Embed Size (px)
Citation preview


TB from Head to Toes
Presented by


*The increasing prevalence of
tuberculosis in both immunocompetent
and immunocompromised individuals
in recent years makes this disease a
topic of universal concern.
Introduction

*Because tuberculosis demonstrates
a variety of clinical and radiologic
findings and has a known propensity
for dissemination from its primary
site, it can mimic numerous other
disease entities..
Introduction


*The World Health Organization (WHO) estimates that each year more than 8 million new cases of tuberculosis occur and approximately 3 million persons die from the disease.
*Ninety-five percent of tuberculosis cases occur in developing countries.
*It is estimated that between 19 and 43% of the world's population is infected with Mycobacterium tuberculosis, the bacterium that causes tuberculosis infection and disease
Epidemiology


Epidemiology
Most cases in the US are due to reactivation,
especially amongst immigrants
Highest risk of progression to active TB is within 2 years of seroconversion
Increase in incidence in late 1980s-early 90s
largely due to HIV
Needs to be reported to the health department


Microbiology
Aerobic
Bacillus (rod-shaped)
Non-spore forming
Non-motile
Cell wall – mycolic acid – retains acid fast
stain
Growth - doubling time of 15-20 hrs.
3-8 weeks for growth on solid media

TB Skin Testing
PPD – purified protein derivative of tuberculin (antigenic)
Delayed type hypersensitivity reaction
PPD may not become “positive” until 3 months after exposure
Boosting effect





Skin Test Interpretation
PPD >/= 5 mm: – HIV patients
– Recent contacts of someone with TB
– Fibrotic changes on CXR c/w prior TB
– Organ transplant recipients
– Immunosuppressed (includes patients receiving the equivalent of 15 mg/day or more of prednisone for one month or more)

Skin Test Interpretation
PPD >/= 10 mm: – Recent immigrants (< 5 years) from high
prevalence areas (Eastern Europe, Latin America, Asia, Africa)
– IV drug users
– Residents and employees of high risk facilities (hospitals, nursing homes, homeless shelters, prisons)
– Children < 4 years of age
– Mycobacteriology lab personnel

Skin Test Interpretation
PPD >/= 10 mm:
– People with medical conditions that place
them at high risk for active TB
Chronic renal failure
Diabetes mellitus
Silicosis
Leukemias/lymphomas
Carcinoma of the head/neck or lung
Weight loss > 10% of ideal body weight
Gastrectomy/jejunoileal bypass

Skin Test Interpretation
PPD >/= 15 mm:
– Low risk people
– Routine tuberculin testing not
recommended for low risk populations

Skin Test Intrepretation
False positives: – Non-tuberculous mycobacterial infection
– BCG vaccination
False negatives: – HIV
– Malnutrition
– Steroid therapy
– Recent infection

BCG
Bacille Calmette-Guerin vaccination: Live attenuated mycobacterial strain derived
from M. bovis
Can yield false positives to PPD – less likely
as time from vaccination increases
Reactions > 20 mm likely are true
CDC advises that the PPD be interpreted by the same guidelines (ignore the BCG history)

Quantiferon Testing
Whole blood in vitro test: – Lymphocytes release IFN gamma in
presence of 2 TB antigens
Will be positive in latent or active TB
Advantages: – No error in interpretation
– No follow-up in 48-72 hours
– No boosting
– Not affected by BCG

Quantiferon Testing
Disadvantages: – Must be processed within 12 hours of
collection
– False + with atypical mycobacteria
– Too many indeterminate results with current version (Q-Gold)
– May be less reliable in pregnant women, children, and immunocompromised
– Does not distinguish between active and latent TB

Causative organism; Mycobacterium tuberculosis COMPLEX
Stained with:
-Modified gram stain: gram positive.
-Carbolfuchsin stain: *Cold method(Kynon)
*Hot(Zeil-Neelson)
- Fluorescent dyes: rhodamine and
auramine stains.
Bacteriology

