Embed Size (px)
Citation preview

RECTAL PROLAPSE

Prolapse of the rectum mainly two types:
Partial or incomplete prolapse (procidentia) when the mucous membrane lining the anal canal protrudes through
the anus only. Complete prolapse in which the whole
thickness of the bowel protudes through the anus.
Rectal prolapse occurs most often at extremes of life e.g, in children between 1-5 years of age and elderly people. More common in female than male.
Prolapse of the rectum mainly two types:
Partial or incomplete prolapse (procidentia) when the mucous membrane lining the anal canal protrudes through
the anus only. Complete prolapse in which the whole
thickness of the bowel protudes through the anus.
Rectal prolapse occurs most often at extremes of life e.g, in children between 1-5 years of age and elderly people. More common in female than male.
Rectal Prolapse: Rectal Prolapse:

Aetiologythe predisposing causes are:-
The vertical straight course of the rectum.
Reduction of supporting fat in the ischiorectal fossa.
Straining at stool. Chronic cough.
the predisposing causes are:-
The vertical straight course of the rectum.
Reduction of supporting fat in the ischiorectal fossa.
Straining at stool. Chronic cough.
In children:

the predisposing causes depend on type of the prolapse.
Advance degree of prolapsing piles.
Loss of sphincteric tone. Straining from urethral
obstruction. Operations for fistula.
is generally regarded as sliding hernia of the recto vesical or recto vaginal pouch due to stretching of the levator from pregnancy, obesity.
the predisposing causes depend on type of the prolapse.
Advance degree of prolapsing piles.
Loss of sphincteric tone. Straining from urethral
obstruction. Operations for fistula.
is generally regarded as sliding hernia of the recto vesical or recto vaginal pouch due to stretching of the levator from pregnancy, obesity.
In adult:
Partial prolapse
Complete prolapse
Prolapse is first noted during defaecation.
Discomfort during defaecation.
Bleeding.
Mucous discharge.
Bowel habit irregular and may lead to incontinence.
Prolapse is first noted during defaecation.
Discomfort during defaecation.
Bleeding.
Mucous discharge.
Bowel habit irregular and may lead to incontinence.

Examining for rectal prolapse
Most NOT evident in lying position as rest Ask patient to bear down – most still not
evident Need to examine after straining on the
toilet for 1-2 minutes – lean forward – observe from behind – estimate in centimetres - ? full thickness circumferential, or partial mucosal only?

Examining for rectal prolapse

Ano-rectal digital examination
Resting tone (low = IAS problem) Squeeze pressure (low = EAS problem) Co-ordination Sensation (? Neurological dysfunction) Assessment stops here for MOST patients

Radiologic examination

Irreducibility (table sugar!)
Infection Ulceration Severe haemorrhage from
one of the mucosal vein Thrombosis and obstruction of the venous returns leading to
oedema Irreducibility and gangrene
Irreducibility (table sugar!)
Infection Ulceration Severe haemorrhage from
one of the mucosal vein Thrombosis and obstruction of the venous returns leading to
oedema Irreducibility and gangrene
Complications of rectal prolapse:

the prolapse tends to disappear spontaneously by the age of 5 years. So conservative
measures are sufficient.
Conservative treatment: constipation and straining at stool are
avoided and the buttocks may be strapped together to discourage
prolapse during defaecation.
Perirectal injection of alcohol/phenol may be used to fix the lax mucosa to
underlying tissue.
the prolapse tends to disappear spontaneously by the age of 5 years. So conservative
measures are sufficient.
Conservative treatment: constipation and straining at stool are
avoided and the buttocks may be strapped together to discourage
prolapse during defaecation.
Perirectal injection of alcohol/phenol may be used to fix the lax mucosa to
underlying tissue.
Prolapse in children:

Partial prolapse:
Injections of 5% phenol in oil in submucosa. 10-15ml total.
Electrical stimulation with sphincteric exercises.
Injections of 5% phenol in oil in submucosa. 10-15ml total.
Electrical stimulation with sphincteric exercises.

