2. Chest devices are encountered on daily basis byradiologists
Chest tubes, central lines, endotracheal tubes and NG tubes are
common New devices are constantly being introduced 3. It is
important to recognizer the presence of a deviceand to have an
understanding of its function as well as complications associated
with its use 4. The proliferation of intensive care units and
theadvances in the treatment of the very ill have greatly increased
the numbers of examinations performed at the patients bedside.
Obtaining a daily chest radiograph is standard practice in most
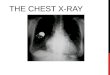
intensive care units 5. Chest radiograph shows that the tip of the
endotracheal tube (black arrow) is slightly above the aortic arch
and well above the carina, in good position. A right chest tube
(white arrow), ECG leads (E), a gown snap (G), and oxygen tubing
(O) are also visible. 6. Medical devices Extra thoracic devices
Pleural devices Tracheal Esophageal Vascular Cardiac Circulatory
assist devices 7. Extra thoracic devices Tubing, clamps, syringes
Ventilator support tubing ECG electrodes Breast prostheses other
apparatus often lie on or under the patient andare imaged with the
chest during the radiographic examination 8. Chest radiograph shows
halo apparatus (with emergencywrench close at hand) for cervical
spine stabilization. 9. ECG leads 10. Pleural Devices chest tubes
are commonly used for evacuating fluid orair from the pleural space
Antero superiorly for pneumothorax Poster inferiorly for fluid
collection 11. Frontal (a) and lateral (b) views show a
thoracostomy(chest) tube ingood position for treatment of a
pneumothorax but not for an effusion. 12. Chest tubes are commonly
used for evacuating uid or air from the pleural space. The normally
positioned tube lies on the surface of the expanded lung, between
the visceral and parietal pleura. The tube is usually placed
anterosuperiorly to evacuate a pneumothorax and posteroinferiorly
for uid collections. 13. the normally positioned tube lies on the
surface of theexpanded lung, between the visceral and parietal
pleurae. Pigtail catheters may be used in place of standard
thoracostomy tubes, and they are popular for empyema drainage and
for installation of medication for treatment of an empyema 14.
Frontal view of the chest shows a pigtail catheter that had
beeninserted under fluoroscopic guidance into a loculated right
empyema for instillation of urokinase and fluid drainage. 15.
Assess the position of chest tube in both frontal andlateral view
and sometime may required CT scanComplication Malposition May enter
the interlobar fissure Lung parenchyma Subcutaneous tissue Tube may
be kinked 16. 58-year-old woman with extrapleural placement of
chesttube. Magnified anteroposterior chest radiograph shows
misplaced chest tube (arrows) within right chest wall. 17.
65-year-old woman with extrapleural placement of chest tube. A,
Magnified anteroposterior chest radiograph shows left chest tube
(arrow) in apparently adequate position. CT scan was requested to
further investigate because of ineffective drainage of left pleural
effusion. 18. Magnified axial CT image shows misplacement of
chesttube within chest wall (arrow). 19. 69-year-old man with
intrafissural placement of chest tube. A, Magnified anteroposterior
chest radiograph showshorizontal course of right chest tube
(arrows). 20. 49-year-old man with intraparenchymal placement
ofchest tube. A, Scout image shows chest tube (arrow) projecting
over right mid lung field. 21. Magnified CT image shows chest tube
(thick arrow)coursing through right upper lobe. There is associated
small pneumothorax (asterisk) and subcutaneous emphysema (thin
arrow). 22. 48-year-old man with chest tube kinking.
Magnifiedposteroanterior chest radiograph performed after chest
tube placement shows kinking of chest tube (arrow) precluding
adequate pleural drainage. 23. 37-year-old man with mediastinal
placement of chest tube. A, Anteroposterior chest radiograph shows
left chest tube (arrows)in inappropriate position, directed
medially and projecting across mediastinum. There is persistent
left pleural effusion. 24. 37-year-old man with mediastinal
placement of chest tube. B, CT image at level of pulmonary artery
trunk confirmsthat tip of chest tube (arrow) is in anterior
mediastinum. 25. 30-year-old male victim of motor vehicle trauma
with abdominal placement ofchest tube. A, Anteroposterior chest
radiograph shows horizontally oriented chest tube (arrow) in left
lower hemithorax. There are several left rib fractures,
opacification of left hemithorax, and subcutaneous emphysema. 26.