QUANTITATION SCALE FOR ACID-FAST BACILLUS
SMEARS ACCORDING TO STAIN USED
Carbolfuchsin (× 1,000) Fluorochrome
(× 250) Quantity Reported
No AFB/300 fields No AFB/30 fields No AFB seen
1-2 AFB/300 fields 1-2 AFB/30 fields Doubtful, repeat
test
1-9 AFB/100 fields 1-9 AFB/10 fields Rare (1+)
1-9 AFB/10 fields 1-9 AFB/field Few (2+)
1-9 AFB/field 10-90 AFB/field Moderate (3+)
> 9 AFB/field > 90 AFB/field Numerous (4+)

Zeil-Neelson Staining
Wire 0.01 ml of specimen 200mm2 slide
Oil immersion field 0.02mm
Slide=10000 field=0.01ml specimen
10,000 organism/slide=1 AFB/field=1000,000 organism/ml
1000 organism/slide=1 AFB/10 field=100,000 organism/ml
100 organism/slide=1 AFB/100field=10,000 organism/ml

QUANTITATION SCALE FOR ACID-FAST BACILLUS
SMEARS ACCORDING TO STAIN USED
Carbolfuchsin (× 1,000) Fluorochrome
(× 250) Quantity Reported
No AFB/300 fields No AFB/30 fields No AFB seen
1-2 AFB/300 fields 1-2 AFB/30 fields Doubtful, repeat
test
1-9 AFB/100 fields 1-9 AFB/10 fields Rare (1+)
1-9 AFB/10 fields 1-9 AFB/field Few (2+)
1-9 AFB/field 10-90 AFB/field Moderate (3+)
> 9 AFB/field > 90 AFB/field Numerous (4+)

Cultures:
- Lowenstein Jensen media: 6-8
weeks.
-Bactec media: 2-8days. Radiolabelled 14c
labelled palmitic acid
-Mycobacterial growth indicator tube: Middbrook broth+o2 sensitive fluroscent sensor to
indicate growth& bacilli can be identified by Gen
Probe method at the same day of detection.

Diagnosis of Active TB
Acid fast stain of sputum
Sputum AFB culture (culture needed for drug susceptibility)
Radiographic imaging (CXR, CT)
PCR/NAT
Fluid Aspiration
Tissue biopsy – higher yield than fluid






Transmission
Transmitted by airborne particles 1-5 microns in size
Ease of transmission depends on duration and proximity of contact as well as the number of bacteria excreted
Infection can result from only 1-5 bacteria entering a terminal alveolus
Only those with active pulmonary TB are infectious

*M tuberculosis is transmitted via airborne
droplet nuclei that are produced when
persons with pulmonary or laryngeal TB
cough, sneeze, speak, or sing .
* Droplet nuclei may be produced by aerosol
treatments, sputum induction,aerosolization
during bronchoscopy, and through
manipulation of lesions or processing of
tissue or secretions in the hospital or
laboratory.

Pathogenesis
– Inhalation -> phagocytosis by alveolar macrophages
– Bacterial multiplication occurs intracellularly
– Lymphatic spread to regional lymph nodes or
hematogenous dissemination
– Immune response results in granuloma formation (containment of infection)
– Cell death in the granuloma results in caseous
necrosis
– Bacteria can remain dormant in the granuloma


Pathogenesis
– Medical conditions that increase risk for
active TB:
Chronic renal failure
Diabetes mellitus
Silicosis
Leukemias/lymphomas
Carcinoma of the head/neck or lung
Weight loss > 10% of ideal body weight
Gastrectomy/jejunoileal bypass



Primary pulmonary tuberculosis
*The first infection with tubercle bacillus.
Includes the involvement of the draining
lymph nodes in addition to the initial
lesion(Ghon).

