Embed Size (px)
Citation preview
Managing diabetes in critically ill hospitalized diabetic patient
Dr. Sumit VermaPost graduate trainee,Dept. of general medicine,medical college & hospital, kolkata.

Hyperglycaemia in hospitalised patients
Hyperglycemia in a known diabetic
Hyperglycaemia in an undetected diabetic
Stress hyperglycaemia.
Stress hyperglycaemia is a means of ensuring adequate delivery of glucose to brain during stress.
Glucose uptake of cns depends on plasma glucose concentration and adequate cerebral blood flow(not dependent on insulin).
Regulated by higher neural centres.
Potential role in etiology of Type I /Type 2 DM
Stress hyperglycaemia may be assosciated with poorer prognosis because it represents a condition of greater gravity causing decompensation in normal individual
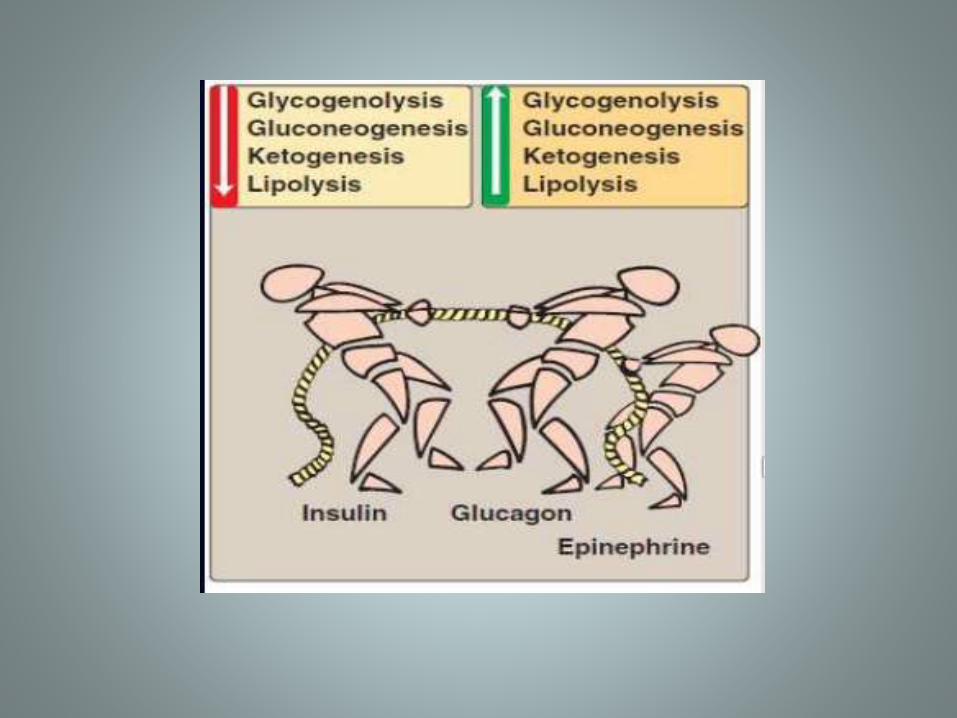
Stress hyperglycaemia
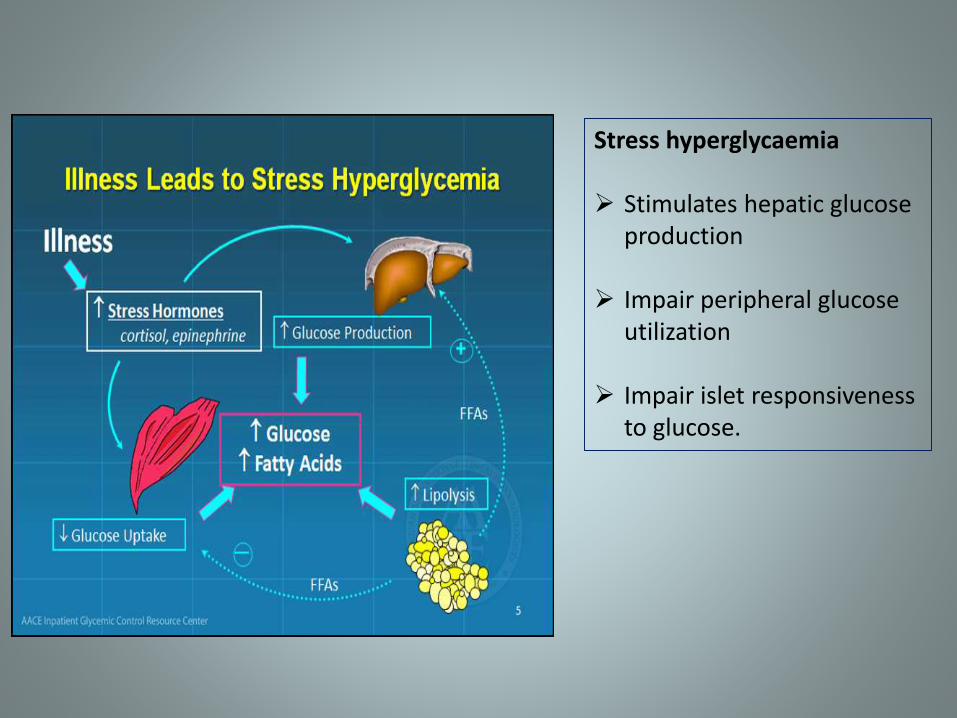
Stress hyperglycaemia
Stimulates hepatic glucose production
Impair peripheral glucose utilization
Impair islet responsiveness to glucose.
