Embed Size (px)
Citation preview

Dangerous Fever in Adult
1
Tipa Chakorn, MD. Emergency Medicine Unit
Department of Medicine, Siriraj Hospital

2
3

4

• Dangerous for whom?
– Patient
– Medical personnel
– Hospital
– Community
• Causes of dangerous fever?
– Infectious cause
– Non-infectious cause
5

• Dangerous condition
– Life threatening or mortality
– Morbidity
• Treatable or preventable condition
• Common condition
6

• Common disease in Thailand
• High mortality and morbidity
– Overall mortality 20-27%
– Old age 40%
• Morbidity and mortality can preventable
7

8

• Classic triad
– Fever
– Stiffness of neck
– Alteration of consciousness
• Gold standard: Culture positive in CSF
9

N Engl J Med 2004;351:1849-59.10
11
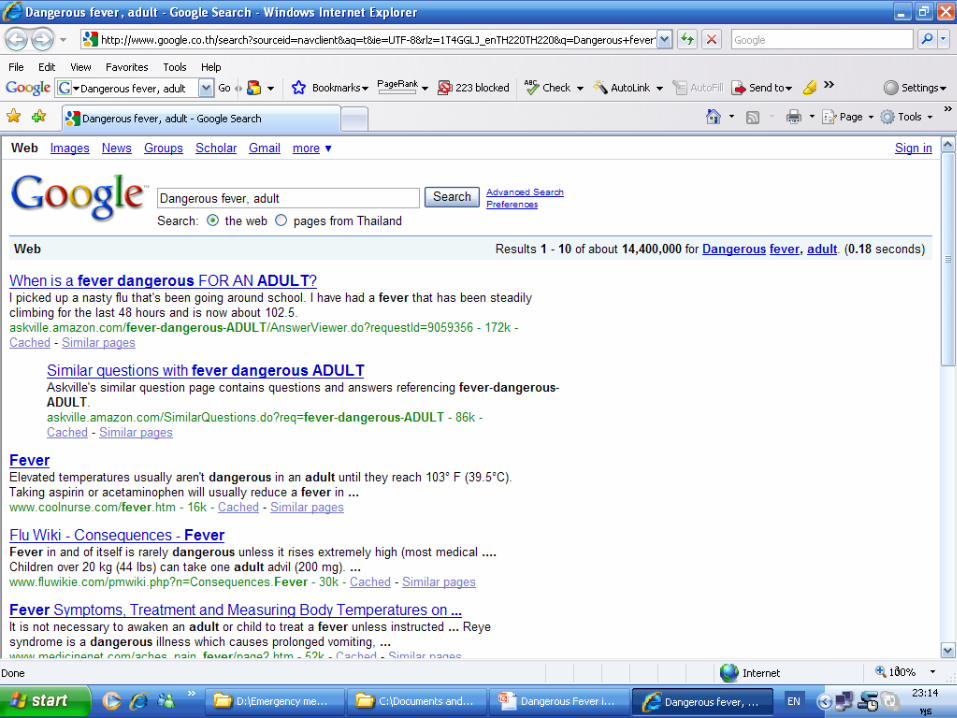
Netherlands: October 1998-September 2002
– 696 patients with Community-acquired acute bacterial
meningitis
– Sensitivity of classic triad 44%
– At least 2 of 4: Classic triad + headache = 95%
– Overall mortality rate 21%
(S.pneumonae>N.meningitides)

Songklanagarind Hospital, Thailand
• Retrospective study: Jan 1982-Dec 2001
• 180 episodes in 161 cases
• Both community and nosocomial bacterial
meningitis
• Classic triad of symptoms: 62.5%
• 100% had at least 1 of 3 finding
Southeast Asian J Trop Med Public Health.2004;35:886-92 12