Clinical features:
Majority: symptomless.(specially in
young adults)
Brief febrile illness.
Loss of appetite.
Failure to gain weight in children.
Cough is not unusual and may mimic
paroxysm of whooping cough.

Physical signs:
•May be normal,
•Crepitation may be heard.
•Primary lesion could be
heard.
•Segmental or lobar collapse
may occur.

Radiological features: •Lymphadenoathy: hilar lymph nodes
are most commonly involved rarely
paratracheal.Calciflcation of the nodes
may occur.
• Pulmonary componant: ( mainly in
adults) segmental or lobar
consolidation or obstructive
emphysema.
•Resolution of radiological shadow 6m-
2ys.

Diagnosis: *Vague ill health with history of contact.
* X-ray.
*Tuberclin test: is usually strongly
positive.
*Sputum and gastric lavage for direct
smear and culture helpful in 20-25% of
cases.
* DNA amplification: PCR.

Primary pulmonary tuberculosis
Primary pulmonary TB typically
manifests radiologically as parenchymal
disease, lymphadenopathy, pleural
effusion, miliary disease, or lobar or
segmental atelectasis.

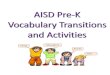
Consolidation in primary tuberculosis. Frontal chest radiograph
demonstrates consolidation in the right middle lobe (straight
arrow) with right hilar adenopathy (curved arrow).

Tuberculomas in primary
tuberculosis. Frontal X-ray
of the right lung
demonstrates well-defined
nodules(arrows), findings
that are consistent with
tuberculomas.

Pulmonary parenchymal changes and lymphadenopathy in primary
tuberculosis. Axial contrast material–enhanced computed
tomographic (CT) scan demonstrates a parenchymal lung cavity in
the lingula (solid white arrow) with enlarged necrotic subcarinal
lymph nodes (black arrows). There is accompanying collapse of
the left lower lobe (open arrow).

Mediastinal TB adenopathy.Axial contrast-enhanced CT
scan demonstrates multiple enlarged mediastinal lymph
nodes with centralareas of low attenuation and peripheral
enhancement (arrows).

Pleural effusion. Axial contrast-enhanced CT scan
demonstrates a large, right-sided pleural collection.The
enhancing parietal pleura is uniformly thickened (arrows).

Miliary tuberculosis. Frontal radiograph shows
fine, discrete nodular areas of increased opacity
bilaterally.

Miliary tuberculosis. High-resolution CT scan obtained with
lung windowing demonstrates numerous fine, discrete nodules
bilaterally in a random distribution


Post primary pulmonary tuberculosis
The most important type of tuberculosis
because it is the most frequent and
smear positive sputum is the main
source of infection responsible for the
persistence of the disease in the
community.

Source;
1. Direct progression of the primary
lesion.
2. Reactivation of the quiescent primary
or post primary.
3. Exogenous infection.

Predisposing factors for reactivation:
1. Malnutrition.
2. Poor housing and overcrowding.
3. Steroid and other immunosuppressive
drugs.
4. Alcoholism.
5.Other diseases: HIV malignancy,
lymphomas , Leukaemia,Diabetes.

Clinical features:
Mainly in middle aged and elderly.
A-Symptoms: 1. May be no symptoms, or just mild debility.
Gradual onset of symptoms over weeks or months.
2. General malaise.
3. Loss of appetite, loss of weight.
4. Febrile course.
5. Night sweating.
6. Cough with or without sputum.
7. Sputum could be mucoid, purulent or blood stained.
8. Could be presented with frank haemoptysis.
9. Tuberculous pneunonia.

B-Signs: 1. May be no signs.
2. Pallor, cachexia.
3. Fever.
4. Post tussive crepitations on the apices.
5. Signs of Consolidation.
6. Signs of fibrosis.
7. Signs of cavitary lesion.
8. Localised wheezes in endobronchial
tuberculosis

Postprimary Tuberculosis
Postprimary disease results from reactivation of a
previously dormant primary infection in 90% of cases;
in a minority of cases, it represents continuation of the
primary disease . Postprimary tuberculosis is almost
exclusively a disease of adolescence and adulthood.

