Embed Size (px)
Citation preview
Candida;treat, or not treat...that is the question
Dr. Volkan İnal

WHY?
Impact of candidiasis
• 9-12% of all BSI• 4th nosocomial BSI in US• 6th in European• Incidence rised 50 % between 2000 to 2005• Mortality 35–75 %
not
uncommon
increasing
incidence
Impact of candidiasis• Candida colonisation - hospital admission;– 22 days (SCOPE)– 14 days (Paris)– 19 days (EPIC II)
• 5-15% colonized at ICU admission
• increases with time to 50-80%
• 5-30% of colonized develop invasive candidiasis
• Accounts for up to 17 % of all ICU-acquired infections
colonize
in time
Impact of candidiasis
• The overall mortality:
– 42.6% (EPIC II)– 35.2% (PATH)– 37.9% (ECMM)– 85.9% (SCOPE) morta
l

Improved
Tx
Empiric
Preemptive
Tx
Resistance
Costs

inappropriate /
late Tx
Ecxess
LOSS
Costs

• Mortality
– receive appropriate antifungal therapy (< 5%)– without appropriate therapy (25-40%)– delayed beyond 12 h after sampling of blood has
been associated with an increase of in-hospital mortality from < 20% to 40%
....inappropriate / late therapy....
mortal

mortalinadequate
Tx

mortal
lateTx

SOME DEFINITIONS

• Treatment with no evidence of infection
• in selected high risk patients• in patients with persistent neutropenia• only for ICUs with a high rate of invasive
candidiasis
Prophylactic

• Treatment in the presence of persistent and refractory fever
• no other known cause of fever• who are at high risk for fungal infection• but no microbiological confirmation
Empric

• Treatment initiated in response to one or more biological markers of infection
• Candida spp. isolated from at least 2 non-contiguous skin and mucosal sites of high risk patients starting antifungals when the following conditions are satisfied:– the presence of long ICU stay (>96 hours)– broad-spectrum antibiotic therapy– the presence of any other risk factors
• severe sepsis• gastrointestinal surgery• TPN• microbiological evidence of Candida infection• multifocal colonisation• a positive result for serum β-d-glucan
Pre-emptive

• multifocal• > 7 days– Gastric aspirates (45.6 %)– Oropharyngeal (34.3 %)– Tracheal aspirates (23.4 %)– Perirectal swabs (21.2 %)– Urine (18.7 %)
• surveillance cultures– rectal, urinary, and respiratory cultures; twice a week– gastric / pharyngeal aspirates / skin rare
Colonisation

• Candida colonization
– low grade– high grade
colonization of at least three body siteson two or more consecutive occasions
Colonisation

Risk Factors
• Increasing age
• APACHE score II > 20
• Immunosuppressive therapy, Neoplasia
• Corticosteroids, Neutropenia
• Inadequate / late antifungal therapy
Risk Facto
rs

• Concomitant bacterial infection, Broad-spectrum
antibiotics
• Diabetes, Renal failure, Hemodialysis
• Recent abdominal surgical procedure
• Parenteral nutrition
• Pancreatitis
Risk Facto
rs
• Colonization of several body sites
• Burns (> 50%)
• Major trauma (ISS > 20)
• Disruption of physiological barriers in digestive tract
• Surgery of the urinary tract in presence of candiduria
Risk Factors

• Urinary catheter, Candiduria > 105 cfu/ml
• Central venous catheter
• Prolonged ICU stay (> 7 days)
• Multiple transfusions
• Hands of healthcare workers
• Contaminated IV fluids, hospital food, medical devices
Risk Facto
rs
Risk Facto
rs
Risk Facto
rs

Mortality rates and risk factors associated with nosocomial Candida infection in a respiratory intensive care unit.Adigüzel N1, Karakurt Z, Güngör G, Yazicioğlu Moçin O, et al. Tuberk Toraks. 2010;58(1):35-43.
• Nosocomial Candida infections; 163 RICU patients– Age 65 +/- 15– Female / Male: 8/18– Longer ICU stay 48.2 +/- 7.5 days vs. 10.3 +/- 0.8– Invasive mechanical ventilations– Central catheters and related infections– TPN– Multiple antibiotics– Ventilator associated tracheobronchitis– Ventilator associated pneumonia– Sepsis
Risk Facto
rs
TR

