Embed Size (px)
Citation preview

Frederik Meijer
Heart & Vascular Institute

Frederik Meijer Heart & Vascular Institute
Cardiogenic Shock
for the Intensivist
Michael Dickinson, MD, FACC, FHFSA
Section Chief, Advanced Heart Failure
Medical Director for Heart Failure and Heart Transplant
Richard DeVos Heart & Lung Transplant Program
Frederik Meijer Heart & Vascular Institute
Spectrum Health
Frederik Meijer Heart & Vascular Institute
Disclosures
None relevant to this presentation.
3

Frederik Meijer Heart & Vascular Institute
Presented to rural ER with chest
pain
Suffered VF arrest in the ER x 2
Resuscitated back to a pulse
after 15 minutes of CPR.
Intubated, on ventilator and
neurologic status unclear.
Cooling protocol initiated and
transferred to the Meijer Heart
Center for cardiac cath.
51 yr old man with chest pain
LAD was then stented.

Frederik Meijer Heart & Vascular Institute
Cardiac Catheterization – acute stent thrombosis
• Recurrent VF
arrests and
hypoperfusion
despite very high
dose pressor and
inotrope doses.
• Maximal medical
support but the
odds of survival
were now very
low.
Frederik Meijer Heart & Vascular Institute
Shock Team activation

Frederik Meijer Heart & Vascular Institute
Clinical Course
Cooling protocol performed.
Clinical condition worsened.
Artificial lung added onto circuit
(ECMO)

Frederik Meijer Heart & Vascular Institute
Clinical Course
Cooling protocol performed.
Clinical condition worsened.
Artificial lung added onto circuit.
After 4 days was weaned from
artificial lung and then off
tandem heart.
■ Cardiac function normalized.
■ Neurologic function normalized.
■ He is fully functional now.
■ He works full time and supports his
family.

Frederik Meijer Heart & Vascular Institute
What is “a changin”?
Acute mechanical circulatory support (ECMO, Impella, etc…)
Failure to rescue
Recognize and treat the variable hemodynamics
9

Frederik Meijer Heart & Vascular Institute
38 year old man admitted for heart failure. Known NIDCM
5 pm: Routine
admission orders. Lasix
40 mg IV.
2 am: BP low. RN calls
PA. IVF bolus given.
2:20 am: Dyspneic,
hypoxemic, hypotension (Dopamine)
3:15 am: Cardiac
arrest and died.
10

Frederik Meijer Heart & Vascular Institute
38 year old man admitted for heart failure. Known NIDCM
5 pm: Routine
admission orders. Lasix
40 mg IV.
2 am: BP low. RN calls
PA. IVF bolus given.
2:20 am: Dyspneic,
hypoxemic, hypotension (Dopamine)
3:15 am: Cardiac
arrest and died.
11

Frederik Meijer Heart & Vascular Institute
What causes failure to rescue?
Not detected
Not recognized
Not acted upon
Not escalated
12
When patient instability / decline / failure is:

Frederik Meijer Heart & Vascular Institute
Hospital Mortality Heart Failure Admissions @ SH
2.80%4.40% 5.20%
8.20%
15.60%17.40%
26.70%
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
Nesiritide Nes + Ntg Nitroglycerin Dobutamine Nes + Mil Milrinone Nes + Dob

Frederik Meijer Heart & Vascular Institute
What does this data tell us?
• If a clinician feels the
need to use inotropes
that patient has just
become high risk
(>8% in hospital
mortality).
• Once you use more
than one vasoactive
your patient has
become very high risk.
2.80%4.40% 5.20%
8.20%
15.60%17.40%
26.70%
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
Nesiritide Nes + Ntg Nitroglycerin Dobutamine Nes + Mil Milrinone Nes + Dob

