Embed Size (px)
Citation preview

OSTEOARTHRITISOSTEOARTHRITIS
Disorder of hyaline cartilage and Disorder of hyaline cartilage and subchondral bone, though all subchondral bone, though all tisues in and around involved tisues in and around involved
joints are hyperthrophic.joints are hyperthrophic.
IncidenceIncidence
The most common form of articular The most common form of articular disorder.disorder.
First appear asymptomatically in the 2nd First appear asymptomatically in the 2nd to 3rd decades and become universally by to 3rd decades and become universally by age 70.age 70.

ClassificationClassification
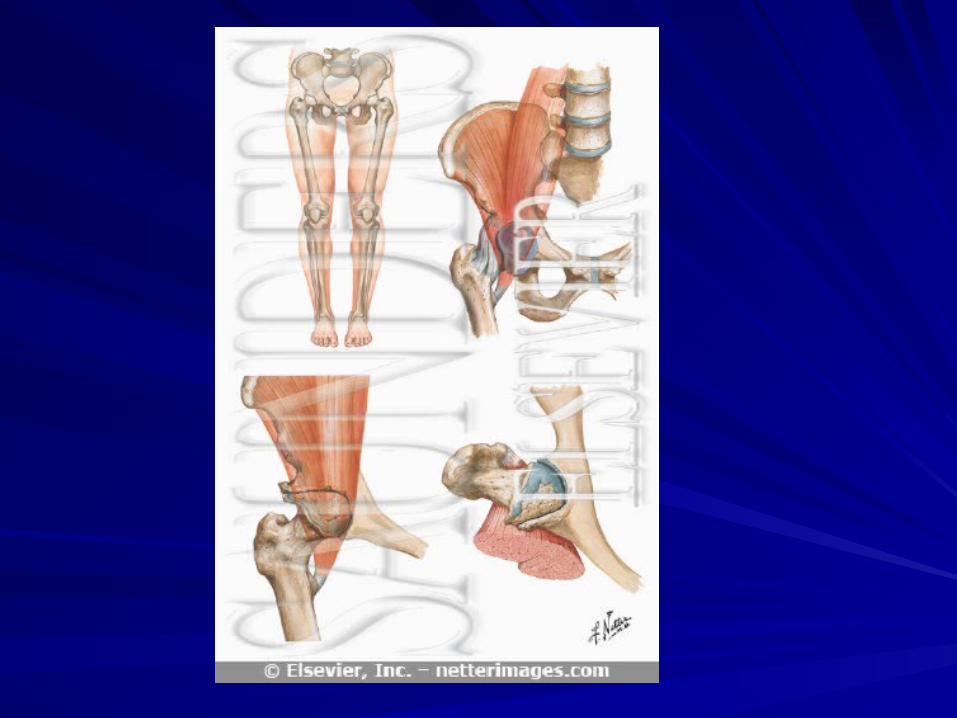
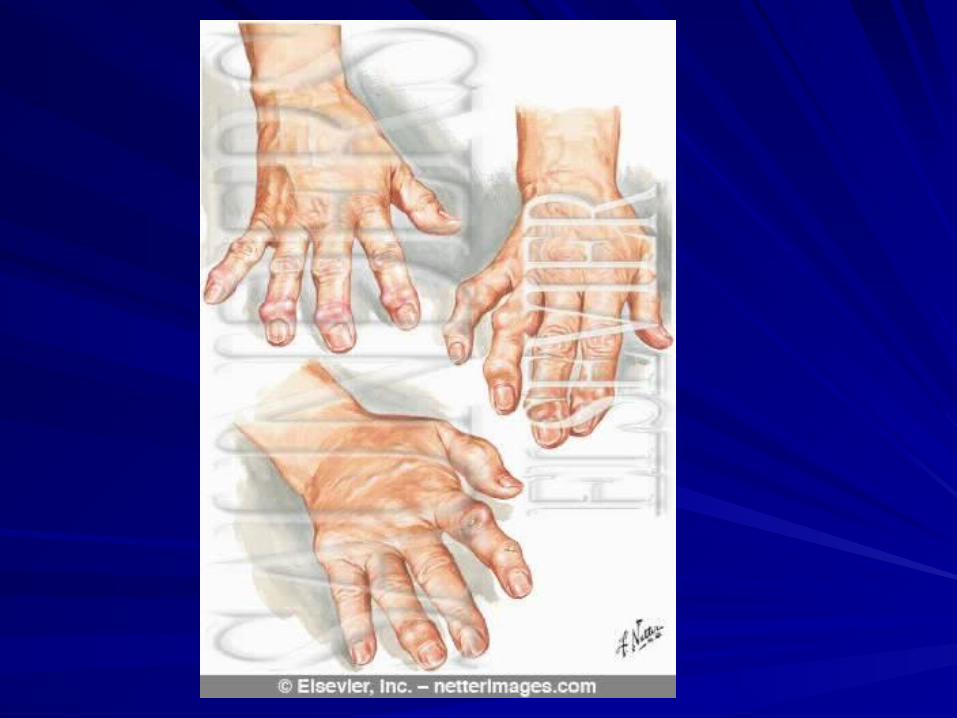
Oa is classified in 2 groups:Oa is classified in 2 groups:Primary OA: includes peripheral joints, notably Primary OA: includes peripheral joints, notably the distal IFJ and PIJ ( producing the distal IFJ and PIJ ( producing Heberden´s Heberden´s and Bouchard´s nodesand Bouchard´s nodes), 1st CMTJ, cervical and ), 1st CMTJ, cervical and lumbar spine.lumbar spine.1st MTPJ ( big toe), hips, knees, intervertebral 1st MTPJ ( big toe), hips, knees, intervertebral disks, zygapophyseal joints in the spine.disks, zygapophyseal joints in the spine.Several variants subset: Several variants subset: erosive, inflammatory erosive, inflammatory OA, DISH.OA, DISH.Secondary: according with the etiologySecondary: according with the etiology