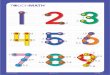
Cavitary postprimary tuberculosis. (Frontal radiograph
demonstrates a thick-walled cavity with smooth inner
margins in the left upper lobe (arrow).

Axial contrast-enhanced CT scan obtained with mediastinal
windowing demonstrates an enlarged mediastinal lymph node
with a central area of low attenuation (arrow).

Axial CT scan obtained with lung windowing demonstrates ill-
defined cavities (black arrows) accompanied by endobronchial
spread in the right upper lobe (white arrow).

Fibroproliferative disease. Axial CT scan
demonstrates bilateral diffuse, coarse, linear, and nodular
areas of increased attenuation with cavitation (arrows).

Lung destruction in postprimary tuberculosis. Axial CT scan
demonstrates a fibrotic, shrunken left lung with
compensatory overexpansion of the right lung extending
across the midline. Bronchiectatic changes are
noted bilaterally (arrows).

Bronchiectasis in postprimary tuberculosis. Axial CT scan
demonstrates bronchiectasis in the left lung (arrows) with areas of
emphysema.

Fibroproliferative disease. Frontal chest radiograph shows
clumped nodular and linear areas of increased opacity in both
upper lobes and in the right middle lobe (white arrows). There
is accompanying volume loss in the right upper lobe as well as
overlying apical pleural thickening (black arrow).

Cavitary tuberculosis associated with aspergilloma. Frontal radiograph shows a
cavity in the left upper lobe (black arrow) with a dependent area of soft-tissue
opacity (solid white arrow). The crescentic area of hyperlucency (open arrow)
represents residual air in the cavity and is referred to as the air crescent sign.
Axial CT scan shows dependent soft-tissue aspergilloma (black arrow) within
the cavity (solid white arrow), along with the air crescent sign (open arrow).

Endobronchial spread of tuberculosis.
Axial CT scan shows severe changes of bronchiolar dilatation
and impaction. Bronchiolar wall thickening (straight arrows) and
mucoid impaction of contiguous branching bronchioles produce a tree-
in-bud appearance (curved arrows).

Tuberculous broncholithiasis. Chest radiograph demonstrates partial atelectasis
of the right upper lobe (straight arrow) with calcified hilar lymph nodes
bilaterally (curved arrows). Axial CT scan demonstrates erosion of the right
main bronchus (straight solid arrow) by a calcified hilar lymph node (curved
arrow). A calcified precarinal lymph node is also noted (open arrow). The
differential diagnosis for mediastinal lymph node calcification includes
histoplasmosis, silicosis, and treated lymphoma.

Tuberculous bronchostenosis.
Axial CT scan demonstrates
narrowing of the right main
bronchus (arrow).

Tuberculous involvement of
the left sternoclavicular
joint. Oblique radiograph
demonstrates irregularity
of the medial end of the left
clavicle (black arrow)
with an associated soft-tissue
mass (white arrow).

Plombage in a patient with postprimary tuberculosis. Frontal chest
radiograph demonstrates typical right-sided Lucite ball plombage.
There is thinning and disorganization of the overlying ribs (straight
arrow). Air-fluid levels in the Lucite balls (curved arrows) suggest
bronchopleural fistulas.

Radiology: 1. Bilateral upper zone fibrotic shadows: with
shift of trachea, mediastinum, distortion of
fissures and diaphragm, and elevation of the
pulmonary hila.
2. Soft confluent shadows of exudative lesion
(D.D pneumonia)
3 Calcification.
4. Cavitation.
5. Tuberculoma.
6. Hilar and paratracheal lymph node
enlargement may be present.