Frederik Meijer Heart & Vascular Institute
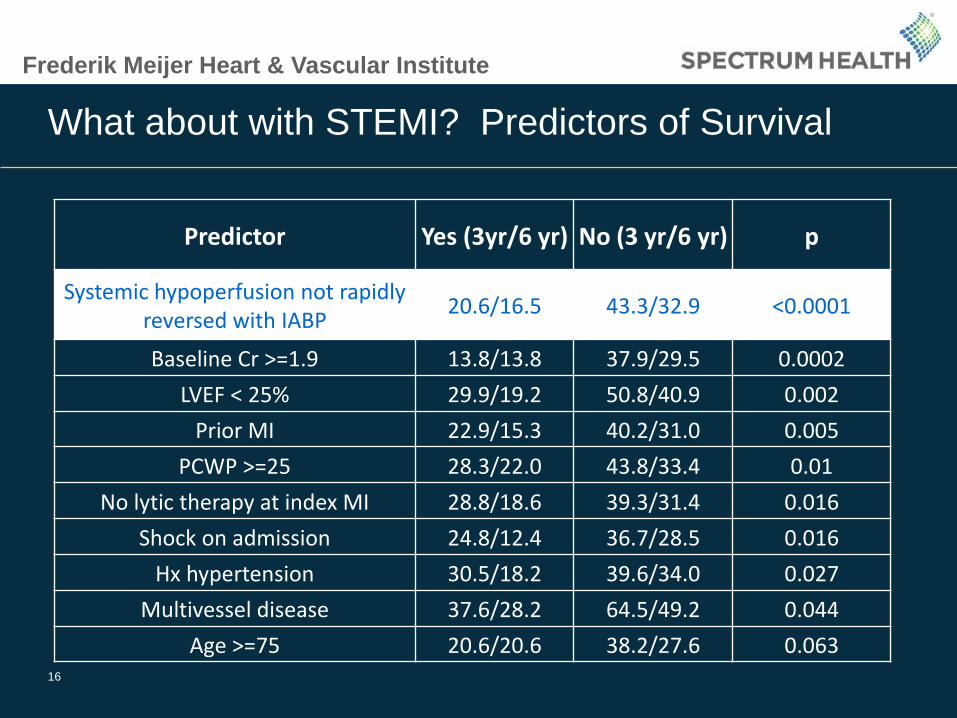
What about with STEMI? Predictors of Survival
Predictor Yes (3yr/6 yr) No (3 yr/6 yr) p
Systemic hypoperfusion not rapidly reversed with IABP
20.6/16.5 43.3/32.9 <0.0001
Baseline Cr >=1.9 13.8/13.8 37.9/29.5 0.0002
LVEF < 25% 29.9/19.2 50.8/40.9 0.002
Prior MI 22.9/15.3 40.2/31.0 0.005
PCWP >=25 28.3/22.0 43.8/33.4 0.01
No lytic therapy at index MI 28.8/18.6 39.3/31.4 0.016
Shock on admission 24.8/12.4 36.7/28.5 0.016
Hx hypertension 30.5/18.2 39.6/34.0 0.027
Multivessel disease 37.6/28.2 64.5/49.2 0.044
Age >=75 20.6/20.6 38.2/27.6 0.06315
Frederik Meijer Heart & Vascular Institute
What about with STEMI? Predictors of Survival
Predictor Yes (3yr/6 yr) No (3 yr/6 yr) p
Systemic hypoperfusion not rapidly reversed with IABP
20.6/16.5 43.3/32.9 <0.0001
Baseline Cr >=1.9 13.8/13.8 37.9/29.5 0.0002
LVEF < 25% 29.9/19.2 50.8/40.9 0.002
Prior MI 22.9/15.3 40.2/31.0 0.005
PCWP >=25 28.3/22.0 43.8/33.4 0.01
No lytic therapy at index MI 28.8/18.6 39.3/31.4 0.016
Shock on admission 24.8/12.4 36.7/28.5 0.016
Hx hypertension 30.5/18.2 39.6/34.0 0.027
Multivessel disease 37.6/28.2 64.5/49.2 0.044
Age >=75 20.6/20.6 38.2/27.6 0.06316