13
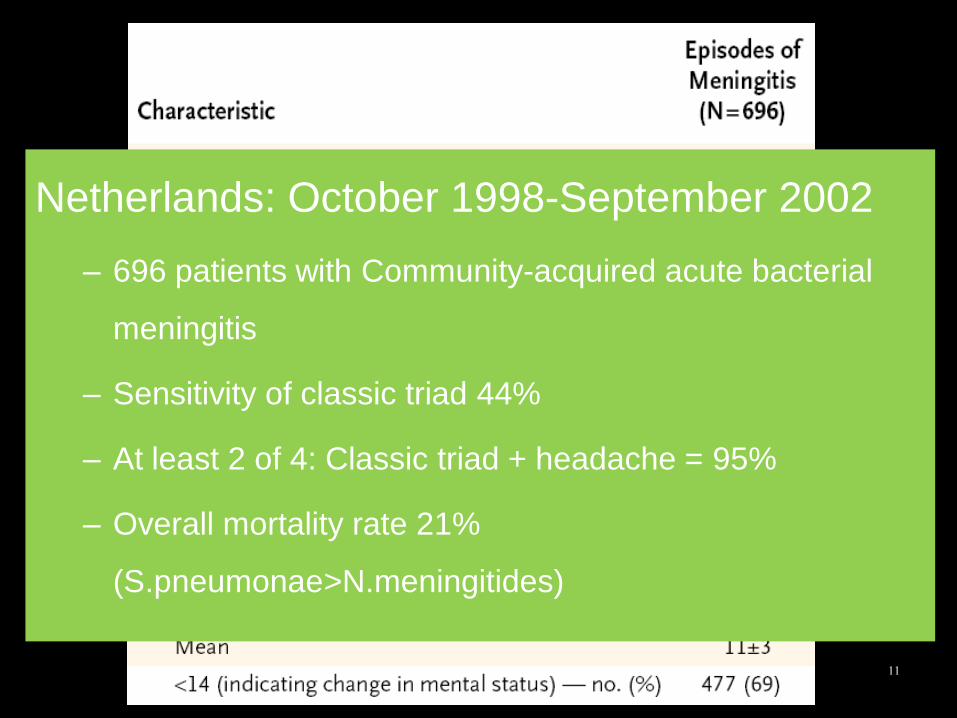
Meta-analysis
• Pooled sensitivity for headache =50%
[95% CI, 32%-68%]
• Nausea/vomiting, 30% [95% CI, 22%-38%])
• The absence of fever, neck stiffness, and
altered mental status effectively eliminates meningitis (sensitivity= 99%-100%)
14JAMA 1999;282(2):175-81

สรปไดวา1. เนองจากเปนโรคทมอตราการเสยชวตสง ดงนน ควร
เลอกใชการวนจฉยทมความไวสงกอน
2. การใช Classic triad ครบทง 3 ขอในการวนจฉยโรค ไมมความไวเพยงพอ
3. ผปวยทมอาการ 2 ใน 4 ของไข ปวดศรษะ คอแขง หรอความรสกตวเปลยนแปลง มโอกาสสงทจะเปนโรคน
4. โอกาสทผปวยโรคนจะไมมไข หรอ คอแขง หรอ ความรสกตวเปลยนแปลงมนอยมาก
15
16

• Kernig’s sign
• Brudzinski’s sign
• Nuchal rigidity
17

• First described in 1880: Yugoslav
• Kernig; 1882
• 1st performed in patient sitting positionextend knee
Mechanism
• Flexion of neck-> spinal cord moves upward about 1
cm in lumbar region -> pain causes resistance to
further movement
• The stretch can be mechanical relieved by flexion at
hip and knee
18

19

• Do not check for meningitis by flexing the neck in
an unconscious patient unless head and neck
trauma has been excluded
• In caution with posterior fossa mass lesion
• False negative: Localized inflame/low inflam
meningtis
• False positive: Other disease of spinal cord, RA,
20

Signs Sensitivity Specificity
Kernig’s sign 5% 95%
Nuchal rigidity 30% 68%
Jolt accentuation 97% 60%
21
15%
9%Brudzinski’s sign

• ไมมการตรวจรางกายทไว และมความจ าเพาะกบโรคเยอหมสมองอกเสบ
• การใชการตรวจรางกายหลายๆ อยางพรอมกนจะชวยเพมความไวในการวนจฉยโรคนได
• ในผสงอาย การตรวจตางๆเหลานมความไว ลดลง
22

