Embed Size (px)
DESCRIPTION
Edward M. Omron MD, MPH
Citation preview

Pulmonary Pearls
Edward Omron MD, MPHPulmonary/Critical Care Medicine

History
• 74 year-old woman presents with 4 days cough, chills, dyspnea and fever
• Hemoptysis with right sided pleuritic chest pain x2 days
• Unable to walk due to dyspnea– 35 pack year tobacco use– Assisted care facility– Recent hospital admission for complicated UTI
treated with levofloxacin

Physical Exam
• Respiratory distress • Temp 101.8 F• Heart Rate 110• Blood pressure 80/55 mm Hg• Dullness to percussion on right side with
crackles

Initial Tests
• ECG: Sinus Tachicardia with LVH• WBC: 18,600• Creatinine: 1.5, BUN 47• ABG
– pH 7.32 – PaCO2 = 47 mm Hg– PaO2 = 58 mm Hg on 4 L NC

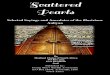
ER Chest X-RAY

What is the most likely pathogen in this patient?
• S pneumoniae• H influenzae• S aureus• P aeroginosa• K pneumoniae• M tuberculosis• Other

Initial Treatment in the ER
• Right IJ central venous access• Fluid bolus 1 Liter 0.9% NS• Oxygen converted to 40% venturi mask• Bipap on the way• Albuterol / Atrovent neb treatments• Transduced CVP < 8 mm Hg after fluid bolus
and second 1 L 0.9% NS given

What antibiotic regimen would you prescribe in the ER?
• Beta Lactam • Respiratory quinolone• 3rd Generation Cephalosporin+macrolide• 3rd Generation Cephalosporin+ respirotory quinolone• Carbopenem+ aminoglycoside• Vancomycin+ respiratory quinolone• Vancomycin + extended spectrum penicillin +
aminoglycoside• Zyvox, Zosyn, levafloxacin• Other

Initial antibiotics given in the ER
• Ceftriaxone 2 gram and levafloxacin 750 mg
• Rationale: – Most likely diagnosis was thought to be CAP
(Strep pneumo + H influ)– Atypical pathogen coverage for legionella

Follow Up
• Urine legionella antigen negative• Sputum: gram + cocci in clusters 4+ which
later grew out MRSA• Blood Cultures: MRSA, PVL+ or CA-MRSA• Community Acquired MRSA

Community Acquired MRSA Sensitivity in this patient
• Oxacillin Resistant• Fluoroquinolone Intermediate• Macrolide Resistant• Cephalosporin Resistant• Vancomycin Sensitive• Clindamycin Sensitive• Linezolid Sensitive• Septra Sensitive

CA-MRSA Pneumonia
• MRSA is an increasing threat in all forms of pneumonia
• CA-MRSA is the newest threat to hospitalized patients with pneumonia
• “Superbug”– Enhanced antibiotic resistance– Higher mortality than MSSA strains– Expresses multiple virulence factors

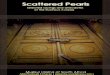
CA-MRSA: 48 hours of destruction
Admission 48 hours later

59 yo with dyspnea and increased work of breathing
• ABG: pH = 7.27, PCO2= 56, PaO2 = 60• Pulse 125, RR = 32, BP= 120/80, Sat 90% RA• WBC 17K, BUN = 30, Creat 1.2• Conversational dyspnea but alert and oriented
• Where should this patient go?– ICU – Monitored Bed – Floor
• How should we manage the airway?

CXR

COPD Management Non-invasive ventilation
• Very useful in acute exacerbation especially with dynamic hyperinflation and muscle failure.
• Can be tried even in hypercapneic narcosis.
• Night time use for severe COPD with hypercapnia may be of benefit if tolerated.