Frederik Meijer Heart & Vascular Institute
So we can say:
NIDCM: Patients who need inotropes (esp > 1 moderate dose)
are high risk. Even if they respond and improve, they are at
risk for the future.
STEMI: Initiate intentional meaningful surveillance:
• If shock doesn’t rapidly reverse with IABP,
• Baseline Cr >=1.9,
• Very low EF (<25%),
• Persistent PA wedge >25 (high LVEDP at cath)
• Advanced age, prior MI, etc…
17

Frederik Meijer Heart & Vascular Institute
What is optimal care?
Detect
• Vitals
• Feel (warm/cold)
• Look (JV pressure)
• Watch urine output, mentation, etc..
Recognize
• Inotropes = risk (two = high risk)
• Unstable after PCI = risk
• Tachycardia, poor urine output
Act
• Intensive surveillance
• Hemodynamic assessment and treatment.
Escalate
• Call for help.
• Shock call -mechanical circulatory support
18
Most of the time a code is called, we should view it as a
failure. How did we not act before it got to this point?

Frederik Meijer Heart & Vascular Institute
19
Frederik Meijer Heart & Vascular Institute
Hemodynamic: Not algorithmic
20
Filling: Enough? Too much?
Pump: Contractile strength / cardiac output?
Vascular tone: Vasoconstricted or vasodilated
(vasoplegia)

Frederik Meijer Heart & Vascular Institute
Vasoplegia
• Low SVR state
• Not well understood but
likely mediated by
inflammatory mediators
• Common in cardiorenal
syndrome
• Common after
resuscitation
21

Frederik Meijer Heart & Vascular Institute
How do you handle vasoplegia?
22
1. Stop vasodilators.
2. Give vasoconstrictors.
3. Correct acidosis.
4. Give them as much
cardiac output as you
can. (Concept of “not
enough” CO)
5. Methylene blue

Frederik Meijer Heart & Vascular Institute
But which drug?
Dopamine:Mostly a vasoconstrictor.
Tachycardia
Norepinephrine: Mostly a vasoconstrictor.
Phenylephrine: Vasoconstrictor.
Milrinone:Inodilator (inotrope plus
vasodilator)
Dobutamine: Inodilator (mostly inotrope)
Epinephrine:Inoconstrictor (inotrope plus
vasoconstrictor)
Nitroprusside: Arterial Vasodilator
Nitroglycerin: Venodilator23

Frederik Meijer Heart & Vascular Institute
How about in cardiac surgery?

Frederik Meijer Heart & Vascular Institute
Inotrope level predicted mortality
0%10%20%30%40%50%60%70%80%
Mortality
Mortality

Frederik Meijer Heart & Vascular Institute
Why did they look at this data?
“Early in our experience, we had no
formal insertion criteria. Patients
were placed on VAD support
after "maximal inotropic support”
and an IABP failed to improve
cardiac hemodynamics,
particularly cardiac output. As a
consequence of this, VADs were
being placed at the surgeon's
discretion and results were poor;
the devices were being placed
late and the incidence of MOSF
was high.” ZERO % survival…
VAD Insertion
Formula:If 2 or more high
dose inotropes and
ongoing
cardiogenic shock,
then place the
VAD.

Frederik Meijer Heart & Vascular Institute
Did it make a difference?
Before After
Placed within 3 hours of
first attempt to wean from
CPB
22% 85%
Placed late (>3 hours) 78% 15%
MOSF 78% 15%
Able to be weaned 22% 80%
Survival to discharge 0% 40%

Frederik Meijer Heart & Vascular Institute
Did it make a difference?
Before After
Placed within 3 hours of
first attempt to wean from
CPB
22% 85%
Placed late (>3 hours) 78% 15%
MOSF 78% 15%
Able to be weaned 22% 80%
Survival to discharge 0% 40%

Frederik Meijer Heart & Vascular Institute
What are the lessons?
• The degree of inotropic support needed predicts survival.
• The mortality curve takes an exponential increase starting
at one high dose inotrope. This is when to “blink”.
• Physicians when left to their own clinical judgment try too
hard to get by without mechanical circulatory support.
• In this setting the outcomes with VAD were terrible.
• Having a rigor which forces you to take the leap to the next
step improves the outcomes with the use of mechanical
circulatory support.
29

