Embed Size (px)
Citation preview
Pituitary Adenoma: How Registry and Statistical Learning Can Improve Care and Reduce CostsWilliam McDonald, MDMedical Director, Abbott Northwestern Laboratory

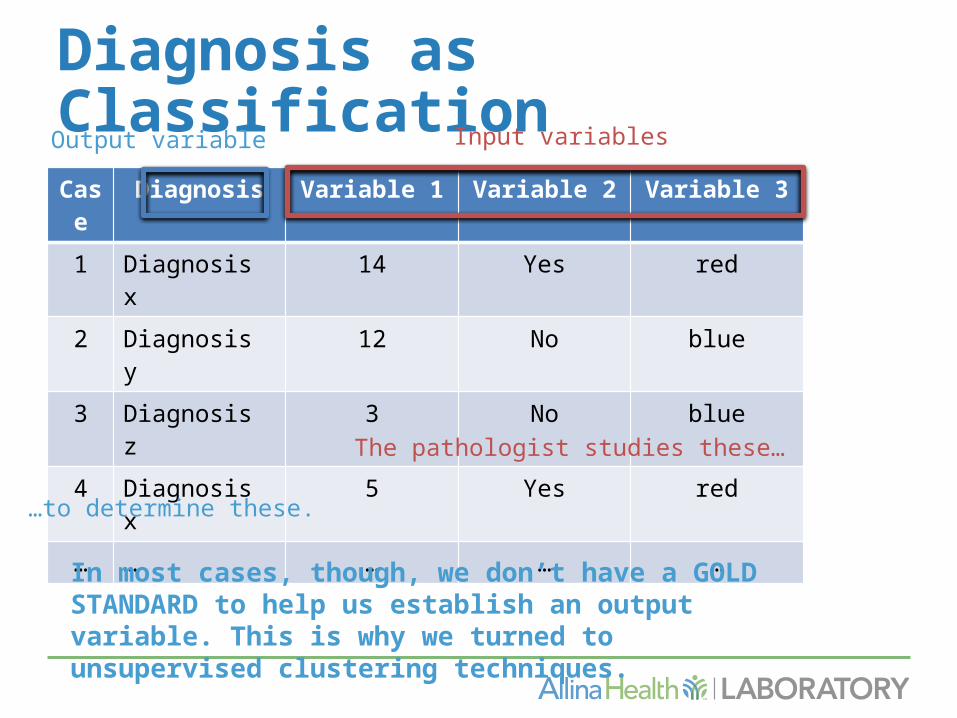
Diagnosis as ClassificationCase Diagnosis Variable 1 Variable 2 Variable 3
1 Diagnosis x 14.1 Yes red
2 Diagnosis y 12.0 No blue
3 Diagnosis z 3.7 No blue
4 Diagnosis x 5.3 Yes red
… … … … …
Output variable Input variables
The pathologist studies these…
…to determine these.
Generally, the greater the number of diagnostic classes and potential input variables, absent GOLD STANDARDS, the more cases are needed to make the classification scheme.

Pituitary Adenoma• 10-15% of intracranial tumors• May produce anterior pituitary
hormones or be hormonally silent• Six anterior pituitary hormones have
corresponding IHC of variable sensitivity and specificity: Prolactin, Growth Hormone, ACTH, FSH, LH, TSH
How Many Classes of Adenoma?• Dependent upon
- Local customs- Available reagents- Availability of electron microscopy- Availability of experts

Why Care About Adenoma Class?• Medical therapy is available for some
adenomas- Dopamine agonists like bromocriptine are
used for prolactinomas - Somatostatin analogs or growth hormone
receptor antagonist Pegvisomant are used to treat growth hormone and TSH-producing tumors
- Pasireotide (a somatostatin-receptor binding agent) in Cushing’s disease

