Embed Size (px)
Citation preview

Novel Trends In Novel Trends In Hemodialysis Vascular Hemodialysis Vascular
AccessAccess
MOATAZ FATTHY MDLecturer of Internal MedicineCairo University
• HISTORY• MODALITIES• IMAGING• NOVEL TRENDS• WHERE WE STAND• TAKE HOME
MESSAGE

• HISTORY• MODALITIES• IMAGING• NOVEL TRENDS• WHERE WE STAND• TAKE HOME
MESSAGE
• A Dutch physician, Willem Johan Kolff, constructed the first working dialyzer in 1943 during the Nazi occupation of the Netherlands.
• He first used glass cannulae to obtain arterial blood from the radial artery, which he returned to the cubital vein.


19661966 till nowtill now… …

• HISTORY• MODALITIES• IMAGING• NOVEL TRENDS• WHERE WE STAND• TAKE HOME
MESSAGE
• A well-functioning vascular access (VA) is a mainstay to perform an efficient hemodialysis (HD) procedure. There are three main types of access:
• Native arteriovenous fistula (AVF)
• Arteriovenous graft (AVG)• Central venous catheter
(CVC).Tunneled & non-Tunneled

• Acute dialysis• Bridge to permenant
access• Superficial venous
insufficiency• Cardiac insufficiency• Surgically unfit patients
• Most common• Durable• More tolerated by
patients • AVG more infection
incidence but rapid use than AVF

