Embed Size (px)
Citation preview

Management of Tremor and Spasticity in Multiple Sclerosis
Val StevensonMS Trust Annual Conference Nov 2015

PlanTremorIntroductionAssessment- impact and what type of tremor?Interventions and team management
SpasticityWhat is spasticity?Impact on the person with MSAssessmentInterventions and team managementCase studies

Tremor
3
An involuntary, rhythmic, muscle movement involving oscillations of one or more parts of the body
Common in MS- Charcot triad: tremor, nystagmus, dysarthria
•Prevalence- 25-58*% of people with MS •Titubation (nodding head tremor) ~ 9% of MS clinic patients*•Presence of tremor associated with greater disability*•Median latency from disease onset to tremor~ 11 years*
Cause1)Demyelinating lesions- cerebellar, basal ganglia and connections2)Coincidental
*Alusi SH et al. Tremor in Multiple Sclerosis. JNNP 1999;66:131-134.

Assessment
4
ImpactMeasurement difficult as tremor, ataxia and other impairments co-existImpact on daily activities most important•Washing, dressing•Feeding, drinking•Hand-writing, keyboardQuality of Life
Tremor diagnosisObservation at rest and in posturesIntention movementsAssociated features•Ataxia- eg. past-pointing, dysarthria, nystagmus•Dystonia•Parkinsonism•Family history

Tremor types
5
Intention tremor (cerebellar dysfunction), commonest cause MS Intensified physiological tremor eg hyperthyroidism, drugsEssential tremorParkinson’s diseaseDystonic tremorOrthostatic tremorHolmes (rubral) tremorPsychogenic tremor
Huntington’s DiseaseHemifacial spasmBallismus

MS tremor (intention and/or postural)
6
Clinically- usually arms +? head, neck, trunk, vocal cords
Pathophysiology of tremor in MS is poorly understood
•MS is by definition a multifocal disease; tremor occurrence cannot easily be linked to a single neuroanatomical site •No postmortem studies on the link between lesion site and the tremor have been undertaken•Pontine lesion load correlates with severity of tremor in MS patients

MS tremor- cerebellum and connections
7
• The predominance of action tremors (postural and intention) point to the cerebellum and its connections as the most likely source of tremor
• Bilateral, asymmetrical involvement indicates that damage to the cerebellum and its connections is often multifocal
• Animal studies- damage to cerebellar efferents (through lesions of the dentate nucleus or superior cerebellar peduncle) may cause disinhibition of thalamic nuclei, which are the main producers of intention tremor
• Alterations in sensory inputs- afferents, (from muscle spindles via spinocerebellar pathways) modulate MS tremor
Complex• The cerebellum contributes to various aspects of motor control-
postural stabilization, coordination, precision and timing of movements all of which can be affected

Management
8
Understand and educate
Target;Afferent inputsCerebellumEfferents/ thalamic nuclei
Strategies;Non pharmacological•Lifestyle changes•Positioning and Orthotics•Cooling
Pharmacological
Surgical

Non pharmacological
9
Physiotherapy/ Occupational therapyExercise-based rehabilitation strategies to improve posture and movement controlSeating- proximal support and stabilityRobotics- practising task to correct movements
OrthoticsWriting, feeding aids relying on postural supportWeighted wrist bands, sensory dynamic splintsNeuroprostheses•Devices that deliver electrical stimulation to the antagonist muscles in an out-of phase manner to the EMG signals of the muscles from which tremor originates eg. spoon (handheld device using active cancellation of tremor technology).
Non pharmacological
10
Lifestyle changes•Reduce caffeine intake•Review drugs, other stimulants•Relaxation techniques•Computer adaptations to aid mouse control
Cooling•Cooling affected limb can improve function for ~ 30 mins*•Task directed eg. ISC, PC use, signing documents
Pulsed Electromagnetic Fields•Reported in 3 patients
*Feys P, Helsen W, Liu X, Mooren D, Albrecht H, Nuttin B, Ketelaer P (2005). Effects of peripheral cooling on intention tremor in multiple sclerosis. J Neurol Neurosurg Psychiatry 76:373–379.