Pituitary Adenoma Classification• Founded on case series, early IHC
and electron microscopy• Complex: up to +/- 18 classes• Canonical literature flawed by
reliance on secondary and tertiary sources, varying class definitions, poor correlation with radiology, serology

Pituitary AdenomasDiagnosis Stain1 Stain2 Stain3 …
Densely granulated corticotroph
+ - - …
Sparsely granulated corticotroph
+ - - …
Crooke cell adenoma
+ - + …
Densely granulated somatotroph
- +/- + …
… … … …
Input variables
Many of these… … and many of these, with no clear gold standards.
Output variable

What Input Variables?• A informal poll at the 2007 American
Association of Neuropathologists annual meeting revealed great variability in the workup of pituitary adenoma
• Workups ranged from 1 H&E-stained section to 4+ IHC with additional electron microscopy in some cases
(unpublished data)
Possible Stains (Partial List)• Prolactin• Growth hormone• ACTH• LH• FSH• TSH• Pit-1• SF-1• Alpha subunit• Tpit
• CAM5.2• Alpha ER• Synaptophysin• Chromogranin• S100• PAS• p53• MIB1/Ki67• Others

Problem and Our Strategy• Many classes• Variable class
definitions• Many input
variables• No consensus on
workup• Limited resources
• Tabulate underlying biology and available IHC
• Tissue microarray for N• Correlation and
clustering techniques• Develop a screening
panel and algorithm• Stepwise testing of
algorithm with clinical correlation

Pathways of Cell Differentiation in Adenohypophysis: Three Main Pathways

The Tissue Microarray

H&E
SF-1
Pit-1

Statistical Learning• Tools for understanding data• Emphasis on estimating an output based
on one or more inputs (supervised methods)
• Unsupervised methods used when output variable (tumor class, for instance) is unavailable
• Many software packages are now available• We used the free, open source program R

Correlation (Pearson’s r) Between IHC
Diagnosis as ClassificationCase Diagnosis Variable 1 Variable 2 Variable 3
1 Diagnosis x 14 Yes red
2 Diagnosis y 12 No blue
3 Diagnosis z 3 No blue
4 Diagnosis x 5 Yes red
… … … … …
Output variable Input variables
The pathologist studies these…
…to determine these.
In most cases, though, we don’t have a GOLD STANDARD to help us establish an output variable. This is why we turned to unsupervised clustering techniques.

Unsupervised Clustering• Used when an output variable
unavailable• Means of data visualization• Clustering attempts to find
homogeneous subgroups among the observations
• Hierarchical clustering and K-means clustering are the most popular

Hierarchical Clustering: Exploratory Set

Hierarchical Clustering: Validation Step
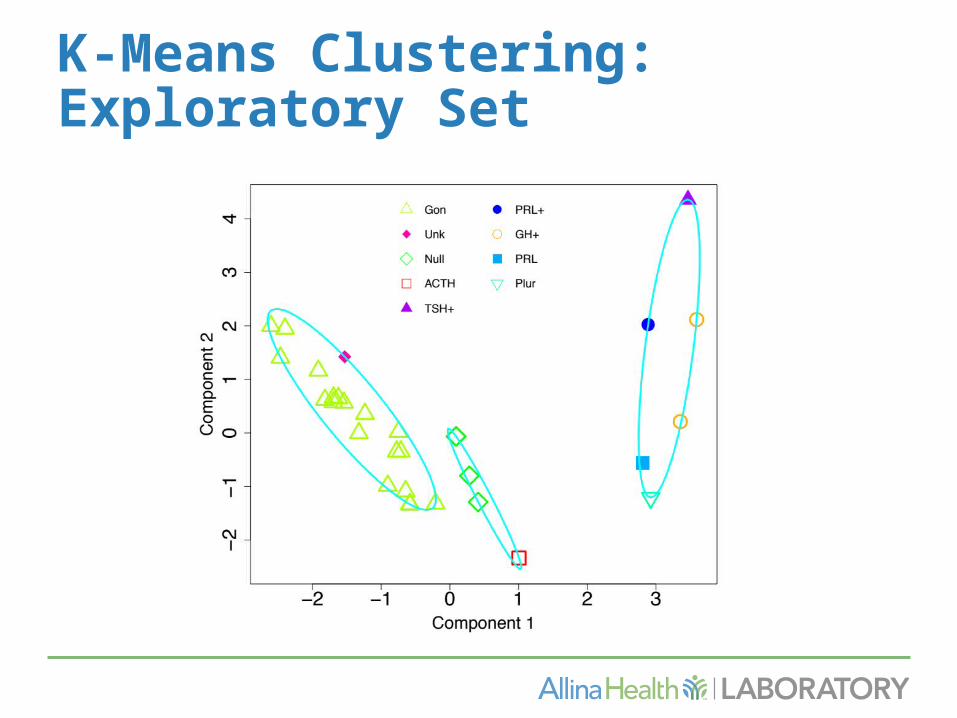
K-Means Clustering: Exploratory Set