Causes of stress induced hyperglycaemia
Hypoxia Hypotension Hypoglycemia –by causing neuroglucopenia Myocardial infarction Surgery Burns Trauma Cold stress
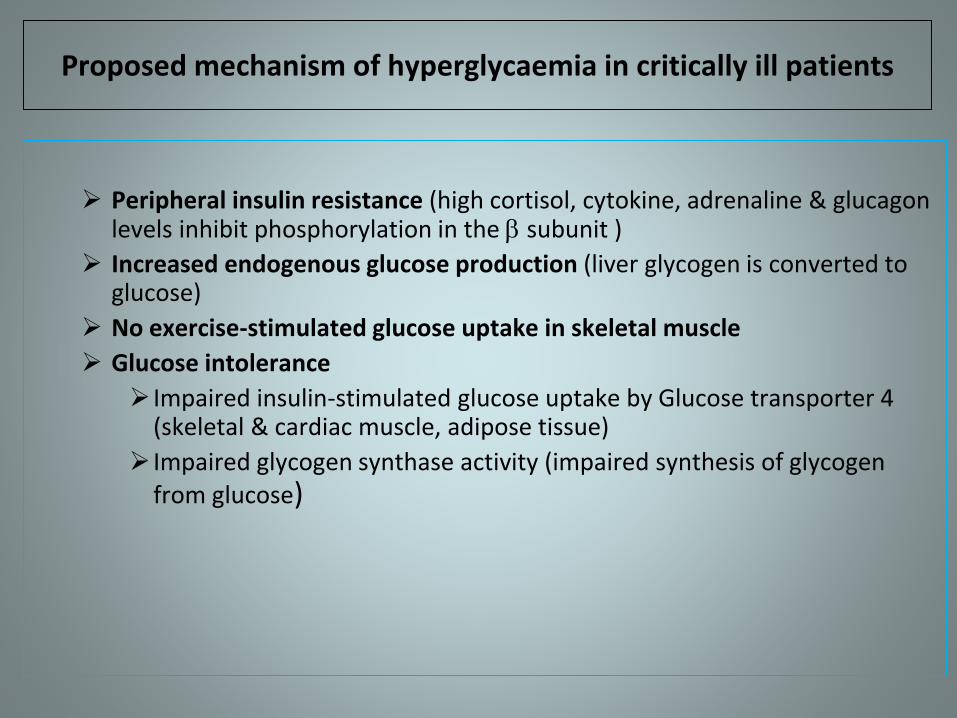
Proposed mechanism of hyperglycaemia in critically ill patients
Peripheral insulin resistance (high cortisol, cytokine, adrenaline & glucagon levels inhibit phosphorylation in the subunit )
Increased endogenous glucose production (liver glycogen is converted to glucose)
No exercise-stimulated glucose uptake in skeletal muscle
Glucose intolerance
Impaired insulin-stimulated glucose uptake by Glucose transporter 4 (skeletal & cardiac muscle, adipose tissue)
Impaired glycogen synthase activity (impaired synthesis of glycogen from glucose)
Higher mortality in trauma patients
Myocardial infarction patients higher risk of cardiogenic shock and inhospital mortality.
Higher mortality in stroke patients.
Hyperglycaemia is assosciated with increased glutamate level in cerebral cortex which is assosciated with neuronal damage.
Higher mortality in non diabetic critically ill patients
Adverse patient outcome due to prolonged hyperglycaemia
past
Historically little attention paid to glucose control
Lack of benchmarks, guidelines, & evidences
Sliding scale insulin protocols
Glucose control started at >200 mg/dlMinimal insulin usedInsulin drips rareFear of hypoglycemia
Intensive insulin therapy VS Conventional therapy trials
Leuven surgical trial
1548 surgical icu patientsDivided in two armsIntensive arm(mean BG 103 mg/dl)Conventional arm(mean BG153 mg/dl)
ICU mortality was significantly lower in intensive arm (4.6% vs 8%)Intensive insulin therapy reduced critical illness neuropathy, acute renal failure ,transfusion requirement and bacteremia.
Single centre trial

Van den berghe et al
In twelve months period, 1500 Surgical ICU patientsWith intensive insulin therapy (IIT) when the blood glucose levels were maintained < 110 mg/ dlThe conventional group had 1.74 times more mortality
IIT patients had 34% reduction in mortality, 46% reduction in sepsis, 41% reduction in dialysis, 50% reduction in the blood transfusion 44% reduction in polyneuropathy
Then Van den Burghe et al. came back again in 2006,“IIT and understanding it’s impact in medical ICU patients” Could not convincingly prove significant reduction in, in-hospital mortality Reduced hospital stay, ARF and duration of mechanical ventilation.
Digami trial
Diabetes and insulin glucose infusion in AMI 1
IV Insulin in first 24 hours and intensified sc insulin for 3 months showed 29% reduction in mortality at 1 year.
Digami 2 showed no reduction in mortality but decrease in incidence of congestive heart failure and reinfarction at 3 months follow up in intensive therapy group.
Published in 2009, 38 tertiary hospitals and 4 community hospitals,6030 patient evaluable in the period of 5 years (December 2004-November 2008)Again the groups were Intensive vs. Conventional;i.e. 81 to 110 mg per dl vs. <180 mg per dl glucose levels were the targetsThe patients were randomized but not blinded
NICE-SUGAR study (Normoglycemia in Intensive Care Evaluation-Survival Using Glucose Algorithm Regulation study)
The outcome studied were:
90-day mortality
Duration of mechanical ventilation
renal replacement therapy,
Length of stay in ICU/hospital & cause of death.
28-day all-cause mortality,
incidence of organ system failure,
transfusion requirements
new positive blood cultures.

Mortality at 90 days was 27.5% in IIT group vs. 24.9% in conventional group
Mortality at 28 days was 22.3% in IIT group vs. 20.8% in Conventional group
Location of death in ICU65.9% in IIT vs. 66.3% in Conventional groupIn-hospital 26.9% IIT vs. 26.2% Conventional group
Incidently the intensive insulin arm had significantly higher incidence of severe hypoglycaemia(6.8% vs 0.5%)
Results
Summary of clinical trials
Tight glucose control is beneficial predominantly in surgical icu patients but attainment is difficult without the risk of severe hypoglycaemia.
no consistent reduction in mortality with intensive control of glycemia , and increased mortality was observed in the largest published study to date.
although severe hypoglycemic events are observed in an unacceptablyhigh number of patients receiving intensive insulin therapy with protocols targeting a BG of 80 to 110 mg/dL, this risk can likely be minimizedwith relaxation of targets, improvement and standardization of protocols, and their careful implementation .
Maintain BG level at a range of 140-180 mg/dl for majority of patients with medical morbidity and 110-140 mg/dl for those with surgical morbidity.
Only iv insulin is recommended .subcutaneous regimens with premixed insulins ,intermediate acting or long acting insulin and SSI are not recommended.