Pharmacological
11
Very difficult
•Poor evidence- case reports, small open label trials•Reduction in tremor does not always equate to functional benefit•Side effects common
Be clear with goals of treatment
Essential to monitor effect and review goals

Evidence
Possibly effective (insufficient evidence to confirm or refute)TopiramateRiluzoleRituximab, NatalizumabIsoniazidCarbamazepineGluthetimidePrimidoneSR-FampridineClonazepamGabapentinBotulinum toxin type A
12
Probably ineffective
LevetiracetamPropanololOndansetronCanabinoids
Botulinum Toxin Type A
Two randomized placebo controlled studies reporting benefit•Tremor reduction•Improved writing ability
However•No improvement in QoL•Increased weakness
Alusi SH, Worthington J, Glickman S, Findley LJ, Bain PG. Evaluation of three different ways of
assessing tremor in multiple sclerosis. J Neurol Neurosurg Psychiatry. 2000;68:756–60.
Brin MF, Lyons KE, Doucette J, Adler CH, Caviness JN, Comella CL, et al. A randomized, double
masked, controlled trial of botulinum toxin type A in essential hand tremor. Neurology. 2001;56:1523–8.
13

Surgery- Deep Brain Stimulation (DBS)
Implantation of electrodes bilaterally or Unilaterally into a given nucleusMechanism of action is not clear, possibly through; •Stimulation of neuro- transmitter release•Blockage of local circuits by preventing action potential generation•Stimulation of axonal firing in afferent/efferent axons or fibres of passageHistorically most common target was unilateral or bilateral stimulation of the thalamic nucleus ventralis intermedius (Vim). More recently ventralis oralis posterior (Vop) a basal ganglia outflow nucleus, and zona incerta (ZI), have gained favour.
May help tremor but is not helpful in the management of other components of the MS movement disorder, such as ataxia
14

DBS- Efficacy and side effectsIn mixed population studies DBS less effective in MS than Parkinson’s Disease or Essential TremorMajority do improve (~70% at 1 year), 10% do not•Tremor improvement may not correlate with improved function or QoLSide effects common (25%)•Reported adverse events include seizures, monoparesis, dysarthria, gait disturbance, intracerebral haemorrhage and relapse of MS
Given the risks of surgery, careful patient evaluation and selection is crucial.•Pure tremor•Avoid in patients with severe underlying spasticity or sensory deficits in the tremulous limb, those with a rapidly progressive MS or in people with severe cognitive impairment
15

1)New or worsening tremor- consider steroids, optimise DMD’s ?Nataluzimab2)Maximise physical strategies•Physio•OT•Seating3) If tremor disabling or embarrassing consider oral therapies•Carbamazepine- Primidine- Gabapentin- Topirimate- Clonazepam4) If drugs ineffective consider;•Botulinum toxin•DBS if pure tremor and good cognitive function
16
Pragmatic approach

Spasticity
17
Common feature of MS•84% of 18,727 patients with MS reported at least some symptoms of spasticity, and 30% reported moderate to severe symptoms*
The impact ranges from minor discomfort to complete immobility with pressure sores and contractures•Pain, spasms and sleep disturbance frequently reported•Reduction in quality of life for patients and caregivers
*Rizzo MA, Hadjimichael OC, Preiningerova J and Vollmer TL. Prevalence and treatment of spasticity reported by multiple sclerosis patients. Multiple sclerosis . 2004; 10: 589-95.

Spasticity as part of the upper motor neuron syndrome
Positive Features
SpasticitySpasms - Flexor
- Extensor - Adductor
Increase in tendon reflexesExtensor plantar responses
ClonusPositive support reaction
Negative Features
WeaknessFatigueLoss of Dexterity
- develops over time, not a direct or immediate effect of a pyramidal tract or cortical lesion

Abnormal muscle tone
Descendinginhibition
Ascending sensory
excitation
Descendinginhibition
Ascending sensory
excitation
Normal muscle tone Abnormal muscle tone
•Loss of descending inhibitory input or reduced spinal cord inhibitory control may result in spasticity•Intrinsic changes within the motor neurons causing prolonged plateau potentials•Increased ascending sensory excitation can increase spasticity
Changes in the
motor neuron

Muscle Stiffness
PassiveConnective Tissue
& muscle
Intrinsic
Cross-bridges in active Muscle
ReflexiveNon NeuralNeural
•Exaggerated stretch reflexes•Reduced inhibitory control•Intrinsic changes within the motor neuron•Disinhibited primitive reflexes•Co-contraction
•Loss of sarcomeres•Contracture
•Transition of muscle fibre type•Thixotrophy