CVCCVC• What patients do
prefer ??
• 1% Japan
• 18% in the United States
• 39% Belgium
• 44% Canada
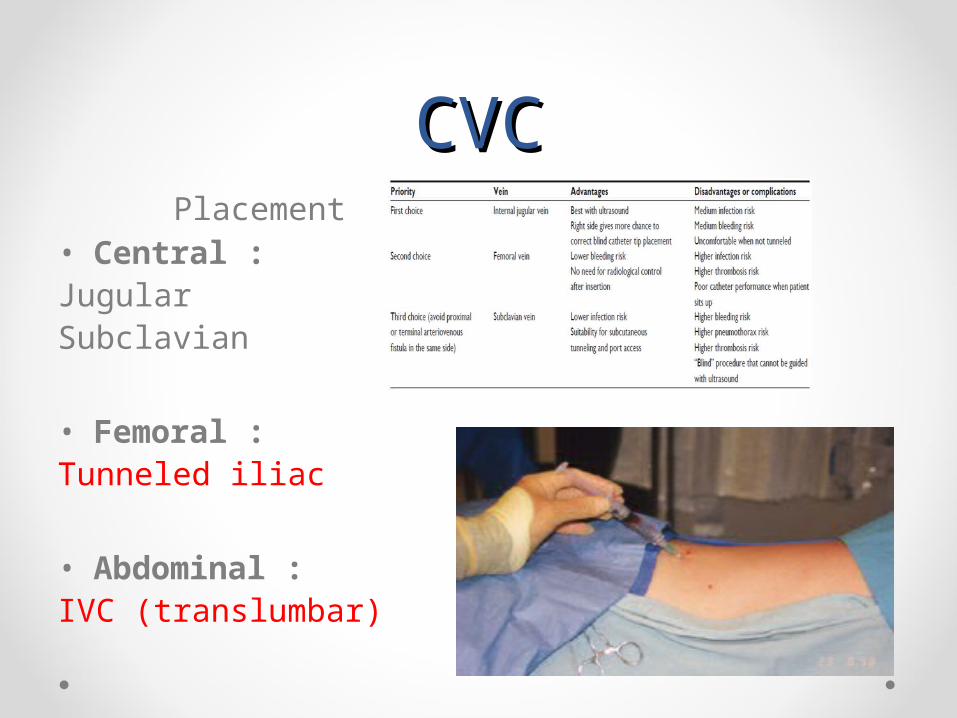
CVCCVCPlacement
• Central :JugularSubclavian
• Femoral : Tunneled iliac
• Abdominal : IVC (translumbar)
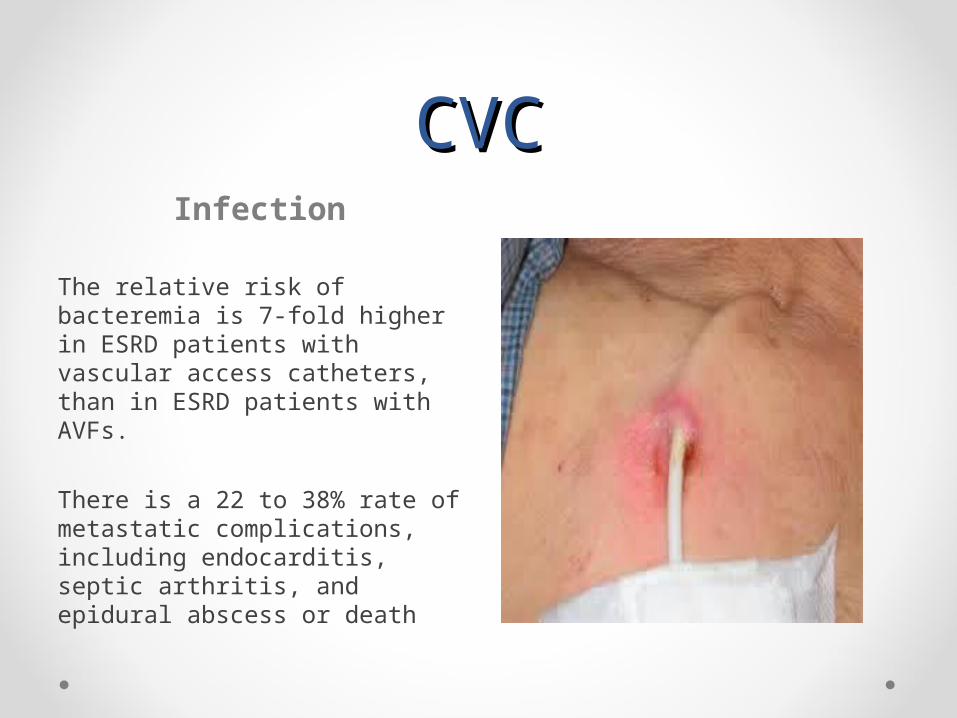
CVCCVCInfection
The relative risk of bacteremia is 7-fold higher in ESRD patients with vascular access catheters, than in ESRD patients with AVFs.
There is a 22 to 38% rate of metastatic complications, including endocarditis, septic arthritis, and epidural abscess or death
CVCCVCInfection
• Tunneled versus non-tunneled catheters
• Silver-sulfadiazine-chlorhexidine coating had a strong bactericidal effect.
• Antibiotic Ointments
• Antibiotic lock solution is a high concentration of antibiotic with or without the addition of an anticoagulant agent, such as tissue plasminogen activator (tPA) or heparin
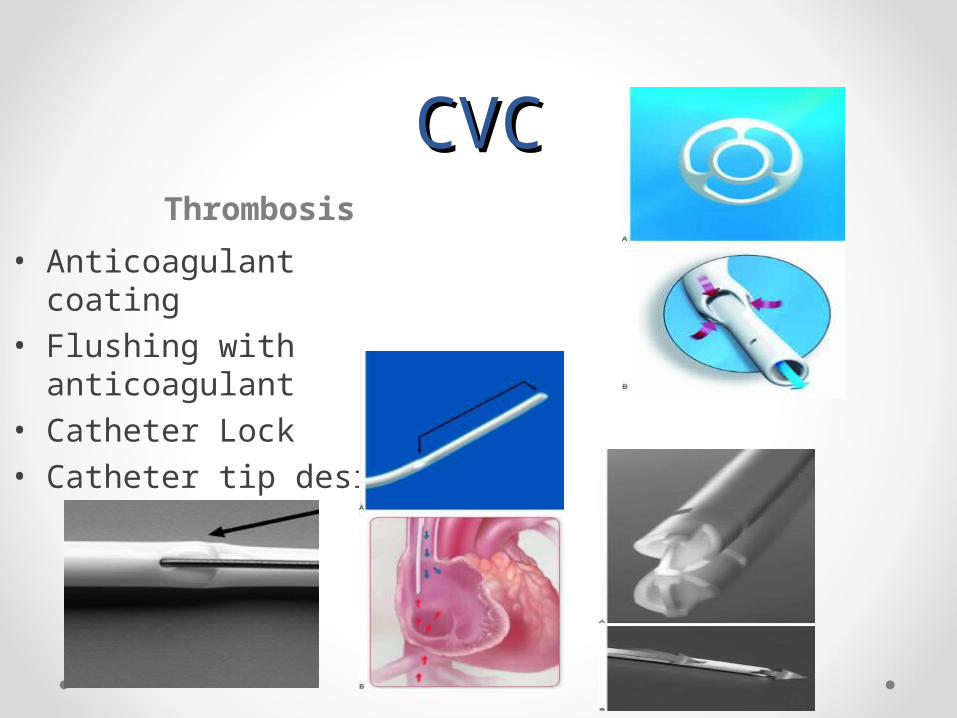
CVCCVCThrombosis
• Anticoagulant coating• Flushing with
anticoagulant • Catheter Lock • Catheter tip design

