Embed Size (px)
Citation preview

HYPERTENSIVE EMERGENCIES
AND URGENCIES
Dr Manjuprasad Moderator:Dr
Padmaja Udaykumar

• Hypertension (HTN) or high blood pressure - arterial
hypertension
• Chronic medical condition- BP
• Heart - work harder than normal to circulate blood
through the blood vessels
2

JNC- 7
• Normal – SBP<120 and DBP<80
• Prehypertension – SBP 120-139 or DBP 80-89
• Stage I hypertension – SBP 140-159 or DBP 90-99
• Stage II hypertension – SBP >160 or DBP >100– Hypertensive urgency
– Hypertensive emergency3

• Hypertensive emergencies:
Severe elevation in BP complicated by impending or
progressive target/end organ damage
• Hypertensive urgencies:
Severe elevation in BP without any target organ damage
4

CNS - encephalopathy, intracranial
hemorrhage, Grade 3-4 retinopathy
Kidneys - acute kidney injury,
microscopic hematuria
Vasculature - aortic dissection, eclampsia
Heart - CHF, MI,
angina
5

Conditions constituting evidence of
end organ damage
• Hypertensive encephalopathy
• Intracerebral hemorrhage
• Stroke
• IHD- AMI, acute LVF with papilloedema,
angina
6

• Eclampsia
• Life threatening arterial bleed
7

ETIOLOGY
• Poor treatment or abrupt discontinuation of the
treatment
• Renal parenchymal disease
• Drugs
• Coarctation of aorta
• Pre eclampsia/ eclampsia
8

PATHOPHYSIOLOGY
• Failure of normal autoregulation
• Release of vasoconstrictors from stressed walls
• Endothelium plays an important role in BP
homeostasis
• Increase in pressure starts a cycle
9

MANAGEMENT
• BP should never be reduced to normal values
- Risk of ischemia and infarction.
• Gen rule:
- MAP should be lowered no more than 20% in first hour
- If pt remains stable, BP lowered to 160/110 in next 2-6
. hrs
10

Treatment goals achieved by
- continuous infusion of a short acting, titratable,
parenteral antihypertensive agent along with constant
BP monitoring
11

TREATMENT
Medication options
1. Oral antihypertensives
• Chronic hypertensive
• Hypertensive urgency
2. IV antihypertensives
• Hypertensive emergency
12

13

IV antihypertensive
• Vasodilators
sodium nitroprusside
nitroglycerine
nicardipine
fenoldopam
hydralazine
enalaprilat
• Adrenergic
inhibitors
labetalol
esmolol
phentolamine
14

Ideal IV antihypertensive
• Lower BP without compromising blood flow to critical organs
• Vasodilators- preserve organ blood flow in the face
. of decreased perfusion
- also tend to increase cardiac output
15

Profile of ideal antiHTN
• Preserves GFR
• Few or no drug reactions
• Rapid onset and offset of action
• Minimal hypotension
• Minimal need of continuous BP monitoring
• No acute tolerance
16

• Ease of use and convenient
• Safe and no toxic metabolites
• Minimal sympathetic activation
• Multiple formulations for short and long term use
17

Sodium Nitroprusside
MOA:- direct smooth muscle dilator
- Nitric oxide component
-reduces preload and after load
- causes cerebral vasodialation
• Ultra short acting
• Immediate onset - DoA : 10min
18

• Dose:
0.1-0.5mcg/kg/min IV infusion
titrate to desired effect
rates>10mcg/kg/min
Adverse effects/Precautions:
Cyanide toxicity
precipitous drop in BP
continuous BP monitoring
reflex tachycardia
Nausea and vomiting
Increased ICP
19

Uses
Drug of choice:
• Perioperative HPT
• Cocaine toxicity
• Aortic dissection(combination)
• Neurologic syndromes
20

Nitroglycerine
MoA:
• Potent vasodilator
• Decrease preload (CO + BP)
• Decreases coronary vasospasm
• Dose: cont infusion
start 5mcg/min, incr by 5mcg/min
every 3-5min to 20mcg/min
If NO Response
increase by 10mcg/min every 3-5min,up
200mcg/min
• Onset : 2-5min/DoA : 5-10min21

• Adverse effects/precautions:– Constant monitoring is essential
– Tolerance from uninterrupted use (12hr withdrawal)
– Headache, tachycardia, flushing
• Contra ind:– Concurrent use with PDE-5 inhibitors - causes significant
hypotension
– Head trauma/cerebral haemorrhage
– Severe anaemia
• Drug of choice:– Acute HF
– ACS
22