Regular insulin or rapid acting insulin analogs (aspart,lispro,glulisine) can be used as iv insulin.glulisine should be used only with normal saline.
Inpatient glucose metrics

Intravenous insulin therapy
Two methods:
Glucose plus insulin infusion: insulin added to dextrose pint and thus delivered together. If delivery of glucose stopped insulin also stopped and viceversa Very safe method of iv insulin delivery. Recommended in patients who are nil by mouth or fasting in
preparation for a surgical procedure or otherwise.
Syringe pump: delivery of insulin is seperated from delivery of glucose which must occur simultaneously. Risk of hypoglycaemia present Rates of insulin delivery can be exquisitely controlled and
modifications can be made on an hourly basis. Probably the best method of glycemic control in patients who
are fasting for any extended period of time.
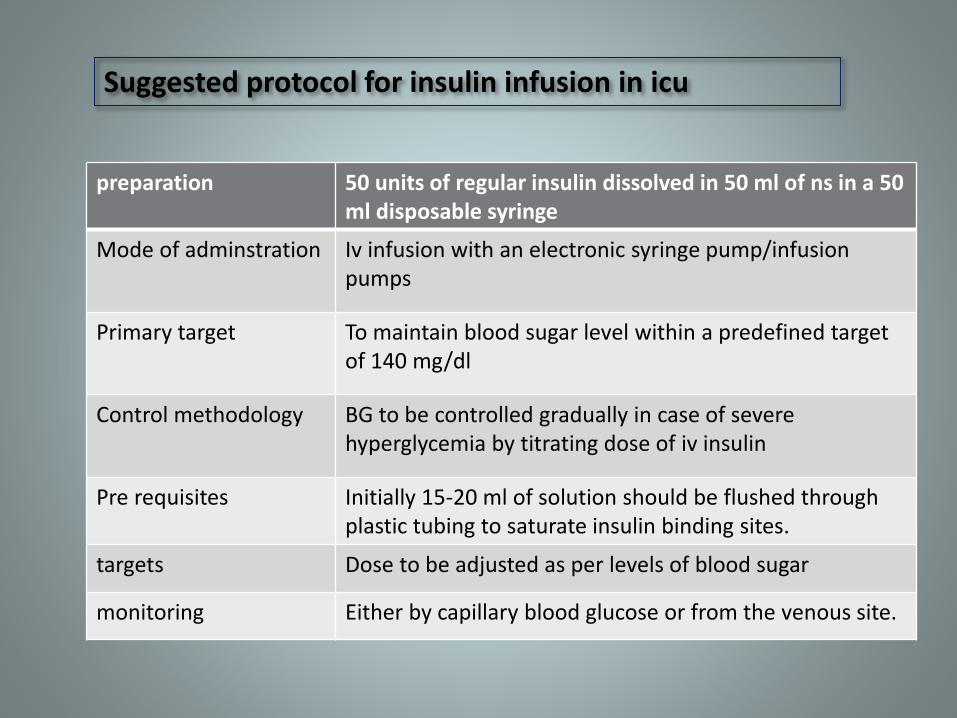
preparation 50 units of regular insulin dissolved in 50 ml of ns in a 50 ml disposable syringe
Mode of adminstration Iv infusion with an electronic syringe pump/infusion pumps
Primary target To maintain blood sugar level within a predefined target of 140 mg/dl
Control methodology BG to be controlled gradually in case of severe hyperglycemia by titrating dose of iv insulin
Pre requisites Initially 15-20 ml of solution should be flushed through plastic tubing to saturate insulin binding sites.
targets Dose to be adjusted as per levels of blood sugar
monitoring Either by capillary blood glucose or from the venous site.
Suggested protocol for insulin infusion in icu
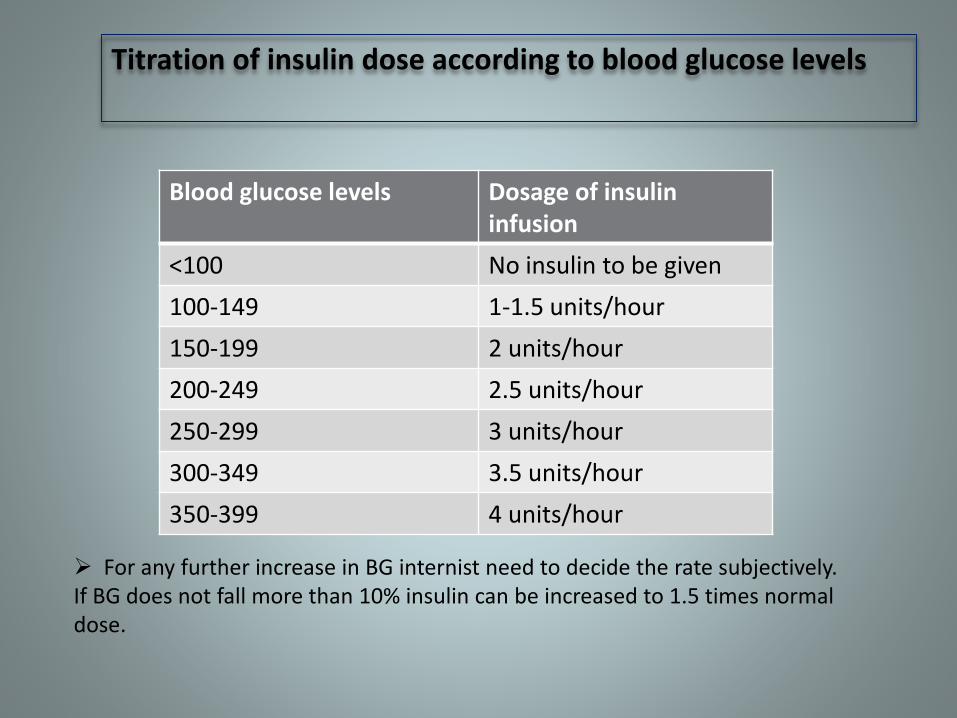
Titration of insulin dose according to blood glucose levels
Blood glucose levels Dosage of insulin infusion
<100 No insulin to be given
100-149 1-1.5 units/hour
150-199 2 units/hour
200-249 2.5 units/hour
250-299 3 units/hour
300-349 3.5 units/hour
350-399 4 units/hour
For any further increase in BG internist need to decide the rate subjectively.If BG does not fall more than 10% insulin can be increased to 1.5 times normal dose.
