Embed Size (px)
Citation preview

8/7/2019 Anemia in Critically Ill Patient1
http://slidepdf.com/reader/full/anemia-in-critically-ill-patient1 1/38
Anaemia in Critically ill Anaemia in Critically ill
patientpatient

8/7/2019 Anemia in Critically Ill Patient1
http://slidepdf.com/reader/full/anemia-in-critically-ill-patient1 2/38
IntroductionIntroduction
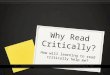
Mean Hb concentration of 11g/dl, with 63% &Mean Hb concentration of 11g/dl, with 63% &29% having a mean Hb of less than 12 and 1029% having a mean Hb of less than 12 and 10respectivelyrespectively
Prevalence of moderate to severe anaemiaPrevalence of moderate to severe anaemia
appears to be 40appears to be 40--50%50% over 90% of patients after 3d in ICU show Hbover 90% of patients after 3d in ICU show Hb
below normal value as compared to 24below normal value as compared to 24--40% in40% innonnon--ICU patientsICU patients
Among non Among non--bleeding ICU pts who did notbleeding ICU pts who did notreceive transfusion, Hb concentrationsreceive transfusion, Hb concentrations by a by amean 0.52g/dmean 0.52g/d

8/7/2019 Anemia in Critically Ill Patient1
http://slidepdf.com/reader/full/anemia-in-critically-ill-patient1 3/38
Figure 1. Course of Hemoglobin (Hb) Patterns by Admitting Hb Level Category Numbers donot total 3534 because of missing data (some forms incomplete).
Vincent, J. L. et al. JAMA 2002;288:1499-1507
Copyright restrictions may apply.

8/7/2019 Anemia in Critically Ill Patient1
http://slidepdf.com/reader/full/anemia-in-critically-ill-patient1 4/38
Classification of anaemiaClassification of anaemia
Decreased RBC productionDecreased RBC production
Lack of nutrients, such as iron, B12, or folate.Lack of nutrients, such as iron, B12, or folate.
Bone marrow disordersBone marrow disorders Bone marrow suppressionBone marrow suppression
Low levels of trophic hormonesLow levels of trophic hormones
The anaemia of chronic disease/inflammation,The anaemia of chronic disease/inflammation,
associated with infectious, inflammatory, or associated with infectious, inflammatory, or
malignant disorders,malignant disorders,

8/7/2019 Anemia in Critically Ill Patient1
http://slidepdf.com/reader/full/anemia-in-critically-ill-patient1 5/38
Increased RBC destructionIncreased RBC destruction ²² HaemolyticHaemolytic
anaemia will ensue when the bone marrow is unable toanaemia will ensue when the bone marrow is unable to
keep up with the need to replace more than about 5keep up with the need to replace more than about 5
percent of the RBC mass per day,percent of the RBC mass per day, Inherited haemolytic anaemiasInherited haemolytic anaemias
Acquired haemolytic anaemias (eg, Coombs' Acquired haemolytic anaemias (eg, Coombs'--
positive autoimmune haemolytic anaemia,positive autoimmune haemolytic anaemia,
thrombotic thrombocytopenic purpurathrombotic thrombocytopenic purpura--haemolytic uremic syndrome, malaria)haemolytic uremic syndrome, malaria)

8/7/2019 Anemia in Critically Ill Patient1
http://slidepdf.com/reader/full/anemia-in-critically-ill-patient1 6/38
Blood lossBlood loss ²² is the most common causeis the most common cause
of anaemia and may take any one of aof anaemia and may take any one of a
number of forms:number of forms: Obvious bleedingObvious bleeding
Occult bleedingOccult bleeding
Induced bleedingInduced bleeding

8/7/2019 Anemia in Critically Ill Patient1
http://slidepdf.com/reader/full/anemia-in-critically-ill-patient1 7/38
Causes of anaemia during criticalCauses of anaemia during critical
illnessillness PrePre--existing anaemiaexisting anaemia
Acquired anaemia Acquired anaemia1.1. HemodilutionHemodilution
2.2. Blood lossBlood loss3.3. Reduced red cell survivalReduced red cell survival
4.4. Reduced red cell productionReduced red cell production
5.5. Abnormal iron metabolism Abnormal iron metabolism
6.6. Nutritional deficienciesNutritional deficiencies7.7. Inappropriate erythropoietin productionInappropriate erythropoietin production
8.8. Abnormal red cell production Abnormal red cell production

8/7/2019 Anemia in Critically Ill Patient1
http://slidepdf.com/reader/full/anemia-in-critically-ill-patient1 8/38
The relation between red cell volume, plasma volume and haemoglobin concentration duringhaemorr hage, healthy euvolaemia, and fluid resuscitation with clear fluids.
Walsh T S , Saleh E Br. J. Anaesth. 2006;97:278-291
© The Board of Management and Trustees of the British Journal of Anaesthesia 2006. All rightsreserved. For Permissions, please e-mail: [email protected]

8/7/2019 Anemia in Critically Ill Patient1
http://slidepdf.com/reader/full/anemia-in-critically-ill-patient1 9/38
BLOOD LOSSBLOOD LOSS
i.i. Frequent blood samplingFrequent blood sampling
�� phlebotomy could account for up to 30% of totalphlebotomy could account for up to 30% of total
blood transfused in ICUblood transfused in ICU
�� ABC study +ve correlation between organ ABC study +ve correlation between organ
dysfunction and no of blood draws and totaldysfunction and no of blood draws and total
volume drawnvolume drawn

