Embed Size (px)
Citation preview

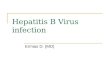
Occult hepatitis B virus infection

phases HBeAg HBV DNA
level
Aminotransfer
ases levelsliv.necroinf-
lamation
Fibrosis
progression
Immunotolerant + High normal No or mild No
Immunoreactive + High Increased or
fluctuating
Moderate to
severe
Rapid
Inactive carier st. _ Low Normal Very low
HBeAg - CHB _ High High Yes
HBsAg – phase
(Occult BI)
Very low or
undetectable
?? ??
recovered (immune) subjects following self limited acute HB

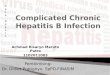
Occult hepatitis B virus infection (OBI)

Definition of OBI

HBs AG Undetectable
Intrahepatic HBV DNA
HBV DNA Detectable +/-

HBsAG - & HBV DNA +
80% 20%Seropositive OBI Seronegative OBI
( anti-HBc+ (+/-) anti-HBs+) ( anti-HBc - , anti- Hbs -)
higher DNA level lower DNA level
recovered (immune) subjects following self limited acute HB

Seropositive
Anti-HBc positive
HBsAg lost after
self-limiting acute
hepatitis
HBsAg lost after
years of chronic
carriage
Anti-HBV never
present
(Iry occult infection)
Seronegative
Anti-HBc negative
Anti HBV antibodies
progressively
disappear over time
OBI

“False” OBI
HBsAg negative & positive serum DNA levels comparable to levels in overt HBV infection.
Infection with HBV mutations in S gene (escape mutants ), producing a modified HBsAg that is not recognized by some or all commercially available detection assays
Raimondo G, et al,. J Hepatol 2008; 49: 652-65
the use of multivalent anti-HBs antibodies in the HBsAg assays is strongly recommended for optimal detection of these variants

Long lasting persistence of HBV ccc –DNA.Levrero M, et al. J Hepatol 2009; 51: 581-592
Viral replication is strongly suppressed:-High HBV-specific immunological pressure- Co-infection with other pathogens- Epigenetic factors
Zerbini A, et al, . Gastroenterology 2008; 134: 1470-1481
Larrubia JR .World J Gastroenterol 2011 March 28; 17(12): 1529-1530,
Recovered (immune) subjects following self limited acute HB

Gold Standard : Analysis of liver tissue and blood for HBV DNA
HBV DNA in blood by nested-PCR, real-time PCR, and transcription based mediated amplification (TMA)
Anti-Hbc is a less than ideal surrogate marker when HBV DNA measurement is not feasible.
Raimondo G, et al,. J Hepatol 2008; 49: 652-65

Auther Diagnosis of OBI Target population OBI Prevalence
El-shaarawy,et al, 2007 Anti-HBc 40 pat. With HCV CLD 50%
El-Sherif, et al, 2009 Anti-HBc/
DNA
71HCV pat.+ Anti-HBc+
29 HCV pat.+ Anti-HBc -
22.5%
0%
Said, et al, 2009 DNA 100 child with
haematological dis.
38%
Ismail, et al, 2010 DNA Haemodialysis
46 HCV RNA +
52 HCV RNA-
6.3%
3.8%
Emara, et al, 2010 DNA 156 HCV pat. On peg-INF 3.9%
Hassan, et al, 2011 DNA 40 HCC : tissue
serum
62.5%
22.5%
Selim, et al, 2011 DNA HCV : 30 enzyme flare
30 no enzyme flare
63.3%
13.3%
Abu-elmakarem,
et al,2012
DNA 145 haemodialysis 4.1%
Said, et al, 2013 Anti-HBc/
DNA
3167 blood donors
303 Anti-HBc +
Anti-HBc +14.2%
17.2%

Transmission Of HBV infection
HCC OBI HBVdevelopment reactivation
Liver disease progression

Target populations.
Antiviral Therapy.

OBI is a phenomenon essentially attributed to the long-lasting presence of HBV cccDNA into the hepatocytes and to a strong inhibition of HBV replication and protein synthesis.
Considering the very low levels of serum HBV DNA, its detection requires the use of a highly sensitive and specific molecular biology techniques.
The inhibition of HBV replication may be reversible and the occult infection may be reactivated, leading to acute and severe forms of classical hepatitis B, which may also occur after transmission of OBI by blood transfusion or organ transplantation.
The long-term persistence of the virus in the liver may induce a very mild but continuing necroinflammation that if other causes of liver injury co-exist - may favor the progression of the chronic liver disease toward cirrhosis.
Moreover, OBI seems to maintain the tumorigenic properties typical of the overt infection, and it is in fact an important risk factor for HCC development.