Surgery always necessary, none are ideal.
Thiersch’s operation
Rectopexy Rectosigmoidectomy Ivalon sponge rectopexy Ripstein operation Low anterior resection (minor)
Surgery always necessary, none are ideal.
Thiersch’s operation
Rectopexy Rectosigmoidectomy Ivalon sponge rectopexy Ripstein operation Low anterior resection (minor)
Complete prolapse:

Rectal cancerRectal cancer

2005 Estimated US Cancer Deaths*
15% Breast
10% Colon and rectum
6% Ovary
6% Pancreas
4% Leukemia
3% Non-Hodgkin lymphoma
3% Uterine corpus
2% Multiple myeloma
2% Brain/ONS
22% All other sites
27% Lung and bronchus
Lung and bronchus 31%
Prostate 10%
Colon and rectum 10%
Pancreas 5%
Leukemia 4%
Esophagus 4%
Liver and intrahepatic 3%bile duct
Non-Hodgkin 3% Lymphoma
Urinary bladder 3%
Kidney 3%
All other sites 24%

Decreasing mortality of CRC
5-year Survival
1960-70 1980-90
Colon cancer 40-45% 60%
Rectal cancer 35-40% 58%


Anatomic Location of CRC
Cecum 14 %
Ascending colon 10 % Transverse colon 12 %
Descending colon 7 %
Sigmoid colon 25 %
Rectosigmoid junct.9 %
Rectum 23 %
70%

Epidemiology
Increasing Incidence of CRC
Incidence 30-40 / 100000 / year
>70 y. of age 300 / 100000 / year
third most common malignant disease
second most common cause of cancer death

Epidemiology
70% of CRC are resectable at diagnosis
Mortality has decreased

Ethiology
Diet: fibers, vit E, vit C Polips (adenomatous) IBD – more then 10 years of progression Smoking Cyclooxigenase inhibitors Genetic cancer

WHO Classification of CRC
Adenocarcinoma in situ / severe dysplasia Adenocarcinoma Mucinous (colloid) adenocarcinoma (>50%
mucinous) Signet ring cell carcinoma (>50% signet ring cells) Squamous cell (epidermoid) carcinoma Adenosquamous carcinoma Small-cell (oat cell) carcinoma Medullary carcinoma Undifferentiated Carcinoma

Bleeding per anumSensation of incomplete bladder emptingTenesmusAbdominal painPalpable rectal tumor
Pacienţi în stadii avansate: pierdere ponderală, hepatomegalie, icter, anemie.
Examenul fizic include: aprecierea stării generale, a prezenţei adenopatiilor periferice şi a hepatomegaliei.
!!!!!! RECTAL EXAMINATION RECTAL EXAMINATION
SymptomsSymptoms SymptomsSymptoms

InvestigationsInvestigationsInvestigationsInvestigations
StagingStaging::
- - Recto- Recto- and colonoscopy and colonoscopy
- - Barium enemaBarium enema
- CT - CT
- - MRIMRI - - EUSEUS
StagingStaging::
- - Recto- Recto- and colonoscopy and colonoscopy
- - Barium enemaBarium enema
- CT - CT
- - MRIMRI - - EUSEUS

RECTOSCOPY COLONOSCOPY + BIOPSY
Indications
- Suggestive images on barium enema
- Suggestive symptoms of colonic cancer
- Screening
-After polipectomy

COMPUTER-TOMOGRAFIA(aspecte CR)
COMPUTER-TOMOGRAFIA(aspecte CR)

EUSEUS
Accuracy 81-93%
More difficult to interpret
Limited value in evaluation of LN invasion
Requires contact with tumor and a lumen in which to be inserted.

MRI – standard of care

Tumor markers
CEA CA 19-9
– Dynamic may be significant for recurrence

TNM Primary Lymph-node Distant Dukesstage tumor metastasis metastasis stage
Stage 0 Tis N0 M0 A A
Stage I T1 N0 M0 A A1
T2 N0 M0 A B1
Stage II T3 N0 M0 B B2
T4 N0 M0 B B2
Stage III
A any T N1 M0 C C1/C2
B any T N2, N3 M0 C C1/C2
Stage IV any T any N M1 D D
Astler-Collermodified
Dukes stage
Clinical Staging of CRC

TisTis TT11 TT22 TT33 T T44
ExtensionExtensionto an adjacentto an adjacent
organorgan
MucosaMucosaMuscularis mucosaeMuscularis mucosae
SubmucosaSubmucosa
Muscularis propriaMuscularis propria
SubserosaSubserosa
SerosaSerosa
TNM Classification

Stage and Prognosis
Stage 5-year Survival (%)
0,1 Tis,T1;No;Mo > 90I T2;No;Mo 80-85II T3-4;No;Mo 70-75
III T2;N1-3;Mo 70-75III T3;N1-3;Mo 50-65
III T4;N1-2;Mo 25-45IV M1 <3

Purpose of Radio(chemo)therapy in
Rectal Cancer
To lower local failure rates and improve survival in resectable cancers
to allow surgery in primarly inextirpable
cancers
to facilitate a sphincter-preserving procedure
to cure patients without surgery: very small
cancer or very high surgical risk

Rectal Cancer Surgery is the mainstay of treatment of
RC After surgical resection, local failure is
common Local recurrence after conventional
surgery:– 15%-45% (average of 28%)
Radiotherapy significantly reduces the number of local recurrences

