Embed Size (px)
Citation preview
New approaches in New approaches in Ventilator Associated Ventilator Associated
Pneumonia (VAP) managementPneumonia (VAP) management
By:By:Sameh ElhabashySameh Elhabashy
Mohamed SharqaweMohamed SharqaweAhmed HabibAhmed Habib
Critical Care and Emergency Nursing DepartmentCritical Care and Emergency Nursing Department
Faculty of Nursing – Cairo University Faculty of Nursing – Cairo University
OutlinesOutlines Introduction.Introduction. Classification of Pneumonia.Classification of Pneumonia. Illustration of (VAP).Illustration of (VAP). Epidemiology and Risk factors.Epidemiology and Risk factors. Types of (VAP).Types of (VAP). Causative Pathogenesis.Causative Pathogenesis. New approaches in diagnosis.New approaches in diagnosis. Protocols of treatment. Protocols of treatment. Prevention Strategies and (VAP bundle).Prevention Strategies and (VAP bundle). Conclusion.Conclusion.
aa
IntroductionIntroduction
VAP occurs frequently and is associated VAP occurs frequently and is associated with significant morbidity in critically ill with significant morbidity in critically ill patients.There is no enough evidence to patients.There is no enough evidence to indicate that VAP is preventable and that indicate that VAP is preventable and that hospitals can decrease VAP rates hospitals can decrease VAP rates kalanuria kalanuria etal,(2014)etal,(2014)
VAP is associated with increased lengths of VAP is associated with increased lengths of ICU and hospital stay, increased mortality ICU and hospital stay, increased mortality rates, and increased costs rates, and increased costs kalarunia et kalarunia et al(2014).al(2014).
Analysis of Analysis of LOSLOS reports demonstrated that reports demonstrated that VAP was associated with a mean increase in VAP was associated with a mean increase in ICU length-of-stay of 6.1 days ICU length-of-stay of 6.1 days
Approximately (50 %) of all antibiotics Approximately (50 %) of all antibiotics
administered in ICUs are for treatment of administered in ICUs are for treatment of
(VAP ).(VAP ).
PneumoniaPneumonia
Pneumonia is an inflammation of the lung Pneumonia is an inflammation of the lung parenchyma that is caused by a microbial parenchyma that is caused by a microbial agent agent
It accounts for approximately (It accounts for approximately (11% to 15%)11% to 15%)of of all hospital-associated infections (HAIs) and all hospital-associated infections (HAIs) and up to (up to (27%) 27%) of all infections acquired in the of all infections acquired in the medical intensive care unit (MICU) and medical intensive care unit (MICU) and coronary care unit (CCU), respectivelycoronary care unit (CCU), respectively
Classification of PneumoniaClassification of Pneumonia
CAPCAP as pneumonia for which the first positive as pneumonia for which the first positive
bacterial culture is obtained within 48 hours of bacterial culture is obtained within 48 hours of admission to the hospital and the patient does not admission to the hospital and the patient does not have risk factors for HAPhave risk factors for HAP
HCAPHCAP
occurs when the patient’s first positive bacterial occurs when the patient’s first positive bacterial culture is obtained within 48 hours of admission culture is obtained within 48 hours of admission and the patient has any of the following risk factors and the patient has any of the following risk factors as chemotherapy, wound care, previous as chemotherapy, wound care, previous admission,...etcadmission,...etc
HAPHAP
in which the patient’s first positive bacterial in which the patient’s first positive bacterial culture is obtained more than 48 hours after culture is obtained more than 48 hours after admission to the hospitaladmission to the hospital
Illustration of (VAP)Illustration of (VAP)
VAP is a sub-classification of HAP.VAP is a sub-classification of HAP.
VAP is pneumonia that develops in a VAP is pneumonia that develops in a
mechanically ventilated patient with a first mechanically ventilated patient with a first
positive bacterial culture beyond 48 hours positive bacterial culture beyond 48 hours
after hospital admission or tracheal after hospital admission or tracheal
intubation, whichever occurred first.intubation, whichever occurred first.
None Modifiable Risk factors for VAPNone Modifiable Risk factors for VAP Male gender.Male gender.
Severity of illness: high APACHE II scores Severity of illness: high APACHE II scores
(>16) correlate with risk of (VAP).(>16) correlate with risk of (VAP).
Preexisting pulmonary disease as (ARDS).Preexisting pulmonary disease as (ARDS).
Trauma, Coma.Trauma, Coma.
Multi-system organ failure.Multi-system organ failure.
Treatment related risk factors as neurosurgical Treatment related risk factors as neurosurgical
proceduresprocedures
Modifiable Risk FactorsModifiable Risk Factors
Duration of ventilation.Duration of ventilation.
3% per day in first week.3% per day in first week.
2% per day in second.2% per day in second.
1% per day after.1% per day after.
Nasotracheal intubation. Nasotracheal intubation.
Recurrent re-intubation.Recurrent re-intubation.
Modifiable Risk Factors (Cont.)Modifiable Risk Factors (Cont.)
Supine position.Supine position.
Enteral feeding.Enteral feeding.
Oropharyngeal colonization.Oropharyngeal colonization.
Stress ulcer prophylaxis.Stress ulcer prophylaxis.
Prior antibiotic therapy.Prior antibiotic therapy.
Types of (VAP)Types of (VAP)
1- Early-onset VAP1- Early-onset VAPoccurs during the first occurs during the first 4 days 4 days of the patient’s of the patient’s admission. admission.
caused by antibiotic sensitive microorganisms caused by antibiotic sensitive microorganisms as MSSA, as MSSA, Streptococcus pneumoniaStreptococcus pneumonia, , Haemophilus Haemophilus influenzainfluenza ……etc ……etc
Types of (VAP) cont.Types of (VAP) cont.
2- late-onset VAP 2- late-onset VAP occurs beyond 4 days after admissionoccurs beyond 4 days after admissioncaused by caused by MDRMDR ( (Pseudomonasaeruginosa, Pseudomonasaeruginosa, Acinetobacter Acinetobacter or or Enterobacter Enterobacter methicillin-resistant methicillin-resistant Staphylococcus aureus Staphylococcus aureus ((MRSAMRSA),….etc),….etc
Prevelance of causative agentsPrevelance of causative agents Staphylococcus aureus Staphylococcus aureus (24.4%)(24.4%) Pseudomonas aeruginosa Pseudomonas aeruginosa (16.3%)(16.3%) Enterobacter Enterobacter spp. (8.4%)spp. (8.4%) Acinetobacter baumannii Acinetobacter baumannii (8.4%)(8.4%) Klebsiella pneumonia Klebsiella pneumonia (7.5%)(7.5%) Escherichia coli Escherichia coli (4.6%)(4.6%) Candida Candida spp. (2.7%)spp. (2.7%) Klebsiella oxytoca Klebsiella oxytoca (2.2%)(2.2%) Coagulase-negative Coagulase-negative Staphylococcus Staphylococcus (1.3%)(1.3%)
EpidemiologyEpidemiology
For the year 2012, NHSN facilities reported For the year 2012, NHSN facilities reported
more than 3,957 VAPs and the incidence for more than 3,957 VAPs and the incidence for
various types of hospital units ranged from 0.0-various types of hospital units ranged from 0.0-
4.4 per 1,000 ventilator days 4.4 per 1,000 ventilator days Dudeck ,(2012)Dudeck ,(2012)
EpidemiologyEpidemiology VAP is the second most common nosocomial VAP is the second most common nosocomial
infection in ICUinfection in ICU VAP accounts for approximately one half of VAP accounts for approximately one half of
all hospital acquired pneumoniaall hospital acquired pneumonia VAP is (VAP is (3 to 10)3 to 10) fold greater than pneumonia fold greater than pneumonia
in nonventilated patients.in nonventilated patients. VAP occurs in (VAP occurs in (9% to 27%)9% to 27%)of mechanically of mechanically
ventilated patients .ventilated patients .
Epidemiology (Cont.)Epidemiology (Cont.)
3% within the first 5 days of ventilation3% within the first 5 days of ventilation 2% between days 5 to 10 of ventilation2% between days 5 to 10 of ventilation 1% thereafter1% thereafter
In the healthy individual, the lower respiratory tract In the healthy individual, the lower respiratory tract is a sterile body site.is a sterile body site.
The body possesses several defense mechanisms to The body possesses several defense mechanisms to prevent contamination of the lungs.prevent contamination of the lungs.
Disease processes, treatment modalities and Disease processes, treatment modalities and personal habits or practices (i.e., cigarette smoke, personal habits or practices (i.e., cigarette smoke, alcohol intake) can impair the body’s natural alcohol intake) can impair the body’s natural defense mechanisms, predisposing the individual to defense mechanisms, predisposing the individual to lower respiratory infection.lower respiratory infection.