EtiologyEtiology
Etiology is unknown.Etiology is unknown.
OA appears to be the result of a complex OA appears to be the result of a complex system of interacting , mechanical , system of interacting , mechanical , biologic, biochemical, and enzymatic biologic, biochemical, and enzymatic feedback loops.feedback loops.
When one or more fails, the clinical events When one or more fails, the clinical events follow.follow.
Cont;Cont;
Anything that change the microenvironment of Anything that change the microenvironment of the chondrocyte.the chondrocyte.
This includes congenital joint abnormalities, This includes congenital joint abnormalities, genetic defects, infectious, metabolic, endocrine, genetic defects, infectious, metabolic, endocrine, and neuropathic diseases.and neuropathic diseases.
Acute or chronic trauma including Acute or chronic trauma including fractures.Virtually any disease process that alter fractures.Virtually any disease process that alter the normal structure and function of hyaline the normal structure and function of hyaline cartilage.cartilage.

PathophysiologyPathophysiology
Hyaline cartilage is avascular, aneural, Hyaline cartilage is avascular, aneural, and alymphatic.and alymphatic.
Chondrocyte divide and increase their Chondrocyte divide and increase their rates of both synthesis and degradative rates of both synthesis and degradative process, they have the longest cell cycle in process, they have the longest cell cycle in the body.the body.
Never dividing unless some alteration Never dividing unless some alteration occurs in the microenviroment.occurs in the microenviroment.

