Embed Size (px)
Citation preview

Leukotriene Antagonists As First-line
Asthma Controller For Step 2
David PriceProfessor of Primary Care Respiratory Medicine, University of Aberdeen;Director of Research in Real-Life, Singapore; Member of ARIA and EPOS Executive; Co-founder of the Respiratory Effectiveness Group; Community Based Respiratory Specialist Norfolk
Wednesday May 20th; 2:15-2:35 PMFour Seasons Ballroom 3-4 (lower level), Colorado Convention Center

Faculty Disclosures: ATS 2015 – Denver (I)
Relevant financial relationships with a commercial interest:
David Price
• Board Membership Company (past and current): Aerocrine Board Membership, Almirall, Amgen, AstraZeneca, Boehringer Ingelheim, Chiesi, Meda, Mundipharma, Napp, Novartis, and Teva.
• Consultancy (current): Almirall, Amgen, AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Meda, Mundipharma, Napp, Novartis, Pfizer, and Teva;
• Grants and unrestricted funding for investigator-initiated studies (past and current): UK National Health Service, British Lung Foundation, Aerocrine, AKL Ltd, Almirall, AstraZeneca, Boehringer Ingelheim, Chiesi, Eli Lilly, GlaxoSmithKline, Meda, Merck, Mundipharma, Napp, Novartis, Orion, Pfizer, Respiratory Effectiveness Group, Takeda, Teva, and Zentiva; Payments for lectures/speaking: Almirall, AstraZeneca, Boehringer Ingelheim, Chiesi, Cipla, GlaxoSmithKline, Kyorin, Meda, Merck, Mundipharma, Novartis, Pfizer, SkyePharma, Takeda, and Teva;
• Payment for manuscript preparation (past): Mundipharma and Teva

Faculty Disclosures: ATS 2015 – Denver (II)
Relevant financial relationships with a commercial interest:
David Price
• Patents (current): AKL Ltd• Payment for development of Educational Materials (past):
GlaxoSmithKline, Novartis; • Stock / stock options (current): Shares in AKL Ltd which
produces phytopharmaceuticals; 80% ownership of Research in Real Life Ltd and its subsidiary social enterprise Optimum Patient Care
• Payment for travel/accommodation/meeting expenses (past): Aerocrine, Boehringer Ingelheim, Mundipharma, Napp, Novartis, and Teva;
• Funding for patient enrolment or completion of research (past): Almirral, Chiesi, Teva, and Zentiva;
• Peer reviewer for Grant committees (past): Medical Research Council (2014), Efficacy and Mechanism Evaluation programme (2012), HTA (2014)

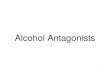
Current asthma management in the UK
1 2 3 4 50
5
10
15
20
25
30
35
GINA treatment stage
Per
cen
tag
e o
f p
atie
nts
N = 29,337
Price D, et al. 2012 Thorax; 67:A186-A187
Stage 1
Beta-agonist
as necessary
Stage 2
Initiate ICS
Stage 3
Add LABA
Increase ICS
dose
Stage 4
Increase ICS
doseAdd
further therapy
Stage 5
High ICS doseOral
steroidsOther
therapies
BTS/SIGN. British guideline on the management of asthma (QRG 141); Oct 2014

Study Rationale: Guideline recommendations
1. Price D. Asthma. 1999;4:74–8.
• Recognition that airway inflammation is present even in patients with mild asthma has led to introducing anti-inflammatory therapy earlier in the management of asthma.
• Many patients with asthma still have considerable symptoms & lifestyle limitation despite ICS management.1 Possible reasons for this include:• Lack of disease recognition• Poor adherence to ICS• Poor inhaler technique• Untreated rhinitis• Smoking• Failure to optimise treatment

Uncertain landscape
• Short-term double-blind double-dummy studies and in patients with significant asthma severity comparing the use of montelukast vs ICS at step 2 suggested that leukotriene antagonists were inferior to ICS. Meta-analysis conclusions:1
• Patients randomised to LTRA had a 60% increased risk of exacerbation compared with those randomized to ICS
• Those randomised to ICS had a significantly increased FEV1 compared with LTRA
• Effects of montelukast and beclomethasone on airway function and asthma control:2
• 400μg BDP significantly improved FEV1 vs LTRA• No significant difference in exacerbations
Ducharme FM. BMJ 2003;326:621
Israel E, et al. JACI. 2002;110:847–54

Studies have shown that efficacy RCTs exclude about 95% of asthma and 90% of COPD routine care populations due to strict inclusion criteria.
Herland K, et al. Respir Med 2005;99:11–19.
Limitations: RCTs inclusions/exclusions
Does it matter…?