Nicardipine
• Ca channel blocker – selective arterial vasodilator
• Onset: 1-5min
DoA: 15-30min
Dose: start 5mg/hr IV infusion, titrate every
15min to max 15mg/hr.
23

Advantages:
• Cause cerebral and coronary vasodilatation
• Precautions: can worsen/cause HF and
liver failure
can exacerbate renal insuff.
• Ideal for CNS emergencies
24

Fenoldapam
MoA:
• Peripheral dopamine agonist (high vs low doses)
causes selective neuro vasodilatation
• mesenteric vasodilatation
• increases renal blood flow and sodium excretion
Onset – <5min, but more gentle, lasts for 30min
Standard BP monitoring is sufficient, no toxic
metabolites
25

Dosing:
• Start at 0.1-0.3mcg/kg/min IV infusion
• May be increased in increments of 0.05-
0.1mcg/kg/min every 15min, until target BP
reached
• Max infusion rate – 1.6mcg/kg/min
26

Precautions:
• Pts with glaucoma
• Dose related tachycardia can occur – angina
• Close BP monitoring
• Close K+ monitoring
• Caution with raised ICP
Drug of choice
• Renal insufficiency
• Stroke ( combination with nicardipine)
27
HydralazineMoA:
• Decreases systemic resistance by direct vasodilation
of arterioles
Dose:
• 5-20mg IV bolus or 10-40mg IM repeat every 4-6hrs
• boluses takes 20min to work
28

Adverse effects/Precautions
• Tachycardia, flushing, headache
• Sodium and water retention
• Increased ICP
• Adjust dose in severe renal dysfunction
• Response may be delayed and unpredictable
• Still drug of choice in pregnancy(Eclampsia)
29

Enalaprilat
• The active component of Enalapril (hydrolyzed in liver
and kidney)
MoA:
• ACE inhibitor
Dose:
• 0.625-2.5mg every 6hr IV
• Onset – within 30 min + long half life
Adverse effects/Precautions
• Contra-indicated – volume depletion, renal vascular
disease
• Prolonged t½ 30

Labetalol
MoA:
• selective alpha blocker – reduce vascular smooth
m. resistance
• non-selective Beta blocker – ↓ cardiac inotropy and
myocard O2 consumption → prevent reflex
tachycardia
31

Dose:
Bolus: effect in 5-10min,max effect at 20min. (DoA:
2-6hrs).
• Cont. infusion: 0.5 – 2mg/min – titrate to
response, max 300mg
• Difficult to titrate due to very wide dose range
32

Advantages:
• smooth onset
• Transition to oral Rx easy (dose equivalent)
• Improve cerebral blood flow – stroke pt
• No need for ICU/Arterial line
33

• Adverse effects/precautions
– Relative CI – Heart failure, heart block, Asthma (bronchoconstriction)
– Vomiting, scalp tingling
– Impaired hepatic function
• Contraindicated in HPT secondary to Cocaine use
(B-blocker effect outway the alpha effect, thus unapposed alpha constriction)
• Drug of choice:
– Aortic dissection
– Hypertensive emergencies
34

Esmolol
MoA:
• highly selective beta blocker
Dose:
bolus: 250-500mcg/kg IV over 1-3min
• infusion: 50-100mcg/kg/min
• may repeat bolus after 5min or increase
infusion rate to 300mcg/kg/min
Onset 1-2min / short acting
35

Adverse effect/Precautions
• Hypotension common
• nausea
• Asthma
• 1st degree AV block
• heart failure
36

Contraindications
• Sinus bradycardia
• Heart block
• Cardiogenic shock
• Bronchial asthma
• Uncompensated CF
Drug of choice:
• Aortic dissection ( with nitrate)
37

Phentolamine
MoA:
• alpha adrenergic receptor blocker
Dose:
• load 5-20mg IV every 5min or
• infusion 0.2-0.5mg/min
• Onset 1-2min
Adverse effect/precautions
• tachycardia
• flushing/headache
• MI
• cerebrovascular spasm38

• Contra-indications– renal impairment
– Concurrent use with PDE-5 inhibitors
– coronary or cerebral arteriosclerosis
• Drug of choice– Cocaine associated HPT crisis
– Pheochromocytoma HPT crisis
39

Neurological emergencies
40

Hypertensive encephalopathy
– reduce MAP by 25% or diastole to 100mmHg
over 8 hrs
– If neurology worsens, suspend Rx
– Drug of choice:
• Sodium nitroprusside
• Labetalol
41

Acute Ischemic stroke
• often loss of cerebral autoregulation
• ischemic region more prone to hypoperfusion
• thus BP reduction not recommended
• unless SBP>220 or DBP>120
• UNLESS planning fibrinolysis – SBP<185
and DBP< 110
Drug of choice:
• Labetalol
• Nicardipine
• Sodium Nitroprusside
42