Cont;Cont;
Cartilage heal depends on the pumpimg Cartilage heal depends on the pumpimg action ( compression and release) of action ( compression and release) of weight-bearing and use.weight-bearing and use.Inital event in OA : mitosis of chondrocyte Inital event in OA : mitosis of chondrocyte with increased synthesis of the with increased synthesis of the proteoglycans and type ll collagen.proteoglycans and type ll collagen.Decrease in concentration of Decrease in concentration of proteoglycans in the inmediate proteoglycans in the inmediate neighborhood of the chondrocyte.neighborhood of the chondrocyte.
Cont;Cont;
Second event: Increased synthesis of Second event: Increased synthesis of bone by osteoblasts in the subchondral bone by osteoblasts in the subchondral bone by intercommunication between bone by intercommunication between chondrocyte and osteoblasts in the chondrocyte and osteoblasts in the subchondral bone cells.subchondral bone cells.With increased bone formation in the With increased bone formation in the subchondral area, physical propierties subchondral area, physical propierties change, the bone become stiffer, and change, the bone become stiffer, and microfractures occur.microfractures occur.
Cont;Cont;
With microfractures comes callus With microfractures comes callus formation and hence more stiffness and formation and hence more stiffness and more microfracture.more microfracture.
Third event: metaplasia of the peripheral Third event: metaplasia of the peripheral synovial cells resulting in formation of synovial cells resulting in formation of osteochondrophytes ( combination bone, osteochondrophytes ( combination bone, connective tissue, fibrocartilage and island connective tissue, fibrocartilage and island of hyaline cartilage on the surface.of hyaline cartilage on the surface.
Cont;Cont;
Fourth event: formation of bony cysts Fourth event: formation of bony cysts
( Pseudocysts) in the marrow below the ( Pseudocysts) in the marrow below the subchondral bone.subchondral bone.
The mechanism is that extrusion of joint The mechanism is that extrusion of joint fluid trough the hyaline cartilage clefts into fluid trough the hyaline cartilage clefts into the marrow with fibroblastic, osteoblastic the marrow with fibroblastic, osteoblastic cellular reaction around the synovial fluid.cellular reaction around the synovial fluid.
Cont;Cont;
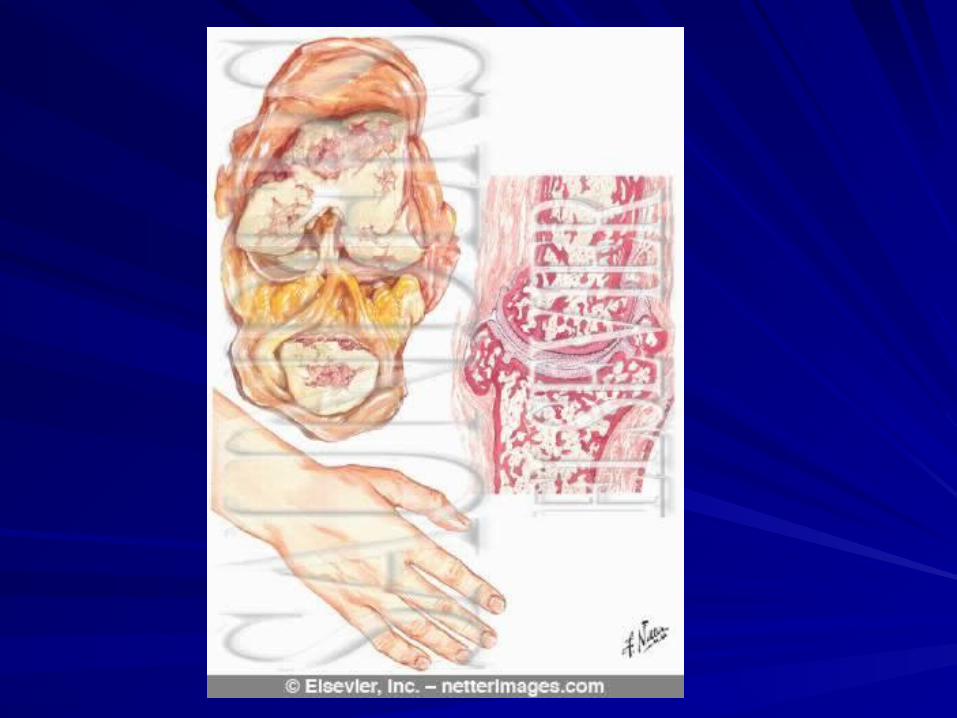
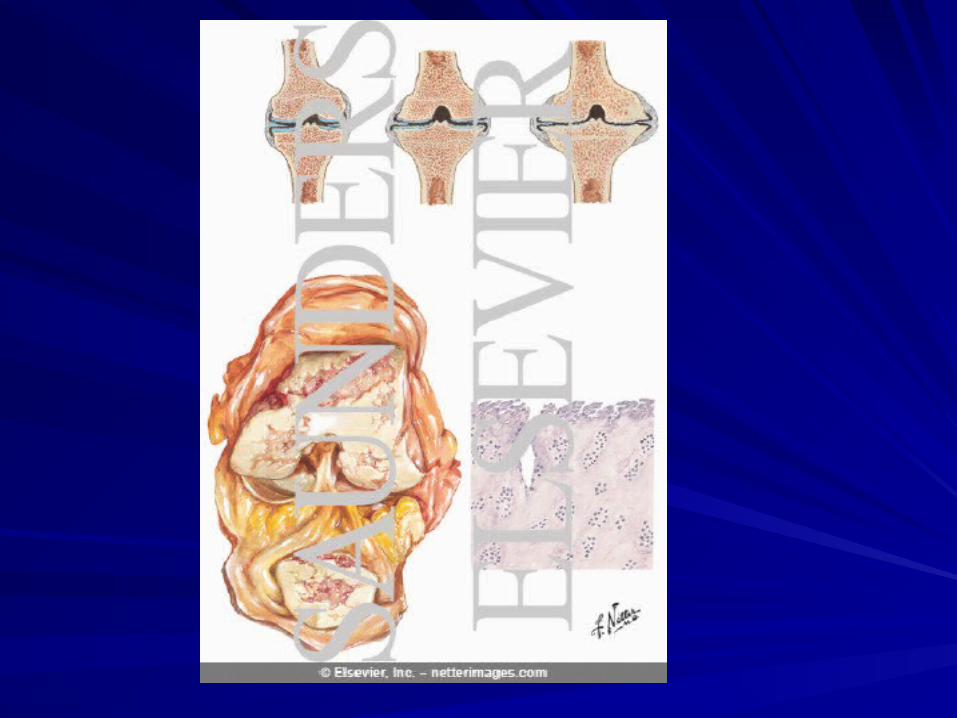
The gross pathology: The gross pathology: roughening or loss of roughening or loss of surface of the hyaline cartilage, pitting, surface of the hyaline cartilage, pitting, and irregularities, proceeding the gross and irregularities, proceeding the gross ulceration with a first focal, diffuse area of ulceration with a first focal, diffuse area of loss of cartilage surface.loss of cartilage surface.
Proliferation of new bone, capsule tendon, Proliferation of new bone, capsule tendon, cartilage, and synovium occur.cartilage, and synovium occur.