RCT references
1) Pawels R et al. N Engl J Med 1997
2) Kips J et al. Am J Respir Crit Care 2000
3) Bateman E. Am J Respir Crit Care 2004
4) Papi A et al. Eur Respir J 2007
5) Busse W et al. J Allergy Clin Immunol 2008
Real-life references
1) Partridge Pulm Med 2006
2) De Marco et al. Int Arch Allergy Immunol 2005
3 and 4) Janson et al. Eur Respir J 2001 3=Italy 4=UK
5 and 6) Breekveldt-Postma et al. Pharmaco-epidemiol Drug Saf 2008 5=fixed combination 6=ICS
7) Stallberg et al. Resp Med 2003
8) Adams et al. J Allergy Clin Immunol 2002
9) Corrigan Prim Care Resp J 2011
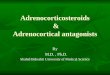
Randomised trials
1 2 3 4 50
20
40
60
80
100
Pe
rce
nta
ge
of
Pa
tie
nts
75-125 75-125
89>95
>80
1 2 3 4 5 6 7 8 90
20
40
60
80
100
45
34
17
49
14.18.3
34
21
40
Real-life studies
Adherence

Updated for the CRITIKAL patients population from Price et al, Abstract presented IPCRG 2014DPI = dry powder inhaler; MDI = metered-dose inhaler
Total patients = 4645
Inhaler errors: common…?

*Montelukast 10 mg once daily + budesonide 400 µg twice daily;
**Budesonide 800 µg twice daily
Price DB, et al. Allergy 2006; 61: 737–742.Price DB,et al. Thorax 2003; 58: 211–216.
Comorbidity interactions: rhinitis can affect response to medication

Chalmers GW et al. Thorax 2002;57:226–230
Kerstjens HA, et al. Eur Respir J 1993;6(6):868-76.
1: Non-smoker + ICS
4: Non-Smoker + Placebo
3: Smoker + Placebo
2: Smoker + ICS
1
2
3
4
Lifestyle interactions: smoking can affect response to medication

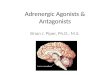
Different types of trial: the evidence paradigmP
opul
atio
n
Broad
Narrow
Ecology of care
FreeConstrained
Highly controlled Pragmatically controlled
Observational
Managed as...
Clinical diagnosis
Confirmed diagnosis Registration RCTs
Long term phase III
Pragmatic RCTs
Observational studies
http://www.effectivenessevaluation.org/ Roche N, Price D et. al 2013 Lancet Respir Med; 1(10):e29-30
ELEVATE

0 2 10 26 52 78 104Week Week:
Tailored treatment as indicated by guidelines
LTRA
Ideally no ICS use
ICS Ideally no LTRA use
Baseline
V1 V2 V3 V4 V5 V6 V7
SABA
Randomisation
Price et al NEJM 2011;364:1695-1707

ELEVATE Rational:meaningful outcome measures
Objective Measures Patient-reported / perceived
Efficacy Trial Endpoints “Real-life” control assessments
Airway function:• Spirometry (FEV1)• Domiciliary PEF
Patient-reported quality of life (QoL)
Airway hyper-reactivity:• methacholine bronchial challenge testing
Symptoms
Exacerbations
Rescue medication use
Price et al NEJM 2011;364:1695-1707

Eligibility Criteria: Conducted at 53 primary care practices in the UK. Enrolled patients 12 - 80 y with physician diagnosis of asthma
Flexibility and Practitioner Expertise: Both treatments, LTRA and inhaled glucocorticoid, were given according to normal clinical practice. All PCPs were eligible to participate
Protocol discouraged treatment changes between randomization and the 2-month visit. Patients receiving disallowed asthma medications remained in the study
Study Design
Price et al NEJM 2011;364:1695-1707

