Embed Size (px)
Citation preview

Structural Trauma and Toxic Stress:Lifecourse Roots of Health InequitiesInterdepartmental Grand Rounds, Kaiser Permanente
Tomás J. Aragón, MD, DrPHAugust 31, 2016
Health Officer, City & County of San FranciscoDirector, Population Health DivisionSan Francisco Department of Public HealthAdjunct Faculty, UC Berkeley School of Public Healthhttp://populationhealth.science (blog)[email protected] (email)

Outline
1. How do we explain racial/ethnic health inequities?
2. San Francisco Department of Public Health
3. San Francisco Community Health Needs Assessment, 2016
4. Structural trauma and toxic stress—The lifecourse roots of health inequities
1

1. How do we explain racial/ethnichealth inequities?

Causes of premature deaths in men and women, San Francisco, 2003–2004How do we explain racial/ethnic health inequities and resilience?
footnoteAge-adjusted Expected Years of Life Lost (eYLL): Male (left), Female (right); © Black (colored red),4 Latino, × Asian/PI, + White; Source: Aragón TJ, et al. PubMed ID: 18402698 2

2. San Francisco Department ofPublic Health

Organization Chart, San Francisco Department of Public Health (SFDPH)
San Francisco Health Commission (7 members)Barbara Garcia, MPA, Director of Health
San Francisco Health Network (SFHN) (96%) Population Health Division (PHD) (4%)Roland Pickens, Director Tomás Aragón, Director & Health OfficerAmbulatory Care Environmental Health- Primary Care (4%) Community Health Equity and Promotion- Behavioral Health (18%) Disease Prevention and Control- Maternal, Child, and Adolescent Health Emergency Preparedness and Response- Jail Health (2%) Emergency Medical ServicesZuckerberg SF General (44%) Epidemiology and SurveillanceLagunda Honda Hospital (12%) Center for Learning and InnovationTransitions Center for Public Health Research
Bridge HIV (Research)Office of Health Equity and Planning
Administration
Source: https://www.sfdph.org/dph/files/reports/PolicyProcOfc/SFDPH-AnnualReport-2014-2015.pdf
3

Patient Distribution by Payer Source, SF Health Network, SFDPH
Primary Care and Behavioral Health Patients by Payer Source, FY 2014–2015
Hospital Patients by Payer Source, FY 2014–2015
4

Patients by Race/Ethnicity, SF Health Network, SFDPH, FY 2014-2015
Source: https://www.sfdph.org/dph/files/reports/PolicyProcOfc/SFDPH-AnnualReport-2014-2015.pdf
5

3. San Francisco Community HealthNeeds Assessment, 2016

San Francisco Framework for Assessing Population Health and Equity
Healthis a state of complete physical, mental and socialwell-being and not merely the absence of disease orinfirmity (WHO 1946).
Public Healthis what we, as a society, do collectively to assurethe conditions in which people can be healthy(IOM 1988).
Population Healthis a systems framework for studying and improvingthe health of populations through collective actionand learning (Source: http://phds.io).
6

San Francisco Community Health Needs Assessment, 2016 (www.sfhip.org)
Demographics Health Outcomes - Sexual HealthCommunity Identified Priorities - Asthma and COPD - Substance AbusePopulation Health Framework - Cancer - TobaccoSocial Determinants of Health - Cardiovascular Disease and Stroke - Tuberculosis- Civic Participation - Children’s Oral Health - Vaccine Preventable Disease- Education and Childcare - Diabetes - Weight- Economic Environment - Food-borne Disease - Nutrition- Health Care Assess and Quality - Health and Well-being - Physical Activity- Housing - Hepatitis B and C - Preterm Births- Natural Environment - Influenza and Pneumonia - Sexual Health- Transportation - Mental Health - Substance Abuse- Safety - Mortality - Tobacco
- Nutrition - Tuberculosis- Physical Activity - Vaccine Preventable Disease- Preterm Births - Weight
7