23

CT brain: benefit or risk?
• Consciousness
• Papilledema
• Neurological deficit
• Delay LP
• Delay treatment
• Increase mortality
24
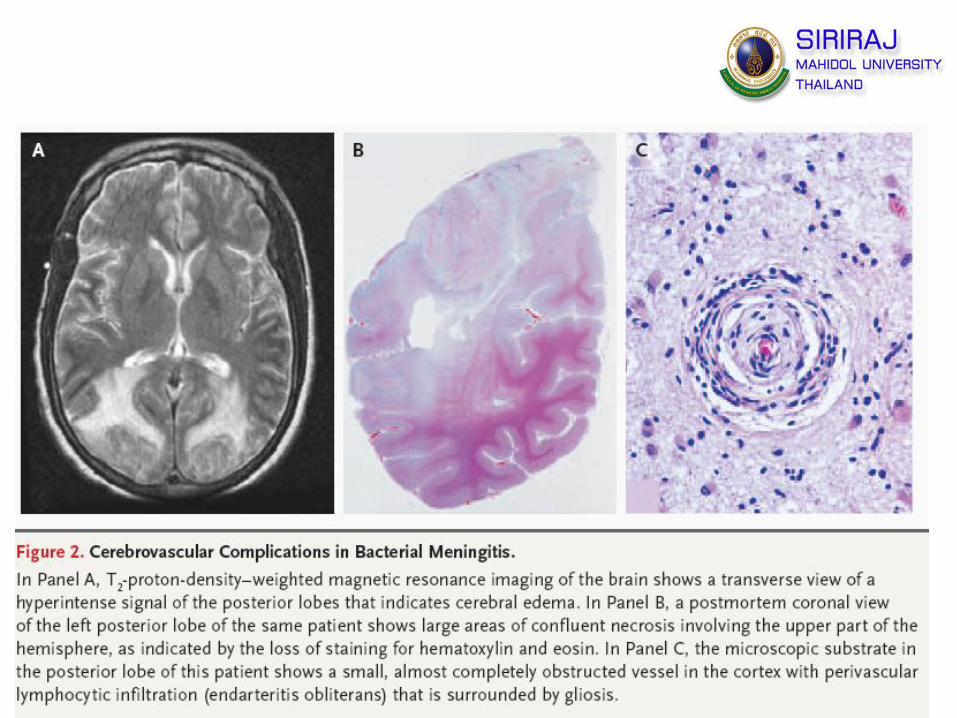
Brain Herniation?

Complication of meningitis
25
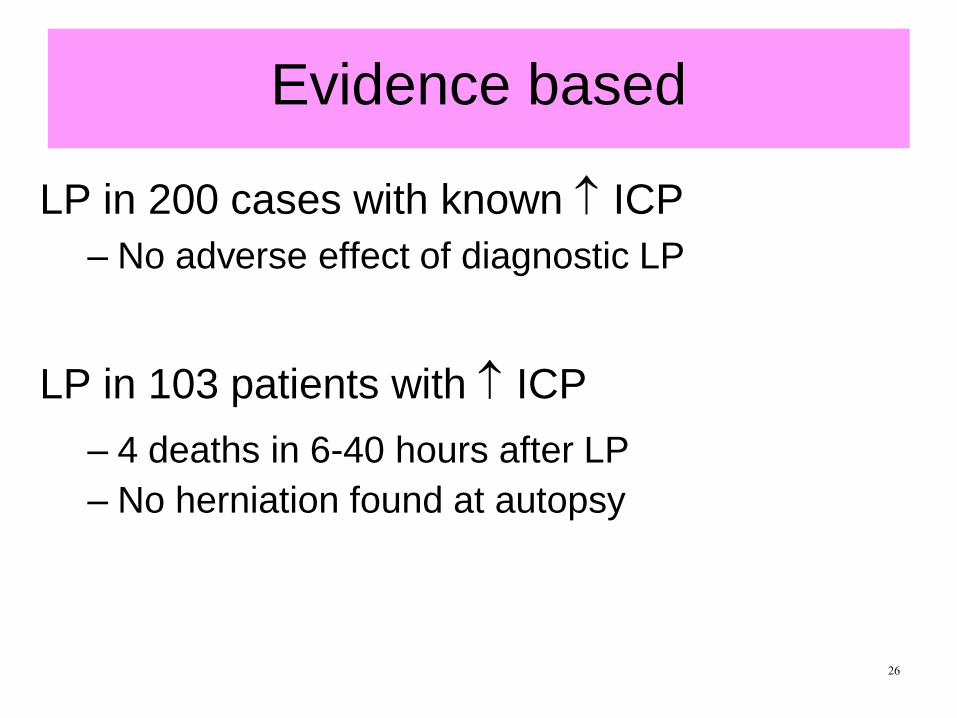
Evidence based
LP in 200 cases with known ICP
– No adverse effect of diagnostic LP
LP in 103 patients with ICP
– 4 deaths in 6-40 hours after LP
– No herniation found at autopsy
26

Prospective study
• 301 adults with suspected meningitis
• 235 CT scan were done
• Compare baseline characteristic between
normal and abnormal CT brain
N Engl J Med 2001;345:1727-33.