K-Means Clustering: Validation Set
Developing the IHC Panel• Biology: three families• Correlations, cluster analysis• Screen Step of SF-1, Pit-1, ACTH• A thought experiment: iterative
testing using TMA data• New algorithm compared with old
algorithm

Testing the Algorithm

The Algorithm• SF-1(+)Pit-1(-)ACTH(-)=Gonadotroph• SF-1(-)Pit-1(-)ACTH(-)=“Null”• SF-1(-)Pit-1(-)ACTH(+)=Corticotroph• Other patterns or clinical/serological
discrepancy add PRL,GH,TSH,Cam5.2
• Note: all diagnoses are checked against clinical and serological information before final diagnosis

Conclusions• IHC results show patterns consistent
with developmental biology of adenohypophysis
• Pit-1 and SF-1 are robust markers of lineage in pituitary adenomas, and can augment or replace several traditional stains
• Alpha subunit was not useful in our hands

Conclusions, continued• Unsupervised statistical learning methods
appear to group cases into biologically relevant groups that corresponded to available clinical information
• By using an algorithm produced by our work, we estimate that - Greater than one-third of cases have a
more accurate diagnosis- One-third fewer IHC are used than in
our previous system
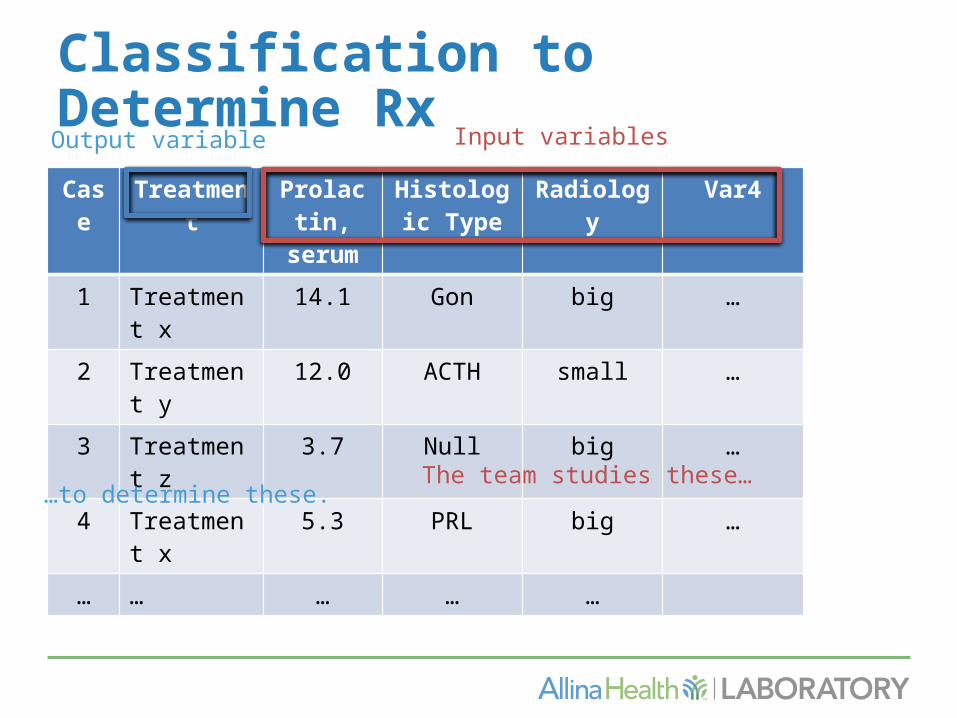
Classification to Determine RxCase Treatment Prolactin,
serumHistologic
TypeRadiology Var4
1 Treatment x 14.1 Gon big …
2 Treatment y 12.0 ACTH small …
3 Treatment z 3.7 Null big …
4 Treatment x 5.3 PRL big …
… … … … …
Output variable Input variables
The team studies these……to determine these.
Acknowledgements• Abbott Northwestern Hospital Foundation• JNNI Neuroscience Research Division
- Nilanjana Banerji, PhD- Bridget Ho, CCRC
• Allina Health Neuroscience Clinical Service Line- Kim Radel, MHA
• U of Illinois at Chicago- Virgilia Macias, MD- Andre Kajdacsy-Balla, MD, PhD
• Jared Crotteau, RN; Michelle Stenbeck, RN• Kelsey McDonald, PhD