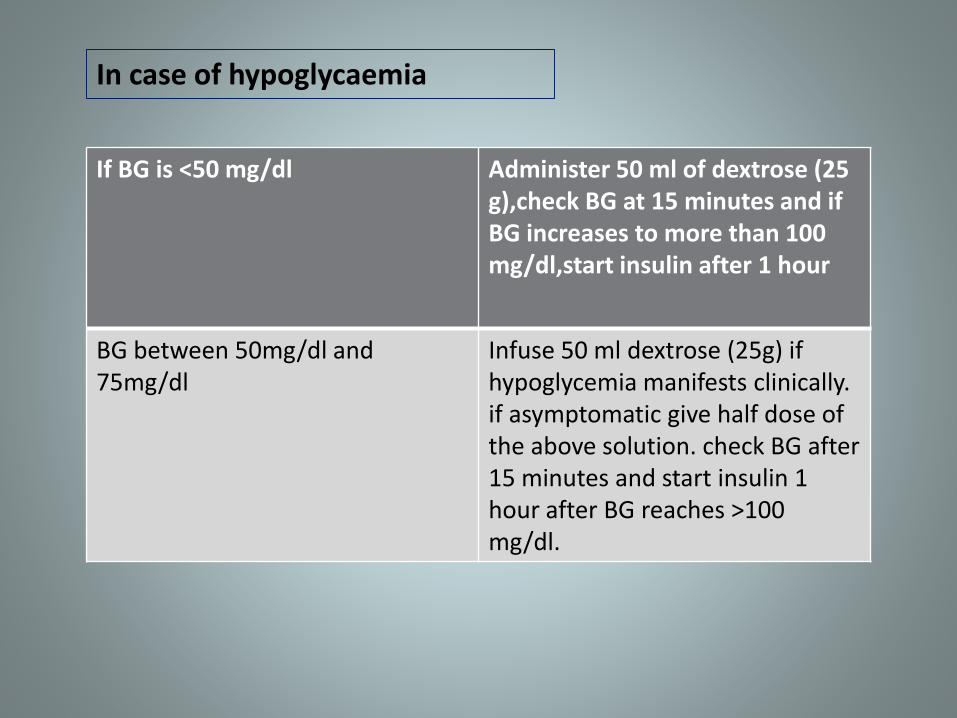
If BG is <50 mg/dl Administer 50 ml of dextrose (25 g),check BG at 15 minutes and if BG increases to more than 100 mg/dl,start insulin after 1 hour
BG between 50mg/dl and 75mg/dl
Infuse 50 ml dextrose (25g) if hypoglycemia manifests clinically. if asymptomatic give half dose of the above solution. check BG after 15 minutes and start insulin 1 hour after BG reaches >100 mg/dl.
In case of hypoglycaemia

Initial estimation at 1 hourly interval
Check every 2 hour if three consecutive readings fall within desired target range
Check every 4 hour if the control target maintained for consecutive 24 hours
Keep on increasing the period of testing in an incremental manner,but revert to earlier steps if the BG exhibits higher readings.
During transition to general ward testing can be structured according to meal timings provided the patient is eating properly.
Monitoring of blood glucose
# If logistic permits CGMS should be used for monitoring BG

Transition to outdoor management
Example insulin requirement while NPO=2 units/hour
adjusted basal dose calculation
patients hourly insulin infusion rate while NPO=2 units/hour
24 hours basal insulin dose during stress=24*2=48 units
abd accounting for stress reduction =2/3*48=32 units of basal insulin/24 hour
Give 50% as basal insulin
Give 50% as scheduled short/rapid acting insulin in divided doses
.
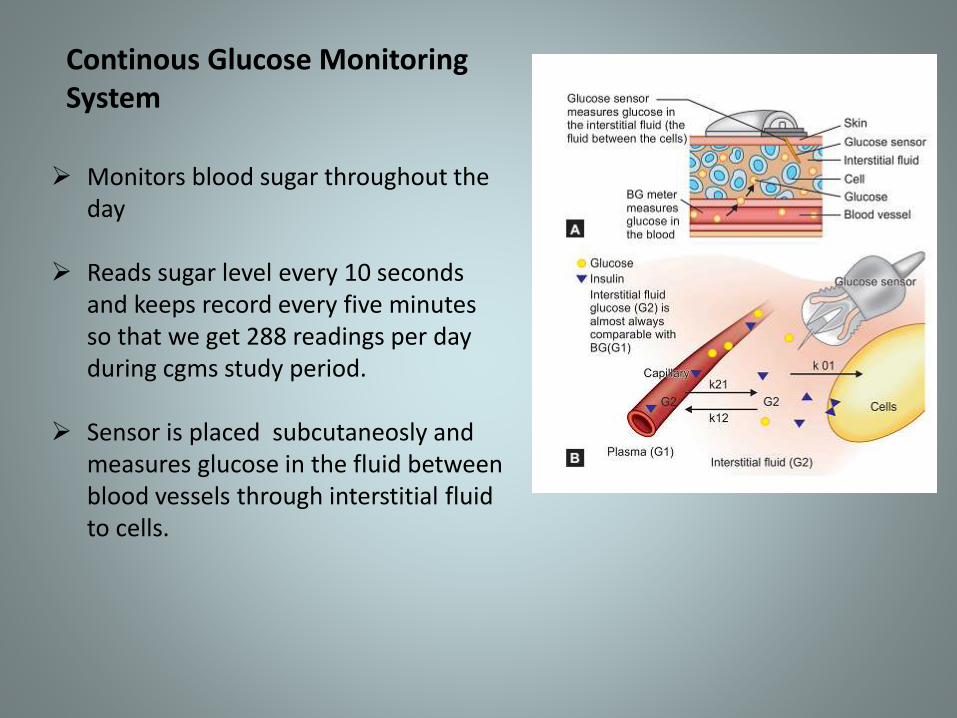
Continous Glucose Monitoring System
Monitors blood sugar throughout the day
Reads sugar level every 10 seconds and keeps record every five minutes so that we get 288 readings per day during cgms study period.
Sensor is placed subcutaneosly and measures glucose in the fluid between blood vessels through interstitial fluid to cells.