Frederik Meijer Heart & Vascular Institute
What does this all mean?
Recognize high risk patients
• Signs/sxsof shock
•
•
• Inotrope need, etc.
• Low BP
• Cool, clammy, low u/o

Frederik Meijer Heart & Vascular Institute
What does this all mean?
Recognize high risk patients
• Signs/sxs of shock
Engage Surveillance
• Active
• Intentional
• Responsive
•
• Inotrope need, etc.
• Low BP
• Cool, clammy, low u/o
• Urine output
• Swan/A-line
• Serial ABG
(q2 or q4 hr)

Frederik Meijer Heart & Vascular Institute
What does this all mean?
Recognize high risk patients
• Signs/sxs of shock
Engage Surveillance
• Active
• Intentional
• Responsive
Engage the shock team
• Shock team criteria
• Inotrope need, etc.
• Low BP
• Cool, clammy, low u/o
• Urine output
• Swan/A-line
• Serial ABG
(q2 or q4 hr)

Shock Team Process
Shock Team
AHF Cards
CT Surgery
CTCC
CV anesth
ECMO team
ChrgRNs
Imaging
IntervCards
33
Rapid, complex
decisionsRapid,
deployment

Frederik Meijer Heart & Vascular Institute
Urgent MCS is HARD to do.. (fast decisions & deployment)
• Which patients?• To act or NOT to act?
• Which modality?
• How to get it all in
place quickly?• Where? OR, ICU, Cath lab,
ER?
• Who? Surgeon, Cardiologist
(Who is qualified and
available?)
?34

Frederik Meijer Heart & Vascular Institute
Extracorporeal CPR (ECMO during CPR)
35
In hospital cardiac arrests
• 115 conventional ACLS / CPR (CCPR)
• 59 extracorporeal CPR (ECMO + CPR and ACLS)
Lancet 2008; 372: 554–61

Frederik Meijer Heart & Vascular Institute
ECPR provided significant benefit
93.2%
76.3%
44.1%
33.9%
38.1%
31.0%
21.2%
15.0%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1 3 14 30
ECPR Survival
CCPR Survival
36
Time (days)

Frederik Meijer Heart & Vascular Institute
This was not ECPR for EVERY arrest
Notes:
Out of 975 cardiac
arrests, 174 came
into the research
protocol, (59
ECPR)
(Patients that did not
rapidly respond to
usual ACLS.)
37
801
11559
Management
Not in trial
CCPR
ECPR

Frederik Meijer Heart & Vascular Institute
Survival based on CPR duration
38

Frederik Meijer Heart & Vascular Institute
Survival based on CPR duration
Notes:
• If initial ACLS does
not revive them
ECPR ALWAYS
had better survival.
• Survival rates
varied between 17
and 42%. (STILL
between 60 and
80% mortality).
• 18% survived with
extreme durations
of CPR39

Frederik Meijer Heart & Vascular Institute
Survived after 3 hours of CPR...
40

Frederik Meijer Heart & Vascular Institute
What do this and other reports teach us?
• If you can urgently deploy
mechanical circulatory support
you can save ACLS refractory
patients.
• Still VERY HIGH mortality
(survival around 25-30%)
• Probably an OK thing to do for
the right candidates.
• Can we better select the “best
use” of this resource?41
Is this patient capable of
surviving a massive insult?

