-
CARDIOGENIC SHOCKFaculty of MedicineUniversity of Brawijaya
-
DEFINITION of SHOCKIT IS NOT LOW BLOOD PRESSURE !!!IT IS
HYPOPERFUSION..Disorder of tissue perfusion as a result of
imbalance between oxygen supply to and oxygen demand of the
cells.All types of shock result in tissue perfusion disorder, which
may develop acute circulatory failure or it is also called shock
syndrome
-
TYPES OF SHOCK**MORE THAN ONE TYPE MAY BE PRESENT
-
DEFINITION OF CARDIOGENIC SHOCKSystolic BP < 90 mm Hg, or 30
mm Hg below baseline for at least 30 mins, evidence of poor tissue
perfusion and persistence of shock after correction of
non-myocardial factors (eg hypovolaemia, hypoxia, acidosis,
arrhythmias)
- CRITERIA FOR CARDIOGENIC SHOCK DIAGNOSIS
-
SHOCK REGISTRY JACC SEPT. 2000, SUPP. A SPECTRUM OF CLINICAL
PRESENTATIONS5.6%28%65%1.4%
MortalityRespiratoryDistressHypotensionHypoperfusion21%22%70%60%
-
RISK FACTORS FOR CARDIOGENIC SHOCK DUE TO AMI [ACUTE MYOCARD
INFARCT]-MEDIATED LV DYSFUNCTIONAge > 65Female genderLarge
infarctionAnterior infarctionPrior infarctionDM (diabetes
mellitus)Prior HTN (hypertension)
-
POST-MORTEM STUDY OF SHOCK HEARTSAt least 40% of the myocardium
infarcted in the aggregate (old and new injury)
80% have significant LAD (left anterior descendent) disease
2/3 have severe 3Vdz (three vessel disease)
-
OUTCOMES OF CARDIOGENIC SHOCKHistoric mortality 60-80%
More recently reported mortality numbers67% in the SHOCK trial
registry56% in GUSTO-I(v.s. 3% in Pts. without shock)
-
OUTCOMES OF CARDIOGENIC SHOCKThe ST pattern in Cardiogenic
shock: 15-30 % Non-ST elevation MIOlderMortality: 77% 70-85% ST
elevations MI/ New LBBBMortality: 53-63%
-
OUTCOMES OF CARDIOGENIC SHOCKThe SHOCK registry
Similar mortality in the two groups62.5% in non-ST
elevation60.4% with ST elevation
-
AETIOLOGY OF CARDIOGENIC SHOCK
myocardial infarction including complications of myocardial
infarction (eg acute mitral regurgitation, VSD, free wall rupture,
LV aneurysm) end-stage cardiomyopathy myocardial contusion
myocarditis LV outflow obstruction (HOCM, aortic stenosis) LV
inflow obstruction (mitral stenosis, LA myxoma) sequela of
cardiopulmonary bypass
-
ETIOLOGIES OF CARDIOGENIC SHOCKAcute myocardial
infarction/ischemiaLV failureVSR(ventricular septal
rupture)Papillary muscle/chordal rupture- severe MR (mitral
regurgitation)Ventricular free wall rupture with subacute
tamponadeOther conditions complicating large
MIsHemorrhageInfectionExcess negative inotropic or vasodilator
medicationsPrior valvular heart
diseaseHyperglycemia/ketoacidosisPost-cardiac
arrestPost-cardiotomyRefractory sustained tachyarrhythmiasAcute
fulminant myocarditisEnd-stage cardiomyopathyHypertrophic
cardiomyopathy with severe outflow obstructionAortic dissection
with aortic insufficiency or tamponadePulmonary emboluSevere
valvular heart disease-Critical aortic or mitral stenosis, Acute
severe aortic or MR
-
PATHOPHYSIOLOGYCompensatory mechanisms such as salt & water
retention and peripheral vasoconstriction tend to exacerbate LV
dysfunction. Also decreased perfusion pressure, especially in the
presence of multi-vessel coronary disease leads to further
depression of myocardial contractility.
-
PATHOPHYSIOLOGY OF SHOCK Effect of: Elevated LVEDP on coronary
flow
LVEDP(mm Hg)
-
PATHOPHYSIOLOGY OF SHOCKHypotension + LVEDP and critical
stenosis Myocardial Hypoperfusion LV dysfunction Systemic lactic
acidosis Impairment of non-ischemic myocardium worsening
hypotension.
-
SCHEMATICLVEDP elevationHypotensionDecreased coronary
perfusionIschemiaFurther myocardial dysfunctionNeurohormonal
activation VasoconstrictionEnd-organ hypoperfusion
-
CLINICAL FINDINGSPhysical Exam: elevated JVP, +S3, rales,
oliguria, acute pulmonary edema
Hemodynamics: decreased CO (cardiac output), increased SVR
(systemic vascular resistance), decreased SvO2 (oxygen
saturation)
Initial evaluation: hemodynamics (PA [pulmonary artery]
catheter), echocardiography, angiography
-
INVESTIGATIONS
Echo for all patients to exclude surgically correctable lesion
and tamponade and to look for RV infarction ECG: normal ECG
virtually excludes possibility of cardiogenic shock caused by MI
(myocardial infarction)
-
DIFFERENTIAL DIAGNOSIS OF CARDIOGENIC SHOCK
AMI (acute myocard infarct)PE (pulmonary embolism)COPD (chronic
obstructive pulmonary disease)PneumoniaAortic
dissectionTamponadeAcute valvular insufficiencyHemorrhageSepsisDrug
OD (over dosage) of negative inotropic/chronotropic agent
-
4 POTENTIAL THERAPIES PressorsIntra-aortic Balloon Pump
(IABP)FibrinolyticsRevascularization: CABG (coronary artery bypass
grafting)/PCI (Per Cutaneous Coronary Intervention)
Refractory shock: ventricular assist device, cardiac
transplantation
-
TREATMENT OF CARDIOGENIC SHOCK optimize preload and afterload.