28
Asociations between baseline clinical characteristics and abnormal finding
on CT of the Head in 235 adults with suspected meningitis

29

30Q J Med 2005; 98:291–298
Retrospective case record study: Canada
• 123 cases of adult acute bacterial meningitis
• Jan 1990-March 2002
• Association between mortality and door to
ATB time
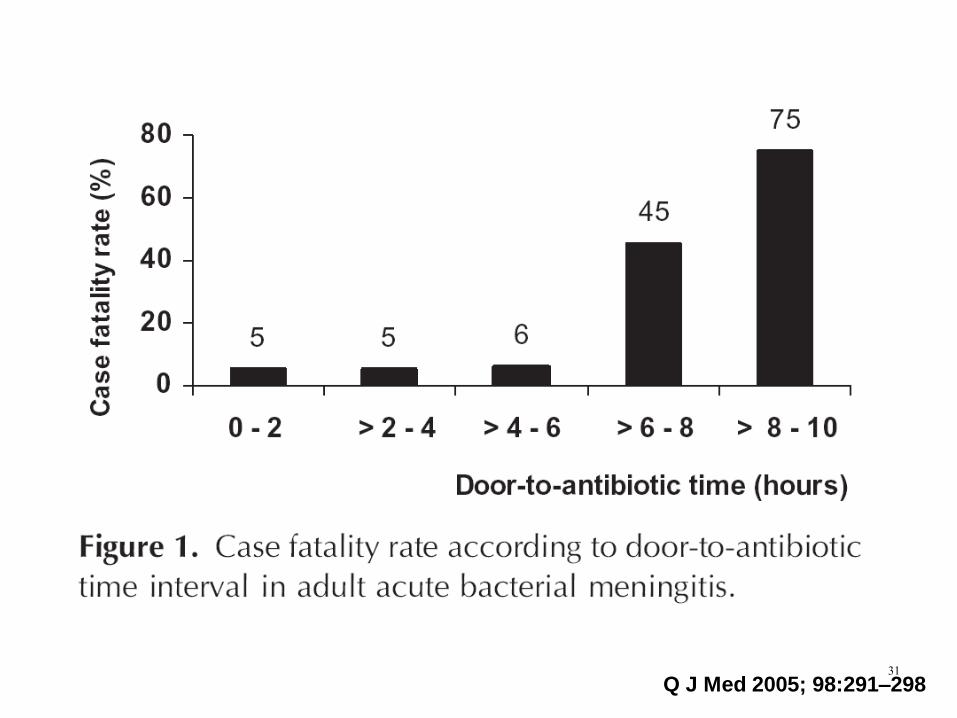
31Q J Med 2005; 98:291–298

32

• Considered with indication
• Antibiotics should be started before CT
33

34

LP data
• Opening Pressure
– Important data
– Only in lateral decubitus (not position usually done under radiology)
• Xanthochromia
– Yellow/orange color of centrifuged CSF
– RBC lysis – oxyhemoglobin, bilirubin
– Blood in subarachnoid space at least 2-4 hrs
– More likely due to blood in CSF and less likely traumatic tap

CSF analysis
Correction factors for traumatic tap
– “Trauma” and RBCs increase protein and with
an increase in RBCs come an increase in
WBCs
– True CSF protein = subtract 1 mg/dL protein for
every 1000 RBC/mm3
– 1 WBC/mm3 for every 700 RBC/mm3