Cont;Cont;
Deterioration and loss of bearing surface, Deterioration and loss of bearing surface, proliferation of all osteoarticular tissue at proliferation of all osteoarticular tissue at the margin of the joints and under the the margin of the joints and under the detached joint surface.detached joint surface.
All cases have active synovial proliferation All cases have active synovial proliferation and synovitis.and synovitis.
Symptoms and signsSymptoms and signs
Initially, OAInitially, OA..is noninflammatory and onset ..is noninflammatory and onset subtle gradual, usually involving one to subtle gradual, usually involving one to only a few joints. only a few joints.
Pain is the earliest symptom, usually made Pain is the earliest symptom, usually made worse by exercise.worse by exercise.
Morning stiffness follow inactivity but last Morning stiffness follow inactivity but last in 15-30 min, improve with exercise.in 15-30 min, improve with exercise.
Cont;Cont;
Acute episodes of severe synovitis may Acute episodes of severe synovitis may occur in those who have gout or occur in those who have gout or pseudogout.pseudogout.
As the disease progresses joint motion As the disease progresses joint motion become diminshed, flexion contracture become diminshed, flexion contracture occur, tenderness and crepitus or grating occur, tenderness and crepitus or grating sensation appear.sensation appear.
Cont;Cont;
Joint enlargement induce by the Joint enlargement induce by the proliferative reaction of cartilage, bone proliferative reaction of cartilage, bone ligament, tendon, capsules, and chronic ligament, tendon, capsules, and chronic synovial proliferation and inflammation is synovial proliferation and inflammation is ultimately characteristic of OA.ultimately characteristic of OA.
As ligament become lax, the joint has As ligament become lax, the joint has increasing instability with more local pain, increasing instability with more local pain, and cliniical appearance of a limpand cliniical appearance of a limp

