Embed Size (px)
Citation preview
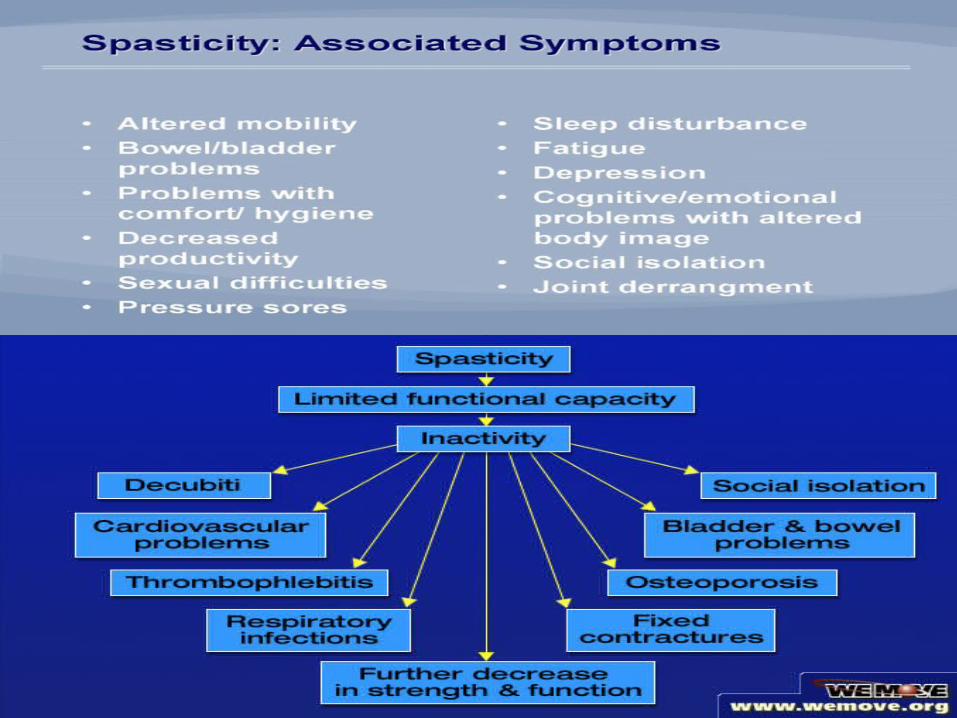
What is Spasticity? Spasticity is a TRIAD of painful mass muscle spasms,
rigid posturing of limbs, and increased reflexes.
Most common definition to be found in literature:It is a motor disorder characterized by a velocity-Dependent increase in tonic stretch reflexes withexaggerated tendon jerks, resulting from hyper excitability of the stretch reflex, as one component of the upper motor neuron syndrome. Lance, 1980
Muscle hypertonia as a result of Exaggerated reflexes