• Non-invasive ventilation– Hypercapneic failure PCO2> 45 mg Hg
• BIPAP: Initial 10 IPAP/ 5 EPAP cm H2O with FIO2 bleed in to maintain sats at 90%, humidified
– Hypoxic and Hypercapneic ventilatory Failure• Bipap: Initial 10 IPAP /10 EPAP cm H2O with FiO2 Bleed
in to maintain sats at 90%, humidified
– Congestive Heart Failure• CPAP at 10 cm H2O with FIO2 Bleed in to maintain sats
at 90%, humidified

COPD Management
• For Acute Exacerbations– Injudicious administration 02 in CO2 retaining
pts may cause acute rise in PaCO2. • Loss of alveolar hypoxemic vasoconstriction
causes flooding of vasculature with alveolar CO2• NOT LIKELY “loss of hypoxemic drive.”
– Appears as such because sudden rise in PaCO2 causes narcosis.
• Titrate to 90% at all times
– Avoid respiratory depressants

Severe COPD
Normal

Severe COPD
Normal

A 73 yo is brought to the emergency room comatose. The family states she had become confused and had swallowed an excess number of sleeping pills. ABG while breathing room air (FIO2 = 0.21) shows the PaO2, is 42 mm Hg, the PaCO2, is 75 mm Hg, and the pH is 7.10. Why is her PaO2 reduced?

Alveolar Hypoventilation
• No increase in P(A-a)O2 gradient
• PAO2 = 150-1.2 (75) = 60
• A-a gradient = 60 – 42 = 18 Nl
• PaO2 +PCO2 = 120

Pulse OximetryPulse Oximetry
• Binding sites for O2 are heme groups
• OXYGEN SATURATION– % of all heme sites saturated with O2
• Measures the difference in the light absorbance characeteristics between Oxy Hb and Deoxy Hb
• SpO2 = Oxy Hb x 100 Oxy Hb + Deoxy Hb• ABG SaO2 is a calculated value from PaO2

Pulse OximetryPulse Oximetry
Whole Blood
PaO2
SaO2
SpO2:Pulse Oximetry
ABG

ProblemProblem
• 28 yo pt with fevers,chills, SOB,cough– Taking Dapsone for PCP prophylaxis– ABG: PaO2 90, PaCO2 35.2, pH 7.43, SaO2 100%– Pulse oximeter 89%– PCP Pneumonia, started on Septra, Clinda, and
Prednisone– ABG: PaO2 378, PaCO2 of 35, pH 7.42, SaO2 100%– Pulse Oximeter 83%– Whats Happening?

MethemoglobinMethemoglobin
• Oxidation of Fe++ to Fe+++ state
• Met-Hb depresses the SpO2 reading
• Dapsone is an oxidant
• Met-Hb depresses the SpO2 to 80’s– Further increases in Met-Hb do not
depress SpO2
• Methylene Blue administration is Rx

Some drugs implicated in causing methemoglobinemia Generic name Use
Dapsone Skin protectant
Benzocaine Local anesthetic
Metoclopramide Gastric stasis
Nitroglycerin Angina
Phenazopyridine Urinary tract analgesic
Prilocaine Local anesthetic
Primaquine Malaria prophylaxis and treatment
Trimethoprim Urinary antibacterial
Amyl nitrite Rarely used clinically; often used by drug abusers

Co-oximetryCo-oximetry
• SpO2 = Oxy-Hb
Oxy-Hb+Deoxy-Hb+CO-Hb+Met-Hb

OximetryOximetry
• 54 yo WM with headaches, dyspnea and a Kerosene heater at home– ABG: PaO2 = 89, PaCO2 = 38, pH = 7.43– SaO2 from ABG= 98%– Pulse Oximetry = 98%– Whats the problem?

OximetryOximetry
• Carboxyhemoglobin: Hb +CO– Does not affect PaO2 or pulse oximetry– P.O. reads CO as oxyhemoglobin– Need co-oximetry if suspected
• Follow Up:– PaO2 = 79, PaCO2 = 31, SpO2 = 53%, pH
=7.36 – CO-Hb46%

Correlation of symptoms and signs with carbon monoxide level Percent of CO in inspired
air Percent of HbCO in blood Signs and symptoms
0.007 10
Common in cigarette smokers; dyspnea during vigorousexertion; occasional tightness in forehead; dilation of cutaneous blood vessels
0.012 20 Dyspnea during moderate exertion; occasional throbbing headache in temples
0.022 30 Severe headache; irritability; easy fatigability; disturbed judgment; possible dizziness and possible dimness of vision
0.035 40+ Headache; confusion; fainting on exertion
0.080 60+ Unconsciousness; intermittent convulsions; respiratory failure; death if exposure prolonged
0.195 80 Fatal
Modified from Winter, P.M., and Miller, J.N.: JAMA 236:1503, 1976, Copyright 1976, American Medical Association.