Embed Size (px)
Citation preview

NON INFECTIOUS CONJUNCTIVITIS & XEROPHTHALMIA
DR.S.VENI PRIYA

Revision Acute conjunctivitis – bacterial, viral ,
ophthalmia neonatorum Chronic – trachoma

Plan of the class Allergic conjunctivitis Immune mediated conjunctivitis – phlycten Xerophthalmia

ALLERGIC CONJUNCTIVITIS Acute allergic rhino conjunctivitis
Vernal kerato conjunctivitis
Atopic kerato conjunctivitis
Giant papillary conjunctivitis

Allergic conjunctivitis IgE mediated hypersensitivity reaction on
exposure to environmental allergens ALLERGENS : pollen ,dust, bacterial
antigens, cosmetics, animal , birds , etc


Clinical features SYMPTOMS Itching , itching, itching Mild redness Mucoid discharge ( ROPY DISCHARGE)

CLINICAL FEATURES - SIGNS CONJ- papillae Chemosis Mild redness

Complications CORNEAL INVOLVEMENT – shield ulcer ,
keratoconus DRY EYES

MANAGEMENTGENERAL MEASURES Avoid exposure to allergens -
DARK GOGGLES Cold compress Not to rub the eyes

TREATMENT To control the present attack Topical steroids - FML , loteprednal Topical antihistamine – CPM, epinastineTo prevent further attacks Mast cell stabilizers – sodium
cromoglycate, olopatidine

ACUTE ALLERGIC RHINO CONJUNCTIVITIS SEASONAL
ALLERGIC CONJUNCTIVITIS
Spring & summer
Commonest form
Tree and grass pollen
PERENNIAL ALLERGIC CONJUNCTIVITIS
↑ Autumn
Milder & less common
House dust mites, animal dander & fungal allergen

ACUTE ALLERGIC RHINO CONJUNCTIVITIS TREATMENT Mast cell stabilisers –
sodium cromoglycate q.i.d
Antihistamines
Combined therapy
Steroids – rarely indicated

VERNAL CONJUNCTIVITIS VERNAL KERATOCONJUNCTIVITIS SPRING CATARRH
Bilateral recurrent allergic conjunctivitis Ig E & cell mediated immune
mechanisms

VERNAL KERATOCONJUNCTIVITIS RISK FACTORS Boys ≥ girls , mean age – 7 yrs
Family history of atopy
Peak incidence in spring & summer

SYMPTOMS ITCHING ROPY DISCHARGE Frequent blinking

VKC – SIGNS Palpebral
Upper tarsal conjunctiva Cornea
Limbal
Mixed

VERNAL KERATOCONJUNCTIVITIS
DIFFUSE PAPILLARY HYPERTROPY OF UPPER TARSUS
MACROPAILLAE / COBBLE STONES - ≥ 1MM
PALPEBRAL FORM

VERNAL KERATOCONJUNCTIVITIS
COBBLE STONE APPEARANCE

VERNAL KERATOCONJUNCTIVITISLIMBAL FORM
Limbal papillae
White spots at
apices – Horner Trantas dots
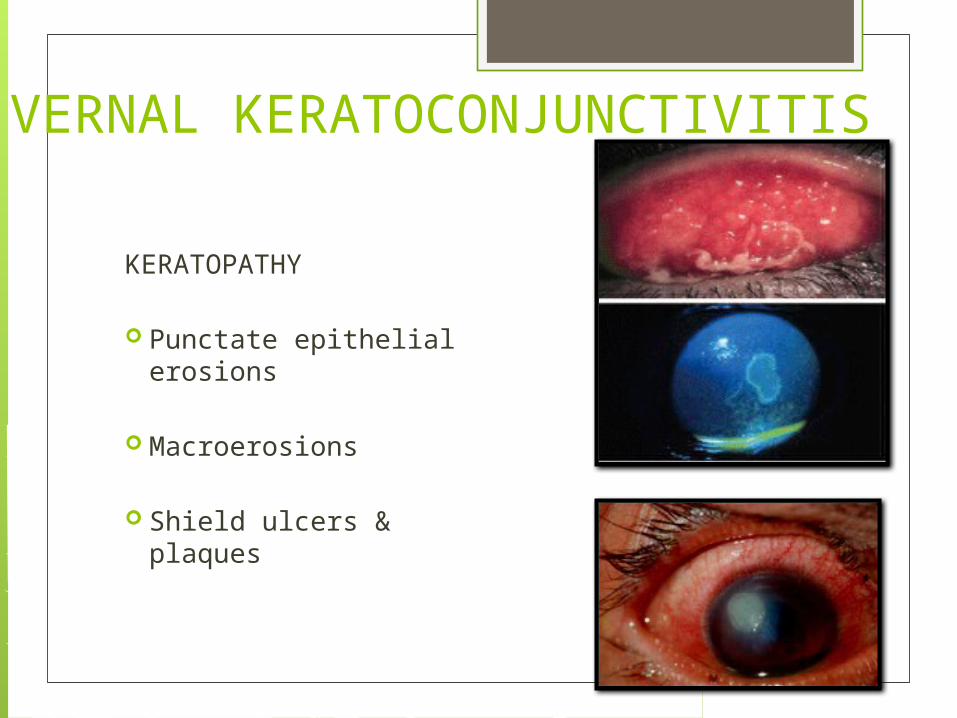
VERNAL KERATOCONJUNCTIVITIS
KERATOPATHY Punctate epithelial
erosions
Macroerosions
Shield ulcers & plaques