• Reflex in general is a stereotyped movement or response elicited by a standard stimulus
• Stretch Reflex - Is the simplest monosynaptic reflex or the two-neuron reflex, an example of which is the tendon jerk reflex or tendon tap reflex
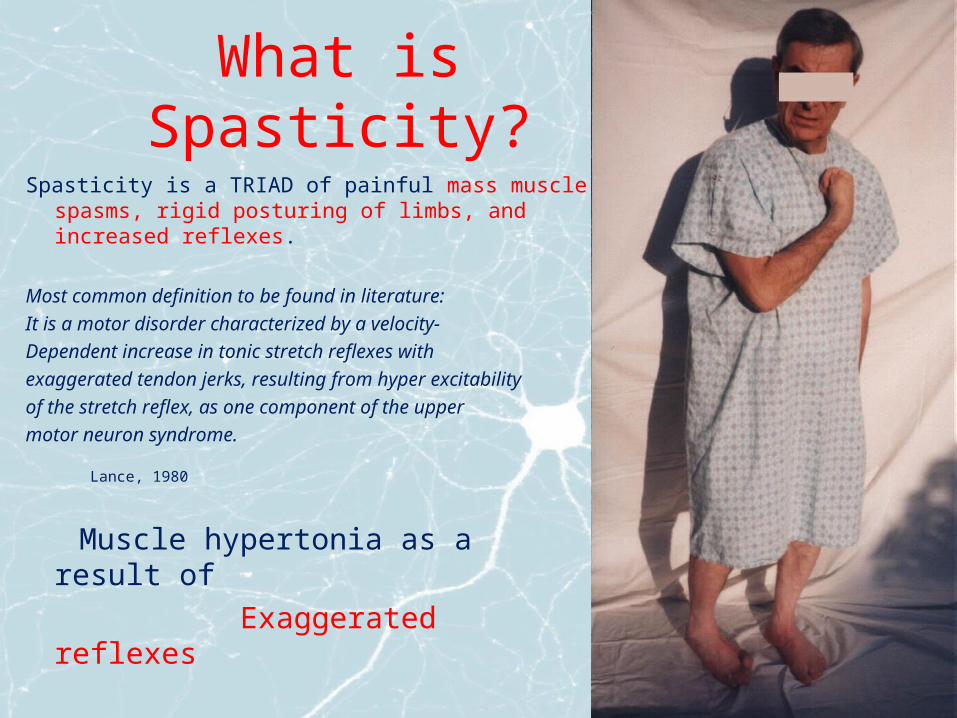
• Skeletal muscles contains specialized proprioceptors called muscle spindles. These receptors sense a change in muscle length and send excitatory impulses to the alpha motor neurons in the spinal cord. Stimulated alpha motor neuron fires back and