Left: Age pyramid, San Francisco, 2009–2013Right: Population projections by age, San Francisco, 2010–2060
Source: San Francisco Community Health Needs Assessment (http://sfhip.org) 8

Left: Population distribution, SF, 2010 vs. 2030, andRight: Population change by race/ethnicity, 1970–2013
Source: San Francisco Community Health Needs Assessment (http://sfhip.org) 9

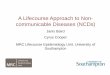
Leading causes of premature deaths, Males, San Francisco, 2010–2013
Source: San Francisco Community Health Needs Assessment (http://sfhip.org) 10

Leading causes of premature deaths, Females, San Francisco, 2010–2013
Source: San Francisco Community Health Needs Assessment (http://sfhip.org) 11

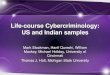
Adult asthma hospitalization rates, by race/ethnicity, San Francisco, 2005–2014
Source: San Francisco Community Health Needs Assessment (http://sfhip.org)
12

Cancer mortality rates, by race/ethnicity, San Francisco, 2009–2012
Source: San Francisco Community Health Needs Assessment (http://sfhip.org) 13

Invasive cancers incidence rates, by ethnicity, San Francisco, 2008-2012
Source: San Francisco Community Health Needs Assessment (http://sfhip.org) 14

Left: Hospitalization rates due to hypertension, San Francisco, 2006–2014Right: Hospitalization rates due to heart failure, San Francisco, 2005–2013
Source: San Francisco Community Health Needs Assessment (http://sfhip.org)
15

San Francisco Unified School District, Annual high school graduation,2009–2010 to 2014-2015
Academic Year
Gra
duat
ion
Perc
ent
020
4060
8010
0
2009-2010 2010-2011 2011-2012 2012-2013 2013-2014 2014-2015
LatinoAsianPacific Island.FilipinoBlack/AfrAmWhite
Source: California Department of Education, Data Quest http://dq.cde.ca.gov/dataquest/ 16

Children (ages 0–17 years) with Child Maltreatment Substantiations,San Francisco, Incidence per 1,000 children
2000 2005 2010 2015
010
2030
4050
60
Year
Rate
per
100
0 ch
ildre
n
BlackWhiteLatinoAsianPI
Source: California Child Welfare Indicators Project http://cssr.berkeley.edu/ucb_childwelfare/ 17

San Franciscans do not have equal opportunity for good healthUnevenly distributed obstacles to health (left); Health inequities (right)
Source: San Francisco Community Health Needs Assessment (http://sfhip.org) 18

4. Structural trauma and toxicstress—The lifecourse roots ofhealth inequities

The lifecourse roots of health and well-being, 2004–2016
19

Structural trauma and toxic stress—The roots of health inequities
Foundational themes
• Life-course of toxic stress, structural racism, and discrimination• Individual and communities suffer from the effects of trauma• The effects of trauma are transmitted across generations• Toxic stress effects child brain, body, and behavior for life
Trauma-informed approaches in San Francisco
• Trauma-informed systems training (Bay Area)• Trauma-Informed Community Building (TICB)• Black/African American Health Initiative (BAAHI)• Healthy Hearts San Francisco (CDC REACH grant)• Our Children, Our Families (collective impact)• San Francisco Health Improvement Partnership (sfhip.org)
20

Childhood adversities and mental health outcomes in homeless adultsSan Francisco, 2016 (Am J Geriatr Psychiatry 2016)
Source: http://www.centerforyouthwellness.org/ 21

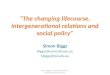
Neural connections and neuroplasticity in the early and late years of life
Source: http://developingchild.harvard.edu
22

Lifecourse Health Development—Variable trajectories
Source: Halfon N, Larson K, Lu M, Tullis E, Russ S. Lifecourse health development: past, present andfuture. Matern Child Health J. 2014;18(2):344-65. PubMed PMID: 23975451 23

How our core capabilities workAutomatic and intentional self-regulation, attention, and executive function
Executive function skill proficiency
Source: http://www.developingchild.harvard.edu 24

