Embed Size (px)
Citation preview

THYROID AND CARDIOVASCULAR
DISEASESDr. I Tammi raju MD,DM.
Dept of cardiology.ASRAM hospital.

THYROID AND CVS
Case 1• A 25 year old female presented
with SOB cl II-III .– Pulse 70/min, – BP- 100/60.– Echo-large pericardial effusion , no
tamponade.– TSH- 33 mIU/mL.Recovered with thyroid correctionMild PE, BP-130/80.

THYROID AND CVS
Case 2• 65 year old presented with palpitaions
and NYHA class 4 breathlessness.– ECG- AF with FVR.– ECHO global hypokinesia , EF40%– TSH<0.01.
• Stabilised and sinus rhythm was restored with antithyroid medications.

THYROID AND CVS
OVERVEIW• Introduction• Hemodynamics • Hypothyroid and heart• Hyperthyroid and heart• Subclinical hypothyroid and
hyperthyroid • Amiodarone and heart.

THYROID AND CVS
INTRODUCTION• In ontogeny, the thyroid and heart
anlage migrate together.
• Thyroid gland and the heart share a close relationship that arises in embryology.

THYROID AND CVS
CARDIOVASCULAR HEMODYNAMICS

THYROID AND CVS
CARDIOVASCULAR HEMODYNAMICS
• Thyroid hormone effects on the heart and peripheral vasculature include
– decreased SVR and – increased resting heart rate, – Increase in left ventricular
contractility, and – blood volume

THYROID AND CVS
• Vascular resistance
• Thyroid harmone relaxes VSMCs, reduce peripheral vascular resistance.
• Hypothyroidism decreases EDRF, thereby increasing peripheral vascular resistance.
CARDIOVASCULAR HEMODYNAMICS

CARDIAC CONTRACTION SERCA PHOSPHOLAMBAN
SYSTEM
SERCA
Reuptake of calcium in early diastole
Phosphorylation of Phospholamban
relaxation of LV
inhibits SERCA
Contraction of LV
inhibitsT3
Cytosolic Calcium increase -- contractiondecrease-- relaxation
Ca++
Ca++

THYROID AND CVS
Diastolic function

THYROID AND CVS
• Herat rate• The pacemaker-related genes,
are transcriptionally regulated by thyroid hormone.
• Stimulation of -adrenergic receptors accelerates diastolic depolarization and increases heart rate.

THYROID AND CVS
• Basal metabolic rate • Thyroid hormone increases BMR in
almost every tissue and organ system in the body.
• This increased metabolic demands lead to changes in cardiac output, SVR, and blood pressure.

THYROID AND CVS
• Blood pressure• Hyperthyroidism:
– Arterial stiffness is increased– Typically causes systolic blood pressure
to rise– A widened pulse pressure
• Hypothyroidism:– Endothelial dysfunction and impaired
VSM relaxation lead to increased SVR.– lead to diastolic hypertension in 30% of
patients.

THYROID AND CVS
• Cardiac output• Increased • In hyperthyroidism, cardiac output 50%
to 300% higher than in normal individuals.
• In hypothyroidism, decrease by 30% to 50%.
• Restoration of normal cardiovascular hemodynamics can occur with treatment.

THYROID AND CVS
• Pulmonary Hypertension • Primarily in hyper thyroidism• The increase in cardiac output without the
concomitant decline in pulmonary vascular resistance observed in the systemic circulation.
• Some evidence exists that autoimmune disease may play a role in both hypothyroid- and hyperthyroid-linked cases of primary pulmonary hypertension.

EFFECTS OF THYROID HORMONE ON CARDIOVASCULAR HEMODYNAMICS.

