MR imaging for nodal staging in rectal cancer: are there any criteria in addition to the size?by Kim JH, Beets GL, Kim MJ, Kessels AG, Beets- Tan RG. Eur J Radiol 2004; 52:78-83
A Systematic Approach to the Interpretation of Preoperative Staging MRI for Rectal Cancerby Fiona Taylor et alAJR 2008; 191:1827-1835
Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer.by Kapiteijn E, Marijnen CA, Nagtegaal ID, et alN Engl J Med 2001; 345:638-646
Patterns of neoplastic foci and lymph node micrometastasis within the mesorectum (pdf)Wang C, Zhou Z, Wang Z, et al Langenbecks Arch Surg. 2005;390:311;318
Wait-and-see policy for clinical complete responders after chemoradiation for rectal cancer.by Maas M
J Clin Oncol. 2011 Dec 10;29(35):4633-40
WWW. Radiology assisstaant
THANK YOU!





