But.. spasticity does not But.. spasticity does not occur in isolation occur in isolation
WeaknessLoss of dexterity
Fatigue
Pain
Ataxia
Sensory loss
Bladder and bowel impairment
Cognitive impairment
Non-neural changes- contractures

Impact of spasticity and spasms
Feeding
Sexual activity
Safety
Washing
Dressing
Bladder & Bowel
Mood
Relationships
Posture
Maintains muscle bulk
Likes movement associated with spasms
Uses spasms to assist mobility
Maintains vascular flow, prevent DVT
-ve +ve
Mobility
Transfers
Body Image
Remember spasticity can also be useful..

Accurate assessment is key to everything-Devising management plan and monitoring interventions
Information gathering•Effect of spasticity, spasms on daily activities•Assess patients (and families) expectations
PT appointmentNursing telephone assessment MDT Clinic
Expertise of team- One stop shop’- Sharing and learning for person and team- Good practice for invasive procedures decision making

Consider
• What is the main problem?• Hopes/ expectations• Clarify terminology used• Are there trigger or aggravating factors?• Is pain related to spasticity or other cause?
Neuropathic, musculoskeletal• Is the spasticity helpful for function?• Is it focal or generalised?• What is the individuals level of knowledge about
spasticity?

Assessment- Hands on
• Observe-posture, movement• Feel resistance to passive movement• Determine biomechanical component• Define underlying weakness• Measure; this should be integral to
assessment process• Combination of qualitative and
quantitative measures, individualised
Does the spasticity need treating?

Primary
Options for spasticity management
Ongoing Medical, Therapy & Nursing
Oral
Medication
Intrathecal
Baclofen
Intrathecal
Phenol
Inpatient
Rehabilitation
MILD
SPASTICITY
SEVERE
SPASTICITY
Surgical
Options
Teamwork
Intermediate
Secondary
Focal Treatments

Spasticity management
Oral
Medication
Botulinum
Toxin
Intrathecal
Baclofen
Intrathecal
Phenol
Inpatient
Rehabilitation
Surgical
Options

Individualised treatment plan
Education•What is spasticity?•Contribution of spasticity to current problems/ functionManagement of trigger factors•More education…Physical management programme•Positioning, Seating, Standing, Stretches, StrengtheningPharmacological treatment

Physical intervention
Remove physical trigger factorsDetermine spasticity needed for function and what is notIf needed prevent contracture and overuse of spasticityIf not needed re-educate movement patternsMaximise use of weakened musclesMaintain/improve soft tissue length- splinting, standing, positioning/ posture management

Pharmacological therapies
Generalised Baclofen, Tizanidine, Dantrolene, Benzodiazepines,
Gabapentin, Canabinoids
Focal Botulinum toxin Regional nerve blocks
Intrathecal Baclofen Phenol

Optimisation- Getting the most out of the drugsTiming
Tablets on waking.. Not with breakfast Adjust to activities eg. Car travel, work patterns, therapy, sexual activity
Drug choice Take advantage of other drug actions
Clonazepam and sedation- for nocturnal spasms Gabapentin- for neuropathic pain ? Sativex for pain, bladder dysfunction, poor sleep
Mechanism for monitoring effect and adjusting dose Patient and carer education, treating therapists, GP
Remember- the aim is to improve function and minimise complications, not simply to reduce spasticity

Oral agents for spasticity
Drug Dose Action Half life (hrs) Side effects
Baclofen 5 – 40mg tds GABA - B ~ 4 Sedation weakness
Tizanidine*LFT mon
2 – 12 mg tds α2 adrenergic agonist
2.5 Sedation, dry mouth
hypotension
BZPs Drug dependent GABA - A 18 – 50 Sedationdependence
Dantrolene*LFT mon
25 – 100mg qds Ca2+ release 8 – 9 SedationGI upset
Liver failure
GabapentinPregabalin
100 – 1200mg tds50 – 300 mg bd
VGCCh?GABA
5 – 7 Sedation, poor concentration, unsteadiness

Sativex [Δ9-tetrahydrocannabinol (THC) and cannabidiol (CBD)]
Combination of the cannabis extracts Δ9-tetrahydrocannabinol (THC) and cannabidiol (CBD) Several studies have shown a small benefit or trend in reducing spasticity (50% responder rate)Generally well-tolerated
Side effects (mostly psychotropic effects of cannabis), seem to be dose related Granted UK license in June 2010 as an add on therapy for moderate to severe spasticity in MS