30-year-old male victim of motor vehicle trauma with abdominal
placement of chest tube. B, CT image shows traumatic left
diaphragmatic rupture with migration of abdominal content to left
hemithorax. Chest tube (black arrow) is seen within mesenteric fat
abutting small bowel loops. Note splenic rupture (white arrow)
related to trauma. 27. Tracheal Device Tracheal intubation is a
life saving procedure but canbe life threatening if placed
incorrectly The tip of the tube should be 5 cm above the carina 28.
The carina is just cauded to the aortic arch 29. Chest radiograph
shows that the tip of the endotracheal tube(black arrow) is
slightly above the aortic arch and well above the carina, in good
position. A right chest tube (white arrow), ECG leads (E), a gown
snap (G), and oxygen tubing (O) are also visible. 30. Complications
When advanced too far, the endotracheal tube usuallyenters the
right main bronchus, causing various combinations of hyperinflation
and atelectasis of the two lungs, depending on the positions of the
end and side holes. endotracheal tubes can also be placed in the
esophagus the soft tissues of the neck. 31. 6-year-old woman with
misplaced endotracheal tube. Magnifiedanteroposterior chest
radiograph shows that tip of endotracheal tube (thick arrow) is too
high, at level of thoracic inlet. Endotracheal tube cuff (thin
arrows) is overdistended. This abnormal position may cause vocal
cord injury. 32. 60-year-old woman with inadvertent right main
bronchialintubation. Anteroposterior chest radiograph shows
endotracheal tube tip (arrow) in right main bronchus, resulting in
complete collapse of left lung and leftward shift of mediastinum.
33. Frontal view shows a double-lumen endotracheal tubewith
selective intubation of the left main bronchus (arrow). 34.
66-year-old man with left-sided double-lumen endotracheal tube.
Magnifiedanteroposterior chest radiograph shows double-lumen
endotracheal tube with its left tip (thick arrow) in left main
bronchus. Right tip (thin arrow) is noted within trachea for
ventilation of right lung. Double-lumen endotracheal tube allows
control of distribution of ventilation to each lung. It is
important to differentiate between double-lumen endotracheal tubes
and inadvertent selective bronchial intubation with single-lumen
catheters. 35. Esophageal devices NG tubes Esophageal balloons
Esophageal stents PH probe 36. NG tubes Nasogastric tubes and
feeding tubes are frequentlyvisualized passing through the
mediastinum on their way to the stomach and intestines. Esophageal
balloons and esophageal stents used to treat benign and malignant
esophageal disease may manifest themselves at chest radiography.
37. Vascular devices Routinely used for Monitoring hemodynamic
function Hemodialysis Administrating fluids Medication Nutrition
38. Venous devices are usually inserted, eitherpercutaneously or
surgically, via the subclavian, internal jugular, or femoral veins.
Arterial devices usually are placed through the femoral artery
central lines typically have one to three lumens A central venous
catheter is ideally positioned in the superior vena cava for the
monitoring of pressure or infusion of medication and nutrition. 39.
Swan-Ganz is a multilumen catheter used formeasuring hemodynamic
pressures and cardiac output.A better term to use is pulmonary
artery catheter. Accurate measurement of pulmonary arterial wedge
pressure 40. chest radiograph shows a right subclavian
single-lumencentral venous catheter and a left subcutaneous port
catheter, which enters via the left subclavian vein. Both catheter
tips are in the superior vena cava. 41. The port is usually
connected to a central venouscatheter or to an arterial catheter
and can be used for instillation of fluids, medications,
chemotherapeutic agents, parenteral nutritional solutions, and
blood products. It can also be used for withdrawal of blood
samples. 42. Frontal view of the chest shows a left subclavian
Groshongcatheter with its tip in the proximal most portion of the
superior vena cava. (b) Close up view of the catheter tip. 43.