Cont;Cont;
Tenderness on palpation and pain on Tenderness on palpation and pain on passive motion are late signs muscle passive motion are late signs muscle spams and contracture add to the pain.spams and contracture add to the pain.
Mechanical block, deformities and Mechanical block, deformities and subluxations, subchondral bone collapse, subluxations, subchondral bone collapse, osteochondrophytes, muscle atrophy and osteochondrophytes, muscle atrophy and pseudocysts.pseudocysts.
Cont;Cont;
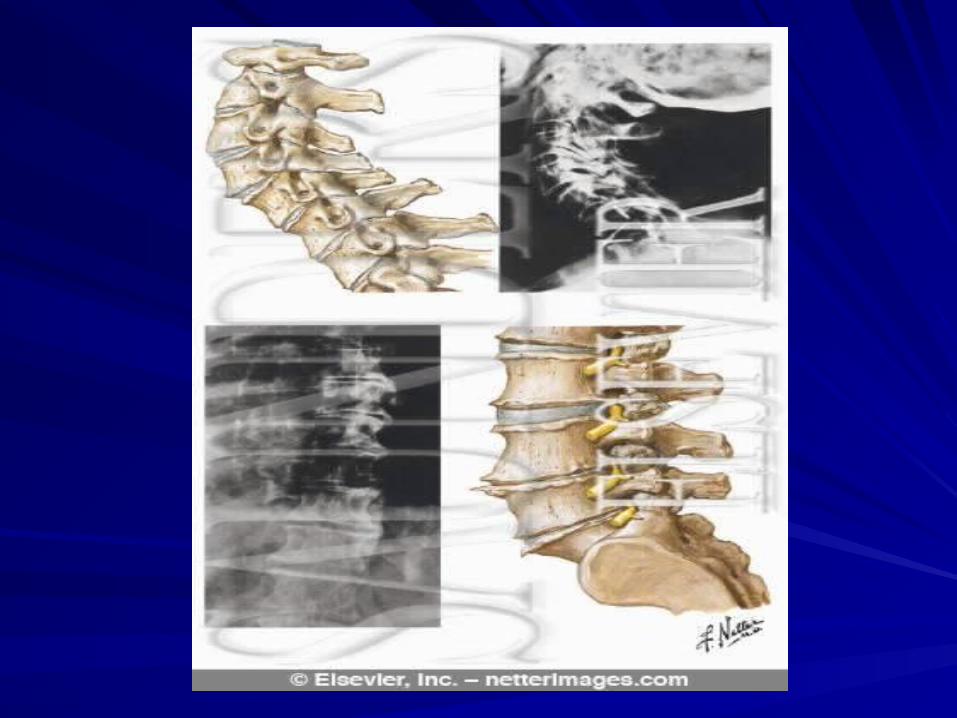
OA of the cervical and lumbar spine: is OA of the cervical and lumbar spine: is common. In the cervical spine the common. In the cervical spine the symptoms may be related to radiculitis by symptoms may be related to radiculitis by compression of nerve roots secondary to compression of nerve roots secondary to proliferative osteochondrophytes, proliferative osteochondrophytes, functional compromise of the vertebral functional compromise of the vertebral artery, neuromyopathy secondary to artery, neuromyopathy secondary to compresion, spinal cord infarcts or compresion, spinal cord infarcts or esophageal compression, by anterior esophageal compression, by anterior bony projection.bony projection.
DiagnosisDiagnosis
Based on symptoms and signs or by X-ray Based on symptoms and signs or by X-ray in asymptomatic patients.in asymptomatic patients.
Laboaratory and X-ray studies:Laboaratory and X-ray studies:
ESR is normal or moderately increased.ESR is normal or moderately increased.
X-ray and radiologic criteria:X-ray and radiologic criteria:
A) Irregular or asymmetric narrowing of A) Irregular or asymmetric narrowing of the joint space.the joint space.