VERNAL KERATOCONJUNCTIVITIS
KERATOPATHY Pseudogerontoxon –
resembles arcus senilis
Peripheral superficial vascularisation
HSV keratitis & keratoconus

VERNAL KERATOCONJUNCTIVITISTREATMENT TOPICAL Mast cell stabilisers - ↓ need for steroids
Antihistamines
Steroids – mainstay Fluromethalone 0.1 %
Cyclosporin – qid in steroid resistant cases
MUST KNOW Other names IgE mediated & cell mediated allergic Itching & ROPY DISCHARGE Papillae – COBBLE STONE APPEARANCE limbus – HORNER TRANTA’S SPOT TREATMENT – antihistamine steroid mast cell stabilizer

ATOPIC KERATOCONJUNCTIVITIS Associated with atopic dermatitis , asthma,
allergic rhinitis . Chronic, unremitting , extremely severe form
of allergic conjunctivitis → significant visual morbidity

GIANT PAPILLARY CONJUNCTIVITIS
Giant papilla- > 1 mm Soft CL wear, ocular prosthesis , exposed
sutures, filtering blebs FB sensation , redness, itching, CL intolerance TREATMENT: Remove the cause Lubricating eye drops Same as allergic conjunctivitis


ASSIGNMENT ocular side effects of using steroids (topical /
systemic) Name four ocular diseases in which steroids
are used for treatment

Immune mediated -PHYLCTENULAR CONJUNCTIVITIS Hypersensitivity reaction to endogenous
bacterial protein (tuberculosis, adenoiditis/tonsillitis)
TYPES : Conjunctival Limbal Corneal


CLINICAL FEATURES SYMPTOMS : Mild irritation Redness SIGNS : SMALL NODULE necrosis ulcer

TREATMENT Short course of topical steroids

XEROPHTHALMIA

XEROPHTHALMIA Spectrum of ocular disease ranging caused
by vitamin A deficiency. Nutritional blindness CAUSES: malnutrition, malabsorption,
chronic alcoholics, diseases which precipitate malnutrition like measles, malaria, diarrhoea , acute illness in children.

HOW ? VITAMIN A is essential for the synthesis of
retinal photo pigments & conjunctival glycoproteins.
RHODOPSIN Visual cycle delayed dark adaptation / Night Blindness
Conjunctival epithelial dysfunction ocular surface dryness

XEROPHTHALMIA

XEROPHTHALMIA XN: NIGHT BLINDNESS EARLIEST SYMPTOM responds rapidly to vitamin A therapy [ within
24-48 hours]

CONJUNCTIVAL XEROSIS X1 A : - the conjunctival epithelium undergoes
KERATANISING METAPLASIA. i.e. the normal columnar epithelium is transformed into stratified squamous epithelium. Goblet cells will be lost & keratinization occurs.
- conjunctival xerosis – starts at the temporal side

CONJUNCTIVAL XEROSIS
BITOT’S SPOT- keratin + saprophytic bacilli
[ CORYNEBACTERIUM XEROSIS] accumulate on the xerotic surface FOAMY APPEARANCE== BITOT’S SPOT
- Begin to resolve within 2-5 days & disappear by 2 weeks of treatment
-In Chronic cases, the spots will not disappear

BITOT’S SPOT

CORNEAL XEROSIS – X2 Lustreless dry appearance , in the inferior
limbus Responds within 2-5 days, disappear within 2
weeks of treatment

CORNEAL XEROSIS
X3A & X3B : KERATOMALACIA
COLLIQUATIVE NECROSIS/ LIQUAFACTIVE NECROSIS sterile corneal melting
Round or oval punched out ulcers involving the inferonasal quadrant
Perforation adherent leucoma, anterior staphyloma, phthisis bulbi

KERATOMALACIA

XEROPHTHALMIA- XS &XF XS: CORNEAL SCARRING -Nebula, macula , leucoma XF: XEROPHTHALMIC FUNDUS
/UYEMURA’S FUNDUS -Small white lesions in the retina

XEROPHTHALMIC FUNDUS
TREATMENT - MEDICAL EMERGENCY
VITAMIN A: ( 3 DOSES) 2 LAKH I.U - ORALLY OR 1 LAKH I.U – I.M 1ST DAY, 2ND DAY & WITHIN 1-4 WEEKS CHILDREN BETWEEN 6-11 MONTHS: HALF
THE DOSE CHIDREN < 6 MONTHS : QUARTER THE
DOSE

TREATMENTOCULAR LESIONS: Lubricants Broadspectrum antibiotics Cycloplegics FORTIFIED DIET

QUESTIONS VKC / SPRING CATARRAH XEROPHTHALMIA
Causes of night blindness Treatment of xerophthalmia Treatment of allergic conjunctivitis What is Bitot’s spot ? Difference between papillae & follicle.

24.2.16 - symposium Causes of Limbal nodule Acute red eye – enumerate the causes. How
to differentiate between them. Ophthalmia neonatorum Trachoma – clinical features & management

Thank u





