The lifecourse health development of adult inequitiesRe-conceptualizing early lifecourse policies to strengthen lifelong health
Source: Center for the Developing Child at http://developingchild.harvard.edu/ 25

Adverse Community Experiences and Resilience:A Framework for Addressing and Preventing Community Trauma
From The Prevention Instituteand Kaiser Permanente, 2015 26

Trauma-informed community building (San Francisco)Lead: Emily Weinstein, Bridge Housing & Jessica Wolin, San Francisco State University
TRAUMA INFORMED COMMUNITY BUILDINGA Model for Strengthening Community in Trauma Affected Neighborhoods
Weinstein, Wolin, Rose
Source: http://bridgehousing.com/PDFs/TICB.Paper5.14.pdf
27

Black/African American Health Initiative, April, 2014Lead: Dr. Ayanna Bennett, San Francisco Department of Public Health
BAAHI components
1. Collective impact2. Workforce development3. Cultural humility training
Collective impact
1. Heart health (focus: hypertension)2. Behavioral health (focus: alcohol)3. Women’s Health (focus: breast cancer)4. Sexual Health (focus: Chlamydia)
28

Hypertension Control Dashboard, Primary Care Hypertension Equity InitiativeLead: Dr. Ellen Chen and Kimberly Puccetti, Primary Care, San Francisco Health Network
Dec Feb Apr Jun Aug Oct Dec
0%
50%
100%
% Patients With Controlled BP
0 Patients Needed
Total: 60%
AA: 58%
58%
CMHC
Dec Feb Apr Jun Aug Oct Dec
4 Patients Needed
Total: 81%
AA: 62%
78%
CPHC
Dec Feb Apr Jun Aug Oct Dec
7 Patients Needed
Total: 71%
AA: 58%63%
CSC
Dec Feb Apr Jun Aug Oct Dec
19 Patients Needed
Total: 67%
AA: 60%
65%
FHC
Dec Feb Apr Jun Aug Oct Dec
0%
50%
100%% Patients With Controlled BP
40 Patients Needed
Total: 69%
AA: 63%
70%
RFPC
Dec Feb Apr Jun Aug Oct Dec
21 Patients Needed
Total: 70%
AA: 66%
71%
MHHC
Dec Feb Apr Jun Aug Oct Dec
0 Patients Needed
Total: 74%
AA: 72%
67%
OPHC
Dec Feb Apr Jun Aug Oct Dec
17 Patients Needed
Total: 69%
AA: 67%
75%
PHP
Dec Feb Apr Jun Aug Oct Dec
0%
50%
100%
% Patients With Controlled BP
7 Patients Needed
Total: 65%
AA: 62%
64%
PHHC
Dec Feb Apr Jun Aug Oct Dec
12 Patients Needed
Total: 68%
AA: 54%
60%
SAFHC
Dec Feb Apr Jun Aug Oct Dec
0 Patients Needed
Total: 62%
AA: 62%
61%
SEHC
Dec Feb Apr Jun Aug Oct Dec
73 Patients Needed
Total: 59%
AA: 54%
65%
TWUHC
LEGEND: Total Hypertensive Population Black Hypertensive Population Patients Needed to Reach Goal Black BP Control Goal
True North: Quality & EquityPrimary Care Driver Metric: HTN Equity
Black Hypertensive Patient Population
Dec Feb Apr Jun Aug Oct Dec
0%
50%
100%
% Patients With Controlled BP
169 Patients Needed
PC Total: 68%
PC AA: 61%
65%
SFHN PC TUHC670
SEHC969
SAFHC194
RFPC588
PHP203
PHHC348
OPHC
MHHC423
FHC391
CSC141
4,122
SFHNPC
29

Healthy Hearts SF—Prescriptions for free physical activity in the communityLead: Jacque McCright, Community Health Equity and Promotion, Population Health Division
URL: https://www.facebook.com/HealthyHeartsSF/Video: https://youtube.com/watch?v=aZIjTSfc2lk
30