Sativex- Eur J Neurol 18:1122-31, 2011
Enriched study design572 patients underwent 4 week trial272/572 achieved >20% improvement in spasticity NRS ‘responders’241 randomized to double blind placebo controlled 12 week studyResults show significant differences in spasticity NRS, spasm and sleep scoresLarge placebo effect; (74% active cf 51% placebo were responders)

Combining drugs
Start low and go slow
Start first choice drug Increase according to effect or tolerance Stop titration when desired effect achieved or side effects occur
If no effect at full tolerated dose, withdrawAdd in 2nd drug
Repeat process

What if the drugs don’t work?
Review trigger factors and physical management programme before escalating therapy
Other treatment options:Focal treatments
Chemical neurolysis or botulinum toxinIntrathecal baclofenIntrathecal phenolSurgery
Focal intervention- Botulinum toxin
•Focal spasticity•Neural component only - Neuromuscular blockade •Weakens the targeted muscle •Usually muscle power recovers by about 3 months; related to axon sprouting•But period of weakness provides an opportunity for stretching / splinting
*Without therapy input probably pointless..

Concentration of GABA receptors at dorsal horn of laminae 1- 4
Intrathecal infusion is therefore delivered direct to site of action
Who is it for?Severe lower limb spasticityOral medication, therapy and nursing no longer managing spasticity effectivelyResponsive to ITB Realistic, appropriate and achievable goalsIndividual/ Carer agrees with treatment goals and to be responsible for pump follow up
Intrathecal Baclofen

ITB therapy
ITB Therapy provides baclofen continually to the cerebral spinal fluid (CSF), and hence the receptors, via a pump and catheter system
Slide courtesy of Medtronic


Intrathecal dose is approx. 1% of oral equivalent
60,000
600
0
10,000
20,000
30,000
40,000
50,000
60,000
Oral Intrathecal
1.240
0
0.2
0.4
0.6
0.8
1
1.2
1.4
Oral Intrathecal
µg o
f bac
lofe
n
µg p
er m
illili
tre
of C
SF
Daily dose Therapeutic dose
Avoids systemic side effects

Contraindications to ITB therapy
•Known allergy to baclofen (need to have tried it orally prior to ITB)•IV drug user•Concomitant significant sepsis•Chronic pressure sores not a contraindication•Psychological issues•Needle phobia, lack of commitment, body image issues•? Precarious ambulation

Not contraindications…
•Pregnancy or potential pregnancy•MRSA colonisation•Spinal fusion (cervical approach can be used if necessary)•Epilepsy•LP or VP shunts•Malnutrition•Need for MRI scans •Walking!
How is it done?
Aspects of ITB service:•MDT spasticity assessment & measures Patient selection•Trial•Implant•Discharge planning•Long term follow up Pump refill and dose titration 24 hour help-line

Trial procedure
Need ITU/ anaesthetic availabilityContinue normal oral medicationDefine goals of treatment and of trialPerform outcome measures pre and postBolus or continuous infusion LP’s or temporary catheter Children may have GA for catheter placementMonitor vital signs every 30 mins

Pump implant
Pump Pocket:Abdominal Incision usually
Intrathecal Catheter: Lumbar Incision