Two types of CGMS
Professional cgm(for health care providers)
Personal (REAL- time) continous glucose monitoring (for patients)
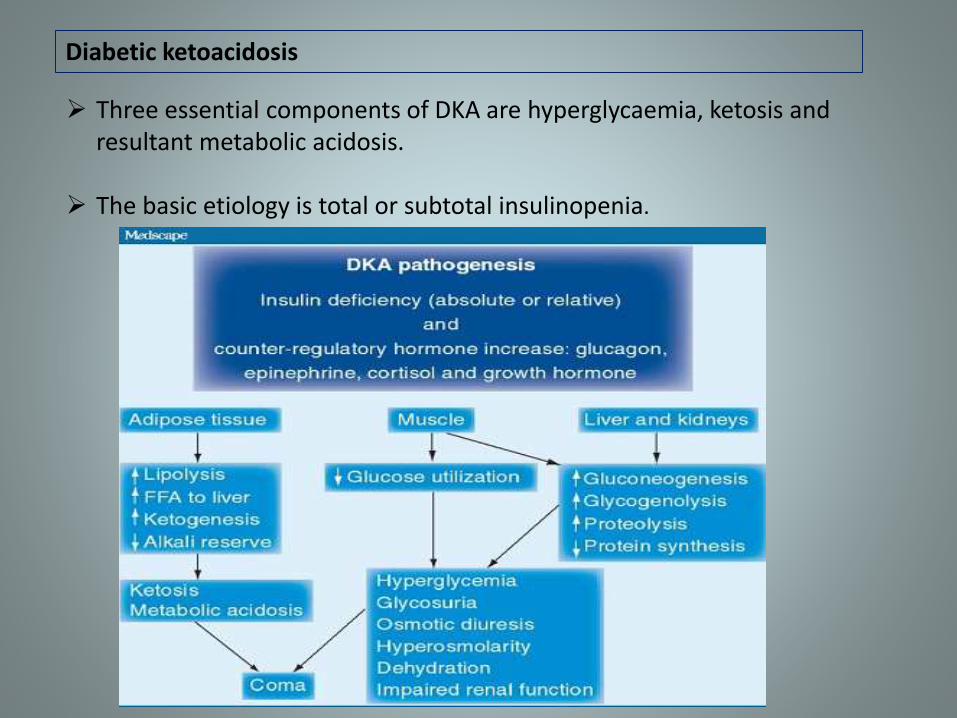
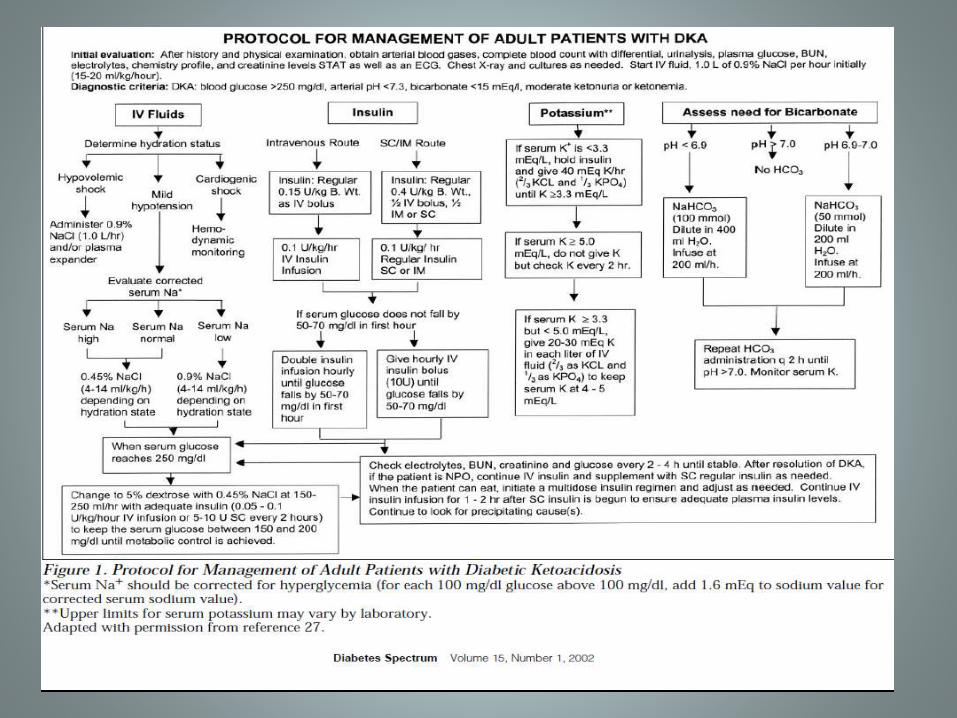
Diabetic ketoacidosis
Three essential components of DKA are hyperglycaemia, ketosis and resultant metabolic acidosis.
The basic etiology is total or subtotal insulinopenia.