Radiotherapy in the management of RC
– Preoperative RT (30+Gy): 57% relative reduction of local failure
– Postoperative RT (35+Gy): 33% relative reduction

ESMO Recommendations
Resectable cases– Surgical procedure: TME– Preoperative RT: recommended– Postoperative chemoradiotherapy: T3,4
or N+
Non-resectable cases: local recurrences– Preoperative RT with or without CT

Predicting risk of recurrence in RC
Surgery-related
-Low anterior resection
-Excision of the
mesorectum
-Extent of
lymphadenectomy
-postoperative anastomoticleakage
-Tumor perforation
Tumor-related
-Anatomic location
-Histologic type
-Tumor grade
-Pathologic stage
-radial resection margin
-neural, venous, lymphatic invasion

Total Mesorectal Excision (TME)
Local recurrence rates after surgical resection of RC have decreased from about 30% to < 10%
– 1. Radio(chemo)therapy– 2. Importance of circumferential margin
(TME)

Abdomino-perineal resectionMILES
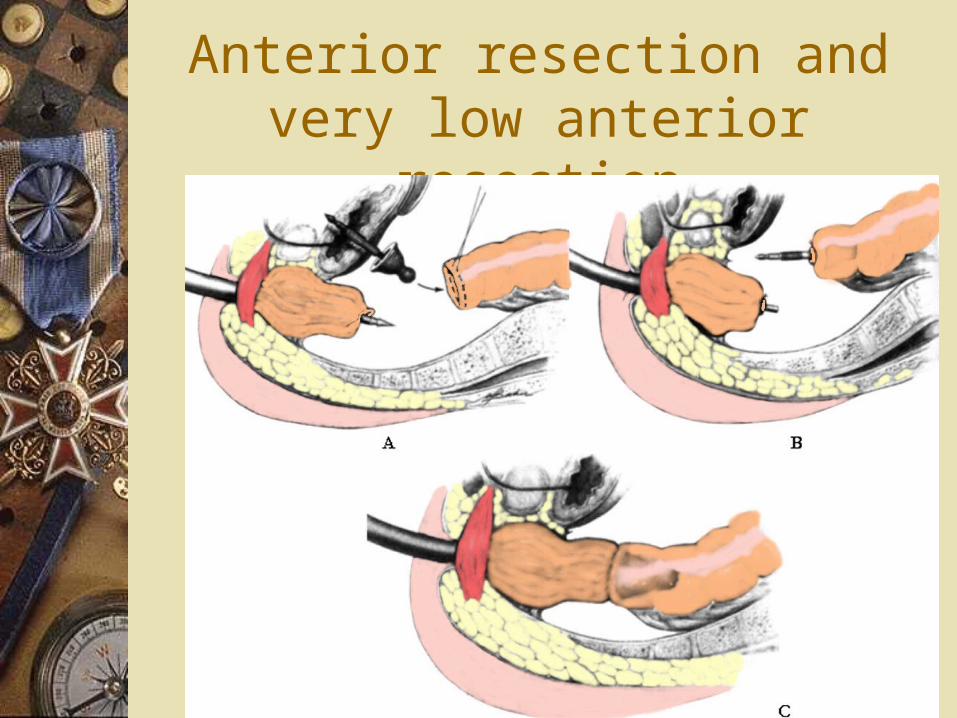
Anterior resection and very low anterior resection

Follow up!!Follow up!!

Epidermoid carcinoma
75% of all malignancies of the area– Early: verucous, nodular lesion– Late: ulcerated, indurated, nodular nmass
Palpable inguinal nodes May invade the rectum: false impression of
rectal carcinoma Lymphatic spread: like rectal + inguinal
nodes

Treatment
External radiation + concomitant chemotherapy
Radical surgery in case of failure

Malignant melanoma
Horrible prognosis Dark mass protruding from the anus 50% pigmented Lymph node MTS early Treatment - not clear advantage of any
alternative

Bowen’s disease:Squamous cell carcinoma in situ Like all other places of skin Plaque-like eczematoid lesion + pruritus Biopsy-carcioma in situ + hyperkeratosis
and giant cells Therapy: local excision with safety
margins

Basal cell carcinoma
Ulcerating tumor (uncommon) “Rodent ulcer” like every other place of
skin exposed Doesn’t spread distantly Local excision

Paget’s disease
Rare condition Pale plaquelike condition with induration +
nodular mass (not always) Nodular mass= coloid carcinoma from
glands or other skin appendages Local excision (without mass) Radical surgery + chemo + RT for coloid
carcinoma


