shortens the muscle thus releasing the tension and signalization from its spindles…
Can It be that simple…?
1. Level of complexity: Inhibitory interneurons mediating reciprocal innervation
Activation of agonists is linked to inhibition and relaxation of antagonists
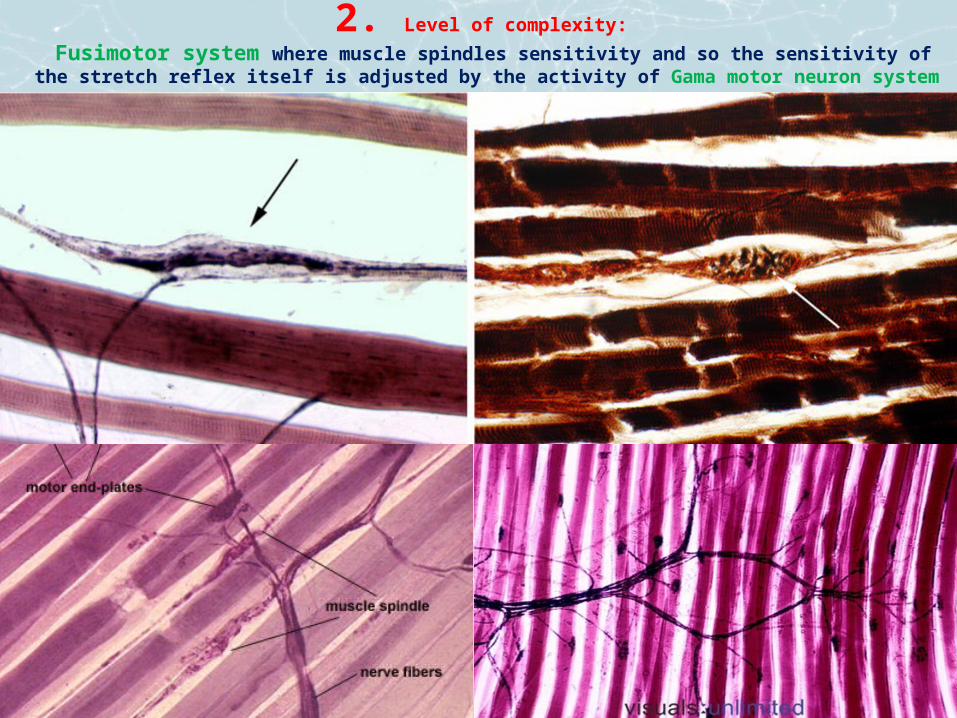
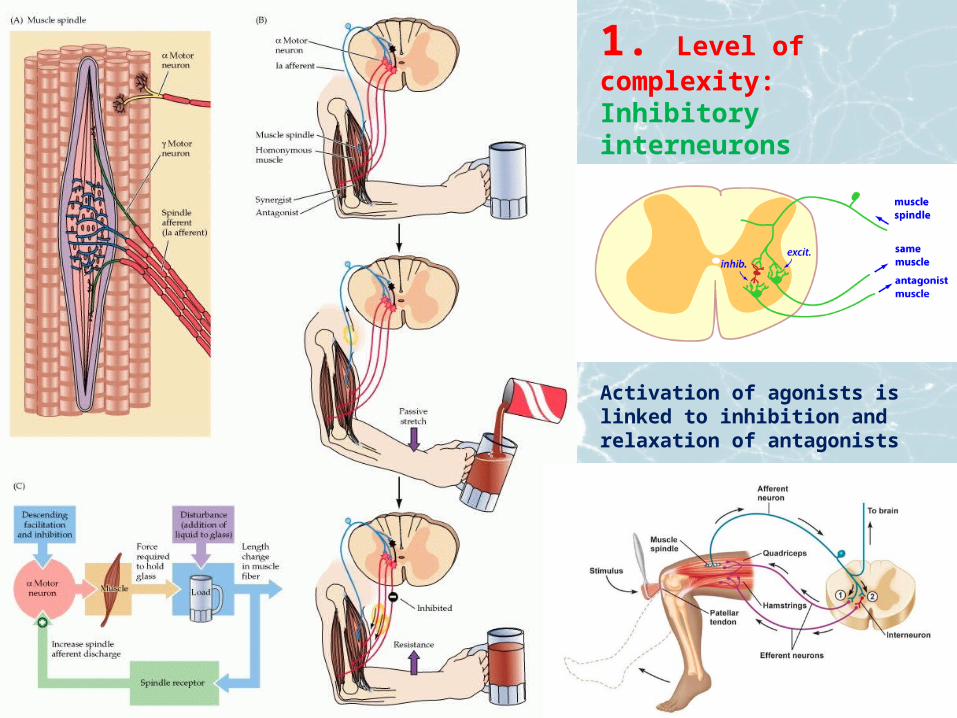
2. Level of complexity: Fusimotor system where muscle spindles sensitivity and so the sensitivity of the stretch reflex itself is adjusted by
the activity of Gama motor neuron system