LEAD Initiative, San Francisco Department of Public HealthLead: Barbara Garcia, and inspired by the Kresge Emerging Leaders in Public Health
Adapted from the Lean Transformation Framework (http://www.lean.org) 31

Core principles of trauma-informed systemsSFDPH initiative lead by Dr. Kenneth Epstein
We serve diverse, traumatized communities under chronic, toxic stress. Our diversestaff often live in or come from these communities. Therefore, we need to designhealing organizations. Here are six core principles of healing, trauma-informed systems:
1. Understanding trauma and stress2. Compassion and dependability3. Safety and stability4. Collaboration and empowerment5. Cultural humility and responsiveness6. Resilience and recovery
For more information visit: http://www.t2bayarea.org.32

Cultural/Racial Humility
In 1998, Melanie Tervalon and Jann Murray-García published a groundbreaking articlethat challenged the concept of “cultural competency” with the concept of “culturalhumility.” Cultural humility1 is committing to lifelong learning, critical self-reflection,and personal and institutional transformation.
1. Commit to lifelong learning and critical self-reflection.2. Cultivate humility,2 opening our hearts to transformation.3. Realize our own power, privilege, and prejudices.4. Redress power imbalances for respectful partnerships.5. Recognize and validate our common humanity.6. Promote institutional accountability.
1Adapted from Drs. Melanie Tervalon, Jann Murray-García, and Kenneth Hardy2“Humility is the noble choice to forgo your status and use your influence for the good of others. It isto hold your power in service of others.” (Source: John Dickson, Humilitas, http://a.co/gV1cldW)
33

The PEOPLE model for community health improvementInspired by The Prevention Institute’s Adverse Community Experiences and Resilience
P = People,E = EquitableO Opportunity,P = Place, andL = Life courseE Equity
34

The PEOPLE model for community health improvementInspired by The Prevention Institute’s Adverse Community Experiences and Resilience
35

The PEOPLE model for community health improvementInspired by The Prevention Institute’s Adverse Community Experiences and Resilience
• Life-course of toxic stress, structuralracism, and discrimination
• Individual and communities sufferfrom the effects of trauma
• The effects of trauma are transmittedacross generations
• Toxic stress effects child brain, body,and behavior for life
36

QUESTIONS?Acknowledgments (in alphabetical order)
Abbie Yant, Alice Chen, Amor Santiago, Aneeka Chaudhry, Ayanna Bennett, Barbara A Garcia,Barry Lawlor, Belle Taylor-McGhee, Brittney Doyle, Cecilia Thomas, Christine Siador, CindyGarcia, Colleen Chawla, Colleen Matthews, Curtis Chan, Darlene Daevu, David Serrano Sewell,Deborah Sherwood, Deena Lahn, Ellen Chen, Estela Garcia, Greg Wagner, Guliana Martinez,Hali Hammer, Iman Nazeeri-Simmons, Isela Ford, Israel Nieves-Rivera, Jacque McCright,James Illig, Jeannie Balido, Jenee Johnson, Jessica Wolin, John Grimes, Jonathan Fuchs,Judith Martin, Karen Pierce, Kenneth Epstein, Kenneth Hardy, Kevin Grumbach, Kim Shine,Kirsten Bibbins-Domingo, Leigh Kimberg, Lisa Golden, Maria X Martinez, Marlo Simmons,Mary Hansell, Michelle Albert, Michelle Kirian, Michelle Long, Muntu Davis, Nadine BurkeHarris, Patricia Erwin, Paula Fleisher, Perry Lang, Rachael Kagan, Rhea Bailey, RhondaSimmons, Roberto Vargas, Robin George, Roland Pickens, Ron Weigelt, Stuart Fong, SusanEhrlich, Susan Philip, Tessa Rouverol Collejo, Thomas Boyce, Tracey Packer, VeronicaShepard, Wanda Materre, Wanetta Davis, Wylie Liu
37