Frederik Meijer Heart & Vascular Institute
Intra-aortic balloon pump (IABP)
Use is becoming much
less.
42

Frederik Meijer Heart & Vascular Institute
ISAR-SHOCK
13 IABP vs. 12 Impella
• Better immediate CI
improvement
• More anemia
• 1 incident of limb
ischemia
Too small. Unanswered
questions.43

Frederik Meijer Heart & Vascular Institute
IABP-SHOCK II
300 IABP vs. 298 control
• No difference in mortality
• Trend toward benefit if
age < 50 or first MI
Questions:
• RCA (RV infarcts?)
• Cross over? Selection
bias?
• Rapid PCI trumps
everything else
44

Frederik Meijer Heart & Vascular Institute
Impella
Versions:
• 2.5 for protected PCI
• CP (3.5) for protected
PCI and acute
cardiogenic shock
• 5.0 = surgically placed
• RP = right sided
45

Frederik Meijer Heart & Vascular Institute
Impella lessons learned
1. Hard to use in very dilated hearts.
2. You can’t ask it to do more than it can do.
• If you need 5 liters then use something that delivers 5 liters.
• If you just stomp on the gas you will get hemolysis.
3. A good tool for the acute ischemic heart.
46

Frederik Meijer Heart & Vascular Institute
47

Frederik Meijer Heart & Vascular Institute
48

Frederik Meijer Heart & Vascular Institute
Early Impella had higher survival
49

Frederik Meijer Heart & Vascular Institute
Centrimag
Very nice pump with
favorable hemolysis
profile.
Surgically placed.
Common to use atrial
inflow. (Beware
microembolic events
from native LV)
Durable device.50

Frederik Meijer Heart & Vascular Institute
ECMO = ExtraCorporeal Membrane Oxygenation
• Remove blood.• Oxygenate the blood
• Remove CO2 from the blood
• Warm the blood
• Return the blood and
pump it at desired flow
(2-6 liters/minute)
• Components:• Pump = Replace heart fxn
• Oxygenator = Replace lung fxn51

Frederik Meijer Heart & Vascular Institute
ECMO MODE: Proportion of VA to VV
Definition: Percent of patients > 18 years old with VA vs VV access.
“VA” = VA, VA+V and VA-VV
“VV” = VV, VVDL and VVDL+V
Source: ELSO Data
VA84%
VV16%
Adult ECMO Patients Broken Down by Mode
2015
(82/98)
(16/98)

Frederik Meijer Heart & Vascular Institute
ECMO Survival: Patients Discharged Alive
53
Percent of patients > 18 years of age that were discharged alive vs. those who
died during this hospitalization (All Causes) Source: ELSO Data
Survived63%
Died37%
Adult ECMO Patients2015
(36/98)
(62/98)

Frederik Meijer Heart & Vascular Institute
ECMO Survival: by VA or VV Mode
54
Definition: Percent of patients > 18 years old with VA vs VV access.
“VA” = VA, VA+V and VA-VV
“VV” = VV, VVDL and VVDL+VELSO survival: Cardiac 39% Respiratory 55%
Source: ELSO Data
Survived63%
Died37%
Adult VA Patients 2015
(31/83)
(52/83) Survived67%
Died33%
Adult VV Patients2015
(5/15)
(10/15)

Frederik Meijer Heart & Vascular Institute
ECMO Survival: ECPR
55
Survival of Adult ECMO Patients with ECPR
2015
Source: ELSO Data
(2/6)
(4/6)
(2/6)
(4/6)
Survived33%
Died67%
(4/6)
(2/6)

Frederik Meijer Heart & Vascular Institute
Acute MCS: Immediately ask, “What next?”
Early crossover
was mean
mean 2.5 +-
0.8 days
Late crossover
was mean 6.7
+- 3.2 days
56Artif Organs. 2017 Mar;41(3):224-232. doi: 10.1111/aor.12758. Epub 2016 Sep 23.

Frederik Meijer Heart & Vascular Institute
Summary
• Detect / Recognize / Act / Escalate• “You are so important that we are going to do more
than might be necessary.”
Failure to Rescue
• Not a cookbook.
• Wet or dry? Cold or warm? Vasoconstricted or vasodilated?
Hemodynamic Treatment
• Acute MCS can and is saving people who normally would have died.
• “The times – they are a changin!”Shock Team
57

Frederik Meijer Heart & Vascular Institute
QUESTIONS / COMMENTS?Thanks for your attention!
58