Patient population
• INCLUSION CRITERIA• Aged 12–80 year• Capable of understanding study and
procedures • A diagnosis of asthma:
• Documented reversibility after inhaled SABA, and/or
• PEF variability on PEF diary, and/or • Physician diagnosed asthma and/or • Physician diagnosis of asthma +
history of response to treatment• Not currently receiving, and had not
received, inhaled steroid or LTRA within the previous 12 weeks.
• EXCLUSION CRITERIA• Other clinical trial involvement
within 90 days.• Change in asthma medication
within previous 12 weeks.• Abuser of alcohol or illicit drugs.• Other pulmonary disorder
or unresolved respiratory infection in previous 12 weeks.
• A history of life-threatening illness
• Systemic, intramuscular or intra-articular corticosteroids in previous 2 weeks
Price et al NEJM 2011;364:1695-1707

Blinding…..
• General practitioners (GPs)/practice asthma nurses and participants were aware of the randomisation
• Study research assistants were blinded to the randomisation.
• Random allocation given directly to GPs / practice nurses by independent automated telephone system
• GPs / practice nurses had minimal involvement in data collection and continued with normal management following allocation
• Study research assistants collected resource use information, prescribing record data, and clinical resource utilisation data at the end of the study period
• When collecting resource data research assistants were blind to the randomised allocation of the participants

Outcome measuresPrimary:• Asthma Quality of Life Questionnaire (AQLQ) at 2 monthsThe trial was designed to test for equivalence wrt the MiniAQLQSecondary outcome measures included (at 2 months and 2 years):• Asthma Quality of Life Questionnaire (AQLQ) at 2 years• Adherence (based on prescription records)• Asthma Control Questionnaire (ACQ)• Royal College of Physicians 3-item asthma questionnaire
(RCP3)• 14-item Mini Rhinoconjunctivitis Quality of Life Questionnaire
(MiniRQLQ) • Severe asthma exacerbations - course of oral steroids or
hospitalization for asthma
Price et al NEJM 2011;364:1695-1707

Statistical Methods
• Primary analysis: intention-to-treat analysis of the MiniAQLQ score at 2 months.
• Criterion for equivalence: 95% confidence interval for the difference in the MiniAQLQ score would be between –0.3 and 0.3.
• Conservative approach in selecting 0.3 (min. clinically important difference for MiniAQLQ = 0.5)
Price et al NEJM 2011;364:1695-1707

ELEVATE: demographics and drop out rates Comparison to other studies (ELEVATE Step 2, GOAL)
1. Bateman ED, et al. Am. J. Respir. Crit. Care Med. 2004; 170: 836-844. 170. p.836, (2004)
Characteristic ELEVATEStep 2; N=306
GOAL1
Strata 1; N=1098
Sex (% Female) 51% 57%
Age * 45.8 (16.4) 36.3 (15.6)
Quality of Life (Juniper AQLQ 1, worst, to 7)
4. 74 (1.04) 4.4 (1.00)
Lung Function *86
%PPEF77
%PFEV1
Percent reversibility * 8.9% (9.86) 22% (12.2)
Smokers – current 21.9% 9.5%
Drop out rate 4.0% 15.4%

Months
ELEVATE: main results
Price et al. N Engl J Med. 2011 May 5;364(18):1695-707
Months

Adjusted Mean Difference
2 mo -0.02 (-0.24, 0.20)2 yr -0.11 (-0.35, 0.13)
Price et al. N Engl J Med. 2011 May 5;364(18):1695-707
Main results: primary outcome

WHY THE DIFFERENCE…?

Different types of trial: the evidence paradigmP
opul
atio
n
Broad
Narrow
Ecology of care
FreeConstrained
Highly controlled Pragmatically controlled
Observational
Managed as...
Clinical diagnosis
Confirmed diagnosis Registration RCTs
Long term phase III
Pragmatic RCTsObservational
studies
http://www.effectivenessevaluation.org/ Roche N, Price D et. al 2013 Lancet Respir Med; 1(10):e29-30
ELEVATE
Long term phase III
`Different population
Different Management`

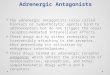
The PRECIS Wheel• The Pragmatic–Explanatory Continuum Indicator Summary
(PRECIS) wheel provides a structured approach to assessing the extent to which studies may provide direct/indirect evidence
• 9 “spokes,” each representing a different element of the study design (e.g., study eligibility criteria, expertise of individuals applying the intervention).
• Each spoke, or axis, represents an explanatory– pragmatic (i.e., efficacy–effectiveness) continuum, and aspects of a trial are scored/positioned along each respective axis depending on the extent to which they reflect the characteristics of an explanatory (efficacy) RCT or a pragmatic effectiveness trial
Thorpe KE, et al. CMAJ 2009;180:E47–E57.