Ongoing follow up
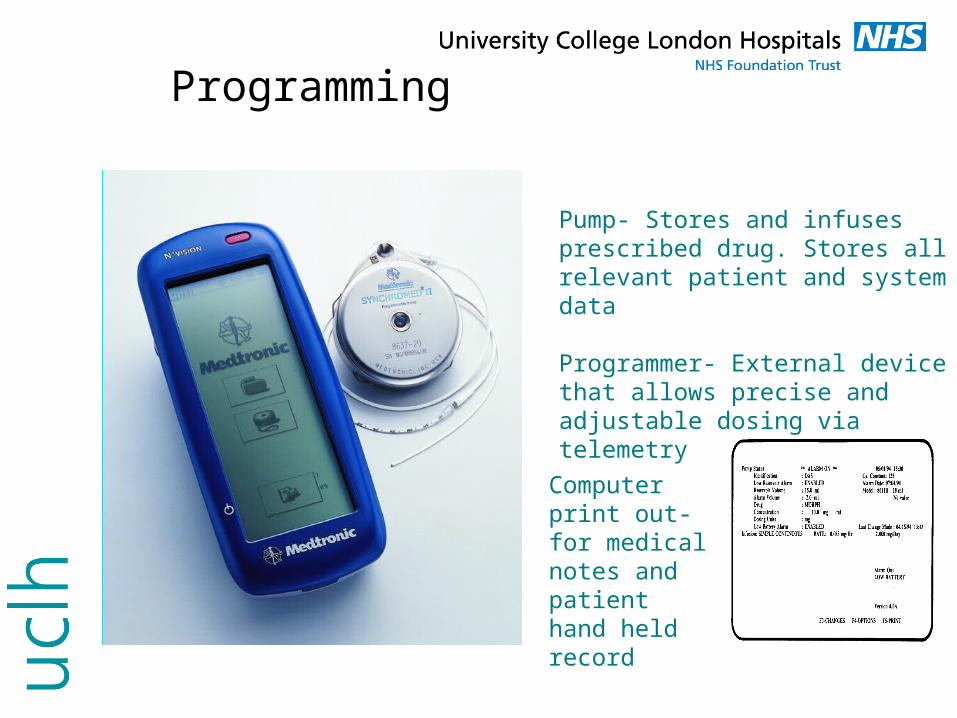
Programming
Computer print out- for medical notes and patient hand held record
Pump- Stores and infuses prescribed drug. Stores all relevant patient and system data
Programmer- External device that allows precise and adjustable dosing via telemetry

Dosing patterns
Time
Increasing dose

Pros and cons of ITB
ProsExtremely effectiveFlexible dosingNo systemic side effects (particularly CNS)Consistent treatmentNo drug interactionsAllows reduction of oral medications
ConsSurgical procedureRisk of complications Catheter issues, infectionPotential risks (can be fatal) Overdosing Withdrawal (missed refill apt)Limited battery lifeMinimal effect on upper limbsMay compromise walkingBody image issues

Case study 1
•59 yr old lady (C), diagnosed with MS in 1986, now Secondary Progressive•Using rollator indoors, scooter outside•Independent personal care, very active•Difficulty doing ISC due to spasticity•Oral meds causing side effects•Poor sleep•Pain and discomfort

Case study 1- Progress
August 2009On Tizanidine 12mg tds, Clonazepam 1mg nocte, Amitriptyline 20mg nocte. Previously tried baclofen (gastric ulcer) and gabapentin (ineffective)Successful ITB trial at 25mcgImplanted (dose on discharge 63mcg/day), Tizanidine stopped and Clonazepam 0.5mcg, Amitriptyline 10mg (to be weaned as outpatient)
Feb 2010- PresentOff all antispasmodics (remains on; trimethoprim, movicol, bladder bot tox)Stable dose of 68.9mcg/day intrathecal baclofen
Flex pattern with higher dose overnight

Outcome measures
Measure Baseline 6 weeks 20 months
Max Ashworth L=3, R=3 L=0, R=0 L=0, R=0
Spasm frequency
L=4, R=4 L=0, R=0Provided used T roll at night
L=0, R=0Very rare spasms reported
10m timed walk Rollator 54.8s, 48 steps
2 sticks 20s, 22 steps1 stick 19.9s, 23 steps
2 sticks 17s, 21 steps
VAS effort of gait
6/10 4/10
VAS satisfaction of gait
8/10

Case study 2
• 49 yr old lady presented in 2003, diagnosed with SPMS in 2005.
• Independent pivot transfers, wheelchair user, standing in OSF, few steps in parallel bars only
• Drowsy on medication• Previous Mitoxantrone, currently Copaxone

Case study 2- progress
• March 2010 on tizanidine 36mg, clonazepam 0.5mg, gabapentin 300mg
• Implanted with ITB pump 100mcg/ day and meds weaned
• May 2010 on 117.7mcg/day ITB and no oral antispasticity drugs. Easier transfers, bed mobility, burst of physio (Aug-Dec 2010).
• Dec 2010 able to walk short distances with rollator• June 2011- 15m tolerance with 2 crutches• Sept 2011 Walking 60m with ease, swimming,
managing stairs• 10m timed walk; 23 steps in 27 seconds with 2 elbow
crutches