CARDIOVASCULAR CHANGES WITH THYROID DISEASE

THYROID AND CVS
HYPOTHYROIDISM

THYROID AND CVS
HYPOTHYROIDISM• Major cardiovascular changes
– decrease in cardiac output – decrease in cardiac contractility – reduction in heart rate – increase in peripheral vascular resistance.
• Others– Hypercholesterolemia , – diastolic hypertension, – carotid intimal media thickness

THYROID AND CVS
• CLINICAL MANIFESTATIONS — • Exertional dyspnea and exercise
intolerance -due to skeletal muscle dysfunction.
• Cardiac dysfunction with poor contractility, dilatation
• Edema, often nonpitting

THYROID AND CVS
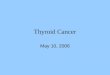
Rhythm • Bradycardia• Low QRS voltage• Widespread T-wave inversions (usually
without ST deviation)• QT prolongation-rarely Torsedes • First degree AV block• Interventricular conduction delay

THYROID AND CVS
• Mechanism• Myxoedematous deposits within
the myocardium.• Decreased activity of the sympathetic nervous system.• Effects on the myocardium of reduced levels of thyroxine (i.e. reduced inotropy/chronotropy)

THYROID AND CVS
Bradycardia (30 bpm) with Low QRS voltages (esp. in the limb
leads). and widespread T-wave inversions.
MYXOEDEMA

THYROID AND CVS
AFTER THERAPY
Rate- 70 bpm Disappearance of T-wave inversions.

THYROID AND CVS
PERICARDIAL EFFUSION•Pericardial effusions, in approximately 25% of patients and may be quite large. •Increased systemic capillary permeability and disturbances in electrolyte metabolism.• characterized by a high protein and cholesterol content.

THYROID AND CVS
• Lipid abnormalities and others:– Marked increase LDL and apo B-
• cholesterol 7-hydroxylase is negatively regulated by T3(decreased cholesterol catabolism)
– High Homocysteine – High Creatine kinase — The isoenzyme
distribution is almost completely MM,indicating skeletal muscle, not myocardial.

THYROID AND CVS
• Accelerated coronary artery disease .– Hypercholesterolemia – Diastolic hypertension, and – Elevated homocysteine levels– Elevated C-reactive protein and – Endothelial dysfunction
• Patients with angina pectoris probably have less symptoms as they are less active and peripheral oxygen demands decrease.

TREATMENT • In older patients or
those with a history of angina, begin therapy with a low dose of T4, as an example 12.5 or 25 mcg daily, because of the possibility of inducing an arrhythmia or an exacerbation of angina.
• If revascularization is indicated better to start T4 after the procedure.

THYROID AND CVS
HYPERTHYROIDISM

THYROID AND CVS
HYPERTHYROIDISM• Increases in
– heart rate – cardiac contractility, – systolic and mean pulmonary artery
pressure, – cardiac output, diastolic relaxation, and – myocardial oxygen consumption
• Reductions in – systemic vascular resistance and – diastolic pressure

THYROID AND CVS
• Tachycardia, at rest, during sleep, and exaggerated during exercise.
• Palpitations – tachy/forceful cardiac contractility• Hyperdynamic precordium.• Systolic hypertension with widened pulse
pressure • Exertional dyspnea, which is due to respiratory
and skeletal muscle weakness
Clinical features

THYROID AND CVS
• Means–Lerman scratch • Uncommon heart murmur which occurs in
patients with hyperthyroidism. • It is a mid-systolic scratching sound best
heard over the second left intercostal space at the end of expiration.
• Results from the rubbing of the pericardium against the pleura in the context of hyperdynamic circulation and tachycardia,
• Mimic the sound of a pericardial rub.

THYROID AND CVS
ANGINA PECTORIS• Increase in cardiac oxygen consumption,
due either to a – direct effect of triiodothyronine (T3) on
cardiac muscle or to an – increase in peripheral oxygen demand.
• Prinzmetal angina– In the young patient with normal
coronary anatomy, this may be due to coronary vasospasm .