AVFAVF• The AVF needs to be
planned at least one or two months before starting HD, a time required for the proper maturation of the VA.
• RCAVF• BCAVF• BBAVF

AVFAVF
The most frequent complications related to AVFs are •Insufficient maturation of the AVF•Stenosis•Thrombosis•Infection•aneurysm, pseudoaneurysm•heart failure•steal syndrome” due to ischemia and high-rate flow AVF.

AVGAVG
• Not last as long as AVFs and they have higher rates of infection and thrombosis
• Grafts present a second choice of VA
• They can be placed any where
• Straight, curved or loop configuration
• They may offer a large surface area for cannulation.
AVGAVG
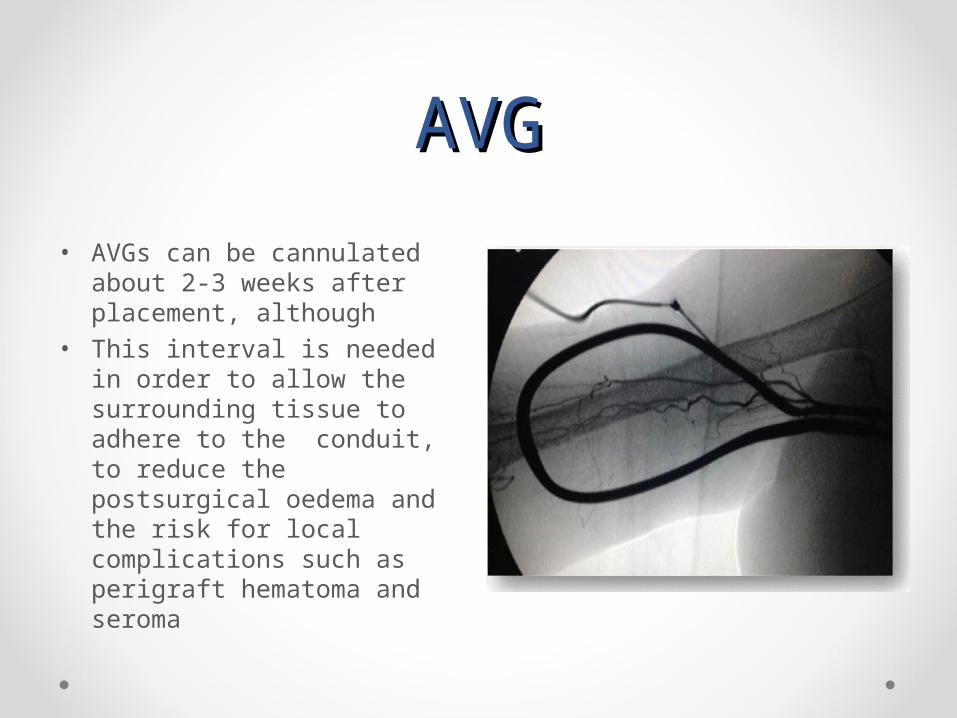
• AVGs can be cannulated about 2-3 weeks after placement, although
• This interval is needed in order to allow the surrounding tissue to adhere to the conduit, to reduce the postsurgical oedema and the risk for local complications such as perigraft hematoma and seroma
• HISTORY• MODALITIES• IMAGING• NOVEL TRENDS• WHERE WE STAND• TAKE HOME
MESSAGE