Acute ICH/SAH
• Treatment based on clinical/radiographic
evidence of raised ICP
• Raised ICP – MAP<130 (1st 24hrs)
• No raised ICP – MAP<110
Drug of choice:
• Sodium Nitroprusside
• Labetalol
• Nicardipine
43

Cardiovascular emergencies
44

ACS• Treat if SBP>160 and or DBP>100
• Reduce MAP by 20 -30% of baseline
• Nitrates should be given till symptoms
subside or until DBP<100
Drug of choice:
• Nitroglycerine
• Labetalol
• Nicardipine
45

Acute HF (pulmonary edema)
• Treat with vasodilator (additional to diuretics)
• Sodium Nitroprusside in conjunction with
• Morphine, oxygen and loop diuretic
• Enalaprilat also an option
46
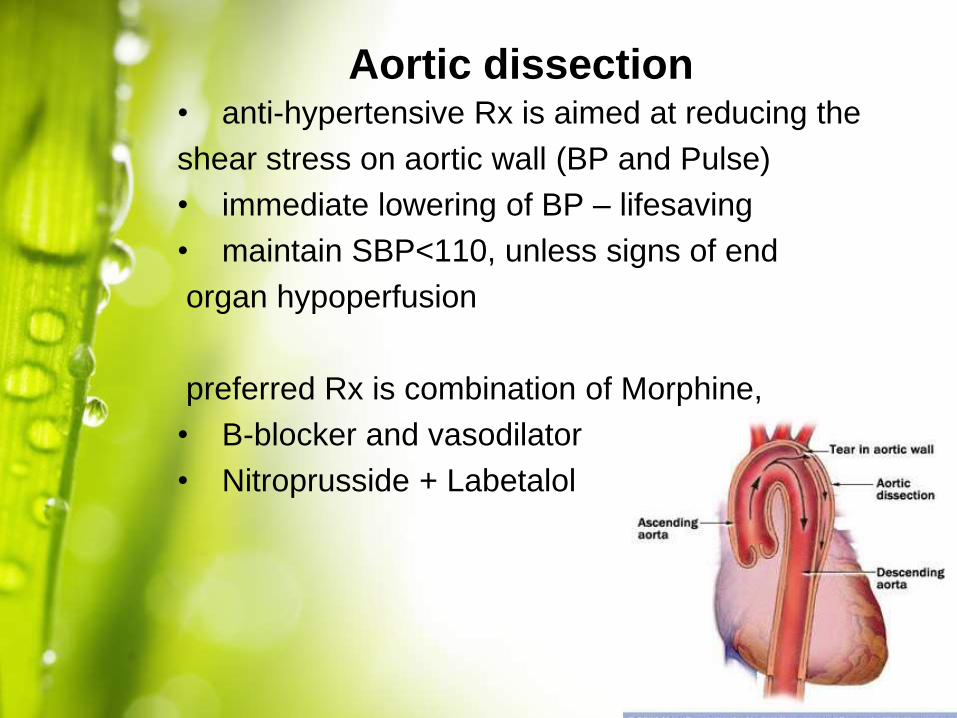
Aortic dissection• anti-hypertensive Rx is aimed at reducing the
shear stress on aortic wall (BP and Pulse)
• immediate lowering of BP – lifesaving
• maintain SBP<110, unless signs of end
organ hypoperfusion
preferred Rx is combination of Morphine,
• B-blocker and vasodilator
• Nitroprusside + Labetalol
47

Other disorders
48

Cocaine toxicity/pheochromocytoma
– Hpt and tachycardia rarely require specific Rx
– Alpha adrenergic blockers – preferred
– B – blockers can be added, but only after
alpha blockade.
Drug of choice
• Phentolamine
• Labetalol
• Diazepam
49

Pre-eclampsia/Eclampsia
– Goal SBP<160 and DBP<110 in pre-and-
intrapartum periods.
– Platelets < 100 000, BP should be maintained <
150/100
– IV Magnesium to prevent seizures
Drug of choice:
• Methyldopa
• Hydralazine
50

Perioperative hypertension
– Target BP to within 20% of baseline, except if
potential for life threatening arterial bleeding
– Typically related to catecholamine surge post-
op.
Drug of choice:
• B-blocker
• Labetalol
51

52
References
• Goodman and Gilman – 12th edition
• Rang and Dales pharmacology 7th edition
• Textbook of medical pharmacology – Padmaja
udaykumar
• Hypertensive emergencies- Louis Muller
53

54

• Cheese reaction, cold remedy
55





