Cont;Cont;
B)- Increased in radiologic density of the B)- Increased in radiologic density of the subchondral bone.subchondral bone.C)-Formation of osteochondrophytes at the C)-Formation of osteochondrophytes at the periphery of joints.periphery of joints.D) Formation of Pseudocysts in the subchondral D) Formation of Pseudocysts in the subchondral bone marrow.bone marrow.Differential diagnosis: RA, AKS, Psoriatic Differential diagnosis: RA, AKS, Psoriatic arthritis, seronegative spondyloarthropathies, arthritis, seronegative spondyloarthropathies, crystal deposits, endocrine, metabolic and crystal deposits, endocrine, metabolic and neoplastic disorders affecting the bone.neoplastic disorders affecting the bone.

Prevention and treatmentPrevention and treatment
The most modifiable risk factor is the The most modifiable risk factor is the obesity.obesity.The goals in the treatment of OA are the The goals in the treatment of OA are the relieve of pain, improve function and relieve of pain, improve function and prevent disability.prevent disability.Patient educationPatient educationPhysical measures: exercise, supportive Physical measures: exercise, supportive devices, alteration in DA, thermal devices, alteration in DA, thermal modalities and psychosocial measures.modalities and psychosocial measures.
Pharmacology therapyPharmacology therapy
Topical agents: Capsaicin ( depletion of Topical agents: Capsaicin ( depletion of substance P, neurotransmitter), topical substance P, neurotransmitter), topical NSADs.NSADs.
Systemic oral agents: acetaminophen, Systemic oral agents: acetaminophen, tramadol, codeine, dextropropoxyphene.tramadol, codeine, dextropropoxyphene.
Etoricoxib, lumiracoxib, celecoxib.Etoricoxib, lumiracoxib, celecoxib.
Nutraceuticals: nutricional supplements Nutraceuticals: nutricional supplements with potential pharmacologic value.with potential pharmacologic value.

Cont;Cont;
Glucosamine sulphate, chondroitin Glucosamine sulphate, chondroitin sulphate, S- adenosylmethionine (SAM-e) sulphate, S- adenosylmethionine (SAM-e) MSM ( methylsulphonylmethane), shark MSM ( methylsulphonylmethane), shark cartilage, cat´s claw.cartilage, cat´s claw.Adyuvants agents: tricyclic antidepresants, Adyuvants agents: tricyclic antidepresants, antispasmodics, injection of lidocaine or antispasmodics, injection of lidocaine or depot corticosteroids.depot corticosteroids.Intrarticular therapy: Hyaluronan and Intrarticular therapy: Hyaluronan and corticoids.corticoids.

Cont;Cont;
Structure disease modifying agents:Structure disease modifying agents:
These substances retard the progression These substances retard the progression of OA and/or enhance a normal reparative of OA and/or enhance a normal reparative process.process.
These agents are categorized as follow:These agents are categorized as follow:
Growth factors and cytokinesGrowth factors and cytokines
Sulfated and non-sulfated sugars.Sulfated and non-sulfated sugars.
Hormones and other steroidsHormones and other steroids

Cont;Cont;
Enzyme inhibitors: glucosamine sulfate, Enzyme inhibitors: glucosamine sulfate, metalloproteinases inhibitors such as metalloproteinases inhibitors such as tetracyclines, growth factors and cytokines tetracyclines, growth factors and cytokines and chondrocyte stem system and chondrocyte stem system transplantation.transplantation.
Collagenase inhibitors.Collagenase inhibitors.
Surgical intervention: for intractable pain, Surgical intervention: for intractable pain, and restoration of compromised function.and restoration of compromised function.

Cont:Cont:
Total hip and knee arthroplasties, Total hip and knee arthroplasties, osteostomies, arthroscopy intervention osteostomies, arthroscopy intervention
surgical arthroscopy for repair and for surgical arthroscopy for repair and for partial removal of damaged menisci, partial removal of damaged menisci, arthroscopy lavage.arthroscopy lavage.