Radiological classification: 1.Minimal: slight or moderate opacity. No
cavity. Extent not more than space
above 2nd costocondral junction.
2. Moderately advanced: In one or both
lungs. slight or moderate opacity, extent
equivalent to volume of one lung. Dense
confluent shadow equivalent to one third
the volume of one lung. Diameter of
cavities not more than 4 cm.
3. Far advanced:
Any lesion>the moderately advanced.

Diasnosis: 1) Clinical
2) Plain X-ray.
3) Sputum Examination: direct smear and culture (very
important).
4) Other samples: Gastric aspirate, laryngeal swab, fiberoptic
specimens (wash,brush,biopsy),transtracheal spirate.
5 Polymerase chain reaction.)
6) Tuberclin test: mainly strongly positive
7) Others
White blood cells if normal favour the diagnosis
ESR may be elevated.
Normocytic normochromic anaemia.
CT may be useful in detecting small cavities,
or calcification.


Miliary Tuberculosis
Produced by acute dissemination of tubercle
bacilli via the blood stream.The term miliary
derives from the radiological picture of
diffuse, discrete nodular shadows about the
size of millet seed (2mm).

A- Classical form: Clinical features: Most common in infants and young children with acute
or subacute febrile illness.
In adults: the onset is insidious, gradual vague ill health.
Malaise, Cough (usually dry), dyspnea. Night sweat is
less common.
Headache suggest associated tuberculous meningitis
Chest examination is free, crepitations may be found.
Hepatomegaly, splenomegaly, lymphadenopathy,
neck rigidity may be found in rare cases.

Diasnosis: 1) Clinical.
2) Xray.
3) Choroidal tubercles in fundus examination
4) Tuberclin test not conclusive
5) Direct smear and culture of sputum if
present.
6) Other samples as transtracheal aspirate,
fiberoptic specimens may be obtained.
7) If failed to prove therapeutic trial for 2
weeks



















Cardiac Tuberculosis
Although tuberculosis rarely involves the heart
pericardial involvement may occasionally be
seen with mediastinal and pulmonary
tuberculosis and is a cause of calcific
pericarditis (

Tuberculoma of the right atrium in a patient with miliary tuberculosis. Axial T2-weighted
magnetic resonance (MR) image demonstrates a hyperintense mass in the right atrium (straight
arrow). Note also the right pleural effusion (curved arrow). The mass proved to be a
tuberculoma at surgery. Tuberculous pericarditis in a patient with pleuropulmonary
tuberculosis. Axial CT scan demonstrates pericardial thickening (straight solid arrow).
Pulmonary tuberculomas (curved arrows) and a right pleural effusion (open arrow) are also
seen.

Skeletal Tuberculosis
Tuberculous Spondylitis (Pott Disease)
The spine is the most frequent site of osseous
involvement in tuberculosis , with the upper lumbar
and lower thoracic spine being involved most
frequently. More than one vertebra is typically
affected, and the vertebral body is more commonly
involved than the posterior elements. An anterior
predilection is seen in the vertebral body

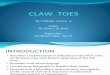
Tuberculous spondylitis. Lateral radiograph demonstrates obliteration of the disk
space (straight arrow) with destruction of the adjacent end plates (curved arrow)
and anterior wedging. Subligamentous spread of spinal tuberculosis. Lateral
radiograph demonstrates erosion of the anterior margin of the vertebral body
(arrow) caused by an adjacent soft-tissue abscess.

Tuberculous spondylitis. Axial CT scan demonstrates lytic
destruction of the vertebral body (black arrow) with an
adjoining soft-tissue abscess (white arrow).

Iliopsoas abscess. Axial CT scan demonstrates
large, multiloculated iliopsoas abscesses
bilaterally (arrowheads). Note also the presacral
abscess (solid arrow) accompanied by erosion of
the anterior sacrum (open arrow).

Calcified psoas abscess. Axial CT scan
demonstrates bilateral tuberculous psoas
abscesses with peripheral calcification (arrows).