Groshong catheter has closed, rounded tip Near the tip in the side
of the catheter is a three-position valve. The valve is designed to
allow fluid to flow in and out through the valve, but it remains
closed when it is not in use. This catheter does not require
routine clamping or heparin solution to keep open. It does require
periodic flushing with 0.9% normal saline. 44. A good rule of thumb
is that the catheter tipshould be within the mediastinal shadow.
Placement more distally increases the chance of pulmonary
infarction or vessel rupture. 45. Frontal chest radiograph shows a
right jugular Swan-Ganz catheter with its tip (arrow) in the right
lower pulmonary artery. 46. Frontal chest radiograph shows a
Swan-Ganz catheter(white arrow) in the left pulmonary artery via
the inferior vena cava. Note also the bilateral chest tubes (black
arrows) and ECG leads (E). 47. Complications of catheter insertion
vary with the catheters used and the sites employed Pneumothorax is
a common complication Vessel lacerations and perforations can
produce hematomas, hemothorax, and infusion of fluid into the
mediastinum, thorax, or other inappropriate space Nerve injury is
usually a complication of improper puncture technique Looping of
catheters may lead to knotting. 48. Malpositioning of pulmonary
artery catheter isexceedingly common, found in approximately 25% of
catheters placed. This may lead to false readings and an increased
risk for complications. Complications of pulmonary artery catheter
placement include pneumothorax, pulmonary infarction, cardiac
arrhythmias, pulmonary artery perforation, endocarditis, and sepsis
49. Cardiac Devices Cardiac pacemakers, valve prostheses, and
artificialhearts chest radiography is commonly employed in the
assessment of patients with heart disease recognition of cardiac
devices and the problems associated with them is important for all
individuals involved in the care of these patients. 50. Heart
valves Mechanical Biologic Mechanical Heart valves most require
life-long treatmentwith anticoagulants. Biologic valves are less
durable than mechanical valves, with some deterioration developing,
frequently 510 years after placement, but they do not usually
require anticoagulant treatment. It is not important and often
impossible to know the specific name of a particular prosthetic
heart valve, but it is important to recognize its presence The
mitral and aortic valves are those most commonly replaced 51.
Mechanical heart valve. Lateral view of the chest shows a
Hemextilting bileaflet mechanical mitral valve prosthesis. Median
sternotomy wires and surgical clips are also evident. 52.
Mechanical heart valve. Lateral view of the chest shows
aStarr-Edwards caged ball mechanical mitral valve prosthesis. 53.
Biologic heart valve. Frontal view of the chest shows aHancock
porcine mitral valve prosthesis (arrow). A singlelead pacemaker,
ECG leads, and median sternotomy wires are also seen. 54. Biologic
heart valve. Frontal view of the chest shows aHancock porcine valve
prosthesis in a Rastelli conduit going from the right ventricle to
the pulmonary artery. 55. Lateral view of the chest in an elderly
patient shows a mitral annuloplastyring (black arrow) and a
dual-lead cardiac pacemaker. Sternal wires, surgical clips, and ECG
leads are also present. The sternal wires are used to close a
sternal dehiscence. The patient has both horizontal sternal wires
and vertical intercostal wires (white arrows). 56. Lateral view of
the chest in a child shows an occlusionbasket (umbrella) for
treatment of an atrial septal defect. 57. Cardiac Pacemakers common
in older adults being treated for abnormalcardiac rhythms caused by
coronary artery disease Cardiac pacemakers improve cardiac
function, reduce the severity of clinical symptoms, and reduce
mortality and morbidity. A cardiac pacemaker is composed of two
main elements: (a) a pulse generator and (b) lead wires with
electrodes for contact with the endocardium or myocardium 58.
Pacemakers range from simple temporary epicardialelectrodes to very
complex pacemakers with multiple atrial and ventricular leads 59.