Evaluation of risk factors in patients with candiduria.Nayman Alpat S, Özguneş I, Ertem OT, Erben N, et al.Mikrobiyol Bul. 2011 Apr;45(2):318-24.
• 93 hospitalized patients– Longer stay in ICU 9.56 ± 9.09– Nosocomial origin n= 45, 90%– Higher rate of antibiotic prior to candiduria 86%– Presence of urinary system intervention– Catheter use– Immunosuppression
Risk Facto
rs
TR

• Surgical• Longer ICU LOS• Invasive applications/instrumentations• Sepsis• Broad spectrum antibiotics
Risk Facto
rs
TR

diagnosis

• Blood cultures 50% sensitivity, takes 1-3 days
• Beta-D-Glucan– sensitivity 51 - 100% – specificity 59 - 98.4%– false positive due to dialysis, TPN, cardio-pulmonary bypass,
intravenous immunoglobulins, other fungi like Aspergillus, fusarium, trichosporon etc
diagnosis

• adjunct to culture for the diagnosis of IC and is currently
recommended in several guidelines:
– European Organization for Research and Treatment of Cancer/Invasive Fungal
Infections Cooperative Group
– National Institute of Allergy and Infectious Diseases
– Mycoses Study Group (EORTC/MSG)
– European Society of Clinical Microbiology and Infectious Diseases (ESCMDI)
– Society of Critical Care Medicine (SCCM)
– European Society of Intensive Care Medicine (ESICM)
beta-d-glucan
diagnosis

• Mannan– sensitivity 58 - 60%– specificity 59%
• Anti-mannan– sensitivity 93 %– specificity 83 %
• Mannan combined to Anti-mannan– sensitivity 83%– specificity 86 %
diagnosis

• Antimycelial antibodies (Candida albicans germ tubespecific antibody CAGTA)
– sensitivity 77–89 %– specificity 91–100 %
diagnosis
• Fungal PCR - Detection of Candida DNA– provenIC;• sensitivity 95%• specificity 92 %,
– probable IC• sensitivity 85%
• Genetic risk testing mutations, such as the CARD9 and DECTIN-1 genes
diagnosis

... combinations??• BG + CAGTA
– sensitivity 90.3 %– specificity 54.8 %
• Blood culture + BG / PCR– sensitivity 79 %– specificity 98 %
• Mn-Anti-Mn– sensitivity 89.3 %– specificity 63.0 %
• BDG + mannan antigen– sensitivity 89.3– specificity 85.0 %
diagnosis

PREDICTION RULES


Colonosation Index
CI = non blood cultures/total sites cultured
«blood cultures are not considered»
cCI = cultures with heavy growth/total culture
«+++ / 100.000»Colonization may turn into invasion
if CI 0.5 or cCI 0.4

Leon Score
Clinical Features ScoreSepsis 2Surgery 1TPN 1Multifocal colonization 1
A score of > 2.5 associated with 7x candidemia

Ostrosky Zeichner Score
• ICU stay for at least 4 days• + Antibiotic use• + Central Venous Catheter• + any 2 of the following:
SurgeryTotal parenteral nutrition(TPN)HemodialysisPancreatitisSteroidsImmunosuppression




GUIDELINES

IDSA 20092009

IDSA 2009
• Documented Candidemia – Tx
• Empirical Tx critically ill patients with risk factors for invasive candidiasis and no other known cause of fever, risk factors, serologic markers, culture data from nonsterile sites
• Empirical Tx suspected invasive candidiasis in neutropenic patients
• Prophylaxis solid-organ transplant recipients, neutropenic patients receiving chemotherapy, stem cell transplant recipients
2009

IDSA 2009
• asymptomatic candiduria NO Tx if low risk group
• symptomatic candiduria with suspected disseminated candidiasis Tx
• Growth of Candida from respiratory secretions rarely indicates invasive candidiasis and NO Tx
2009

2010
• it is difficult to universally recommend antifungal prophylaxis
• apart from patient groups with a known very high risk• Antifungal prophylaxis may also be reasonable where local
incidence rates and epidemiology are compelling
• Among stable patients with multifocal Candida colonization and/or a multitude of clinical-risk factors, preemptive therapy is currently not indicated
• Among patients with refractory fever despite broad-spectrum antibacterial therapy, empiric antifungal therapy may be reasonable where local incidence rates are high (e.g. >10%)
2010

2011

European Society for Clinical Microbiology and Infectious Diseases
ESCMID 20122012