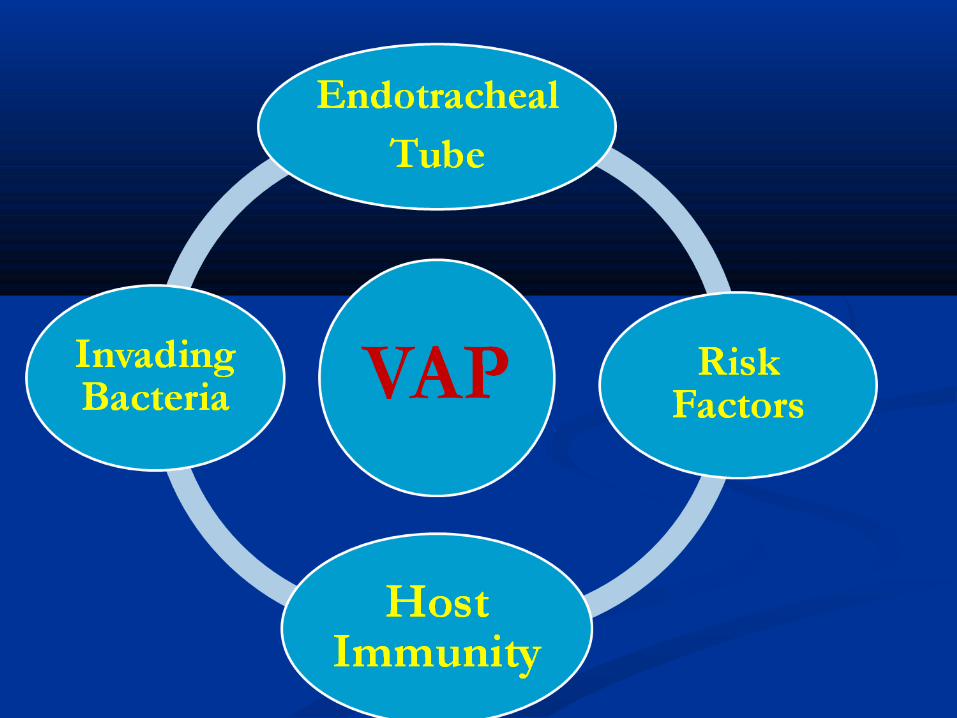
the endotracheal tube, presence of risk factors, the endotracheal tube, presence of risk factors, virulence of the invading bacteria and host virulence of the invading bacteria and host immunity largely determine the development of immunity largely determine the development of VAPVAP
Infectious bacteria obtain direct access to the lower Infectious bacteria obtain direct access to the lower respiratory tract viarespiratory tract via
MicroaspirationMicroaspiration
Development of a biofilmDevelopment of a biofilm
pooling of secretions around the cuffpooling of secretions around the cuff
impairment of mucociliary clearanceimpairment of mucociliary clearance
it has recently been noted that critically ill it has recently been noted that critically ill patients may have impaired phagocytosis and patients may have impaired phagocytosis and behave as functionally immunosuppressed.behave as functionally immunosuppressed.
Mechanical ventilation is the primary risk factorMechanical ventilation is the primary risk factor Colonization of the oropharynx and dental Colonization of the oropharynx and dental
surfaces act as a reservoir of bacteriasurfaces act as a reservoir of bacteria
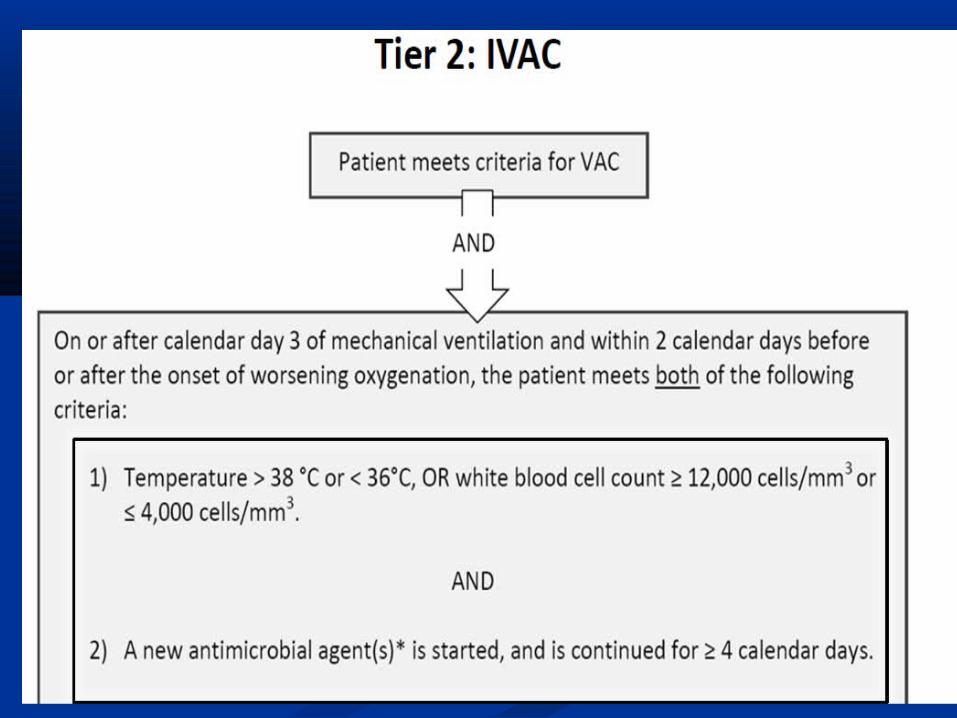
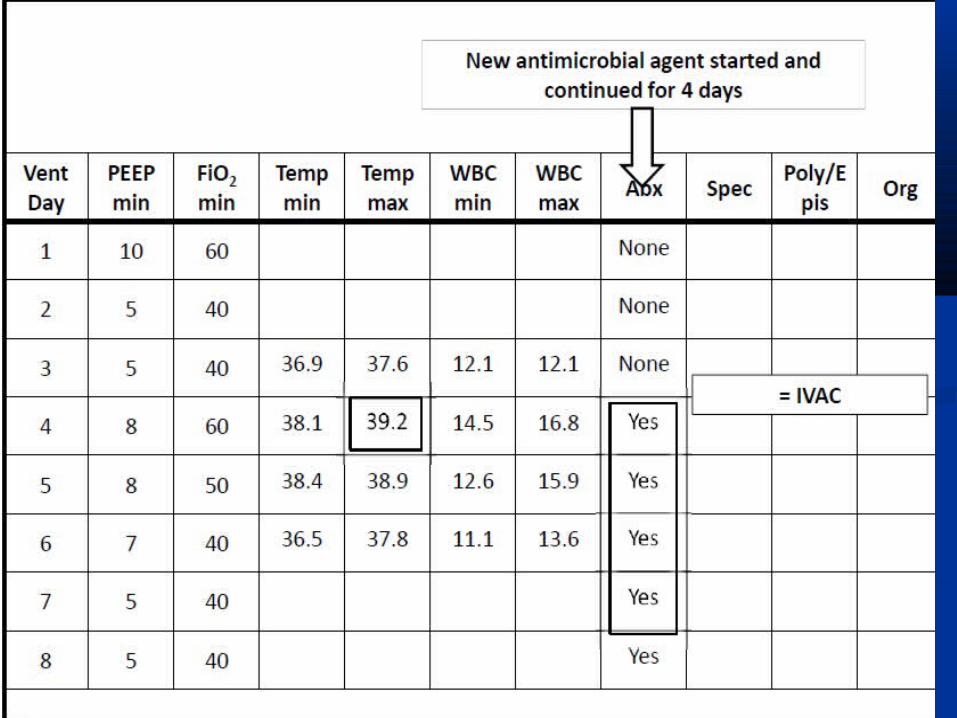
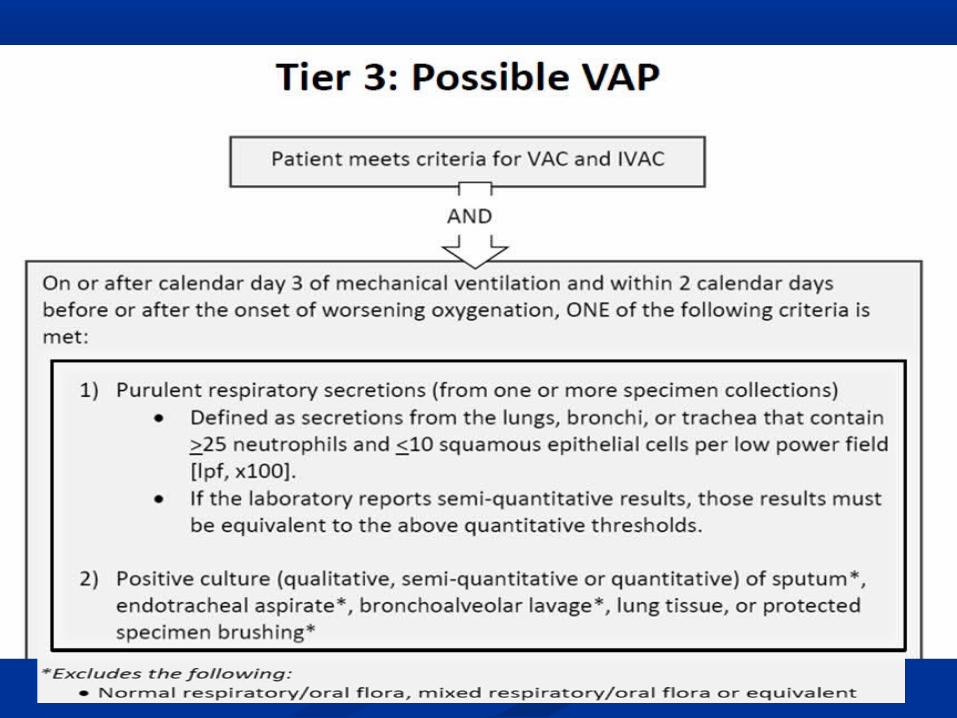
Ventilator-associated events Ventilator-associated events (VAEs) as a new approach for (VAEs) as a new approach for
diagnosis of (VAP)diagnosis of (VAP)
Why “Ventilator Associated Events” (VAE)? ‐Why “Ventilator Associated Events” (VAE)? ‐BACKGROUND AND RATIONALEBACKGROUND AND RATIONALE
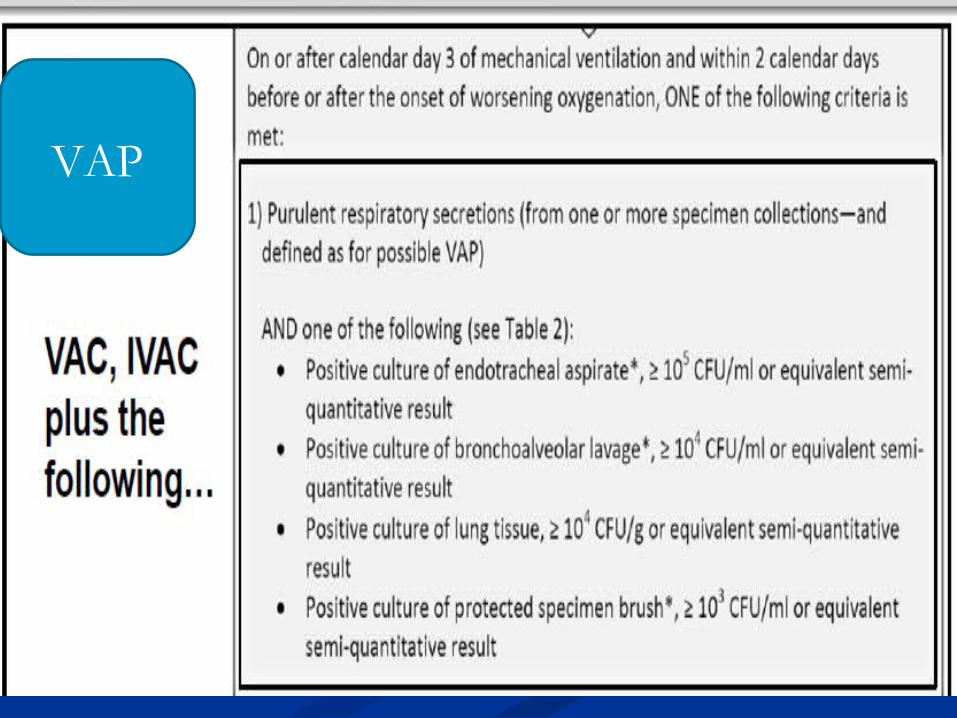
Operational definition of ventilator Operational definition of ventilator associated pneumonia(VAP).associated pneumonia(VAP).
In 2002, The In 2002, The National Healthcare Safety Network (NHSN)National Healthcare Safety Network (NHSN) and Centers for and Centers for
Disease Control and Prevention (CDC) defined ventilator-associated Disease Control and Prevention (CDC) defined ventilator-associated
pneumonia (VAP), as a new or progressive and persistent radiographic pneumonia (VAP), as a new or progressive and persistent radiographic
abnormality developing in a patient on mechanical ventilation (within 48 hours abnormality developing in a patient on mechanical ventilation (within 48 hours
of mechanical ventilation).of mechanical ventilation).