Frontal (a) and lateral (b) views of the chest show a single
electrode epicardialcorkscrew subxiphoid pacemaker (arrowhead in a,
black arrow in b). There are also coils (white arrow) occluding a
previous right Blalock-Taussig shunt. In addition, ECG leads and
sternal wires are evident. 60. Frontal (a) and lateral (b) views
show an atrioventricularsequential pacemaker with one electrode in
the right atrial appendage (RA) and the other at the right
ventricular apex (RV). Also shown are ECG leads (E) and the
battery-control pack (B) for the pacemaker. 61. Biventricular
devices (CRT) 62. Because there can be such a wide variation in
theproper positioning of pacemaker leads, it is often difficult for
the to know if a pacemaker is properly positioned. Pacemaker lead
fracture is now rarely seen because of improvements in the
flexibility of the metal alloys used in electrode construction. 63.
Coronary Artery Surgery and Stents Revascularization techniques
include CABG surgery,coronary artery angioplasty, and coronary
artery stent placement. Median sternotomy is the usual surgical
approach for CABG surgery, and sternal wires the common method of
fixation of the two sternal segments At present, almost 90% of
coronary interventions include stent placement Complications
associated with coronary artery stents are stent thrombosis and
restenosis. 64. Lateral view of the chest shows sternal wires
(arrowhead), vascular clips ofa saphenous vein bypass graft to the
right coronary artery (curved arrow), and those of the left
internal mammary graft to the left anterior descending coronary
artery (straight arrow). 65. PA chest radiograph demonstrates
bilateral pulmonary artery stents ina patient with bilateral
pulmonary artery stenosis and aneurysmal right ventricular outflow
tract following tetralogy repair. 66. Circulatory Assist Devices
The high mortality from cardiogenic shock continuesto spur efforts
to develop mechanical support for the circulatory system Most
mechanical support for patients with heart failure consists of
devices that assist the heart without replacing it. 67. Mechanical
cardiac assist devices can be divided into three groups: (a)
temporary cardiac assist devices (b) permanent cardiac assist
devices (c) heart replacement devices. short-term cardiac assist
devices are the intraaotic balloon pump and newer left ventricular
assist devices (VADs) 68. Frontal (a) and lateral (b) views of the
chest show aThoratec left VAD (arrow). 69. Abdominal image shows a
HeartMate VAD. 70. Abdominal image shows a Novacor VAD. 71. chest
show a CardioWest total artificial heart. the four prostheticvalves
and the two coil, reinforced polyurethane tubes carrying pulses of
compressed air to the two artificial ventricles. 72. Cropped
frontal view (a) and full lateral view (b) of the chest show a
CardioWest total artificial heart. Note the four prosthetic valves
and the two coil, reinforced polyurethane tubes carrying pulses of
compressed air to the two artificial ventricles. 73. More x rays
for interactive session 74. 30-year-old man with malpositioned
feeding tube. Anteroposteriorchest radiograph shows that feeding
tube has entered right main bronchus, traversed right lower lobe
bronchus (white arrows), and has its tip overlying right upper
quadrant of abdomen (black arrow), raising concern for possible
perforation of right hemidiaphragm. Note associated right
pneumothorax (asterisk). 75. Frontal view of the chest shows
ping-pong ball plombagein the right apex, as well as a cardiac
pacemaker. 76. Frontal view of the chest shows a right apical
oleothorax(wax plombage). Extensive pleural calcification includes
the surface of the wax ball (arrows). 77. Implanted bilateral brain
stimulators 78. A pacemaker is one of the common devices
encountered on a chest x-ray. The usual location for a pacemaker is
the anterior left upper chest wall (black arrow). Pacemakers may
have either 1 or 2 leads. The wires connecting the pacemaker to the
intracardiac electrodes must be intact (yellow arrow). The typical
position ofthe cardiac electrodes is in the right ventricle (red
arrow) for a single lead, and also in the right atrium for a
dual-lead pacemaker. It is important to compare the electrode
position to that in previous studies because an electrode may
become dislodged. 79. a) Frontal view of the chest shows an
esophageal stent (blackarrows) that was placed to ameliorate the
effects of an esophageal malignancy. There are also two chest tubes
(), a peripherally inserted central catheter (white arrow), ECG
leads (E), a gown snap (G), and a transjugular intrahepatic