2012

2012

• Candida isolation from respiratory secretions should never trigger Tx
• (1,3)-b-D-glucan detection in serum or plasma prompting antifungal treatment is marginally supported
• Asymptomatic candiduria should not Tx• Symptomatic cystitis should be Tx
ESCMID 2012 - Diagnosis-driven approach (pre-emptive)
2012

IRANIAN 20132013

IRANIAN 20132013

IRANIAN 2013
2013

IAC 20132013

IAC 2013• Direct microscopy examination for yeast detection from purulent and necrotic
intra-abdominal specimens obtained during surgery or by percutaneous aspiration is recommended in all patients with nonappendicular abdominal infections including secondary and tertiary peritonitis
• Samples obtained from drainage tubes are not valuable except for study of colonization
• Blood cultures should be taken through peripheral vein punctures upon diagnosis or suspicion of intraabdominal infections and tertiary peritonitis, and specific media for fungi are recommended
• Antifungal susceptibility test should be performed on yeast isolates from blood, sterile sites, and other appropriate specimens
2013

IAC 2013
• Systemic antifungal treatment should be considered when adequate intra-abdominal specimens (obtained surgically or within 24 h from external drainage) are positive for Candida, irrespective of the fungal concentration and the associated bacterial growth
• Positive cultures from drains should not be treated, especially if the drains are in place for more than 24h
2013

IAC 2013
• mannan / antimannan / BDG test should be performed in patients with secondary or tertiary peritonitis and at least one specific risk factor for IAC
• Patients with recent abdominal surgery and recurrent gastrointestinal perforation or anastomotic leakage should receive Tx
2013

IAC 2013
• Empirical antifungal treatment may be considered in patients with a diagnosis of intra-abdominal infection and at least one specific risk factor
• In patients with intra-abdominal infection with or without specific risk factor for Candida infection, empirical Tx should be administered if a positive mannan / antimannan or BDG or PCR test result is present
2013
Rev Esp Quimioter 2013;26(2):131-150
EPICO 20132013

• blood cultures at the time of suspected
• use direct vision (microscopy)
• Initiate early Tx
• Echinocandin the first-line
• At least one ophthalmological evaluation
EPICO 20132013

Rev Esp Quimioter 2014;27(3): 196-212
EPICO 2.0 20142014

EPICO 2.0 2014
• Empirical Tx is recommended in secondary nosocomial peritonitis with risk factors and in tertiary peritonitis
• Early and appropriate Tx• Echinocandins• Neutropenic patients
2014

ITALIC 20142014

ITALIC 2014
• In the asymptomatic patient, the isolation of a Candida strain from a non-sterile body site (bronchial aspirate, tracheal aspirate, bronchoalveolar lavage fluid or sputum) should not prompt any Tx and should be merely considered as colonisation
• Antifungal prophylaxis should not be administered in non-immunocompromised
2014

• However, in a patient with signs and symptoms of infection, multiple Candida colonisation, including isolation from urine in a patient fitted with a bladder catheter, might be suggestive of a Candida infection and might prompt Tx
ITALIC 20142014

• The repeated isolation of Candida from fluids obtained from a surgical drainage should not be underestimated and should prompt additional investigations, even in the absence of clinical signs and symptoms
• The same applies to Candida isolation from peritoneal fluids in a patient undergoing peritoneal dialysis
ITALIC 20142014
• BDG is diagnostic
• results should be interpreted in the presence of other risk factors and the patient’s clinical conditions
• There is insufficient evidence to recommend the use of the BDG test as a screening tool in patients without symptoms
ITALIC 20142014

• The mannan/antimannan detection test may be useful for the diagnosis of IC
• The separate detection of either mannan or antimannan cannot be recommended
ITALIC 20142014

• Echocardiography persistent candidaemia to rule out Candida endocarditis
• Fundoscopic examination should be performed and possibly repeated in every patient with IC to rule out chorioretinitis and endophthalmitis
ITALIC 20142014

2014

2014

2014

NOT support the use of antifungal treatment in patients with VAP and Candida in the endotracheal secretions
2014