Radiographic abnormality. (required)Radiographic abnormality. (required)
One or more systemic signs or e.g. (fever, or altered mental status. in addition One or more systemic signs or e.g. (fever, or altered mental status. in addition
to selected pulmonary criteria (e.g. respiratory secretions, new onset of cough, to selected pulmonary criteria (e.g. respiratory secretions, new onset of cough,
rales, bronchial breath sounds, or worsening oxygenation). (required)rales, bronchial breath sounds, or worsening oxygenation). (required)
laboratory evidence of infection and for in immunocompromised patients e.g laboratory evidence of infection and for in immunocompromised patients e.g
leukocytosis . (optional).leukocytosis . (optional).
The problemThe problem This definition has since been found to be This definition has since been found to be neither sensitive neither sensitive
nor specific nor specific for VAP therefore, cannot be accurately used for VAP therefore, cannot be accurately used
for surveillance purposes. For example, a chest radiograph for surveillance purposes. For example, a chest radiograph
may demonstrate a haziness that could be pneumonia, may demonstrate a haziness that could be pneumonia,
atelectasis, or pleural effusion and that become especially atelectasis, or pleural effusion and that become especially
difficult to characterize on a portable film.difficult to characterize on a portable film.
The authors determined that the most accurate radiographic The authors determined that the most accurate radiographic
sign for pneumonia was an sign for pneumonia was an air bronchogramair bronchogram, which had a , which had a
diagnostic accuracy of 64%. (The study by Wunderink, et al.)diagnostic accuracy of 64%. (The study by Wunderink, et al.)
Due to these realizations The CDC is to be Due to these realizations The CDC is to be commended for being inclusive and bringing commended for being inclusive and bringing together a large number of organizations and together a large number of organizations and expertise to develop this a new term, ventilator-expertise to develop this a new term, ventilator-associated event (VAE), (starting in 2012 –associated event (VAE), (starting in 2012 –2013).2013).
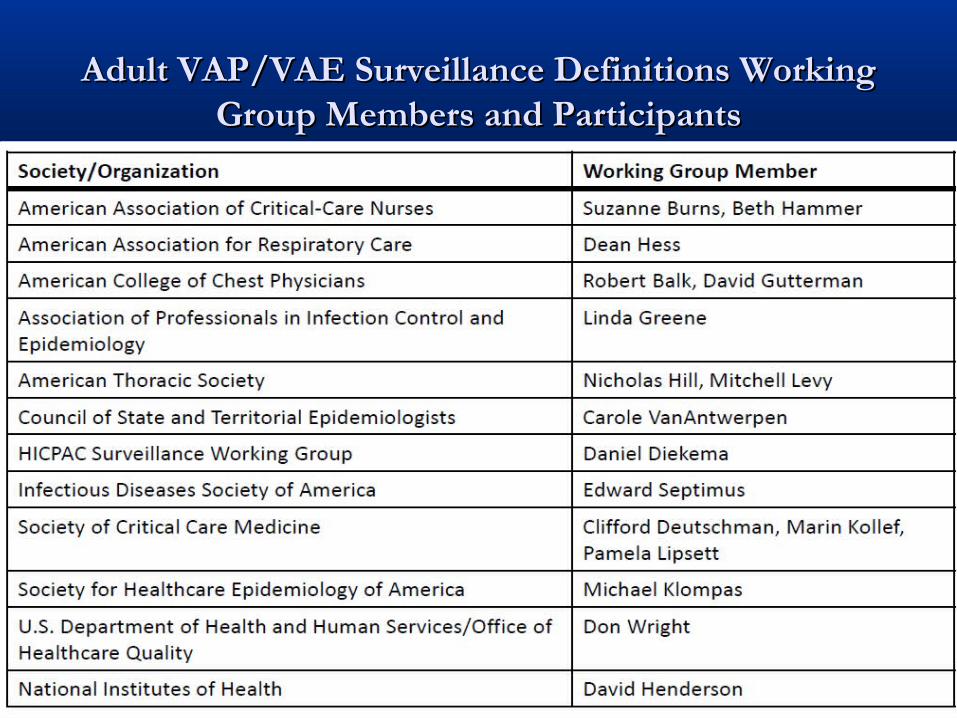
Adult VAP/VAE Surveillance Definitions WorkingAdult VAP/VAE Surveillance Definitions WorkingGroup Members and ParticipantsGroup Members and Participants
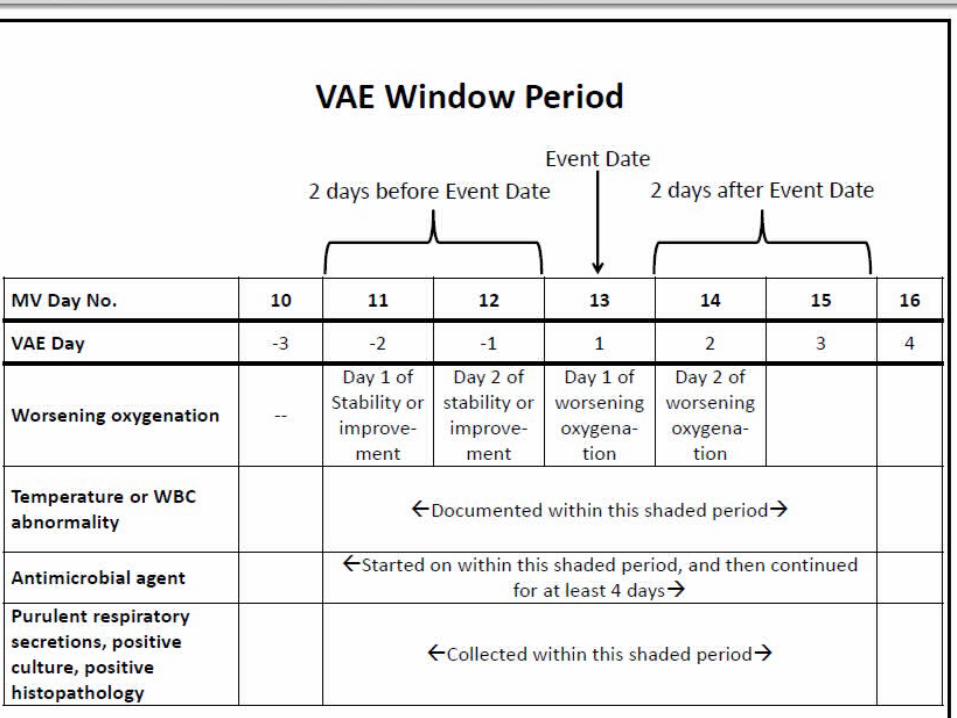
What is (VAE)?What is (VAE)?