Extraspinal Tuberculous
Osteomyelitis
Tuberculous osteomyelitis is usually hematogenous
in origin and is most commonly seen in bones of
the extremities, including the smallbones of the
hands and feet. In long, tubular bones, tuberculosis
often involves the epiphyses.In children,
metaphyseal foci can involve the growth plate. This
feature differentiates tuberculosis from pyogenic
infection

Tuberculous osteomyelitis involving the skull. Axial contrast-
enhanced CT scan demonstrates a bilobed, peripherally
enhancing cold abscess centered along the right frontal bone
(arrow, arrowhead). Note the significant edema and the mass
effect on the underlying brain parenchyma. Axial CT scan
obtained with bone windowing demonstrates an ill-defined
lytic area of bone destruction (arrow).

Tuberculous spondylitis. Sagittal T2-weighted MR
image demonstrates areas of increased signal
intensity due to edema in vertebral bodies.
Accompanying disk narrowing (white arrow) and
extension of the disease into the spinal canal (black
arrow) are also seen.

Tuberculous osteomyelitis. Anteroposterior radiograph
demonstrates a lytic area of bone destruction (arrow) with
transphyseal spread of infection across the growth plate.

Tuberculous arthritis of the knee joint. Frontal radiograph
demonstrates periarticular osteopenia (black arrow), peripheral
osseous erosions (white arrow), and relative preservation of the
joint space. Tuberculous arthritis of the knee joint. Sagittal
gadolinium-enhanced T1-weighted MR image demonstrates
peripheral enhancement around the low-signal-intensity joint
collection (straight arrow). Note the presence of marginal joint
erosions (curved arrow).

Gastrointestinal Tuberculosis
Although abdominal tuberculosis is usually
secondary to pulmonary tuberculosis,
radiologic evaluation often shows no evidence
of lung disease
Ileocecum and Colon The ileocecal region is the most common area of
involvement in the gastrointestinal tract due to
the abundance of lymphoid tissue. The natural
course of gastrointestinal tuberculosis may be
ulcerative, hypertrophic, or ulcerohypertrophic

Ileocecal tuberculosis.
Radiograph obtained
with peroral
pneumocolon technique
demonstrates a conical
and shrunken cecum
(straight arrow)
retracted out of the iliac
fossa by contraction of
the mesocolon. Note also
the narrowing of the
terminal ileum (curved
arrow).

Ileocecal tuberculosis. Axial CT scan demonstrates concentric cecal
wall thickening (arrow). Axial CT scan obtained caudad to a
demonstrates diffuse thickening of the terminal ileum (arrow).
Ileocecal tuberculosis and peritoneal tuberculosis (wet type). Axial
CT scan demonstrates concentric thickening of the cecum (straight
solid arrow). Small bowel dilatation (curved arrow), ascites in the
greater peritoneal space, and thickening of the peritoneum
(open arrow) are also seen.

Peritoneum Peritoneal involvement in tuberculosis is rare and is
usually associated with widespread abdominal
disease involving lymph nodes or bowel .Three
principal types of tuberculous peritoneal
involvement are recognized. The wet type is the
most common and is associated with large amounts
of viscous ascitic fluid that may be either diffusely
distributed or loculated .The fluid demonstrates high
attenuation at CT due to its high protein and cellular
content .The dry or plastic type is uncommon and is
characterized by caseous nodules, fibrous peritoneal
reaction, and dense adhesions

The fibrotic fixed type (consists of large omental
masses, matted loops of bowel and mesentery,and,
on occasion, loculated ascites .CT may also
demonstrate tethering of bowel loops. Infiltration
of the mesentery, when associated with a large
amount of ascites, may have a stellate appearance
at CT.

Peritoneal tuberculosis (dry type). Axial CT scan
demonstrates thickening and infiltration of the
peritoneum (white arrows) along with thickening
of bowel loops. Note the small amount of loculated
fluid (black arrow).