The PRECIS Wheel
Pragmatic (A) vs Classical RCT mapped on the PRECIS wheel domains. The visual representation shows the clear gaps in the efficacy trial design
B. Malmstrom K, et al. Ann Intern Med 1999;130:487–495.
A. Price D, et al. Health. Technol Assess 2011;15:1–132
Wong GW, et al. Ann Am Thorac Soc. 2014;11:472
• Choice of a Clinically Relevant Endpoint
• Duration of Follow-up Relevant to Patient Care
• LTRA and ICS given according to normal clinical practice.
• Patients receiving disallowed asthma medications remained in the study

Call the detective…
ELEVATE adherence
Price et al. N Engl J Med. 2011 May 5;364(18):1695-707
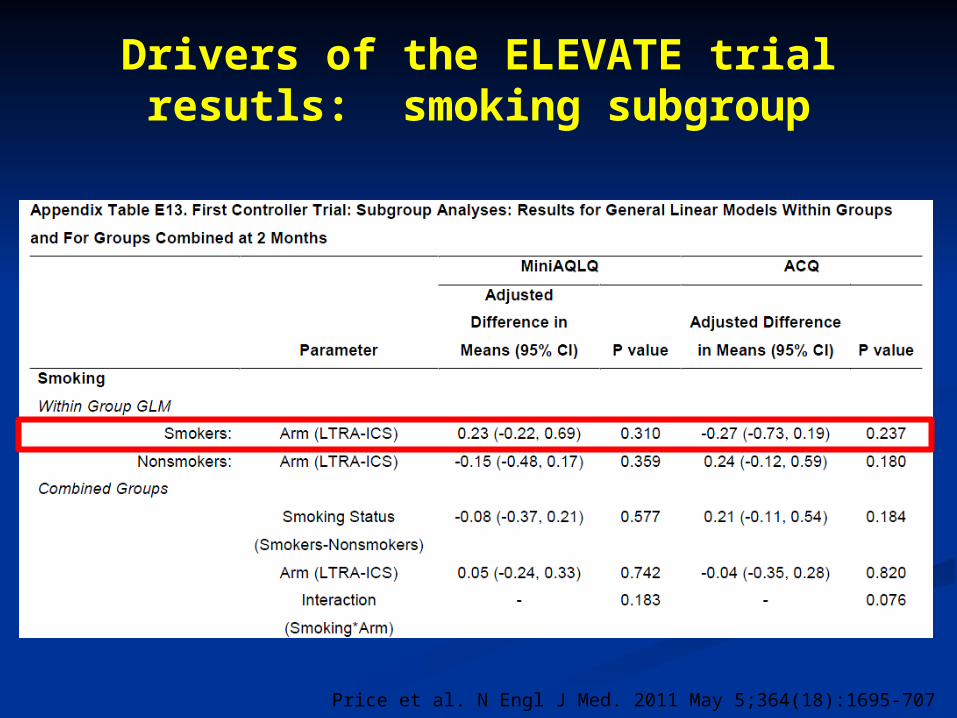
Drivers of the ELEVATE trial resutls: smoking subgroup
Price et al. N Engl J Med. 2011 May 5;364(18):1695-707

Drivers of the ELEVATE trial results: rhinitis subgroup?
Price et al. N Engl J Med. 2011 May 5;364(18):1695-707
• MiniRQLQ score was significantly better at 2 months but not at 2 years for patients receiving LTRA

Crossover implications
• Non-adherence in a non-inferiority trial can create a bias toward a finding of equivalence.
• Substantial crossover can result in greater similarity between the treatment regimens that are ultimately followed, yielding similar outcomes in comparator arms

Changes in Treatment According to Assigned Treatment
Bias away from the Null:
Number of patientsLTRAn(%)
ICSn(%)
Total in group 145 155
Changes at 2 months 8 (6%) 5 (3%)
Changes at 2 years 45 (31%) 32 (21%)