References1. Allred DC, Harvey JM, Berardo M, Clark GM (1998) Prognostic and predictive factors in breast cancer by immunohistochemical analysis. Modern pathology : an official journal of the United States and Canadian Academy of Pathology, Inc 11 (2):155-1682. Asa S (2011) Tumors of the Pituitary Gland. AFIP Atlas of Tumor Pathology, vol 15. American Registry of Pathology, Washington, DC3. Asa SL, Bamberger AM, Cao B, Wong M, Parker KL, Ezzat S (1996) The transcription activator steroidogenic factor-1 is preferentially expressed in the human pituitary gonadotroph. J Clin Endocrinol Metab 81 (6):2165-2170.4. Asa SL, Puy LA, Lew AM, Sundmark VC, Elsholtz HP (1993) Cell type-specific expression of the pituitary transcription activator pit-1 in the human pituitary and pituitary adenomas. The Journal of clinical endocrinology and metabolism 77 (5):1275-12805. Chanson P, Salenave S (2004) Diagnosis and treatment of pituitary adenomas. Minerva endocrinologica 29 (4):241-2756. DeLellis RA, Lloyd RV, Heitz PU, Eng C (2004) World Health Organization Classification of Tumours. Pathology and Genetics. Tumours of Endocrine Organs. vol Book, Edited. IARC Press, Lyon, France7. Everitt BS, Landau S, Leese M, Stahl D (2011) Cluster Analysis. Wiley Series in Probability and Statistics, 5th edn. Wiley, West Sussex, United Kingdom
8. Friend KE, Chiou YK, Laws ER, Jr., Lopes MB, Shupnik MA (1993) Pit-1 messenger ribonucleic acid is differentially expressed in human pituitary adenomas. J Clin Endocrinol Metab 77 (5):1281-1286.9. Hartigan JA, Wong MA (1979) A K-means clustering algorithm. Journal of the Royal Statistical Society Series C (Applied Statistics) 28 (1):100-10810. Jentoft ME, Theis JD, Vrana JA, Dasari S, Dogan A (2013) Characterization of Pituitary Adenomas by Mass Spectrometry Based Proteomics. Paper presented at the 89th Annual Meeting of the American Association of Neuropathologists, Inc., Charleston, SC, June 201311. Kleinschmidt-DeMasters BK (2006) Subtyping does matter in pituitary adenomas. Acta neuropathologica 111 (1):84-85. doi:10.1007/s00401-005-1105-612. Kovacs K, Horvath E, Ryan N, Ezrin C (1980) Null cell adenoma of the human pituitary. Virchows Arch A Pathol Anat Histol 387 (2):165-174.13. Kovacs K, Scheithauer BW, Horvath E, Lloyd RV (1996) The World Health Organization classification of adenohypophysial neoplasms. A proposed five-tier scheme. Cancer 78 (3):502-510. doi:10.1002/(SICI)1097-0142(19960801)78:3<502::AID-CNCR18>3.0.CO;2-214. Lamolet B, Pulichino AM, Lamonerie T, Gauthier Y, Brue T, Enjalbert A, Drouin J (2001) A pituitary cell-restricted T box factor, Tpit, activates POMC transcription in cooperation with Pitx homeoproteins. Cell 104 (6):849-859.15. Luo X, Ikeda Y, Parker KL (1994) A cell-specific nuclear receptor is essential for adrenal and gonadal development and sexual differentiation. Cell 77 (4):481-490.16. Meehl PE (1986) Causes and effects of my disturbing little book. J Pers Assess 50 (3):370-375.17. Mete O, Asa SL (2012) Clinicopathological correlations in pituitary adenomas. Brain Pathol 22 (4):443-453. doi: 410.1111/j.1750-3639.2012.00599.x.18. Mete O, Asa SL (2013) Therapeutic implications of accurate classification of pituitary adenomas. Semin Diagn Pathol 30 (3):158-164. doi: 110.1053/j.semdp.2013.1006.1002.