Peritoneal tuberculosis (fibrotic type). Axial contrast-enhanced
CT scan demonstrates enhancing thickened peritoneum
(straight arrow) with an adjoining matted loop of small bowel
(curved arrow).

Abdominal tuberculous lymphadenitis. Axial contrast-enhanced CT scan demonstrates multiple
enlarged mesenteric lymph nodes with central areas
of low attenuation (arrow).

Hepatic tuberculosis.
Axial contrast-enhanced
CT scan demonstrates multiple nonuniform,
low-attenuation lesions within the liver (straight arrows).
An enlarged gastrohepatic lymph node is also
seen (curved arrow).

Tuberculous
pyonephrosis.
Retrograde pyelogram
shows filling of the dilated
hydronephrotic lower and
middle pole of the right
kidney. The collecting
system has irregular
margins (straight solid
arrow) and shows
irregular filling defects
(curved arrow) from
necrosis of the
parenchyma. Upper pole
calcification is also seen
(open arrow).

Renal tuberculosis. Chest radiograph that includes
the upper abdomen
demonstrates lobar
calcification in the right kidney
(black arrow). Note also the
bilateral fibrocalcific changes
in the upper lobes (white
arrows).

Renal tuberculosis Axial contrast-enhanced
CT scan demonstrates left tuberculous pyonephrosis
(straight solid arrow) with extension of the inflammatory
process into the perinephric space (curved arrow)
and accompanying peritoneal disease (open arrow).

Adrenal tuberculosis. Axial contrast-enhanced
CT scan demonstrates bilateral adrenal masses
with central low-attenuation areas (arrows).

Bladder tuberculosis.
Axial contrast-enhanced CT scan demonstrates a thickened and
deformed bladder with an enhancing wall (straight arrow). There is
extension of the inflammatory process to the anterior abdominal wall
(curved arrow). Intravenous urogram demonstrates a thickened,
contracted, low-capacity bladder (thimble bladder) (arrowhead) with
minimal dilatation of both ureters.

Endometrial tuberculosis.
Hysterosalpingogram demonstrates an obliterated
and deformed endometrial cavity (arrow)
due to tuberculous endometritis.

Cranial tuberculous meningitis. Axial gadolinium-enhanced T1-weighted MR image demonstrates leptomeningeal
enhancement along the left sylvian fissure (straight arrow). There is an
accompanying ring-enhancing granuloma in the left parieto-occipital region
(curved arrow).

Cranial tuberculomas Axial contrastenhanced CT scan demonstrates multiple
ring-enhancing lesions (straight arrows) along with
diffuse meningeal enhancement (curved arrow).

Solid caseating tuberculous granulomas involving the
cerebellum. Axial T2-weighted MR image demonstrates
multiple granulomas with central areas of hypointensity in
the cerebellum (arrows). Tuberculous granulomas involving
the cerebellum. Axial T1-weighted MR image demonstrates
isointense lesions with mildly hyperintense rims in the
cerebellum (arrows).

Bilateral tuberculous mastoiditis.
Highresolution CT scan of the temporal bone demonstrates
bilateral destructive lesions in the mastoid processes (straight
arrows). There is an accompanying cold abscess overlying
the right temporo-occipital region (curved arrow).

Orbital tuberculosis.
Axial contrast-enhanced CT scan demonstrates
an enhancing retinal lesion in the left orbit
(arrow).

Conclusions Tuberculosis can affect virtually any organ system in the
body and can be devastating if left untreated. The
increasing prevalence of this disease in both
immunocompetent and immunocompromised individuals
makes tuberculosis a topic of universal concern.
Tuberculosis has a variety of radiologic appearances and
can mimic numerous other disease entities. A high degree
of clinical suspicion and familiarity with the various
radiologic manifestations of tuberculosis allow early
diagnosis and timely initiation of appropriate therapy,
thereby reducing patient morbidity.