Embed Size (px)
Citation preview

Update on New AntifungalsUpdate on New AntifungalsGrand RoundsGrand Rounds
Jack D. Sobel, M.D.Jack D. Sobel, M.D.Professor of MedicineProfessor of Medicine
Wayne State University School of MedicineWayne State University School of MedicineDetroit, MIDetroit, MI

A 74-year-old male is admitted with a one day history of fever, chills and rigors. He also reports nausea, vomiting but denies any urinary or respiratory symptoms. He is a Type I, severe diabetic on a moderately high dose of insulin, whose control has been poor.
Past medical history is positive for two episodes of myocardial infarction, coronary angioplasty ~2002, moderate intermittent claudication and a mixed sensory-motor peripheral neuropathy. Hypertension for approximately 20 years.

In the E.M. Department, he was found to be moderately dehydrated, temperature 103.2°F, pulse 128/m, BP 110/60, but was lucid and fully orientated. JVP not elevated, lungs clear to auscultation and CVS examination revealed a summation gallop and grade 2/6 ESM at left parasternal border. Abdominal exam was normal. Rectal exam showed mild BPH and a symmetrical peripheral neuropathy was evident. No pulses detectable below popliteal region.

Laboratory StudiesLaboratory Studies• Hemoglobin 14.39%• WBC 17,900/mm3
L. shift7% bands
• Platelets 390,000/mm3
• BUN 79 mg%• Creatinine 3.1%• ABG/electrolytes Moderate ketoacidosis• Glucose 480 mg%• Urine WBC – TNTC
Numerous bacteriaGram stain – GNRGlucose ++1Protein ++1Yeast +

Laboratory StudiesLaboratory Studies
• Blood cultures pending
• Urine cultures pending
• Abdominal ultrasound: moderate right hydronephrosis

A presumptive diagnosis of urosepsis with ketoacidosis and dehydration was made and in the E.R. patient was given Cefepime, rehydration and insulin and transferred to MICU.

• Rehydrated and electrolytes and metabolic status corrected
• BP 150/75, Pulse 115/m
• Fails to defervesce – 102.8°F
• Blood culture positive for a yeast
• Urine cultures:
105/ml E. coli
105/ml Candida albicans
105/ml Candida glabrata
Over the Next 48 HoursOver the Next 48 Hours

• Initially treated for bacterial pyelonephritis only – with marginal benefit
• Candidemia needs to be treated.
• Which antifungal?
• Consideration in selecting antifungal
• Renal insufficiency
• Urine concentrations of antifungal
• Candida species identification
• Pathogenesis
IssuesIssues

• Given fluconazole 100 mg IV/daily
BUT
• Remained febrile, tachycardiac
• Blood cultures pending
• I.D. consult obtained

• MRI of abdomen obtained
• Right hydronephrosis, mild hydroureter
• Mass in right dilated pelvis
• Urology – placed right nephrostomy tube
• Dye study via tube revealed a mass suggestive of fungus ball and papillary necrosis

• Amphotericin B desoxycholate (conventional)• Lipid formulation - Ambisome®
- Abelcet®
• IV azole - Fluconazole - Itraconazole - Voriconazole - Posaconazole• IV echinocandin
- Caspofungin
- Anidulafungin
- Micafungin
• Combination-
AmB + fluconazole-
AmB + flucytosine• Sequential
Selecting an AntifungalChoices

A Look At The AntifungalChoices
Amphotericin B desoxycholate
• Mainstay for > 30 years
• Broad spectrum, fungicidal
• Predictable/?inevitable toxicity
• Many experts no longer use AmB!!!

• Nearly normal renal function
• Not receiving other nephrotoxic agents
• Short course anticipated
• Able to tolerate a few chills
• Neonate (amazing toleration)
• Experienced physician who understands azotemia is temporary and side effects manageable
Still Role for Conventional AmB??
Maybe Not

Fluconazole - How Good?

Advantages
1) Safe, excellent penetration
2) Effective and broad spectrum
3) C. albicans resistance continues to be rare
4) Inexpensive
5) Can switch to oral with excellent absorption
Fluconazole

Concerns About Fluconazole
• Candida krusei - Yes, but…
• Other Candida non-albicans species
No problem except
C. glabrata
• Persistent candidemia 10-15%
(usually with in vitro sensitive strains)

Concerns About Fluconazole -C. glabrata
• MIC’s: 57% Susceptible (< 8 µg/ml)32% S-DD (16-32 µg/ml)
11% Resistant (> 64 µg/ml)• Can we overcome resistance with dose 800
mg/d?No supporting data!
• Have we seen clinical resistance i.e. failure with C. glabrata?? Not really?
• In Rex study 9/11 responded• Anecdotal failure Yes• Worth the risk?? Stable patient – Yes
(BSI ~ 15-30%) Seriously ill – No!!!