Case 2
• In August 2011 she returned home to Canada for a holiday. She walked indoors all the time there as the house was not wheelchair accessible. Improved strength and stamina with this
• When she returned home she put her manual and powered wheelchairs away in the garage. She now only uses these for long distances outdoors.
• She has started swimming once a week. Goes for walks in the park with family, attends a regular exercise group and is considering a return to some sort of voluntary work.
Intrathecal Phenol
• Protein coagulation & necrosis• Axonal degeneration • Indiscriminate destruction of motor and sensory fibres• Irreversible… but may need to be repeated
Service requirements
• Spasticity assessment & measures• Expert injector• Local anaesthetic trial as inpatient• Nursing, physio and wheelchair service follow up

Selection criteria
• Severe lower limb spasticity• Oral medication, physiotherapy, nursing no
longer effective• ITB not appropriate or Phenol preferred• Bladder & bowel dysfunction with effective
management programme in place• Aware of potential sexual dysfunction• Sensory impairment of lower limbs• Patient aware of irreversibility (stem cell
treatment…)

Lumbar spinal anatomy
Cerebrospinal fluid
FrontMotor nerves
Sensory nerves
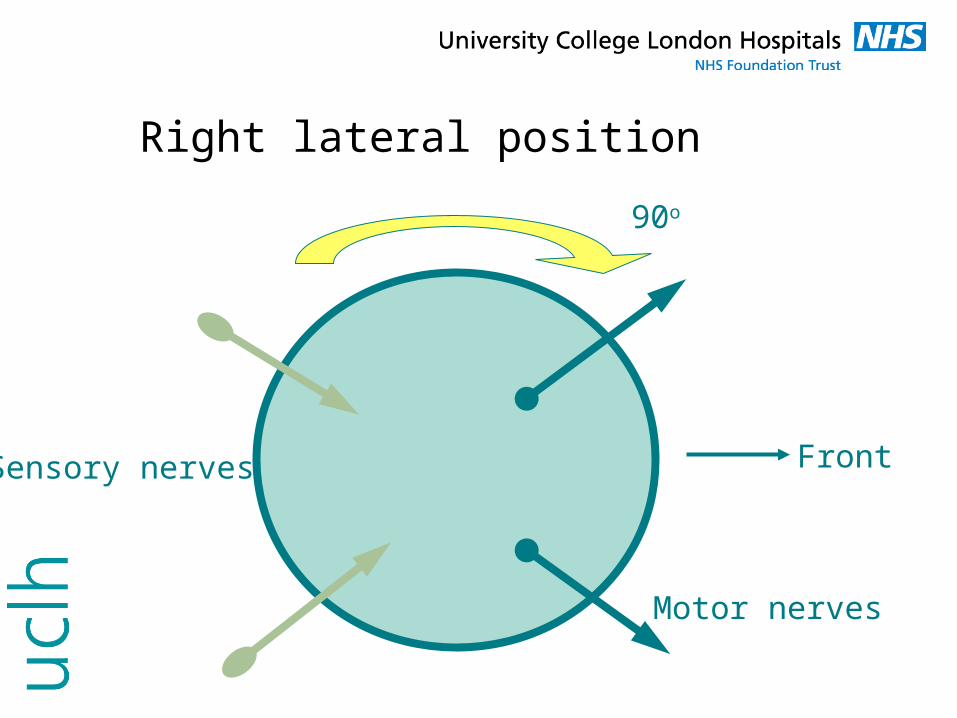
Right lateral position
Front
90o
Motor nerves
Sensory nerves