Gamma-motor neurons regulates the sensitivity of the stretch reflex by adjusting the level of tension in the intrafusal muscle fibers of the muscle spindles. This helps to regulate muscle length and tone. Stimulation of a γ-motor neuron contracts the ends of the intrafusal fibres and consequently stretches the middle part of the muscle spindle. This part of the spindle is innervated by type Ia sensory fiber that go on to synapse with alpha-motoneurons, completing the GAMMA LOOP
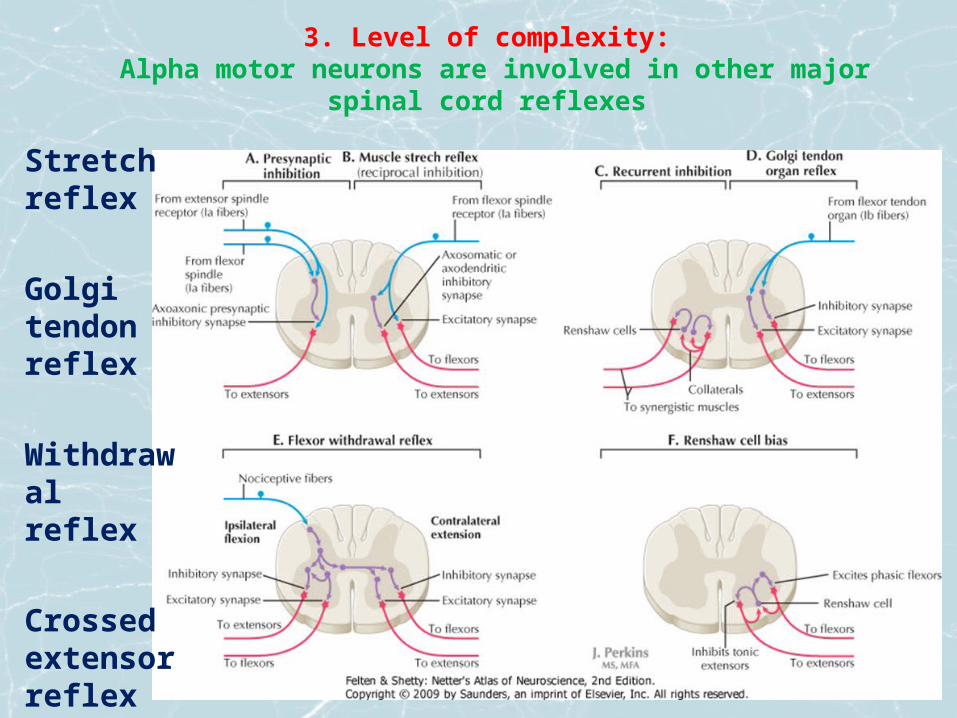
3. Level of complexity: Alpha motor neurons are involved in other major spinal cord reflexes
Stretch reflex
Golgi tendon reflex
Withdrawal reflex
Crossed extensor reflex