CSF Findings
Normal Bacterial Viral Fungal TB
WBC
(TNC)
0-5 100-10,000 5-3000 5-500 5-500
Cell type >50% PMN >50% lymphs
>50% lymphs
>50% lymphs
Protein 50-80 mg/dL
>200 Nl/slight increase
Nl/slight increase
Increase
Glucose 70-80 mg/dL
>60% serum
<40, <60% of serum glucose
Normal normal <40 or nl
Gm stain 60% + Neg 50% indiaink + crypto
AFB + 25-35%
Pressure 75-200 mm Hg
Inc Nl Inc Nl/inc

CSF analysis
• Gram stain
• AFB stain
• Culture
38

Limitation
• Post treatment
– Culture may be negative after few hours
– Decreased positive Gram stain
• Follow up LP
– Mostly recommend few days after treatment if
the clinical does not response well
– CSF sugar: 1st change
39

40

41Q J Med 2005; 98:291–298

42

Recommendation
• A delay more than 3 hours for receiving
antibiotics was associated with 3 month
mortality
• Rapid administration of ATB in ED
43

4444Q J Med 2005; 98:291–298
45

• Most common
– S.pneumoniae
– N.meningitidis
– H. influenzae
– Listeria monocytogenes: Aging > 50 years
Micro-organism
46

Siriraj Hospital, 1993
47

Songklanagarind Hospital
1982-2001
48

Empirical ATB
49
50

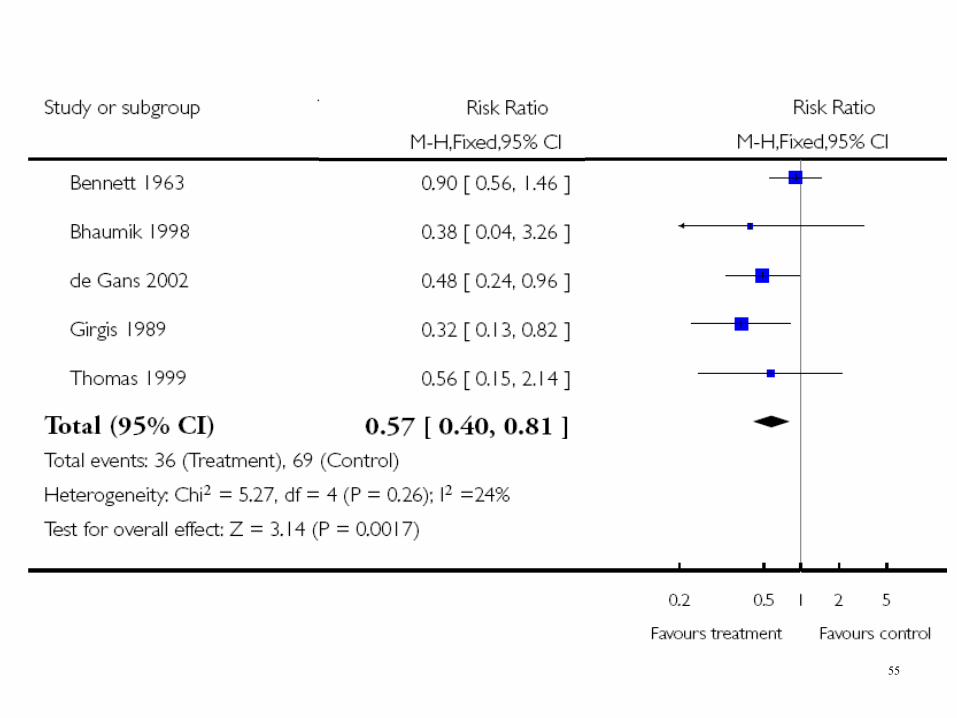
First large report in Vietnam in 2002
– May have benefit in S.pneumoniae
– Should start previous or in the same time of ATB
– Decrease mortality rate
51

• Overall mortality
– Adult
• Severe hearing loss
• Short term neurological sequenle
• Long term sequenle
• Causative species
• Timing
52

All age group
53

Mortality in adult
54
55

Causative species
56

57

58

59

60

Timing
61

62

63

64

65



![[PPT]Inflammation/Fever - Arkansas State · Web view* Many non-infectious disorders can also produce fever NON-SPECIFIC Patterns of fever: Intermittent fever Remittent fever Sustained](https://img.dokumen.tips/doc/110x75/5ab7b6f17f8b9a28468bebe4/pptinflammationfever-arkansas-state-view-many-non-infectious-disorders-can.jpg)