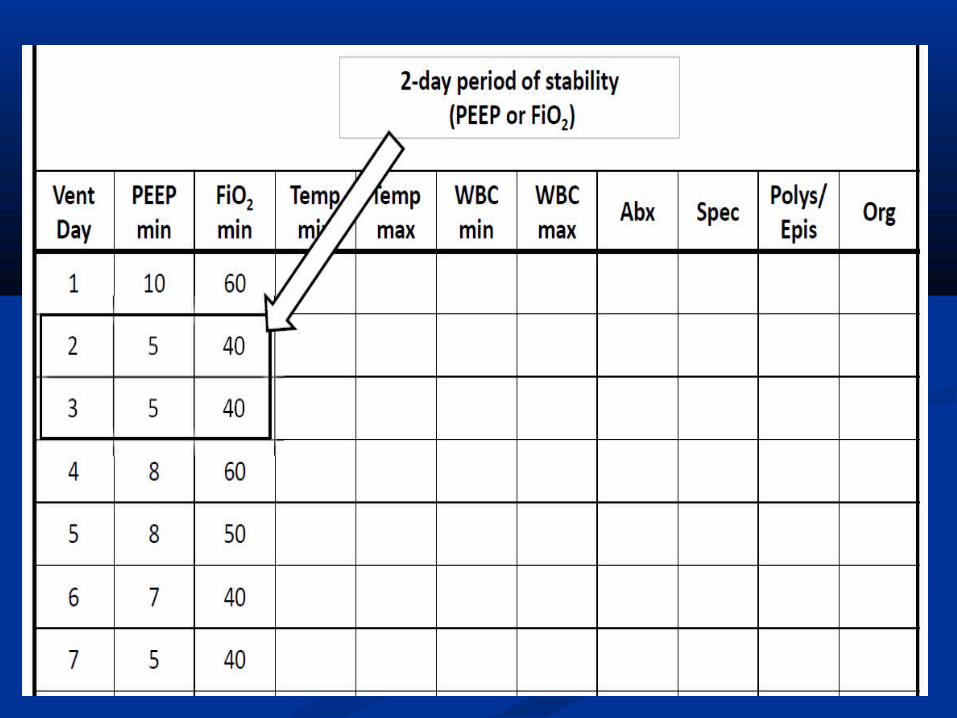
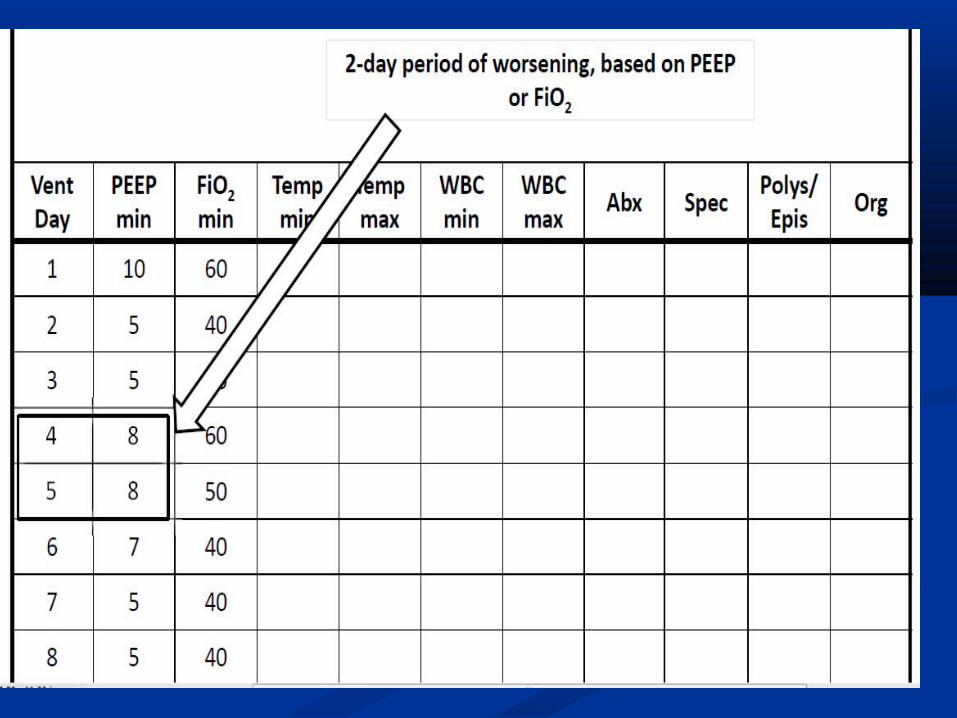
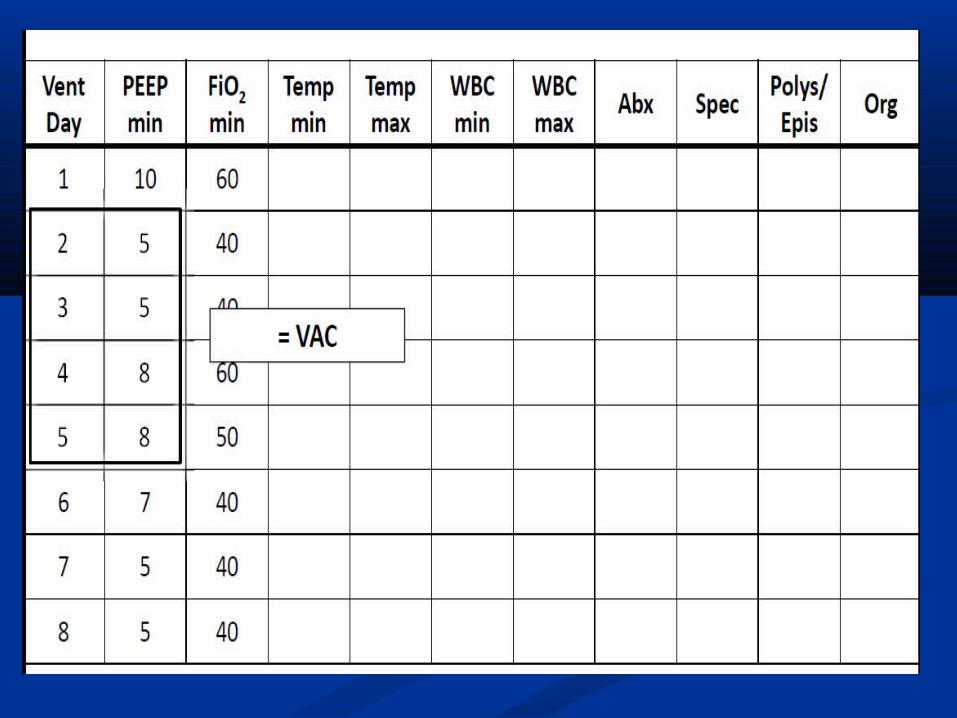
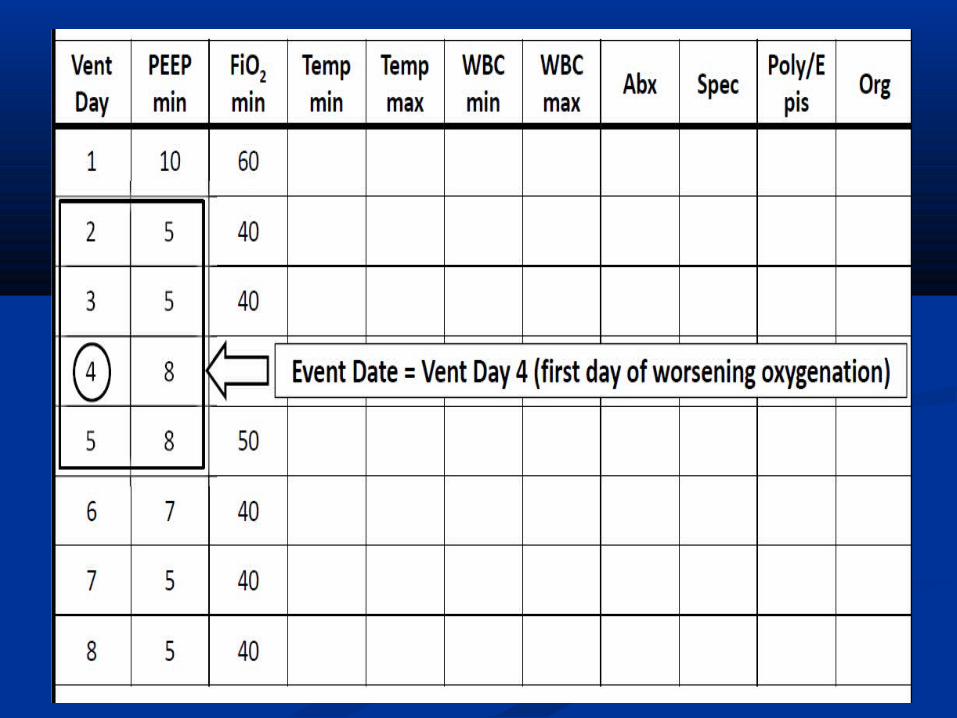
Ventilator-associated event (VAE), groups all the Ventilator-associated event (VAE), groups all the conditions that result in a significant and sustained conditions that result in a significant and sustained deterioration in oxygenation, defined as a greater than deterioration in oxygenation, defined as a greater than 20% increase in the daily minimum fraction of 20% increase in the daily minimum fraction of inspired oxygen (fioinspired oxygen (fio22)or an increase of at least 3 cm )or an increase of at least 3 cm H2O in the daily minimum positive end-expiratory H2O in the daily minimum positive end-expiratory pressure (PEEP) to maintain oxygenation.pressure (PEEP) to maintain oxygenation.