Lumbar puncture
Front

Modified right lateral position
Front
30o
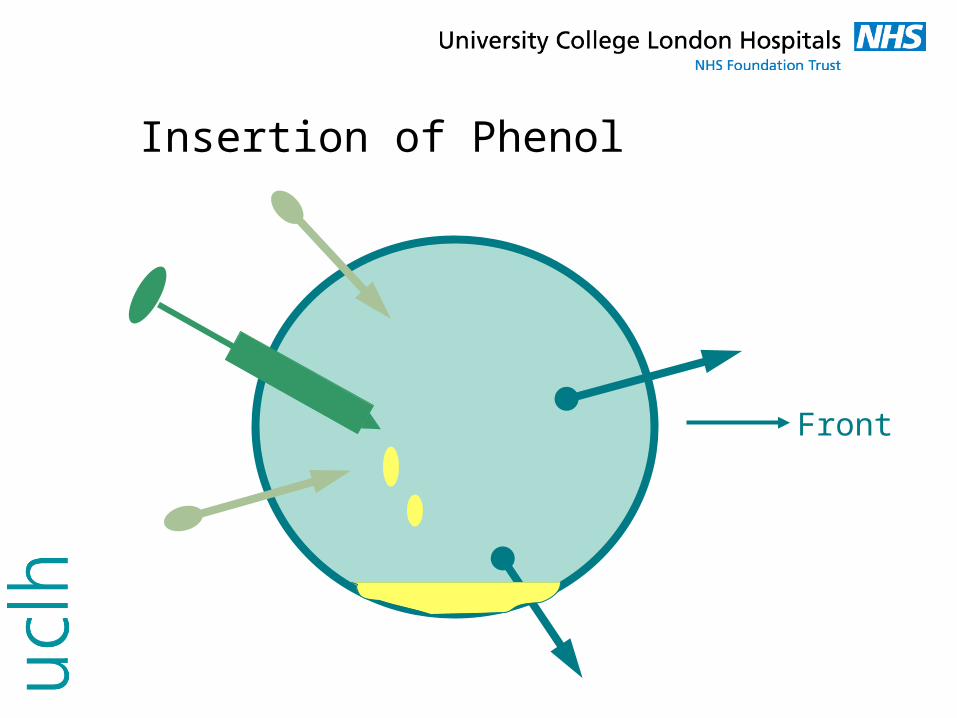
Insertion of Phenol
Front

End result
Damaged motor nerve

Case Study
• 51 year old lady with secondary progressive MS• Essentially bed bound although manages to sit
out about once every few weeks in a customised chair for a short period of time
• Pain is the most troublesome symptom• Unable to change position in the bed and any
care tasks are painful and extremely difficult to perform

Outcome MeasuresOutcome Measures Pre trial AssessmentPre trial Assessment10/ 0910/ 09//20122012
Left RightLeft Right
Post Trial InjectionPost Trial Injection11/09/201211/09/2012
Left RightLeft Right
Post phenol injectionsPost phenol injections14/ 09 /201214/ 09 /2012
Left Right Left Right
Tone (Ashworth)Tone (Ashworth) Hip flexorsHip flexors Knee extensorsKnee extensors Hip extensorsHip extensors Knee flexorsKnee flexors Hip adductorsHip adductors Ankle plantar-flexorsAnkle plantar-flexors
Unable to Unable to formally formally assess due to assess due to lack of passive lack of passive range and range and frequent frequent spasmsspasms
Unable to Unable to formally assess formally assess due to lack of due to lack of passive range passive range and frequent and frequent spasmsspasms
0000000000
0000000000
0000000000
0000000000
Spasms (Frequency scale)Spasms (Frequency scale) 44 44 00 00 00 22
Spasm descriptionSpasm description Flexor, Flexor, adductor and adductor and internal rotatorinternal rotator
Mainly flexor in Mainly flexor in naturenature
No spasms observedNo spasms observed Occasional short lived spasms Occasional short lived spasms affecting the foot onlyaffecting the foot only
Passive range of movement Passive range of movement (Goniometry)(Goniometry)
Hip flex Hip flex –– ext extKnee flex Knee flex –– ext ext
70/60/070/60/0110/75/0110/75/0
110/90/0110/90/0145/100/0145/100/0
105/35/0105/35/0`45/65/0`45/65/0
120/75/0120/75/0145/85/0145/85/0
100/40/0100/40/0145/65/0145/65/0
110/60/0110/60/0145/90/0145/90/0
Numeric Rating ScalesNumeric Rating ScalesVisual Analogue Score (VAS)Visual Analogue Score (VAS) PainPain Comfort Comfort in bedin bed
9966
0000
0000

Acknowledgements
To all of the patients who consented to their photos and videos being used to help with education and training of health professionalsTo you all for listening….
Any questions?






![Spasticity Following Spinal Cord Injury€¦ · Spasticity Following Spinal Cord Injury 1.0 Introduction 1.1 Definition Spasticity is traditionally defined as “[…] a motor disorder](https://img.dokumen.tips/doc/110x75/5f136925b49f3c20e6289c19/spasticity-following-spinal-cord-injury-spasticity-following-spinal-cord-injury.jpg)






