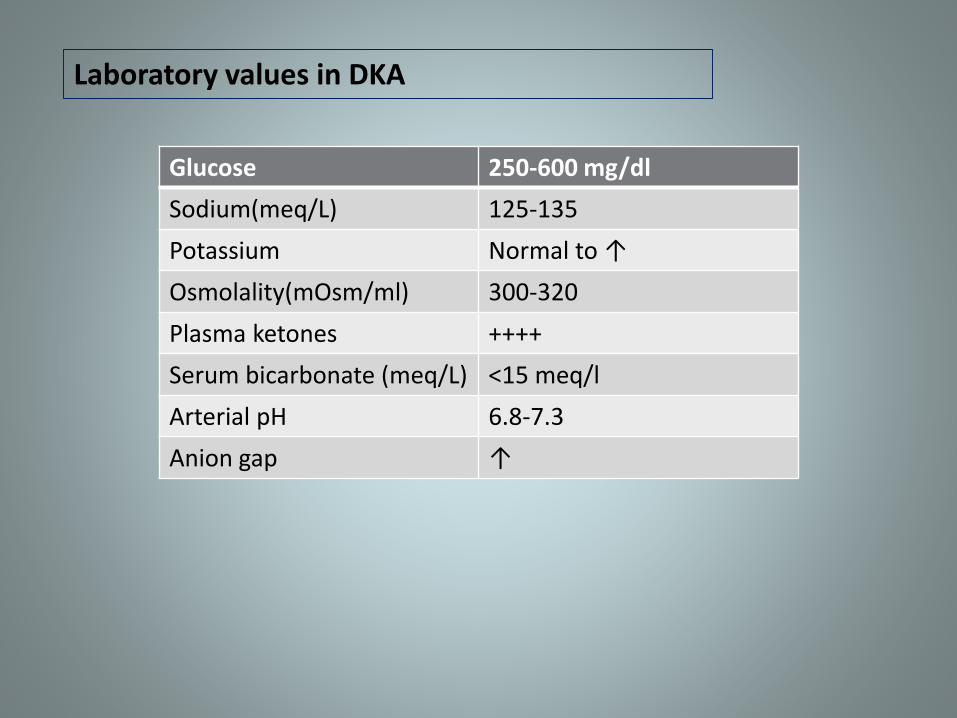
Laboratory values in DKA
Glucose 250-600 mg/dl
Sodium(meq/L) 125-135
Potassium Normal to ↑
Osmolality(mOsm/ml) 300-320
Plasma ketones ++++
Serum bicarbonate (meq/L) <15 meq/l
Arterial pH 6.8-7.3
Anion gap ↑
Manifestation of diabetic ketoacidosis
symptomsNausea/vomiting
Thirst/polyurIa
Abdominal pain
sob
Precipitating events
Inadequate insulin
infection
Infarction
Drugs
pregnancy
Physical findings
Tachycardia
Dehydration/hypotension
Kussumals respiration
Abdominal tenderness
Lethargy/obtundation
2-3 L of 0 .9 % saline over first 1-3 h(15-20 ml/kg per hour);
Subsequently 0.45% saline at 250-500 ml/h
Change to 5% glucose and 0.45% saline at 150-250 ml/h when plasma glucose reaches 200mg/dl
Fluid replacement
Insulin adminstration in DKA
Adminster short acting insulin iv 0.1 units/kg then 0.1 units/kg per hour by continuous iv infusion.
Increase two to three folds if no response by 2-4 hours
If initial k+ is < 3.3 meq/L do not adminster insulin until the potassium is corrected.
If the initial serum potassium is >5.2 meq/L do not supplement k+ until the potassium is corrected.
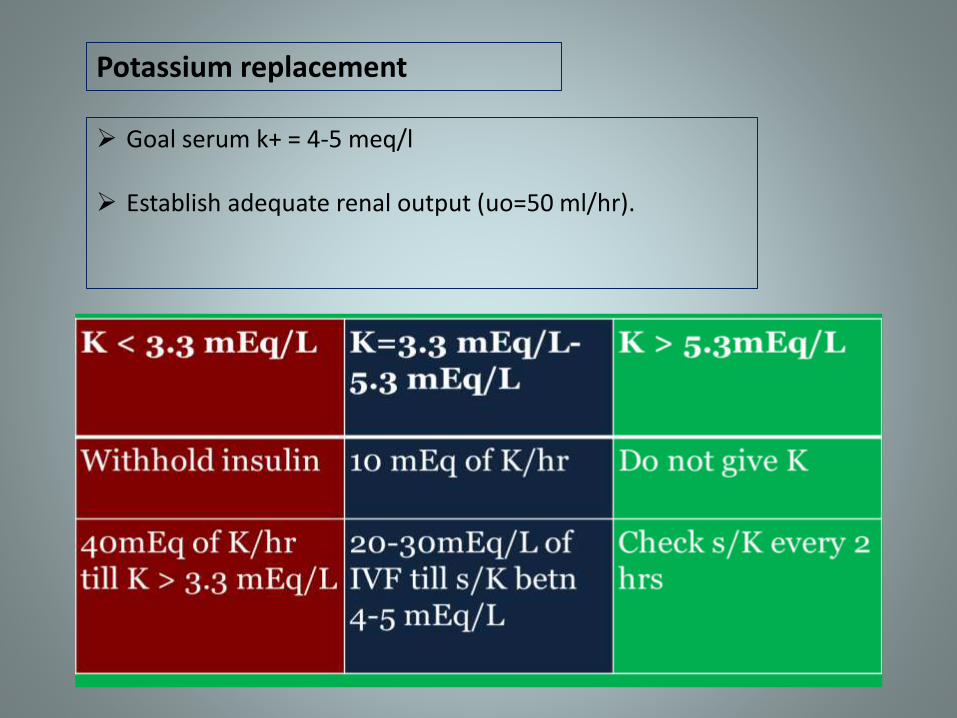
Potassium replacement
Goal serum k+ = 4-5 meq/l
Establish adequate renal output (uo=50 ml/hr).
Only if ph <7.2
Bicarbonate 50 Meq/L of sodium carbonate in 200 ml of sterile water with 10 meq/L KCl per hour for 2h until the ph >7
Bicarbonate adminstration and rapid reversal of acidosis may impair cardiac function, reduce tissue oxygenation and promote hypokalemia.
Bicarbonate therapy in DKA
Resolution of DKA
Goals Resolve ketoacidosis Normal ag Ketones may remain because of slower resolution of acetone
Neurologicaly alert
Plasma osmolarity<315 mosm/ml
Taking oral feeds
Add long acting insulin based on prior dosing or 24 hour insulin requirements on drip.