THYROID AND CVS
RHYTHM• Atrial tissue is very sensitive to the
effects of thyroid hormone .• More
– APCs, – non-sustained SVT, – VPCs,
• Reduced heart rate variability

THYROID AND CVS
RHYTHMATRIAL FIBRILLATION
• 2% and 20%.• Associated with
– Male sex,– increasing age , >60yrs.– coronary heart disease. – heart failure.– valvular heart disease .
• subclinical hyperthyroidism -- same relative risk

THYROID AND CVS
ATRIAL FIBRILLATION

THYROID AND CVS
• Treatment of AF- – BB- beta1-selective or nonselective agent to
control the ventricular response– Digoxin- better avoid decreased sensitivity to
this drug– CCB- may lead to hypotension.
• Anticoagulation is controversial.– Increased vitamin K metabolism leading to an
increase in sensitivity to warfarin anticoagulation.
– Advancing age is the main risk factor– Asprin is effective safe alternative.

THYROID AND CVS
HEART FAILURE

THYROID AND CVS
HEART FAILURE • High output failure- not used these days• Factors responsible
– Exaggerated sinus tachycardia or – atrial fibrillation (rate-related) – Mitral valve prolapse (MVP)– MR
• Increased prevalence in Graves’ and Hashimoto’s diseases .
• Treated with BB and I 131.

THYROID AND CVS
PULMONARY HYPERTENSION
• PH has been reported with increasing frequency in patients with overt hyperthyroidism.
• Pulmonary artery pressures average twice normal values (10 mmHg) and may be as high as 30 to 50 mmHg.
• These changes reverse with treatment of the hyperthyroidism .

THYROID AND CVS
MOYAMOYA DISEASE • Characterized by anatomic occlusion of the
terminal portions of internal carotid arteries.• In these patients, treatment of the
hyperthyroidism can prevent further cerebral ischemic symptoms.
• This reinforces the importance of routine thyroid function tests (to include TSH) in patients who present with cardiac and cerebral vascular ischemic symptoms
» Im SH, Oh CW, Kwon OK, Kim JE, Han DH. Moyamoya disease associated with Graves disease: , J Neurosurg. 2005;102:1013–1017

THYROID AND CVS
SUBCLINICAL HYPO & HYPER THYROIDISM

THYROID AND CVS
SUBCLINICAL HYPOTHYROIDISM
• On TSH screening, the magnitude of subclinical thyroid disease may exceed that of overt disease by threefold to fourfold.

THYROID AND CVS
• Subclinical hypothyroidism alters – lipid metabolism, – atherosclerosis, – cardiac contractility, and – systemic vascular resistance
(endothelium-dependent vasodilation).• Presence of antithyroid antibodies
increases risk

THYROID AND CVS
• Patients with subclinical hypothyroidism have – prolonged isovolumic relaxation times, – systolic contractile function does not
change .
• Replacement with T4 at a mean dose of 68 μg/day (range, 50 to 100 μg/day) – restored isovolumic relaxation times to
normal, – systemic vascular resistance declined and – systolic function improved significantly

THYROID AND CVS
• Study from the U.K. General Practitioners data base showed that treatment of TSH levels between 5 and 10 mIU/mL lowered the incidence of ischemic heart disease events and cardiovascular mortality in patients younger than 70 years.

THYROID AND CVS
SUBCLINICAL HYPERTHYROIDISM
• Serum TSH level is low (<0.1 mIU/mL) and T4 and T3 levels are normal.
• The prevalence of atrial fibrillation after 10 years was 28% Vs 11% with a relative risk of 3.1.

THYROID AND CVS
• Therapy can be individualized with regard to three specific groups.
• The first group – excessive thyroid medication, needs
reduction of dose.• The second group
– Previous diagnosis of thyroid cancer who are receiving T4 to suppress TSH.
– younger patients -- beta blockers can useful– In older patients, lowering the T4 dosage .

THYROID AND CVS
• The third group – Endogenous thyroid gland overactivity,
including Graves disease or nodular goiter.
– Older patients are at risk for AF– Methimazole 5 to 10 mg/day – Consideration should be given to the
use of radioiodine for definitive therapy.