4. Level of complexity:Alpha and Gama motor neurons are influenced by sensitive stimulation



5. Level of complexity: Spinal neuronal network is influenced by all higher neural structures involved in the control of movement
Motor CortexPlanning and
Directing voluntary movement
Brainstem CentersBasic movements and
Postural control
BASAL GANGLIAInitiation
Of movement
CEREBELLUMSensory motorcoordination
Local circuit neuronsReflex coordination
Motor neuron poolsLower motor neurons
SKELETAL MUSCLES
Brain stemtracts Coticospinal
tracts
6. Complexity can be beautiful…
7. The structure is all alive• It means
dynamic• Not only moving
but also changing in time
• And some kind of software is running on it…That is changing too

What is Spasticity?• Lance’s definition has been criticized for being too narrow by
describing spasticity as being only a form of reflex hypertonia• But the increase of stretch reflexes is not the only reason of
muscles thightness. It is one of multiple factors on the neural part of the Upper motor neuron syndrome
• The non-neural effects can add significantly to the neural mechanism as the fixed static state of muscles and joints further interferes with modulation of tonus by alteration of the feedback
• Immobilization in spastic position leads to sensory deficits and contributes to development of pain
• The factor of time with structure remodelation is important for the clinical picture and therapy
Other definitions of Spasticity
• Factors which can lead to a mechanical resistance in movement are the reduced elasticity of the tendons and the biomechanical changes of muscle fibers
Dietz 1992• Excessive activation/co contraction: Too many muscles with
inappropriate force Sarmann 1977• Altered sequence of muscle firing Dewald 2001• Loss of central command to generate and sustain force, with no loss of
contractile capacity Sarmann 2002• Delayed initiation and termination of muscle contraction Chae 2002
• Change in muscle function caused by hypertonia resulting from upper motor neuron syndrome and leading to spastic movement disorder
Jiri 2011
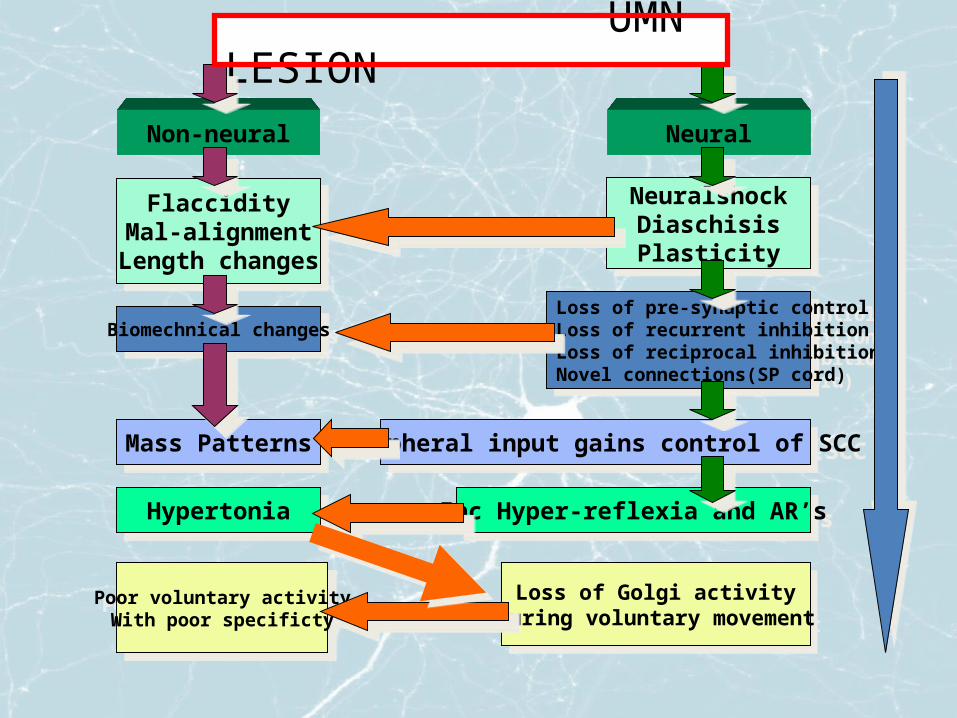
UMN LESION
Non-neural Neural
FlaccidityMal-alignmentLength changes
Biomechnical changes
Mass Patterns
Hypertonia
Poor voluntary activityWith poor specificty
NeuralshockDiaschisisPlasticity
Loss of pre-synaptic controlLoss of recurrent inhibitionLoss of reciprocal inhibitionNovel connections(SP cord)
Peripheral input gains control of SCC
Inc Hyper-reflexia and AR’s
Loss of Golgi activityDuring voluntary movement

Pathophysiology of Impairment After a Central Nervous System Lesion
Gracies et al., 1997

Spastic muscles EMG

So what causes a muscle to become spastic?
• Not completely understood, despite considerable investigation
• Interruption of descending inhibitory pathways or alteration of central inhibitory commands
• Rearrangement of spinal circuitry and changes in the muscle itself occurring with time

Characteristics of SpasticityRather then being a uniform specific symptom it is a part
of upper motor neuron syndrome with: • Hyperactive stretch reflex• Abnormal cutaneous reflexes • Spastic dystonia with imbalance between flexors and extensors leading to
slow effortful movement• Increased resistance to passive movement• Abnormal posturing of extremities leading to muscle shortening• Stereotypical movement synergies and uncoordinated movements• Clonus• Abnormal antagonist contraction during voluntary agonist effort• Extra-segmental co-contraction with abnormal contraction distant from
the muscles involved in a voluntary effort
Leading to SPASTIC MOVEMENT DISORDER

Management of Spasticity
1. Prevention of exacerbating factors:Increased nociceptive input: Infection, Pressure sores, Bladder stones, Urine retention, Fecal impaction, Injuries, Soft tissue stretch by wrong position or forced movement, Fatigue and stressMedication
2. Physiotherapy: Intelligent cooperation with organism adaptation and self repairing ability

3. Pharmacological Intervention:• Generalized Spasticity: Oral Agents – Baclofen– Dantrolene Sodium – Tizanide Hydrochloride
Side effects limiting dosage
• Regional Spasticity: Intrathecal Baclofen
• Focal Spasticity: Botulinum Toxin injection

4. Surgical Intervention
Neurosurgery
Dorsal rhizotomiesPeripheral neurotomies
Orthopedic surgery
Tendon LengtheningTendon Transfer Osteotomy - for skeletal deformityArthrodesis - joint fusion
Despite all therapeutic options our effort only rarely meets full success…