Other drivers…?
The subgroups of patients:
• Smoke and have non-eosinophilic disease?
• With/without evidence for a mixture of chronic and reactive
obstructive pulmonary disease?
• With rhinitis versus:
• Diagnosed vs Managed vs Self-reported
• With reversibility/without (limited) reversibility?
• Staying with assigned randomised therapy versus those going
off that therapy/those going to other therapy
• With higher vs lower ACQ cut points?
• Duration since diagnosis versus response

Strengths
• UK Government Funded
• Choice of a Clinically Relevant Endpoint
• Relevant Comparison of Alternative Treatments
• Duration of Follow-up Relevant to Patient Care
• Intensive Monitoring of Adverse Events
• Open-label Design with Patient-Reported Primary Outcome
• Equivalence Design with Flexible Treatment Regimens Allowing Bias Away from the Null
• Equivalence design with substantial cross-over
• Un-blinded design with primary endpoint based on patient self-assessment
Limitations

CONCLUSIONS

Conclusions: ELEVATE
The question asked by ELEVATE was:
“In a broad primary are population who have been considered for commencement of regular anti-inflammatory therapy, is initiation of therapy via LTRA non-inferior to ICS?”
The results suggest that starting anti-inflammatory therapy as LTRA is non-inferior to initiating as ICS:• In this new-initiation patient population • Treated in a less onerous ecology of care than is
used in a classical RCT

Real-life studies
Clinical drivers: representative dataCharacteristics of routine care populations (clinical, demographic,
lifestyle) can interact with “pure” classical RCT efficacy results
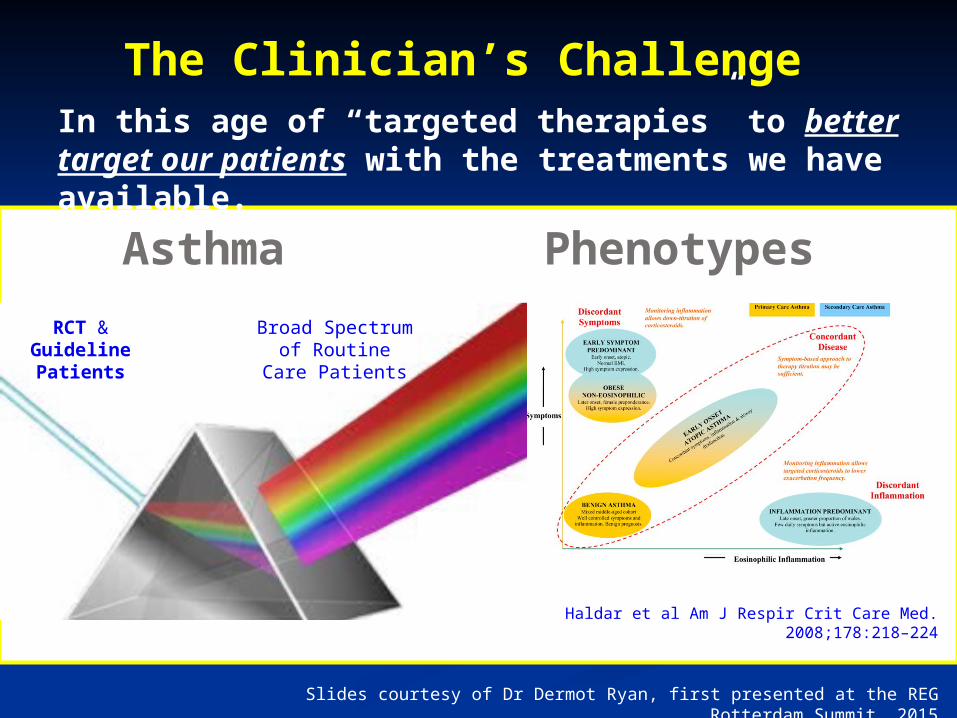
Slides courtesy of Dr Dermot Ryan, first presented at the REG Rotterdam Summit, 2015
Haldar et al Am J Respir Crit Care Med. 2008;178:218–224
RCT & Guideline Patients
Broad Spectrum of Routine Care
Patients
In this age of “targeted therapies” to better target our patients with the treatments we have available.
The Clinician’s Challenge
Asthma Phenotypes