2014
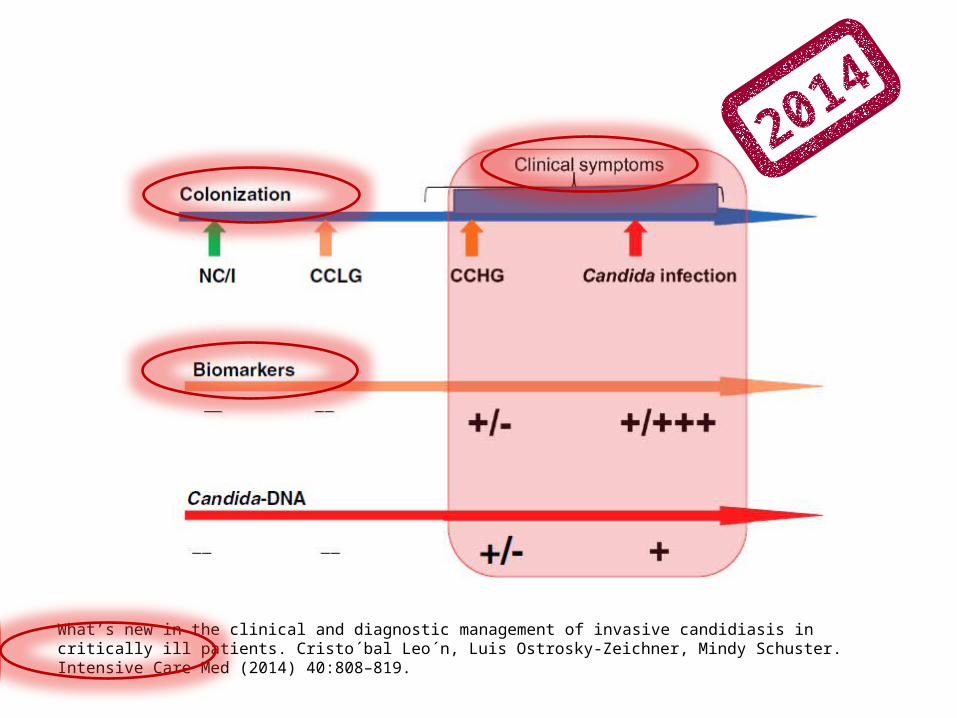
What’s new in the clinical and diagnostic management of invasive candidiasis in critically ill patients. Cristo´bal Leo´n, Luis Ostrosky-Zeichner, Mindy Schuster. Intensive Care Med (2014) 40:808–819.
2014
• included 12 unique trials (eight comparing fluconazole and four ketoconazole with no antifungal or a nonabsorbable agent) involving 1606 randomized patients
• Prophylaxis with fluconazole or ketoconazole in critically ill patients reduces invasive fungal infections by one half and total mortality by one quarter
• In patients at increased risk of invasive fungal infections, antifungal prophylaxis with fluconazole should be considered
Antifungal agentsfor preventing fungal infections
in non-neutropenic critically ill patients
Antifungal agents for preventing fungal infections in non-neutropenic critically ill patients (Review)
Copyright © 2012 The Cochrane Collaboration. Published by JohnWiley & Sons, Ltd.
Routine / selective antifungal administrationfor control of fungal infections
in patients with cancer
• 32 trials, 4287 patients were included
• Intravenous Amphotericin-B was the only antifungal agent that reduced total mortality
• It should therefore be preferred when prophylactic or empirical antifungal therapy is introduced in cancer patients with neutropenia
Routine versus selective antifungal administration for control of fungal infections in patients with cancer (Review)
Copyright © 2014 The Cochrane Collaboration. Published by JohnWiley & Sons, Ltd.
Nystatin prophylaxis and treatmentin severely immunodepressed patients
• 14 trials (1569 patients)
• People on chemotherapy for cancer, receiving a transplant or with AIDS are at risk of fungal infections (lifethreatening)
• The review found that nystatin was no better than placebo (no treatment)
Nystatin prophylaxis and treatment in severely immunodepressed patients (Review)
Copyright © 2014 The Cochrane Collaboration. Published by JohnWiley & Sons, Ltd.

Antifungal agentsfor preventing fungal infections
in solid organ transplant recipients
• 14 unique trials with 1497 randomised participants were included
• antifungal prophylaxis with fluconazole significantly reduces the incidence of IFIs with no definite mortality benefit
• In transplant centres where the incidence of IFIs is high, or in situations where the individual risk is great, antifungal prophylaxis should be considered
Antifungal agents for preventing fungal infections in solid organ transplant recipients (Review)
Copyright © 2009 The Cochrane Collaboration. Published by JohnWiley & Sons, Ltd.
To takeaway
2014

Thanks





























