Embed Size (px)
Citation preview

Quality Incentives in Healthcare: How do they affect Product Value?Thursday August 22th 2013

Speaker
Tim Clark
Vice President Scientific AffairsICON Clinical Research
Ron Halbert, MD, MPH: Vice President, Health Economics

What we will discuss
Agenda
Quality Incentives in Healthcare: How do they affect product value?
We believe a strategic approach to quality should be considered as part of product development and commercialization
Proof of impact on quality has become a prominent component in US health care reimbursement
Developing a strategy requires understanding how quality is measured and incentivized

4
In this webinar, we will:
Agenda (cont’d)
Examine the interactions between quality and product development; and
Lay a foundation for a strategic approach for manufacturers.
Explore the evolution of quality incentives in the US;

5
There are many definitions of quality
For this presentation, quality refers to measurement of healthcare delivery or outcomes against an accepted standard, often tied to performance incentives
Manufacturing- Characteristics of the Product- Consistency- Purity- Others Scientific
- Reproducibility of Results
- Small p-values Sales- Customer Satisfaction- Repeat Business

6
Multiple challenges have led to an increased focus on quality
Cost Pressure
Lack of Information
• Costs of treatment are rising• Business, governments are finding it harder to pay for healthcare• Increased efforts to restrain costs
• Little public information on quality, cost of health services• Incomplete data at point of care to support decision-making• Lack of data infrastructure to gather & share information
Misaligned Payment
• Payment based on volume, not quality• Payment system comes with perverse incentives
Treatment Variation
• Not enough data on what works best• Providers not always following best practices• Quality appears suboptimal (preventable errors, over/underuse, etc.)
The emphasis on these types of problems differs by stakeholder

7
Indicators of clinical quality are part of a much larger movement
Institute of Medicine Aims for Improving Healthcare1
Source: Institute of Medicine. Crossing the Quality Chasm. Washington, DC, National Academy Press, 2001.
• Safe: Avoiding injuries to patients
• Effective: Providing services based on scientific knowledge
• Patient-Centered: Providing care respectful and responsive to patient preferences, needs, values
• Timely: Reducing waits and harmful delays
• Efficient: Avoiding waste
• Equitable: Providing care that does not vary in quality because of personal characteristics

8
Does quality care lead to cost savings?
• Although it is commonly believed that higher quality care leads to cost savings1, this is not always true
• Some “quality” reduces costs2
o Avoiding unnecessary tests, redundant services, or non-efficacious therapieso Prevention of hospitalization through better outpatient care
• Some “quality” increases costs3
o Better access to careo Better follow-up leading to more careo Earlier and more widespread preventive interventions
Payers hope that quality will reduce costs OR at least reassure the publicthat patient care is not being harmed by cost reduction
1. Porter ME & Teisberg EO. Redefining Health Care. Boston: Harvard Business School Press, 2006.2. McWilliams JM, et al. JAMA Intern Med 2013;17:1-9.3. Joynt KE, Jha AK. JAMA 2012;307:1082-3.

9
• Product improves outcomes• Product helps meet quality targets• Product lowers overall healthcare costs (?)
There is a reciprocal relationship between quality-based incentives and product value
Quality Product
• Measurement leads to increased diagnosis• Indicator explicitly endorses product use• Measurement draws attention to disease/product
To maximize product value, consider both sides of the equation

Why care about quality?
• Quality is a key driver in US healthcare

11
Proof of impact on quality has become a key driver in healthcare reimbursement
• Led by CMS, payers are transforming from passive to active purchasers of high quality health care• Payers are moving from offering purely positive incentives to introducing
penalties for not participating in quality programs or not achieving quality targets
• Spearheaded by Accountable Care Organizations (ACO) and Patient Centered Medical Homes (PCMH), integrated care is being pushed to make healthcare more efficient while maintaining quality
• Bundled payments provide further incentives for integrated care, while maintaining quality standards
Quality represents one aspect of health care reform, affecting public as well as private payers

12
Quality evolves from measurement to incentive in a predictable pathway
Establish Metrics
• Measurement science• Focus on metric development, performance characteristics
ElectronicReporting
• Reporting incentives• Focus on improving data quality
Voluntary Participation
• Positive performance incentives• Focus on participation• Rewards for performance & improvement
Mandatory participation
• Negative performance incentives• Focus on performance standards• Negative incentives for non-participation, poor performance
Benchmarking
• Public reporting• Focus on quantifying variation• Identifying best performers
Payment Restructuring
• Integrated incentives• Risk transferred to provider• Value-based purchasing• Bundling

13
CMS is integrating quality-based components into payment for all provider classes
Physicians
Medicare Advantage Plans
HospitalsEHR Incentive Program (“Meaningful use”)
Hospital Compare
ACO (Shared Savings Program)
Hospital Value-Based Purchasing
EHR Incentive Program (“Meaningful use”)
PQRI / PQRS
Physician Compare
Physician Value-Based Purchasing
Electronic Claims Submission
Medicare Quality Bonus Payment (“Stars”)
ACO (Shared Savings Program)
Value-Based Purchasing