Fluconazole + AmB Combination1
• Not antagonistic
• Faster clearance of blood cultures
• Lowest rates of persistent candidemia
• More toxic
• Enthusiasm for combination ↓ with arrival of newer antifungals
1Rex J et al, CID, 2003

What About IV Itraconazole?
• Late in coming – why? No IV
• Now IV itraconazole in cyclodextrin 200 mg q 12h x 2 d then 200 mg/d
• Oral solution equivalent to oral fluconazole
• Slightly broader spectrum but more drug interactions
• Little data but probably equivalent in efficacy for Candida

Voriconazole?
• Drug of first choice for primary therapy of IA
• Extremely useful for emerging moulds fusarium, scedosporium spp. also
crypto
But not Zygomycetes
• In fact, 3 major reports of Zygomycosis in HSCT while on vori
• What about Candida spp.?

Voriconazole?
• In vitro 10-100x more active than fluconazole
Active against C. krusei
Active against C. glabrata but MIC’s are higher!!
• Clinically
As effective as fluconazole in OPC/EC (Ally et al 2001)
Effective against fluconazole-resistant mucositis ~70%

Voriconazole for Candidemia
• RCT versus AmB followed by Fluconazole• 422 non-neutropenies, in non-inferiority
study• Response at 12 weeks
• 40.7% versus 40.7% - Equivalent!• Median clearance blood Cx – 2 days• More renal toxicities in AmB/fluc
• Potential as broad spectrum initial choice + later orally

Any Problems With Voriconazole
• > expensive than fluconazole
• ½ life 6 hr – dose b.i.d.
• IV not in presence of renal failure
• Does not get into urine
• > side-effects than fluconazole e.g. visual/photopsia
• > drug interactions e.g. rifampin

Posaconazole
• Not yet available commercially
• Oral and eventually IV
• May have role in mucormycosis for prolonged oral therapy after response to AmB (or 1° or combination therapy)
• Emerging moulds

What about the echinocandins??

EchinocandinsEchinocandinsFungal Cell WallFungal Cell Wall11
Non-competitive Inhibition by:Lipopeptide Class of Antifungals(Enchinocandins, Pnuemocandins,Papulacandins) 2
GTP
UDPglucose
Catalytic subunitRegulatory Subunit (GTPase)
Continuous fibrils of Glucan
Fibrous (1,3) Glucan
Plasma Membrane (phospholipid bilayer)
Surface-Layer Mannoprotein
1-6 Tail1-6 BranchedGlucan
Entrapped Mannoprotein
Chitin
Plasma Membrane
Glycosyl Phosphatidylinositol “(GPI) Anchor” (to mannoproteins)
1,3) Glucan Sythase Enzyme Complex
1Adapted from: Kurtz, MB. ASM News. Jan 1998;64(1):31-9.2Chiou CC et al. Oncologist, 2000;5:120-35.
Ergosterol
Chitin Synthase
Candida, Aspergillus

• Inhibits b1-3 GS, active in growing Candida, Aspergillus hyphal tips and branches• Not active against organisms that don’t have b1-3 glucan
• Poor oral bioavailability• Long half-life (adult 9-11 hours) • Single daily dosing• Minimal renal clearance
• No dose adjustment for renal failure• Few toxicities
• Hepatotoxicities reported with CyA
CaspofunginCaspofungin
R2
OH
NH
N
OH
N
NH
NH
O
H
O
O
HO
NH
O
R5
OH
H
O OH
R4
O
NHH
R3
O
OH
H
H
H
HH
Fatty Acid
R1
H3C

CaspofunginCaspofunginCandidiasisCandidiasis
• Randomized, double-blind, multi-center, powered to show non-inferiority
• Stratified for disease severity and neutropenia, then randomly assigned to receive either
• IV caspofungin OR IV amphotericin B• minimum of 10 days of IV therapy required; antifungal
therapy continued for 14 days after last positive Candida culture
• The primary efficacy endpoint • overall (clinical and microbiological) response at the
end of therapy• Response unfavorable if study drug withdrawn before
improvementMora-Duarte J et al. N Engl J Med. 2002;347(25):2020-9.

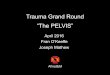
Caspofungin versus Amphotericin B for Caspofungin versus Amphotericin B for Invasive CandidiasisInvasive Candidiasis
0
20
40
60
80
100Caspofungin
Amphotericin B
Su
cce
ssf
ul o
utc
om
es
(%
)
73%73%62%62%
81%81%
65%65%
Analysis of all patients (non-stratified)
Successful outcome = symptom resolution and microbiological clearance
Modified ITT Evaluable patients
Mora-Duarte J et al. N Engl J Med. 2002;347(25):2020-9.

Any Problems With Caspofungin??
• Excellent safety record• Urinary tract infections? MIC’s with C. parapsilosis
- representation among persistent candidemia
- Relevant?• Resistance
- Large epidemiologic surveys – not a problem• However
- Resistance seen in few clinical isolates of C. albicans and C. parapsilosis
- Resistant in murine model

Treatment of Urosepsis Due to Candida spp.
1) Select systemic antifungal for Options:
• Polyene – AVOID!• Caspofungin• Voriconazole• Fluconazole• Flucytosine
2) Nephrostomy tube• Remove fungus ball/debris• Local infusion of AmB, azole, caspofungin• Remove obstruction