Vasodilators should be given with extreme caution. Nitroprusside
may cause coronary steal. Vasodilators particularly important when
mitral regurgitation is a major contributing factor
-
TREATMENT (CONTINUED.)inotropes. Dobutamine unless shock is
profound in which case drugs with vasoconstrictor actions
preferable. Phosphodiesterase inhibitors should be reserved for
those in whom catecholamines have failed to improve cardiac
performance or those in whom arrhythmia or ischaemia limits
catecholamine dose intra-aortic balloon pump. Only of value if
subsequent revascularization is possible
-
TREATMENT (CONTINUED)thrombolysis. No definite evidence that
this alters prognosis. May be less effective in patients with
cardiogenic shock because of poor coronary blood flow. Combination
of thrombolysis and IABP may be more effective. Mortality higher in
those treated with t-PA compared to those treated with
streptokinase
-
TREATMENT (CONTINUED..)PTCA (Percutaneous transluminal coronary
angioplasty). Probably treatment of choice in cases due to IHD
(ischemic heart disease). Both PTCA and CABG need to be performed
within first few hours (ideally within 2-4 h) of onset of symptoms.
Result in improved survival at 6 months and 1 year although not at
30 days
-
TREATMENT (CABG (coronary artery bypass grafting). May be of
benefit if facilities immediately available. Operative mortality is
high
-
TREATMENTPatients with RV infarction leading to cardiogenic
shock particularly sensitive to volume depletion and prone to
deterioration from bradycardia and loss of AV synchrony due to
advanced heart block. Focus of therapy should be immediate
restoration of adequate LV filling pressure, maintenance of sinus
rhythm or synchronized pacing and use of dobutamine to stimulate RV
systolic function
- PRESSORS DO NOT CHANGE OUTCOMEDopamine
-
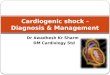
IABP (INTRA AORTIC BALLOON PUMP) IS A TEMPORIZING
MEASUREAugments coronary blood flow in diastole
Balloon collapse in systole creates a vacuum effect decreases
afterload
Decrease myocardial oxygen demand
-
Intra-Aortic Balloon Pump
-
INDICATION FOR IABP
-
CONTRAINDICATIONS TO IABPSignificant aortic regurgitation or
significant arteriovenous shunting Abdominal aortic aneurysm or
aortic dissection Uncontrolled sepsis Uncontrolled bleeding
disorder Severe bilateral peripheral vascular disease Bilateral
femoral popliteal bypass grafts for severe peripheral vascular
disease.
-
COMPLICATIONS OF IABPCholesterol EmbolizationCVA (cerebro
vascular accident) Sepsis Balloon
ruptureThrombocytopeniaHemolysisGroin InfectionPeripheral
Neuropathy
-
HOCM (HYPERTROPHIC OBSTRUCTIVE CARDIOMYPATHY)usual methods used
to treat cardiogenic shock exacerbate obstruction plasma volume
expansion and IV titration of beta-blockers reduce ventricular
outflow obstruction and improve cardiac output
-
PROGNOSIS OF PATIENTS WITH CARDIOGENIC SHOCKpoor only about 1/3
of patients actively treated survive initial episode and many of
the survivors have continuing angina, CCF and decreased exercise
tolerance approximately 1/2 with a surgically correctable lesion
leave hospital RV function usually returns to normal in survivors
of cardiogenic shock associated with RV infarction
-
PROGNOSIS50% of patients who require maximal therapy and IABP to
come off bypass die. If ventricular assist device also required
then only 35-45% survive. Functional prognosis for these survivors
quite good Mortality without aggressive highly technical care is
70-90%. Hospitals without the facilities for IABP or high-risk
angioplasty and surgical intervention should begin initial
resuscitative measures and then make a rapid decision about
transfer to a hospital with the necessary resources
-
Myocardial stunning and hibernation
-
MYOCARDIAL STUNNINGMechanical dysfunction of myocardium which
persists despite absence of irreversible damage and restoration of
normal or near-normal coronary flow and which recovers
spontaneously.Clinically important in 3 settings:- after MI
(especially after thrombolysis or primary angioplasty)- after
complicated coronary interventions (when myocardium may be
ischaemic for long periods, particularly if there is pre-existing
LV dysfunction)- after cardiac surgeryMechanical circulatory
support may be preferable to inotropes for patients with stunned
myocardium as inotropes may adversely influence recovery of
potentially ischaemic segments
-
HIBERNATING MYOCARDIUMMyocardium with impaired function that is
persistently impaired at rest due to decreased coronary blood flow
but which demonstrates improved function when balance between
oxygen supply and demand is improved.Dobutamine echocardiography
can be used to differentiate between stunned myocardium with a
patent artery ( function that persists during infusion) from
stunned myocardium with a stenosed artery or hibernation (initial
followed by deterioration).
-
*Not much data to support the last item*