Embed Size (px)
Citation preview

NIDHI SHUKLA JUGLAN
TORCH INFECTION IN PREGNANCY

TORCH complex is a medical acronym for a set of perinatal infections, That can lead to severe fetal anomalies or even death.
They are a group of viral, bacterial, and protozoan infections that gain access to the fetal blood stream transplacentally via the chorionic villi.

T- toxoplasmosis
O- other infections
R- rubella
C- cytomegalovirus
H- herpes simplex II virus
Other infections- syphilis, varicella zoaster, parvovirus.

TOXOPLASMOSIS
Caused by protozoan intracellular parasite-toxoplasma gondii.
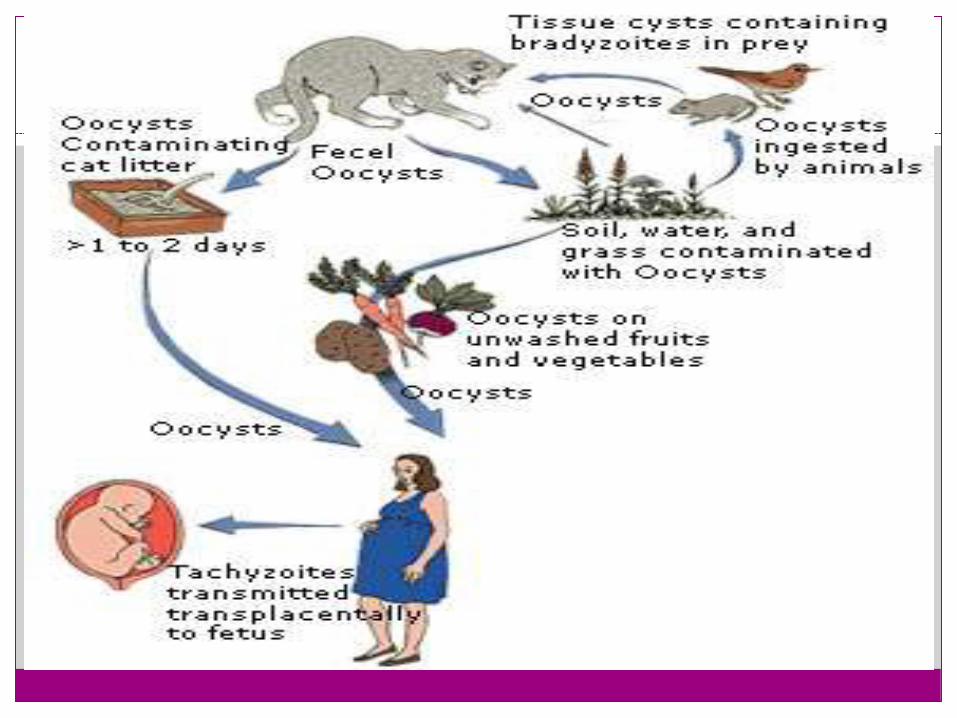
Modes of transmission – feco-oral route
by eating infected raw or cocked meat, or through contact with infected cat faeces.
Or through placenta.

Organism and transmission
T. gondii has three different forms
The definitive host is cat.
The oocytes produced the sporozites in the enteroepithilial cells of cat and passed into the faeces.
Sporozites become infected after 21 days of shedding.
Excystation in the human gut after ingestion of infected sporozytes.

Sporozytes circulates in maternal blood stream.
Trophozytes develop and multiply within the cells causes cell rupture and death.
Host immune response activated and begins third stage.
Host antibody formation reaction converts the parasites from the trophozites into tissue cyst form, and no longer circulate in blood to cause infection.
Fetal infections occurs only in acute phase of infection, when T. gondii in maternal blood transported to placenta and fetus.

Clinical manifestations
Acute toxoplasmosis is mostly subclinical.
Affects 0.3-1% of pregnant women, with an approximately 60% transmission rate to the fetus.
Risk Increases with gestation age.

Primary maternal infection in pregnancy-
Fetal death higher with infection in 1st trimester
Infection rate is higher with infection in 3rd
trimester.
Risk of fetal infection-
1st trimester- 15% ( decreases the incidence of infection but serious diseases are common, including abortion).
2nd trimester- 25%
3rd trimester- 65% ( 90% newborns are without clinical signs of infection.)
Maternal clinical manifestations
Most women are asymptomatic. Only about 10% of women have s/s during acute infection-
1. lymphoadenopathy- indicates recent infection, these are generally non tender, and nonsuppurative.
2. Other symptoms are flu like illness such as-
fever
fatigue
Headache
Muscle pain, sore throat.

Severe and rare symptoms are-
Polymyositis
Dermatomyositis
chorioretinitis
Fetal clinical manifestations
If acute toxoplasmosis is acquired during pregnancy, the infant is at the risk of developing congenital toxoplasmosis.
Clinical triad of signs associated with congenital toxoplasma infection is-
Chorioretinitis
Hydrocephalus
Intra cranial calcification.