portosystemic shunt (T) in the liver. 80. Frontal view of the chest
shows a left jugular Swan-Ganz catheter (arrows), which passes
through a persistent left superior vena cava into the coronary
sinus, through the right atrium and right ventricle, and into the
right pulmonary artery. Also seen are a subcutaneous port (P), an
endotracheal tube (ET), an ECG lead (E), and a nasogastric tube
(not labeled). 81. The electrode is placed in the epidural space
adjacent to the spinal cord. The wires are connected to a
stimulating generator implanted subcutaneously. The electrode
generates a weak electrical current that interrupts the
transmission of pain at a spinal cord level. Spinal cord
stimulation (SCS) is recommended as a treatment option for adults
with chronic pain of neuropathic origin. Most frequently: Brachial
plexopathy, Post-laminectomy syndrome, Post Chemotherapy
Neuropathy, Complex Regional Pain Syndrome (types I and II) and HIV
polyneuropathy. 82. The implantable loop recorder (ILR) is a
subcutaneous electrocardiographic monitoring device that stores ECG
data automatically in response to specific rhythm anomalies or in
response to patient activation.It is mainly used for diagnosis in
patients with recurrent unexplained episodes of syncope or
palpitations, but is also useful for long-term monitoring in
patients with documented or suspected atrial fibrillation, for risk
stratification in patients who have sustained a myocardial
infarction and those who have certain genetic disorders. 83.
48-year-old woman with extravascular placement of
double-lumendialysis catheter. A, Anteroposterior chest radiograph
shows catheter (arrow) inserted via right subclavian vein with its
tip projecting over right atrium. 84. 48-year-old woman with
extravascular placement of double-lumendialysis catheter. B,
Because there was clinical suspicion of malpositioning of catheter,
IV contrast medium was injected and was seen to extravasate into
pleural space (arrows). 85. 72-year-old woman with pulmonary
infarction as complication ofpulmonary artery catheter placement.
Magnified anteroposterior chest radiograph shows that tip of
catheter (black arrow) is too distal (i.e., > 2 cm lateral to
hilum). There is wedged-shaped opacity (white arrows) distal to
catheter, consistent with pulmonary infarction. 86. 75-year-old
woman with displacement of pacemakerlead. A, Posteroanterior chest
radiograph shows dual-lead pacemaker. Tip of right ventricular lead
(arrow) is projected at edge cardiac silhouette. 87. 67-year-old
man with pacemaker lead fracture. Magnifiedanteroposterior chest
radiograph shows fracture (arrow) in pacemaker lead near
battery-control pack. Lead fractures most commonly occur at venous
access site, near tip, or near batterycontrol pack. 88. 7-year-old
man with normal positioning of intraaortic counterpulsation balloon
pump. B, Magnified anteroposterior chest radiograph obtained during
diastole shows inflated radiolucent balloon (thin arrows) as well
as radiopaque tip (thick arrow) within upper descending thoracic
aorta. Catheter is inflated during diastole to increase myocardial
perfusion and is deflated during systole to decrease left
ventricular afterload. 89. misplaced central venous catheters.
6-year-old girl. Posteroanterior chest radiograph shows two
misplacedcatheters. Right internal jugular central venous catheter
(black arrow) has its tip in right atrium. Left subclavian central
venous catheter (white arrow) has its tip in right subclavian vein.
90. Conclusion Various devices are used to monitor and treat
criticallyill patients. The radiographic evaluation of these
devices is important because the potentially serious complications
arising from their introduction and use are often not clinically
apparent. Familiarity with normal and abnormal radiographic
findings is critical for the detection of these complications. 91.
Recommendation The American College of Radiology recommends
dailychest radiography for critically ill patients who have acute
cardiopulmonary disease or are receiving mechanical ventilation, as
well as immediate imaging for all patients who have undergone
placement of endotracheal tubes (ETTs), feeding tubes, vascular
catheters, and chest tubes. These recommendations are made because
the malpositioning of these devices and the serious complications
that may ensue are often not clinically apparent. Radiographic
evaluation of these devices is important, albeit challenging,
because of the technical limitations of portable chest radiography
and the inability of patients to cooperate. 92. Thank You