54% of ventilated patients in USA suffering from 54% of ventilated patients in USA suffering from (VAE).(VAE).
Systemic Response to InflammationSystemic Response to Inflammation The inflammatory response is often confined to the site, The inflammatory response is often confined to the site,
causing only local signs and symptoms. However, systemic causing only local signs and symptoms. However, systemic responses can also occur. Fever is the most common sign of a responses can also occur. Fever is the most common sign of a systemic response to injury, and it is most likely caused by systemic response to injury, and it is most likely caused by endogenous pyrogens (internal substances that cause fever) endogenous pyrogens (internal substances that cause fever) released from neutrophils and macrophages (specialized forms released from neutrophils and macrophages (specialized forms of leukocytes). These substances reset the hypothalamic of leukocytes). These substances reset the hypothalamic thermostat, which controls body temperature, and produce thermostat, which controls body temperature, and produce fever. fever.
Normal range of neutrophils (1.0 – 8.0 k/ul )Normal range of neutrophils (1.0 – 8.0 k/ul )
VAP
Nursing implicationNursing implication
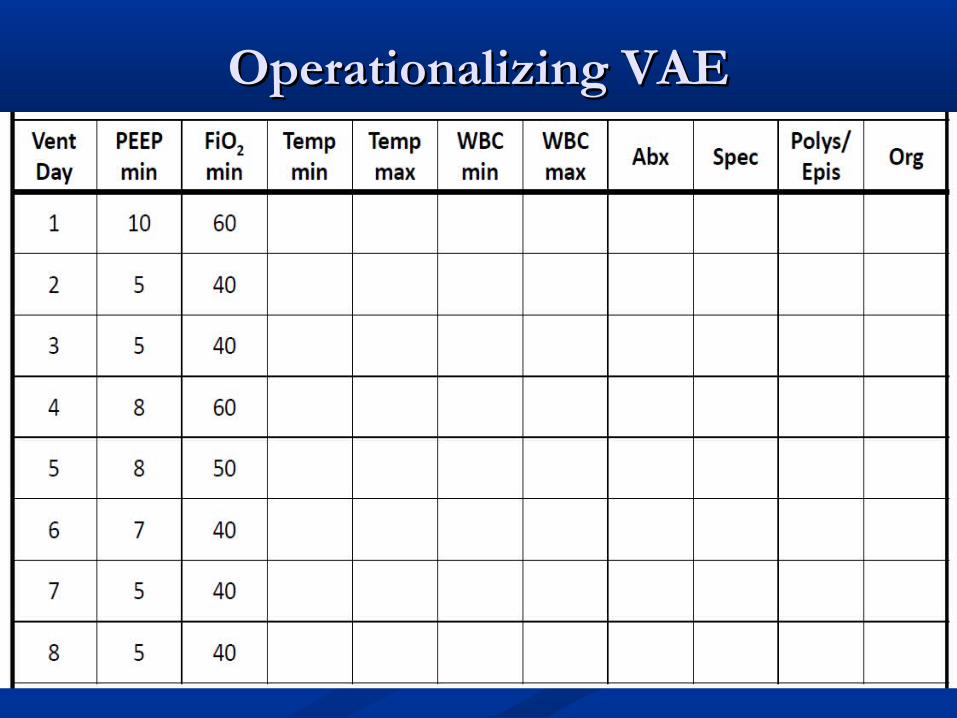
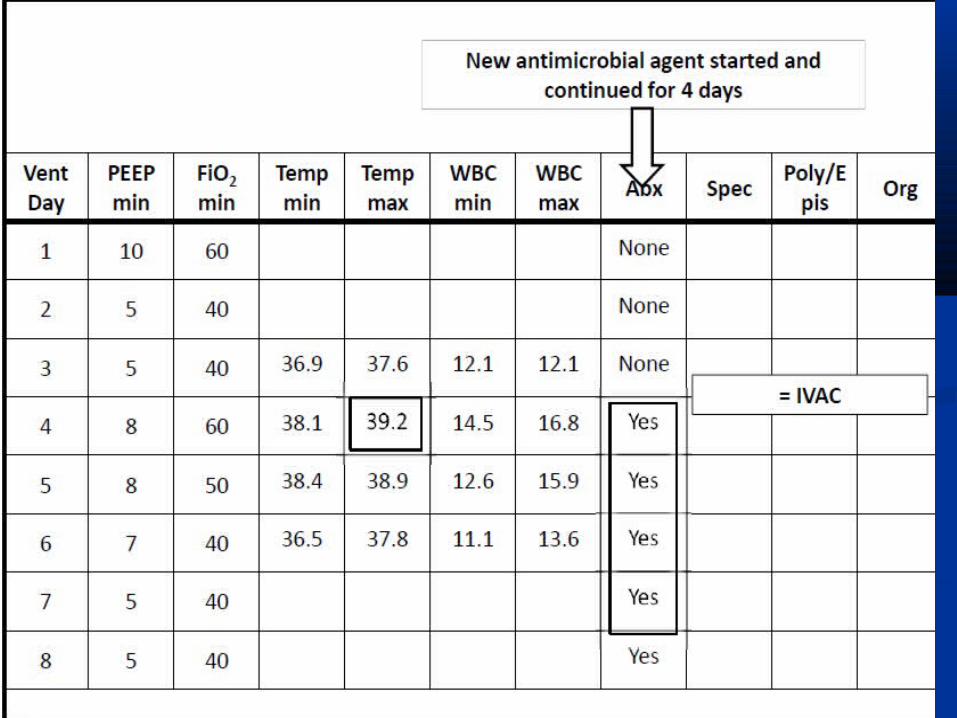
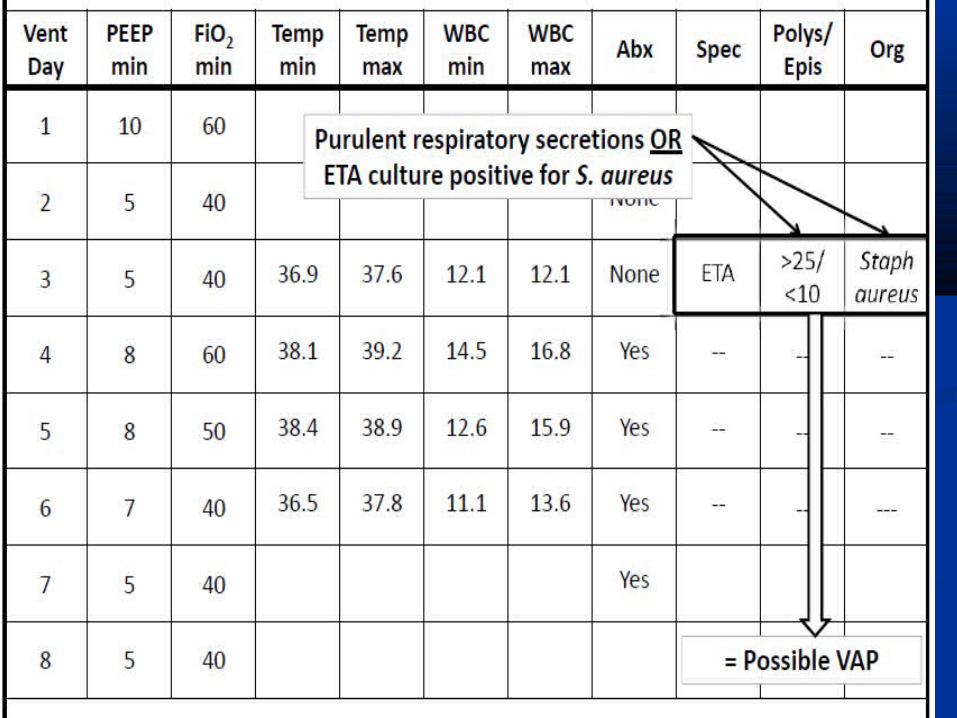
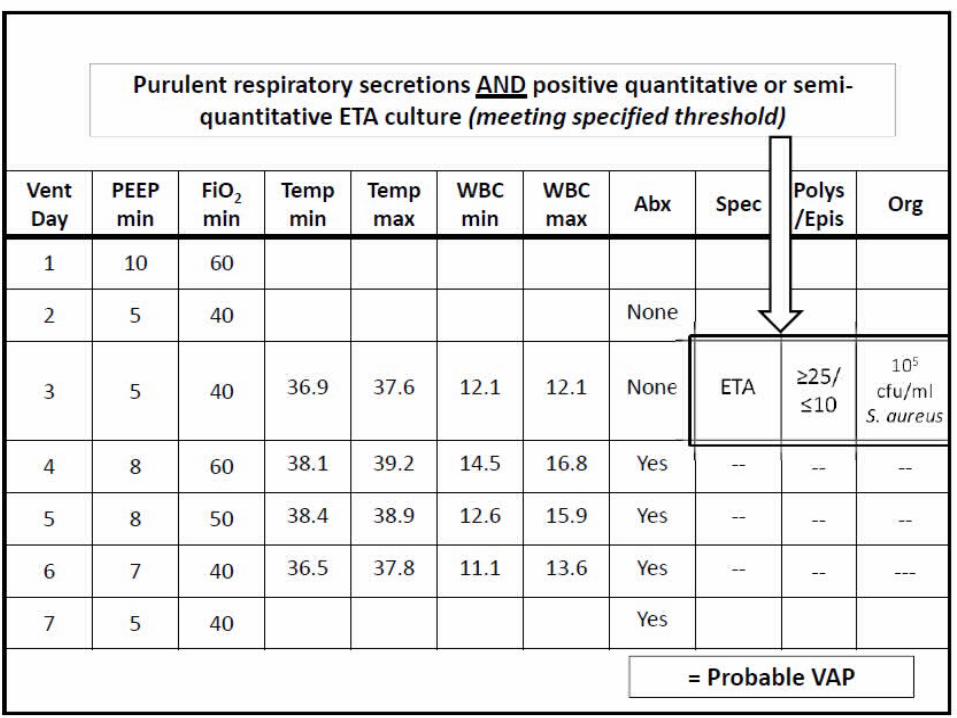
Operationalizing VAEOperationalizing VAE
VAP Prevention and VAP Prevention and treatment treatment
Bundle and clinical pathway Bundle and clinical pathway approachesapproaches
Care BundleCare Bundle
A A care bundlecare bundle is …... is …... “ “A systematic method of A systematic method of
measuring and improving measuring and improving clinical care processes based clinical care processes based on groups of care elements on groups of care elements for particular diagnoses and for particular diagnoses and procedures”procedures”
NHS Modernization AgencyNHS Modernization Agency
Prevention : (Ventilator Bundle)Prevention : (Ventilator Bundle)
The IHI (Institute of Health The IHI (Institute of Health care Improvement) care Improvement) Ventilator Bundle is a series Ventilator Bundle is a series of interventions related to of interventions related to ventilator care that, when ventilator care that, when implemented together, will implemented together, will achieve significantly better achieve significantly better outcomes than when outcomes than when implemented individually. implemented individually.
Ventilator BundleVentilator Bundle The key components of the IHI The key components of the IHI
Ventilator Bundle are:Ventilator Bundle are: Elevation of the Head of the BedElevation of the Head of the Bed Daily "Sedation Vacations" and Daily "Sedation Vacations" and
Assessment of Readiness to ExtubateAssessment of Readiness to Extubate Peptic Ulcer Disease ProphylaxisPeptic Ulcer Disease Prophylaxis Deep Venous Thrombosis Deep Venous Thrombosis