Other symptoms –
Fever
Rash
Microcephaly
Siezures
Jaundice
Thrombocytopenia
Lymphoadenopathy

Diagnostic evaluation
Serological testing-
is done in the immunocompetent patient. Screening for the absence or presence of IgG or IgM specific antibodies is vital to make the diagnosis of acute toxoplasmosis in pregnancy.
Sabin- feldman dye test- indirect fluorescent antibody test detects the level of IgG antibody.
ELISA- to detect IgM.
Lymphnode biopsy
Ultrasound.

Investigation for detecting the fetal transmission-
Cordocentesis
Amniocentesis
USG for fetal triad.

Treatment
Self limiting.
Poorly respond to anti- microbial therapy.
Pregnant women-
Spiramycin 3 gm daily untill term.
Once fetal infection is established-
Sulfadiazine 1gm qid
Pyrimethamine 25 mg Po od (not in 1st trimes.)
Calcium folinate.
4-6 weeks course is given to the mother.

Prevention ??????????
RUBELLA
AKA german measels.
Caused by rubella virus ,a togavirus has single stranded RNA genome.
Transmitted by droplet infection.
Virus has teratogenic properties can cross the placenta where it stops cell development and leads cell death.
Risk of developing fetal anomalies is directly associated with maternal gestational age.

Incidences
1st trimester- 50% major fetal anomalies.
2nd trimester- 25%
3rd trimester- 10%
Spontaneous abortions occur upto 20% of cases. If infection occur within 20 wks of gestation.

Clinical manifestations
Maternal symptoms-
Same as other flu-
1. Rashes
2. Low grade fever
3. Lymphoadenopathy
( suboccipital, posti cervical)
1. Joint pain
2. Headache
3. Conjunctivitis
Congenital rubella syndrome
It is characterized by- Cochlear- sensorineural defects. Cardiac – septal defects, PDA, pulmonary arterial
hypoplasia. Neurological diseases- with a broad range of
presentation from behaviors to memingoencephalitis. Ostitis Hepatosplenomegaly. Microcephaly IUGR Cataracts Thrombocytopenia – blue berry muffin lesions.

Diagnostic evaluation
Serological test to detect rubella specific antibodies.
Routine rubella IgG is done in the first trimester
Rubella IgM is done in suspected case.
Presence of antibodies + rash = confirm the diagnosis.

Treatment
Prevention by active immunization.
No such treatment available.
Self limiting disease.
Maternal screening should be performed in early pregnancy.
In infection is present in pregnancy, mother could not be vaccinated because the rubella vaccine contained live virus which can cross the placenta and affect the fetus.
Infact women should not be vaccinated 28 days before conception.

Symptomatic treatment- analgesic and antipyretics.
Newborn should be managed for complications.

CYTOMEGALOVIRUS
CMV is a member of the herpes virus species.
Double strained DNA virus.
The virus most frequently passed on to fetus during pregnancy.
Acc to American academy of pediatrics about 1% of babies are born with the infection, a condition called congenital CMV.
Transmission- direct person to person contact (saliva, milk, urine, semen, tears, stools, blood, cervical and vaginal secretions).

Incidences
Primary vertical cmv infection caries a 30% - 40% risk of vertical transmission.
Among 30-40% , 2-4% develop severe malformations.
40000 infant per year in the US.

Clinical manifestations
Maternal symptoms-
Fever
Weakness
Swollen glands
Joint stiffness
Muscle ache
Loss of appetite.
Fetal symptoms-
90% are asymptomatic at birth
Petechiae, jaundice
Chorioretinitis
Periventricular calcifications.
IUGR, hearing loss
Microcephaly
Delayed psychomotor development
Heart block
Diagnostic evaluations
Serological testing- IgM are detected
Amniocentesis
Cordocentesis
USG
Fetal MRI ( rarely)

Treatment
No definitive Rx.
Pregnancy termination
Antiviral drugs-
1. Gangciclovir
2. Foscarnet
3. Cidofovir
Most effective drugs- hyper immune globulin.

HERPES SIMPLEX VIRUS-2 INFECTION
Most common STD worldwide.
DNA virus belongs to alpha herpes virinae family
Primary infection to mother can lead severe illness to mother in pregnancy.
The most common infection during pregnancy is primary genital HSV infection.

Effect on pregnancy
Transplacental infection is not usual.
Fetus become infected by virus shed from the cervix and vagina during vaginal delivery.
In utero transmission may occur in rupture of membraines.
Increased risk of abortion is inconducive.
IUGR if infection acquired in 3rd trimester.

Neonatal infections-
Chorioretinitis
MR
Seizures
Microcephaly
Deaths.

Treatment
CS indicated in primary HSV infection.
Suppressive viral therapy from 36 weeks untilldelivery, it includes-
Valacyclovir 500 mg PO bd
Acyclovir 400mg po tds. ( drug of choice)
Thank you





