DopplerDopplerPRE POST
• The gold standard to decide on the type and location of VA is the duplex ultrasound scan.
• Superficial venous system
• Deep venous system
• Arterial system
• RULE OF
6
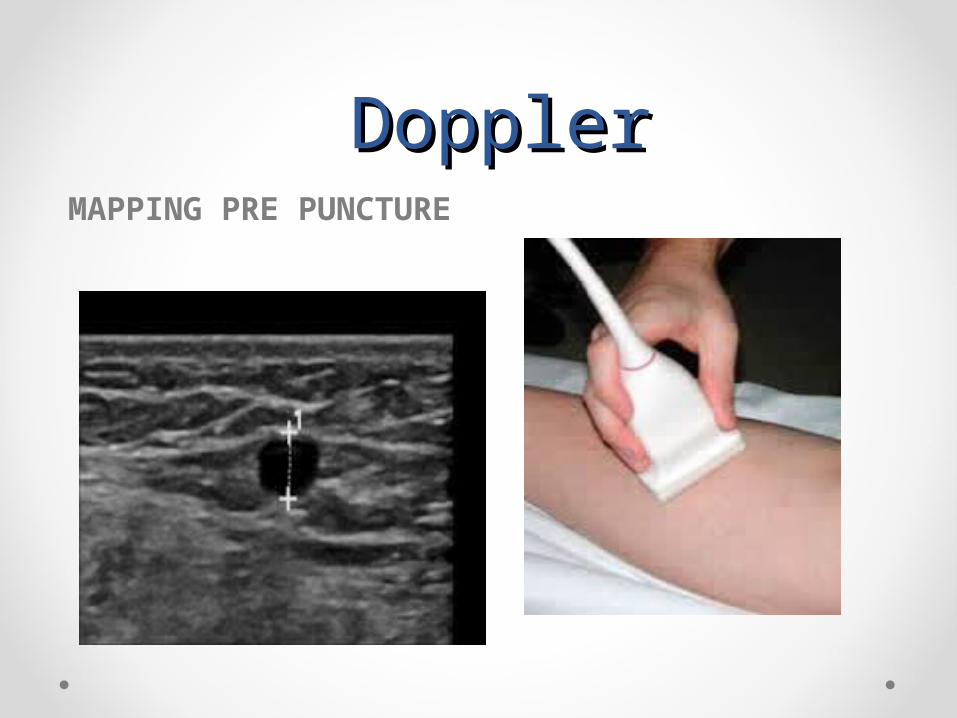
DopplerDoppler MAPPING PRE PUNCTURE
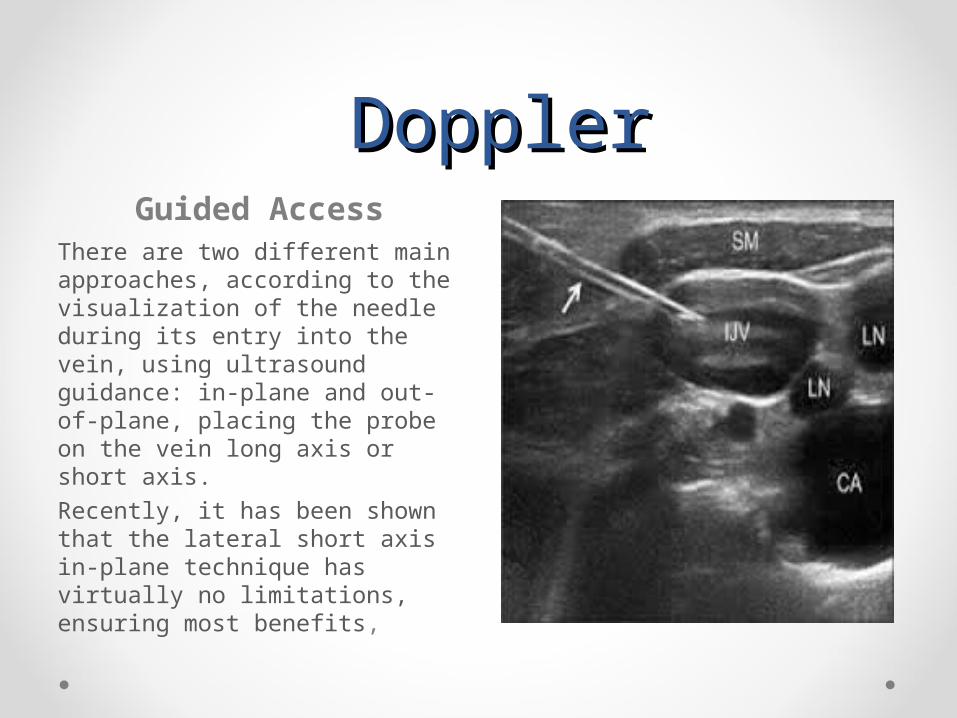
DopplerDoppler Guided Access
There are two different main approaches, according to the visualization of the needle during its entry into the vein, using ultrasound guidance: in-plane and out-of-plane, placing the probe on the vein long axis or short axis. Recently, it has been shown that the lateral short axis in-plane technique has virtually no limitations, ensuring most benefits,