ProphylaxisProphylaxis Daily Oral Care with ChlorhexidineDaily Oral Care with Chlorhexidine Subglottic suctioning.Subglottic suctioning.
Head Of the Bed 35 -45 degreeHead Of the Bed 35 -45 degree If semi-recumbent or supine (34% )If semi-recumbent or supine (34% )
incidence (VAP).incidence (VAP). If semi-recumbent position (8%) If semi-recumbent position (8%)
incidence (VAP).incidence (VAP). ↑↑HOB → ↓risk of aspiration of HOB → ↓risk of aspiration of
gastrointestinal contentsgastrointestinal contents ↓ ↓risk of aspiration of oropharyngeal risk of aspiration of oropharyngeal
secretions secretions ↓↓risk of aspiration of nasopharyngeal risk of aspiration of nasopharyngeal
secretionssecretions
CDC Guideline for Prevention of Healthcare Associated Pneumonias 2004 ATS / IDSA Guidelines for VAP 2005
Head Of the Bed 35 -45 degreeHead Of the Bed 35 -45 degree
↑↑HOB improves patients’ ventilationHOB improves patients’ ventilation
Supine patients have lower Supine patients have lower spontaneous tidal volumes on PS than spontaneous tidal volumes on PS than those seated in upright position ↑HOB those seated in upright position ↑HOB may aid ventilatory efforts and may aid ventilatory efforts and minimize atelectasis.minimize atelectasis.
Head Of the Bed 35 -45 degreeHead Of the Bed 35 -45 degree
Drakulovic et al. (2ooo)Drakulovic et al. (2ooo), conducted a , conducted a randomized controlled trial in 86 randomized controlled trial in 86 mechanically ventilated patients assigned mechanically ventilated patients assigned to semi-recumbent or supine body to semi-recumbent or supine body position. The trial demonstrated that position. The trial demonstrated that suspected cases of ventilator-associated suspected cases of ventilator-associated pneumonia had an incidence of 34 percent pneumonia had an incidence of 34 percent while in the semi-recumbent position while in the semi-recumbent position suspected cases had an incidence of 8 suspected cases had an incidence of 8 percent (p=0.003). Similarly, confirmed cases percent (p=0.003). Similarly, confirmed cases were 23 percent and 5 percent respectively were 23 percent and 5 percent respectively (p=0.018).(p=0.018).
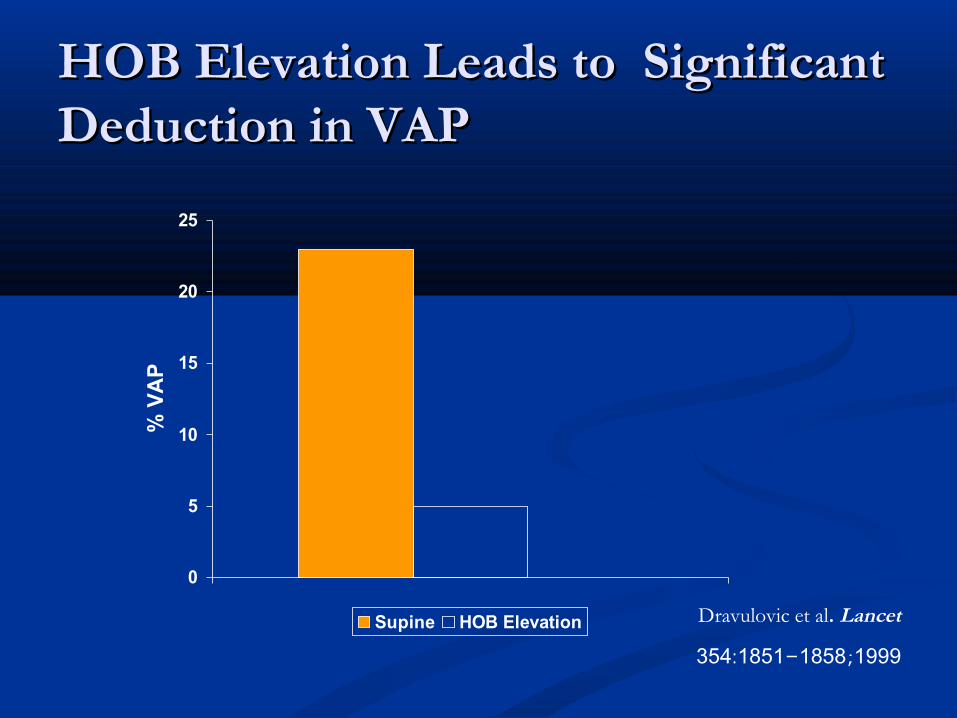
HOB Elevation Leads to Significant HOB Elevation Leads to Significant Deduction in VAPDeduction in VAP
0
5
10
15
20
25
% V
AP
Supine HOB Elevation Dravulovic et al. Lancet
1999;: -354 1851 1858
Daily Oral Care with Daily Oral Care with ChlorhexideneChlorhexidene
Dental plaque can be a Dental plaque can be a significant reservoir for significant reservoir for potential respiratory potential respiratory pathogens that cause pathogens that cause ventilator-associated ventilator-associated pneumonia (VAP). pneumonia (VAP). Chlorhexidene antiseptic has Chlorhexidene antiseptic has long been approved as an long been approved as an inhibitor of dental plaque inhibitor of dental plaque formation and gingivitis. formation and gingivitis.