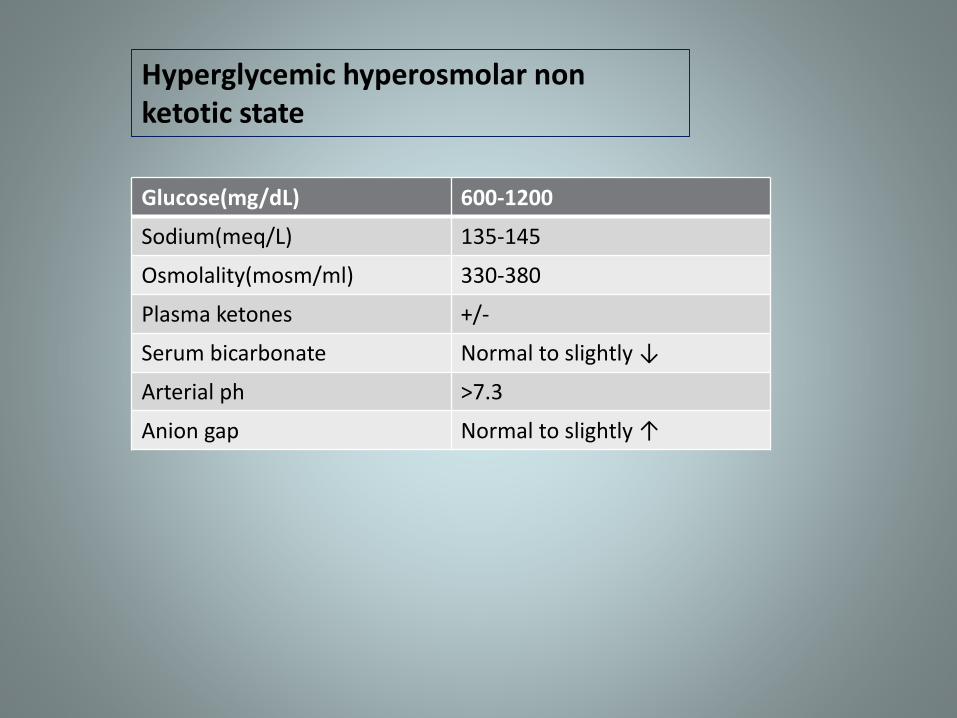
Hyperglycemic hyperosmolar non ketotic state
Glucose(mg/dL) 600-1200
Sodium(meq/L) 135-145
Osmolality(mosm/ml) 330-380
Plasma ketones +/-
Serum bicarbonate Normal to slightly ↓
Arterial ph >7.3
Anion gap Normal to slightly ↑
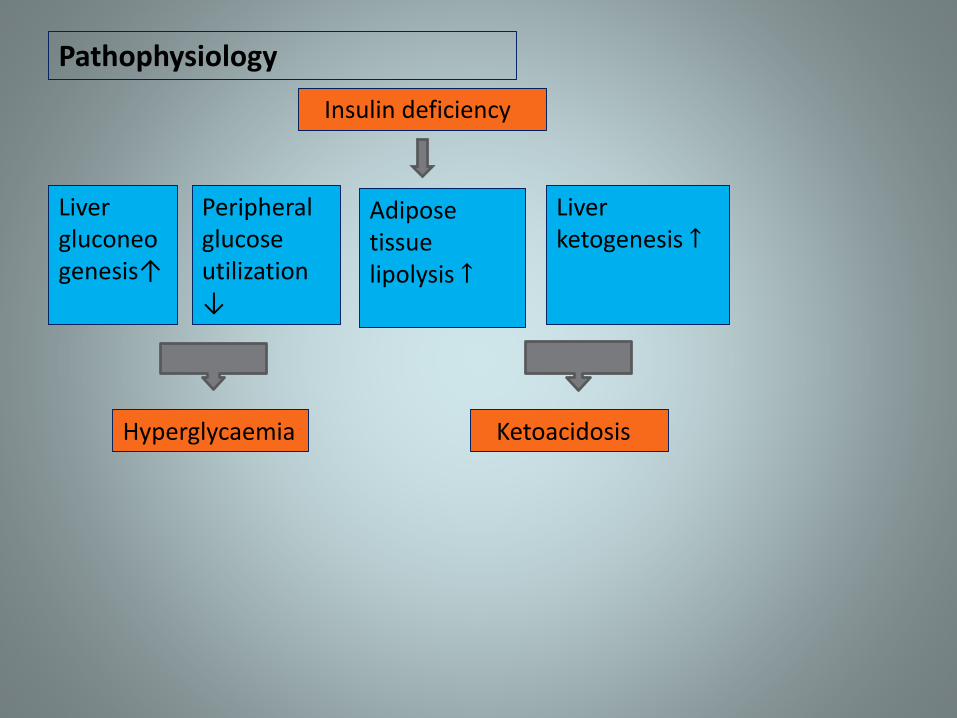
Insulin deficiency
Liver gluconeogenesis↑
Peripheral glucose utilization ↓
Adipose tissue lipolysis ↑
Liver ketogenesis ↑
Hyperglycaemia Ketoacidosis
Pathophysiology
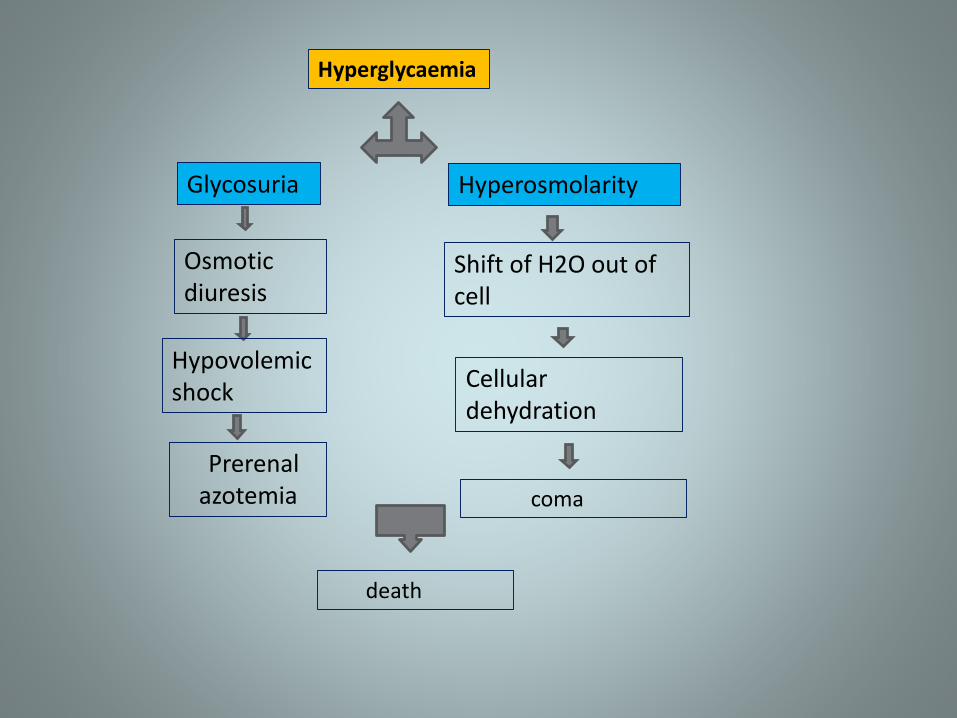
Hyperglycaemia
Glycosuria
Osmotic diuresis
Hypovolemic shock
Prerenalazotemia
Hyperosmolarity
Shift of H2O out of cell
Cellular dehydration
coma
death
Major sign and symptoms of HHNKS
In 50-60% of HHNKS hyperosmolar coma is first sign of diabetes
Dehydration can be manifested by thirst, decreased turgor, soft eyeball and orthostasis
Stupor, coma and convulsions are more common in hhnks than in dka
Vomiting present in 50-60 % of patients(dka) causes further dehydration. may precipitate hyperosmolar state.