19. Nose V, Ezzat S, Horvath E, Kovacs K, Laws ER, Lloyd R, Lopes MB, Asa SL (2011) Protocol for the examination of specimens from patients with primary pituitary tumors. Archives of pathology & laboratory medicine 135 (5):640-646. doi:10.1043/2010-0470-SAR1.120. Pellegrini I, Barlier A, Gunz G, Figarella-Branger D, Enjalbert A, Grisoli F, Jaquet P (1994) Pit-1 gene expression in the human pituitary and pituitary adenomas. J Clin Endocrinol Metab 79 (1):189-196.21. Pison G, Struyf A, Rousseeuw PJ (1999) Displaying a clustering with CLUSPLOT. Comput Stat Data Anal 30:381-39222. Pulichino AM, Vallette-Kasic S, Couture C, Gauthier Y, Brue T, David M, Malpuech G, Deal C, Van Vliet G, De Vroede M, Riepe FG, Partsch CJ, Sippell WG, Berberoglu M, Atasay B, Drouin J (2003) Human and mouse TPIT gene mutations cause early onset pituitary ACTH deficiency. Genes Dev 17 (6):711-716.23. Saeger W, Ludecke DK, Buchfelder M, Fahlbusch R, Quabbe HJ, Petersenn S (2007) Pathohistological classification of pituitary tumors: 10 years of experience with the German Pituitary Tumor Registry. European journal of endocrinology / European Federation of Endocrine Societies 156 (2):203-216. doi:156/2/203 [pii]; 10.1530/eje.1.02326 [doi]24. Shanteau J (1988) Psychological characteristics and strategies of expert decision makers. Acta Psychologica 68:203-215
Useful Web Resources• http://www.r-project.org• http://www.rstudio.com• https://google-styleguide.googlecode
.com/svn/trunk/Rguide.xml
• Ed Boone's R Channel on YouTube












![MR Imaging of Cavernous Sinus Involvement by Pituitary ...€¦ · abnormal pituitary gland and sellar region [13-16], only a few anecdotal cases of CSI by a pituitary adenoma have](https://img.dokumen.tips/doc/110x75/5ed565c51d25941f923a987c/mr-imaging-of-cavernous-sinus-involvement-by-pituitary-abnormal-pituitary-gland.jpg)