Daily Oral Care with Daily Oral Care with ChlorhexidineChlorhexidine
Mouth care twice daily with 0.12% Mouth care twice daily with 0.12% chlorhexidene is significantly effective in chlorhexidene is significantly effective in prevention of VAP among mechanically prevention of VAP among mechanically ventilated patients.ventilated patients.
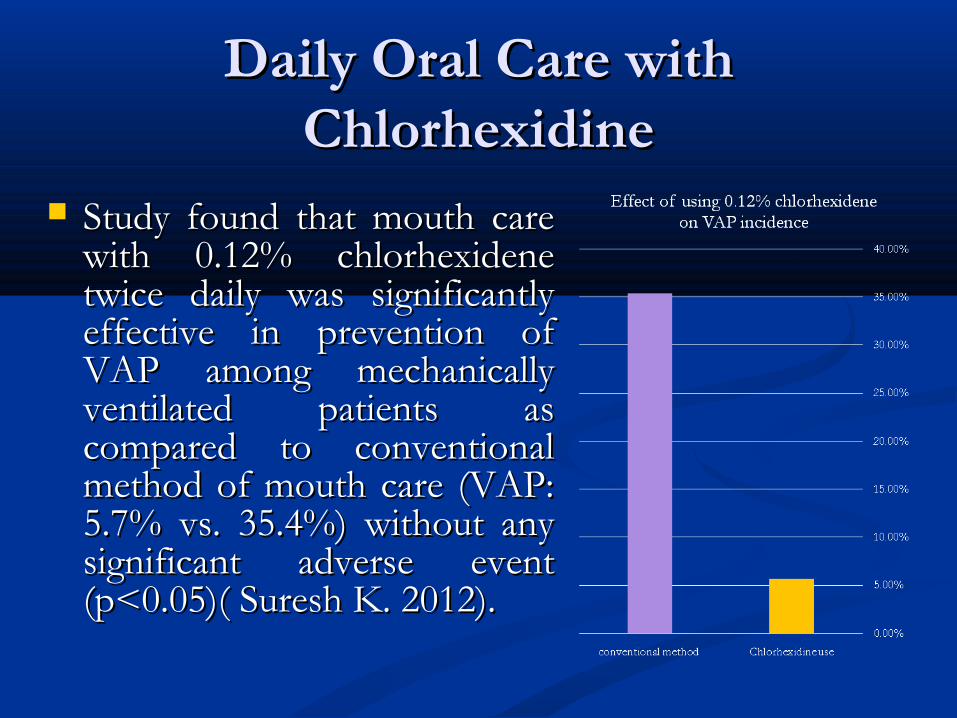
Daily Oral Care with Daily Oral Care with ChlorhexidineChlorhexidine
Study found that mouth care Study found that mouth care with 0.12% chlorhexidene with 0.12% chlorhexidene twice daily was significantly twice daily was significantly effective in prevention of effective in prevention of VAP among mechanically VAP among mechanically ventilated patients as ventilated patients as compared to conventional compared to conventional method of mouth care (VAP: method of mouth care (VAP: 5.7% vs. 35.4%) without any 5.7% vs. 35.4%) without any significant adverse event significant adverse event (p<0.05)( Suresh K. 2012).(p<0.05)( Suresh K. 2012).
Peptic Ulcer Disease (PUD) Peptic Ulcer Disease (PUD) ProphylaxisProphylaxis
It is an appropriate intervention It is an appropriate intervention in all sedentary patients.in all sedentary patients.
Critically ill intubated patients Critically ill intubated patients lack the ability to defend their lack the ability to defend their airway.airway.
Decreasing pH of gastric Decreasing pH of gastric contents may protect against contents may protect against greater pulmonary inflammatory greater pulmonary inflammatory response to aspiration of response to aspiration of gastrointestinal contentsgastrointestinal contents
Peptic Ulcer Disease (PUD) Peptic Ulcer Disease (PUD) ProphylaxisProphylaxis
Surviving Sepsis Campaign Guidelines Surviving Sepsis Campaign Guidelines reviewed literature on PUD prophylaxis:reviewed literature on PUD prophylaxis: ““H2 receptor inhibitors H2 receptor inhibitors are more efficacious are more efficacious that sucralfate and are the preferred agents. that sucralfate and are the preferred agents. Proton Pump Inhibitors have not been Proton Pump Inhibitors have not been assessed in direct comparison with H2 assessed in direct comparison with H2 receptor antagonists and, therefore their receptor antagonists and, therefore their relative efficacy is unknown. They do relative efficacy is unknown. They do demonstrate equivalency in ability to demonstrate equivalency in ability to increase gastric pH.”increase gastric pH.”
Deep Vein Thrombosis (DVT) Deep Vein Thrombosis (DVT) ProphylaxisProphylaxis
Higher incidence of (DVT) Higher incidence of (DVT) in critical illness.in critical illness.
Risk of venous Risk of venous thromboembolism is thromboembolism is reduced if prophylaxis is reduced if prophylaxis is consistently applied.consistently applied.
TARGET: patients TARGET: patients undergoing surgery, trauma undergoing surgery, trauma patients, acutely ill medical patients, acutely ill medical patients, and ICU patients.patients, and ICU patients.
Deep Vein Thrombosis (DVT) Deep Vein Thrombosis (DVT) ProphylaxisProphylaxis
While it is unclear if there is any While it is unclear if there is any association with decreasing rates of association with decreasing rates of ventilator acquired pneumonia, the IHI ventilator acquired pneumonia, the IHI experience is that when applied as a experience is that when applied as a package of interventions for ventilator package of interventions for ventilator care, the rate of pneumonia decreases care, the rate of pneumonia decreases precipitously.precipitously.
The intervention remains excellent The intervention remains excellent practice in the general care of ventilated practice in the general care of ventilated patients.patients.
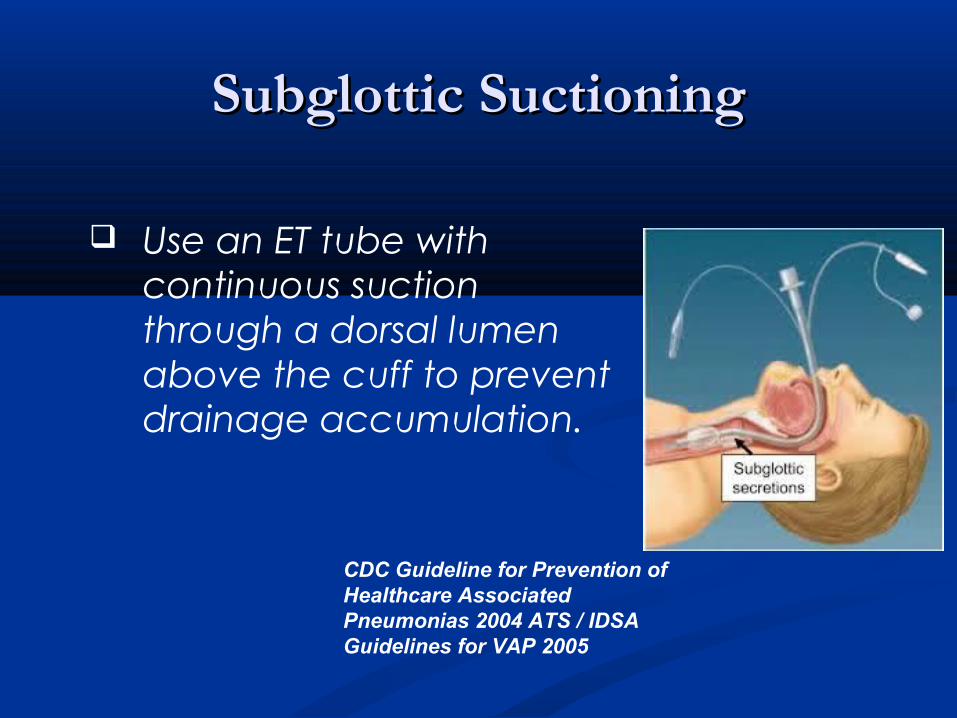
Subglottic SuctioningSubglottic Suctioning
Use an ET tube with continuous suction through a dorsal lumen above the cuff to prevent drainage accumulation.