14
Aggregated payment schemes are being reintroduced, but are now linked to quality
Providers can feel trapped
Aggregated payment (capitation, bundled payment) covers a defined population or service• Incentivizes integration of care by shifting risk to the provider • Potential for reduced care, potentially worsening outcomes
Quality measurement helps insure that health outcomes remain within acceptable ranges• Performance-based incentives supplement provider income, replacing
losses from reduced base payment rates
15
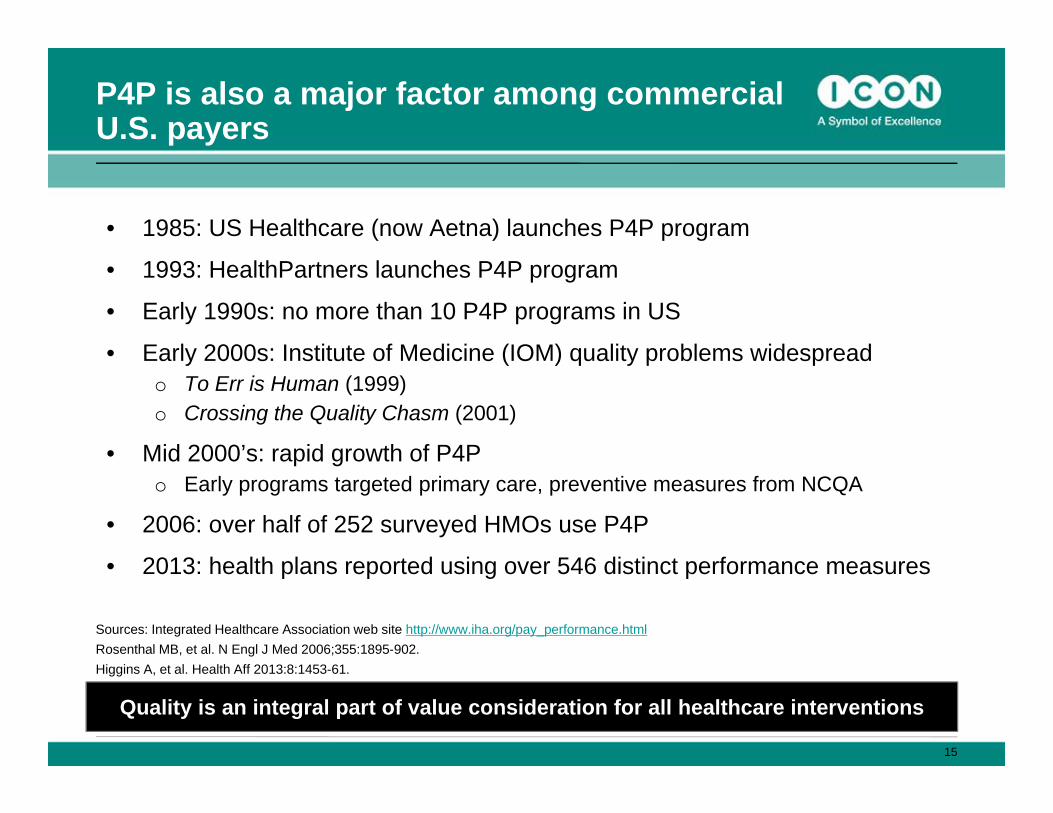
P4P is also a major factor among commercial U.S. payers
• 1985: US Healthcare (now Aetna) launches P4P program
• 1993: HealthPartners launches P4P program
• Early 1990s: no more than 10 P4P programs in US
• Early 2000s: Institute of Medicine (IOM) quality problems widespreado To Err is Human (1999)o Crossing the Quality Chasm (2001)
• Mid 2000’s: rapid growth of P4Po Early programs targeted primary care, preventive measures from NCQA
• 2006: over half of 252 surveyed HMOs use P4P
• 2013: health plans reported using over 546 distinct performance measures
Sources: Integrated Healthcare Association web site http://www.iha.org/pay_performance.htmlRosenthal MB, et al. N Engl J Med 2006;355:1895-902.Higgins A, et al. Health Aff 2013:8:1453-61.
Quality is an integral part of value consideration for all healthcare interventions

16
Pay-for-performance (P4P) is now well established in the US
Payers- Government- Employers
Purchasers- Managed care
- Gov’t contractors
Provider groups- Physician groups
- Facilities
Individualdoctors
The next step is to “engage” patients by including them in the incentive structure
Sources: Rosenthal MB, et al. N Engl J Med 2006;355:1895-902.Sandy LG, et al. Health Aff 2013;8:1440-5.