THYROID AND CVS
AMIODARONE AND THYROID FUNCTION

THYROID AND CVS
AMIODARONE AND THYROID FUNCTION
• Thyroid dysfunction in 60% of pts treated .
• Why– Amiodarone is an iodine-rich (30% iodine
content by weight)– structural similarity to levothyroxine
• Either– hypothyroidism (5% to 25% of treated
patients) or – hyperthyroidism (2% to 10% of treated
patients) in iodine-deficient areas.

THYROID AND CVS
AMIODARONE INDUCED HYPOTHYROIDISM(AIH)
100mg amiodarone 3mg iodine.
Risk factorsPreexistent thyroid disease. Hashimoto’s thyroiditis.
Inhibition of 5 -deiodinase activityInhibits T4 to T3
The average iodine content in diet is about 0.3 mg/day.
Directly inhibit thyroid gland function

THYROID AND CVS
TREATMENT of AIH
• Levothyroxine.
• Monitoring TFT regularly.

THYROID AND CVS
AMIODARONE-INDUCED THYROTOXICOSIS (AIT)
• Less common but perhaps more challenging.
• 2% to 10% and vary directly with duration .
• Onset was often sudden, during chronic treatment, or up to 1 year after stopping therapy.

THYROID AND CVS
• 2 forms of AIT exist.• Type 1 hyperthyroidism
– with preexistent thyroid disease and goiter.– more often in regions where iodine intake is low.
• Type 2 hyperthyroidism is caused by an – inflammatory process that causes increased
release of thyroid hormones from a previously normal thyroid gland.
• Sometimes Difficult to distinguish between them.

THYROID AND CVS
• TREATMENT OF TYPE I AIT:• Thionamides — may be slow response
and large doses may be required.• Surgery — Patients who are refractory
to antithyroid drug therapy should be treated by thyroidectomy.
• Radioiodine ablation - is usually not an option due to low radioiodine uptake in these patients as they are iodine excess in body.

THYROID AND CVS
• Caution:• Amiodarone appears to ameliorate
hyperthyroidism by blocking T4 to T3 conversion, beta-adrenergic receptors, and possibly T3 receptors.
• Amiodarone should not be discontinued until hyperthyroid symptoms are well controlled since worsening of hyperthyroid symptoms due to increased T3 levels.

THYROID AND CVS
• TREATMENT OF TYPE II AIT
• Glucocorticoids — • Patients with type II hyperthyroidism
respond well to moderately large doses of corticosteroids (eg, prednisone 40 to 60 mg/day) even if the amiodarone is continued.

THYROID AND CVS
Whether to continue amiodarone……
• Since the t1/2 is about 100 days, there is no immediate benefit on stopping amiodarone.
• Continue for life-threatening ventricular arrhythmias.
• If not for life-threatening ventricular arrhythmias discontinue if alternative can be used.

THYROID AND CVS
• Treatment if mechanism unknown /“Mixed”form:
• combinationof prednisone (40 mg/day) and methimazole (40 mg/day) is prudent initial therapy. – A rapid response suggests type II
hyperthyroidism; the methimazole can then be tapered or stopped and,
– A poor response initially argues for type I hyperthyroidism. If so, steroids can be tapered.

THYROID AND CVS

THYROID AND CVS
Changes in Thyroid Hormone Metabolism
That Accompany Cardiac DiseaseDecrease in serum T3.

THYROID AND CVS
• Low serum T3 level strongly predicts all-cause and cardiovascular mortality.
• In ACS Serum T3 levels fall by about 20% and reach a nadir after approximately 96 hours.
• Up to 30% of patients with heart failure have a low serum T3 level.
• In view of the deleterious effects of hypothyroidism on the myocardium, T3 replacement may provide benefit.

THYROID AND CVS
When to checkThyroid Function Testing
• Unexplained AF• Unexplained CHF• Pericardial effusion• Diastolic hypertension• On amiodarone every 3
months.• Hyperlipidemia• Critically ill patients.

THYROID AND CVS
When the Thyroid Speaks…the Heart
Listens”MA Sussman.,Circ. Res 2001
THANK YOU