CDC Guideline for Prevention of Healthcare Associated Pneumonias 2004 ATS / IDSA Guidelines for VAP 2005
Subglottic SuctioningSubglottic Suctioning
Smulders et al. Chest;121:858-862
Daily “Sedation Vacation” and Daily “Sedation Vacation” and Daily Assessment of Readiness to Daily Assessment of Readiness to
WeanWean Correlated with reduction in rate of (VAP).Correlated with reduction in rate of (VAP). Sedation vacation results in significant Sedation vacation results in significant
reduction in time on mechanical reduction in time on mechanical ventilation.ventilation.
Duration of mv decreased from 7.3 days to Duration of mv decreased from 7.3 days to 4.9 days-study by Kress et al. (NEJM 2000).4.9 days-study by Kress et al. (NEJM 2000).
Weaning is easier when patients are able to Weaning is easier when patients are able to assist themselves at extubation with assist themselves at extubation with coughing and control of secretionscoughing and control of secretions
Daily “Sedation Vacation” and Daily Daily “Sedation Vacation” and Daily Assessment of Readiness to WeanAssessment of Readiness to Wean
Sedative agents should be stopped, but not disconnected from Sedative agents should be stopped, but not disconnected from the patient.the patient.
Allow the patient to wake.Allow the patient to wake.
If the patient is co-operative and able to understand commands If the patient is co-operative and able to understand commands leave the sedation off.leave the sedation off.
Distressed or agitated patients require re-sedating.Distressed or agitated patients require re-sedating.
Administer boluses as appropriate to achieve safety.Administer boluses as appropriate to achieve safety.
Review the patient’s analgesic requirements if sedation remains Review the patient’s analgesic requirements if sedation remains off.off.
Sedation Vacation RisksSedation Vacation Risks
Increased potential for Increased potential for self-extubation.self-extubation.
Increased potential for Increased potential for pain and anxiety.pain and anxiety.
Increased tone and poor Increased tone and poor
synchrony with the synchrony with the ventilator during the ventilator during the maneuver may risk maneuver may risk episodes of desaturationepisodes of desaturation
VAP TreatmentVAP Treatment
Evidence-Based GuidelinesEvidence-Based Guidelines
General Principals of choosing General Principals of choosing appropriate VAP therapy:appropriate VAP therapy:
Knowledge of organisms likely to be present.Knowledge of organisms likely to be present.
Local resistance patterns within the ICU.Local resistance patterns within the ICU.
A rational antibiotic regimen. A rational antibiotic regimen.
A rationale for antibiotic de-escalation or A rationale for antibiotic de-escalation or stoppage.stoppage.
General Principals of choosing General Principals of choosing appropriate (VAP) therapy:appropriate (VAP) therapy:
Action Blood cultures, 2 sets Urine analysis with culture Thoracentesis, if pleural effusion present Consider antiatelectatic measures (increase of positive-end expiratory pressure and/or tidal vol, bronchodilators, chest physical therapy [including suctioning])
General Principals of choosing General Principals of choosing appropriate VAP therapy:appropriate VAP therapy:
Inadequate therapy during the initial 48 h, despite Inadequate therapy during the initial 48 h, despite provision of adequate therapy after BAL results, was provision of adequate therapy after BAL results, was associated with a mortality rate of 91% .When associated with a mortality rate of 91% .When empirical therapy was appropriate, mortality rates empirical therapy was appropriate, mortality rates were much lower (38%). Delays in the were much lower (38%). Delays in the administration of appropriate antibiotic therapy for administration of appropriate antibiotic therapy for VAP have been associated with excess mortality.VAP have been associated with excess mortality.
Delay in appropriate therapy for 24 h or more was Delay in appropriate therapy for 24 h or more was associated with a 69.7% mortality, compared to associated with a 69.7% mortality, compared to 28.4% in patients treated without the delay (28.4% in patients treated without the delay (PP < < 0.001)0.001) Luna et al. 2003
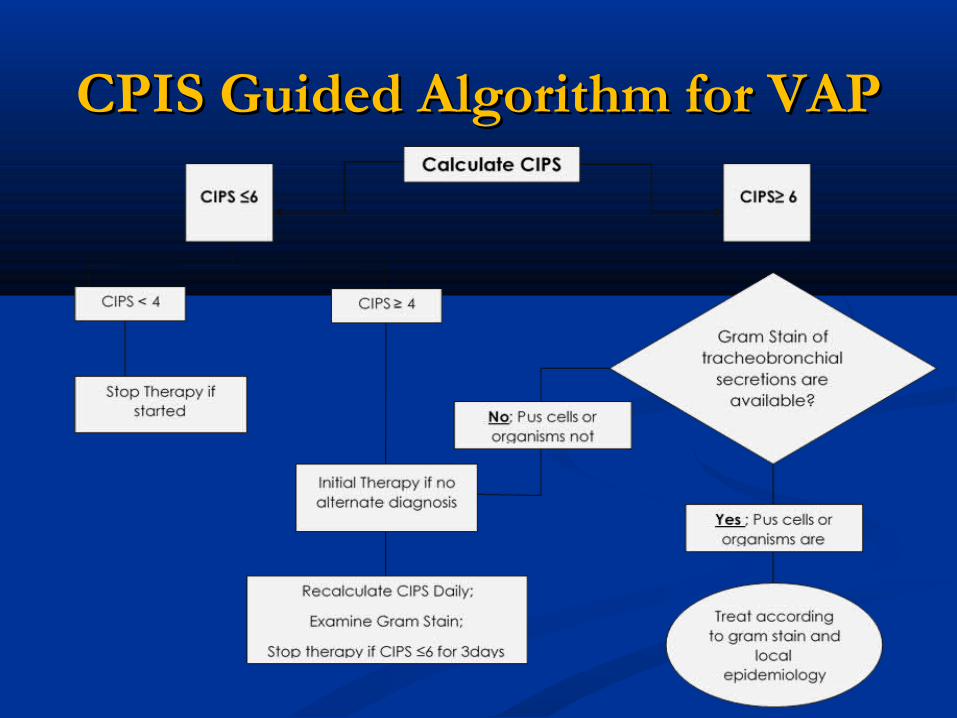
CPIS Guided Algorithm for VAPCPIS Guided Algorithm for VAP
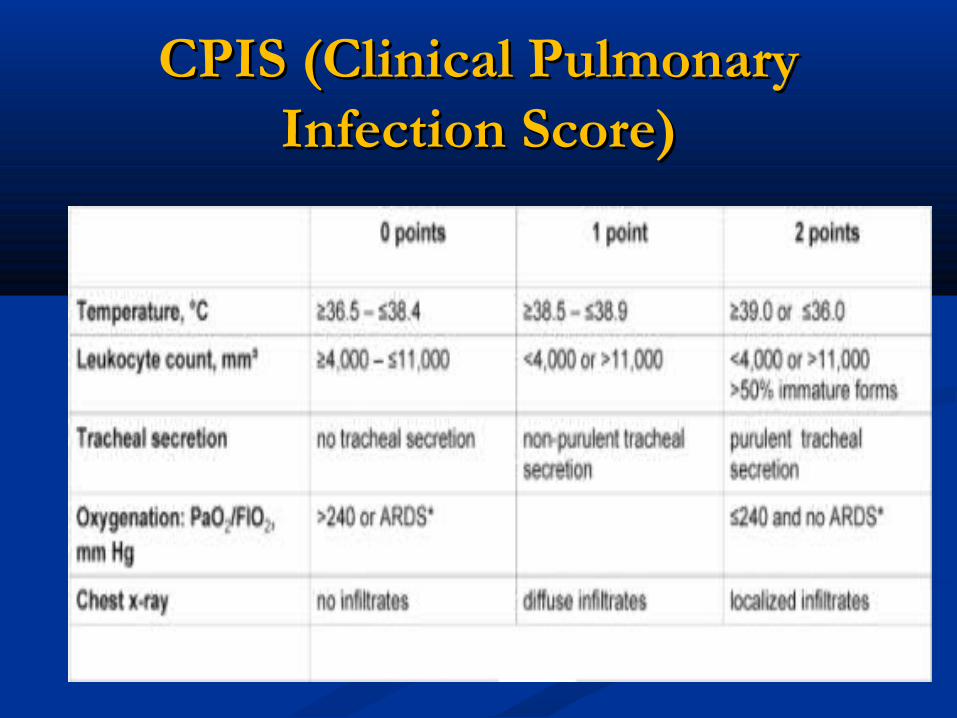
CPIS (Clinical Pulmonary CPIS (Clinical Pulmonary Infection Score)Infection Score)




















![[Validated Audit Process (VAP)] EICC Manual Pengendalian VAP](https://img.dokumen.tips/doc/110x75/587748571a28ab514f8b5fa7/validated-audit-process-vap-eicc-manual-pengendalian-vap.jpg)