17
Payers and providers are being pushed to incorporate quality into health care delivery
As we move into the second half of the adoption curve, quality will become increasingly important
Graph adapted from: Rogers E.M. & Rogers E. Diffusion of Innovations. Free Press; 5th edition: 2003
Adoption of quality processes
in healthcare

18
Quality is being used in product-specificvalue messaging
Source: Advertisement in ATS Morning Minute (electronic newsletter) 18 April 2012
19
Innovative approaches are linking to quality to add value
Sanofi launches iPhone glucose monitor, diabetes coaching1
Source: http://www.fiercepharma.com/story/sanofi-launches-iphone-glucose-monitor-diabetes-coaching/2012-03-29

20
Industry is partnering around quality measurement and improvement
Source: http://www.nccn.org/about/news/newsinfo.asp?NewsID=292

21
But industry involvement is also attracting unfavorable attention
Source: Moynihan RN, et al. PLoS One 2013:10:e10011500.

How is quality measured?
• Developing a strategy requires an understanding of how quality is measured and incentivized

23
• There is evidence to support the measure focus
• There is a documented performance gap• Addresses a high priority area
o National health goal / priorityo Affects large numbers of patients / substantial impact for a smaller populationo Leading cause of morbidity/mortalityo High resource use (current and/or future)o Severity of illness / severity of consequences of poor quality
• Scientific acceptability of the measure
• Required data are feasible to collect
• Usability of measure by potential audiences
• Harmonized with existing or related measures
How are quality measures chosen?
Source: NQF. “Measuring Performance”. http://www.qualityforum.org/docs/measure_evaluation_criteria.aspx

24
• New slide (from NQF?) How are measures chosen?
How are quality measures chosen?
Source: Higgins A, et al. Health Aff 2013:8:1453-61.

25
Quality measures are born, live, and eventually retire
Source: NCQA. http://www.ncqa.org/tabid/425/Default.aspx

26
Quality measures are reviewed periodically and updated as needed
NQF Maintenance Processo Standardized in a 3-year cycle of review and endorsement of measures in 22
topic areas, such as cardiology, neurology, perinatal, and infectious disease
• Annual updateso The measure steward is responsible for updating and maintaining the currency
and relevance of the measure
• Maintenance endorsement every three yearso NQF is responsible for maintenance of NQF endorsement and solicits
information from stewards in order to review measures
• An ad hoc review may be conducted at any time if the evidence supporting the measure has changed
New science is the most effective way to change a measure
Source: NQF. http://www.qualityforum.org/Measuring_Performance/Endorsed_Performance_Measures_Maintenance.aspx

27
Many different organizations influence the quality process
• Organizations may serve the following functions:o Developers create and/or test indicatorso Endorsers approve or endorse indicatorso Users apply indicators in the actual measurement of quality
DevelopersDevelopers
EndorsersEndorsers UsersUsers
Performance measures are related to guidelines and certification/accreditation
Organizations may have multiple functions• NCQA: serves all 3 functions• CMS: endorser and user• NQF: endorser only

28
• We believe a strategic approach to quality should be considered as part of product development and commercialization
Building a product-specific quality strategy

29
Quality measurement depends on the maturity of the underlying science
The maturity of quality science can help guide the development of a disease-specific approach to quality strategy
Immature• No Established SoC
Emerging• Evolving SoC
• Link between intervention and Improvement is debated
Mature• Established SoC
• Link between intervention and improvement is established
• Performance gap is documented

30
How important is a quality strategy for your product?P
opul
atio
n Im
pact
(Pre
vale
nce/
Cos
t)
Maturity of Measurement Science
Rheumatoid Arthritis
Colorectal Cancer
Renal CancerGastric
Cancer
Heart Failure Asthma
Type 2Diabetes
Schizophrenia
Cystic Fibrosis
Knowing where are your key products are on this matrix can help guide a strategic approach
HIV
As you move to the upper right, quality strategy becomes
increasingly relevant

31
Quality should be explicitly considered in developing strategy for products as well as therapeutic areas
• Begin with a quality-specific assessmento What is the state of quality science in the therapeutic area?o Which organizations drive quality-relevant activities?o Are there performance indicators relative to the therapy area?o What trends in the quality environment may affect product success?o Are there relevant policies tied to quality?
• If quality seems to be a potentially important factor:o Begin to outline potential quality-relevant goals and objectiveso Identify potential approaches to achieving goalso Consider costs and benefits of different approaches
Quality strategy should vary by product characteristics and disease state, considering and clinical and commercial goals

ICON Signature Series
• ICON Signature Series is our thought leadership program that offers expert insights into value-driven strategies for clinical development.
• The program features ICON and external experts in all aspects of clinical development and post-approval product value strategies.
• For a list of featured topics and upcoming events go to: http://www.iconplc.com/icon-views/