Fluid replacement in HHNKS
Estimated H20 deficit 10% of body weightReplace 50% of deficit in first five hours Normal saline if HypotensiveNa<140 meq/l
One half normal saline ifNa>145 meq/lPatient normotensive
Rate total 1st 5 hours 3.5-5L6th to 12th hour 250-500 ml/hr

Lactic acidosis
Laboratory findings
Blood lactic acid rise( 5 mmol/L)
Metabolic acidosis
Elevated anion gap
Hyperuricaemia
Hyperphosphatemia
normokalemia

Management
Hydration
Sodium bicarbonate,dichloroacetate, carbicarb
Forced diuresis or haemodialysis
Insulin & thiamine
Perioperative management
Tight glycemic control with insulin is advocated for a better surgical outcome( target b/w 110-140 mg/dl)
Glucose &insulin should be given through separate iv routes.serum potassium should be monitored and maintained throughout supplementation.
Minor procedures where patients need not remain npo for prolonged periods may continue on oha if they are well controlled.
Patients with acute myocardial infarction
Hyperglycaemia associated with poor clinical outcome in AMI.
Indicator vs mediator controversy
Hyperglycemia and hypoglycemia both should be avoided in patients with AMI to decrease morbidity and mortality
Tight glycaemic control may not contribute towards any increased mortality but it reduces risk of complications associated with MI such as ccf and reinfarction.
Sudden cardiac death in diabetes
Scd in dm could occur in assosciation with
CAD(more than one previous MI)
Ischaemic cardiomyopathy,chronic ccf
Diabetic cardiomyopathy (with or without lvh or severe Cardiovascular autonomic neuropathy)
ventricular ectopics
Heavy smoking

Sudden cardiac death contd…
Scd is more often due to vt/vf and less commonly due to cardiac asystole.
Twenty four hour holter monitoring
Tests of CAN, doppler echocardiography
Thallium scan/ mibg scan
Diabetic with kidney disease
Incidence of hypoglycaemia and brittleness in control of BG increases with progression of diabetic ckd.
Biguanides carry increased risk of toxicity particularly at GFR less than 60ml/min
Reduction in insulin dose
Egfr 45-30 (CKD III) needs 10% reductionin mL/ min 30-15(CKD IV) needs 25% reductionLess than 15 (CKD V) needs 50 % reduction
Haemodialysis patients
Initiation of hd in ESRD patients can lead to hypoglycaemic episodes.
In predialysis stages uraemia had produced insulin resistance, on commencing hd patient becomes insulin sensitive.
Increased insulin half life is seen due to reduced degradation.
Glucose is lost into the dialysate especially if dialysate contains no glucose resulting in hypoglycaemia.
Hypoglycaemia is more common in patients with concomitant liver disease like chronic hepatitis b & c, due to depletion of liver glycogen stores.

Heamodialysis contd….
Frequent BG estimation during arterial dialysis line is desirable to prevent intradialytic hypoglycaemia.
Addition of glucose to dialysate so as to obtain a concentration of 80-100 mg/dl.
Hypoglycaemia rare in continous ambulatory peritoneal dialysis because dialysate contains large quantities of glucose.
Ckd stage IV & V modest glycaemic control is advised.
Patients on glucocorticoid therapy
Regular and sustained monitoring of BG should be done in patients on high dose of glucocorticoid therapy.
Treatment naïve patients developing hyperglycemia after glucocorticoid initiation should be managed with insulin.
For patients already on insulin 20% increment in total daily insulin dose at time of high dose glucocorticoid initiation is a reasonable step.

Patients on enteral nutrition
Glycaemic levels show marked variability with type and duration of enteral nutrition(i.e ryles tube or gastrostomy tube)
Insulin analogs should be preferred to control hyper glycaemia in indoor patients on enteral nutrition
Basal plus multiple SC prandial boluses are to be preferred over SSI
Patients receiving parenteral nutrition
Large amount of glucose in parenteral solutions result in severe hyperglycaemia.
Intravenous insulin is the preferred treatment for control of hyperglycaemia in patients receiving parenteral nutrition.
Glucose targets should be based on severity of underlying illness.
Peripartum control of hyperglycaemia
Placental hormones ,growth factors and cytokines increases insulin resistance during pregnancy and this significantly enhances insulin requirements.
Insulin is the preferred therapy in pregnancy complicated by diabetes
Rapid acting insulin analogs aspart and lispro are preferrred for use in pregnancy. detemir is preferred choice as basal insulin.
Patients in active labour should be on glucose, iv insulin plus potassium infusion to prevent hypokalemia, hypoglycaemia as well as ketosis
Incremental insulin dose is required for pregnant ladies receiving long acting glucocorticoid for fetal maturity.
Critically Ill Patients
Intravenous insulin infusions are the preferred method for achieving and maintaining glycemic control in critically ill patients
Insulin therapy should be initiated for treatment of persistent hyperglycemia, starting at a threshold of no greater than 180 mg/dL .
Once insulin therapy has been started, a glucose range of 140 to 180 mg/dL is recommended for the majority of critically ill patients.
With IV insulin therapy, frequent glucose monitoring is essential to minimize the occurrence of hypoglycemia and to achieve optimal glucose control.
THANK YOU….






![Renal Failure Critically Ill[1]](https://img.dokumen.tips/doc/110x75/577d26df1a28ab4e1ea26f52/renal-failure-critically-ill1.jpg)