Embed Size (px)
Citation preview

©Sylvain Chamberland
Orthognathic surgeryA visual aid of what happen.
slideshare.net/sylvainchamberland

©Sylvain Chamberland
Le Fort 1 Osteotomy
• Osteotomy half way between apices of the teeth and infraorbital nerve
Courtesy Dr Carl Bouchard
Piriform rimZygomatic buttress
Infraorbital nerve

©Sylvain ChamberlandDistal to canine cuts
Le Fort 1 Osteotomy
• Down fracture of the maxilla viewed from above
! The maxilla has been separated down from the skull
! Ostetomy cuts are done each side of the mid palatal suture and distal to the canine
Courtesy Dr Martin Gaboury
1 2
3
4
Parasagittal cuts

©Sylvain Chamberland
Segmentation of the maxilla
• When transversal expansion is needed, the maxilla is segmented
! Islet 1, 2, 3 are the 3 segmented part of the maxilla
! Islet 4 is the midpalatal suture
! Blood flow is maintained by soft tissue from the palate and soft palate
Courtesy Dr Martin Gaboury
1 2
3
4
Parasagittal cuts
Distal to canine cuts

©Sylvain Chamberland
Le Fort 1 Osteotomy
• Autogenous corticospongious bone grafting
! Donor site are either the malar bone or the mandibular ramus. Iliac crest can be used.
! Demineralized allogenic bone particles fills the interstice
Courtesy Dr Martin Gaboury
Sinus floor Cortocospongious bone
Allogenic bone particles
©Sylvain Chamberland
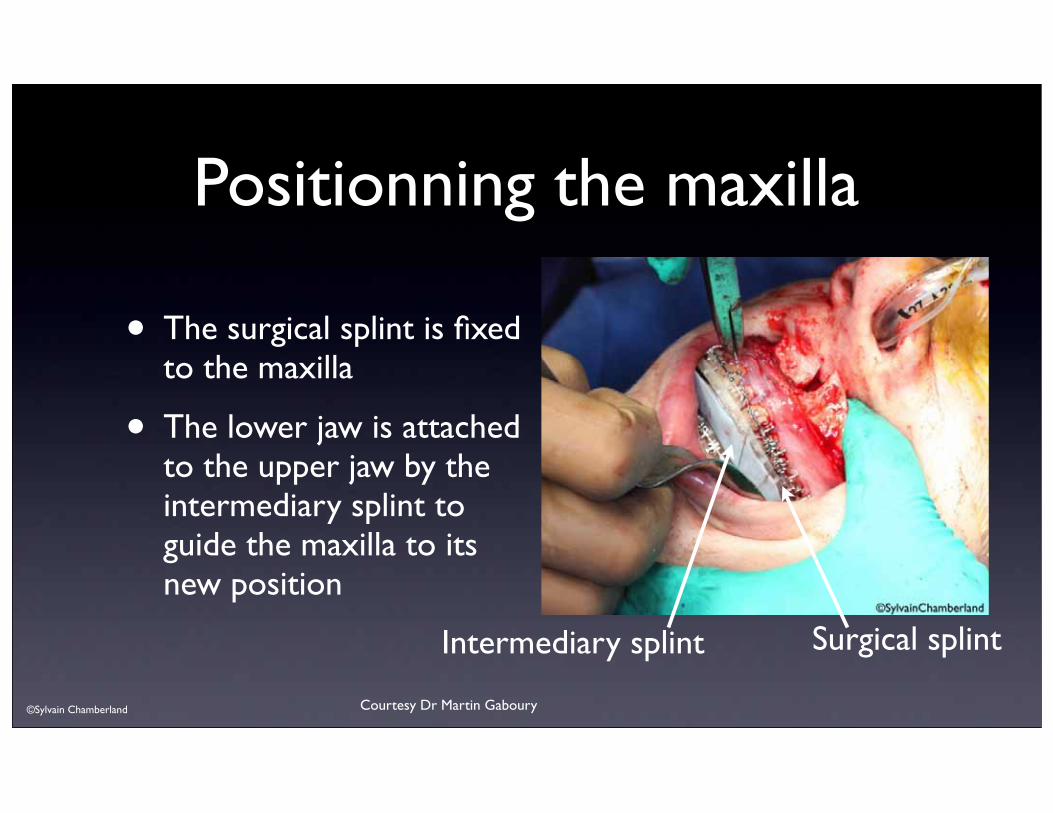
Positionning the maxilla
• The surgical splint is fixed to the maxilla
• The lower jaw is attached to the upper jaw by the intermediary splint to guide the maxilla to its new position
Courtesy Dr Martin Gaboury
Surgical splintIntermediary splint
©Dr Sylvain Chamberland
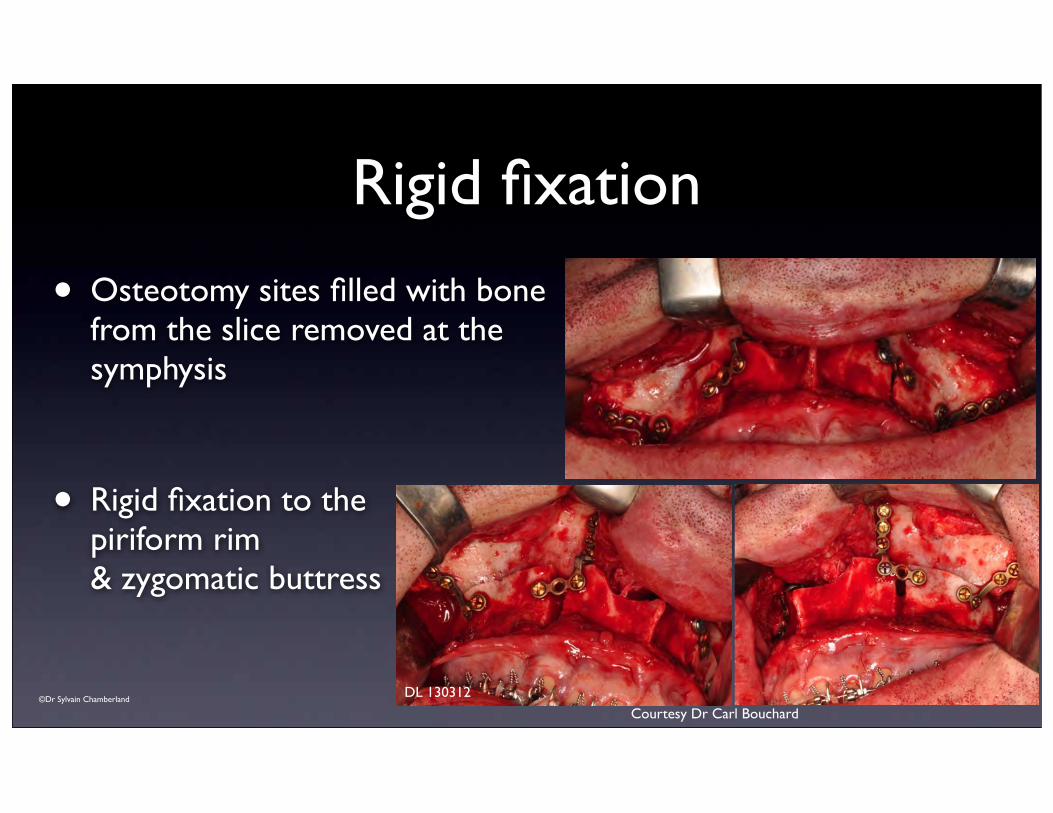
Rigid fixation
• Osteotomy sites filled with bone from the slice removed at the symphysis
• Rigid fixation to the piriform rim & zygomatic buttress
Courtesy Dr Carl Bouchard
DL 130312