• HISTORY• MODALITIES• IMAGING• NOVEL TRENDS• WHERE WE STAND• TAKE HOME
MESSAGE

This review focuses on therapies to prevent or treat AV access failure that are delivered locally through endovascular approaches or perivascular administration
Oral administration
• A randomized, placebo-controlled trials found some benefits on AV graft (AVG) patency of orally administered agents, dipryridamole plus aspirin
• Another ongoing randomized clinical trial is evaluating short-term use of orally administered sirolimus on the patency of AVGs and AV fistulas (AVFs) after clinically indicated angioplasty (Sirolimus Use in Angioplasty for Vascular Access Extension (SAVE)

Endovascular Approach
• DEB• DES• Heparin bioactive graft• Use of biodegradable
stents• Cryotherapy( NO, -10)• Brachytherapy.(ionizing
radiation)
Perivascular Approach
• Application of biologic or pharmacological agents to the adventitial layer of the blood vessel
• During vascular access creation
and also, long after access surgery through ultrasound -guided subcutaneous injection
• Repeat application of a sirolimus-laden polymer gel through ultrasound-guided injection to the vein–graft anastomosis
• Cell-Based Delivery : seeding endothelial cells to AVGs and AVFs through perivascular administration at the time of access creation
• Thiazolidinediones induce adipose tissue production of adiponectin having vasculoprotective effects, including inhibition of smooth muscle cell proliferation and inflammation.


• Bioengineering approaches have been used to create autologous grafts from dermal fibroblasts and endothelial cells obtained through tissue biopsy and expanded in tissue culture


NEEDLE less DIALYSISNEEDLE less DIALYSIS

• HISTORY• MODALITIES• IMAGING• NOVEL TRENDS• WHERE WE STAND• TAKE HOME
MESSAGE

Failed vascular accessFailed vascular access
highlighthighlight • Training for central
access• Image guided • Nurses handling
(puncture, circuit)• Infection control • Lack of follow up• Patient factors
(reluctance)• Vascular surgeons
(priority)• Tx waiting list
• TAKE HOME MESSAGE
• VASCULAR ACCESS IS A PRECIOUS ONE AND NEEDS MORE CAREFUL HANDLING
• FAILED VASCULAR ACCESS IS A NIGHTMARE
















![Unusual Complication of Hemodialysis Cuffed Catheter Tunnel ... · 2019. 7. 30. · hemodialysis patients with vascular access central venous catheter [2, 5]. Infection is the second](https://img.dokumen.tips/doc/110x75/6112f543c4e8093a88485054/unusual-complication-of-hemodialysis-cuffed-catheter-tunnel-2019-7-30-hemodialysis.jpg)