©Dr Sylvain Chamberland
Bilateral sagittal split osteotomy
• Osteotomy cut vertically extending down near the 1st molar and horizontally extending posteriorly to the ramus
• 3 bicortical screws on each side
Courtesy Dr Carl Bouchard

©Dr Sylvain Chamberland
Genioplasty
• Pre-bended 6 mm monocortical plate
• 2 lateral cortical plates to avoid rotation of the distal segment and improve bone contact
Courtesy Dr Carl Bouchard
Mental nerve

©Dr Sylvain Chamberland
Genioplasty
• Wire fixation for genioplasty
! This avoid having any fixation in the resorptive zone
! The twisted part of the wires will be embed by bone apposition
• Note the amount of advancement obtained
Courtesy Dr Dany Morais

©Dr Sylvain Chamberland
Why I don't like rigid fixation for a genioplasty
Poor contact between distal & proximal segment
Screw EmbedLu.Mo.010710 Lu.Mo.130212
Note bone formation over superior portion of fixation device and resorption in area of inferior
portion of fixation device
Screw in the resorptive zone
Apposition zone
Screw prominent

©Dr Sylvain Chamberland
• Lack of bone contact between distal and proxmial segment
• Horizontal rotation of distal segment to the right
• Notch on the left side of the chin
This surgery was NOT performed in Quebec

©Dr Sylvain Chamberland
Courtesy Dr Dany Morais
Why do I prefer osteosynthesis?
Resorptive zone
R: RemodelingA: Apposition
De.Le060608 De.Le130410
Resorptive zone
Apposition zone
Improved contact between proximal and distal segment
Precious D., Armstrong J., Morais D., Anatomic placement of fixation device in genioplasty, OOO 1992,; 73-2-8
Note complete coverage of fixation wires by bone and smooth labial
cortical bone of anterior manbible

©Dr Sylvain Chamberland
Why I don't like posterior openbite after orthognathic
surgery?
• Lack of posterior occlusion may increase pressure at the condyle and cause non-physiologic remodeling or condylar resorption
Jam-packedScrewed Setting occlusion
Pressure
The bite openSlight progressive
retrusion
Condyle resorb







![Hochfrequenz- Chirurgie - · PDF file8 I HF-Chirurgie HF-Chirurgie I 9 Anschlusskabel für die HF-Chirurgie Anschlusskabel für die HF-Chirurgie Geräteseite Länge [m] Stück/VE Artikel-Nr](https://img.dokumen.tips/doc/110x75/5a789cba7f8b9ae91b8cdb80/hochfrequenz-chirurgie-i-hf-chirurgie-hf-chirurgie-i-9-anschlusskabel-fr-die.jpg)