8/7/2019 Anemia in Critically Ill Patient1
http://slidepdf.com/reader/full/anemia-in-critically-ill-patient1 10/38
ii. Blood loss at the time of surgicalii. Blood loss at the time of surgical
procedures preceding admission to theprocedures preceding admission to theICUICU
iii. Blood loss due to trauma precedingiii. Blood loss due to trauma precedingadmission to the ICUadmission to the ICU

8/7/2019 Anemia in Critically Ill Patient1
http://slidepdf.com/reader/full/anemia-in-critically-ill-patient1 11/38
iv.iv. Clinically apparent and/or occult blood lossClinically apparent and/or occult blood loss(Stress Ulcer) from GIT(Stress Ulcer) from GIT
Clinically significant bleeding occurred in 1.5% of Clinically significant bleeding occurred in 1.5% of
ICU patientsICU patients
Incidence of overt GI bleeding ~1.5 to 8.5% amongIncidence of overt GI bleeding ~1.5 to 8.5% amongall ICU patients, but may be as high as 15% amongall ICU patients, but may be as high as 15% among
patients who do not receive stress ulcer prophylaxispatients who do not receive stress ulcer prophylaxis
Incidence significantly reduced due to SUIncidence significantly reduced due to SU
prophylaxis and early introduction of enteral feedingprophylaxis and early introduction of enteral feeding

8/7/2019 Anemia in Critically Ill Patient1
http://slidepdf.com/reader/full/anemia-in-critically-ill-patient1 12/38
Stress Ulcer Stress Ulcer
EarlyEarly-- begins in the proximal regions of thebegins in the proximal regions of thestomach within hoursstomach within hours
LateLate-- develop after the first several days of develop after the first several days of hospitalization tend to be deeper and morehospitalization tend to be deeper and moredistaldistal
Risk FactorsRisk Factors Mechanical ventilation for >48hrs (OR 15.6)Mechanical ventilation for >48hrs (OR 15.6)
Coagulopathy (OR 4.3)Coagulopathy (OR 4.3)

8/7/2019 Anemia in Critically Ill Patient1
http://slidepdf.com/reader/full/anemia-in-critically-ill-patient1 13/38
ProphylaxisProphylaxis
Coagulopathy, defined as a platelet countCoagulopathy, defined as a platelet count<50,000/m3, an INR >1.5, or PTT >2 times the<50,000/m3, an INR >1.5, or PTT >2 times thecontrol valuecontrol value
Mechanical ventilation for more than 48 hoursMechanical ventilation for more than 48 hours History of GI ulceration or bleeding with the pastHistory of GI ulceration or bleeding with the past
year year
Two or more of the following risk factorsTwo or more of the following risk factors ²²
sepsis, ICU admission lasting >1 week, occult GI sepsis, ICU admission lasting >1 week, occult GI bleeding lasting �6 days, and glucocorticoidbleeding lasting �6 days, and glucocorticoidtherapytherapy

8/7/2019 Anemia in Critically Ill Patient1
http://slidepdf.com/reader/full/anemia-in-critically-ill-patient1 14/38
What to give??What to give??
H2 blockers versus PPI H2 blockers versus PPI ²² A meta A meta--analysis of sevenanalysis of sevenrandomized trials found a less GI bleeding among thoserandomized trials found a less GI bleeding among thosewho received a PPIwho received a PPI
H2 blockers versus antacidsH2 blockers versus antacids ²² H2 blocker group had aH2 blocker group had asignificantly lower rate of overt GI bleedingsignificantly lower rate of overt GI bleeding
H2 blockers versus sucralfateH2 blockers versus sucralfate ²²H2 blocker decreasedH2 blocker decreasedovert GI bleeding compared to sucralfateovert GI bleeding compared to sucralfate
SucralfateSucralfate versus antacidsversus antacids ²²antacids group had a lower antacids group had a lower rate of clinically important GI bleeding, but the differencerate of clinically important GI bleeding, but the differencewas not statistically significantwas not statistically significant

8/7/2019 Anemia in Critically Ill Patient1
http://slidepdf.com/reader/full/anemia-in-critically-ill-patient1 15/38
Potential harmPotential harm
Studies suggest that agents that increase gastricStudies suggest that agents that increase gastric
pH maypH may the frequency of nosocomialthe frequency of nosocomial
pneumonia compared to agents that do not alter pneumonia compared to agents that do not alter
gastric pH (eg, sucralfate).gastric pH (eg, sucralfate). Randomly assigned 1200 mechanicallyRandomly assigned 1200 mechanically
ventilated patientsventilated patients-- received either an ivreceived either an iv
ranitidine or sucralfateranitidine or sucralfate-- found that VAP wasfound that VAP was
more frequent in the H2 blocker group, althoughmore frequent in the H2 blocker group, although
the difference was not statistically significantthe difference was not statistically significant

8/7/2019 Anemia in Critically Ill Patient1
http://slidepdf.com/reader/full/anemia-in-critically-ill-patient1 16/38
5.5. Reduced red cell survivalReduced red cell survival�� complement activationcomplement activation
�� changes in RBC deformability and membranechanges in RBC deformability and membrane
characteristicscharacteristics
�� Inflammatory mediators (ILInflammatory mediators (IL--1. TNF1. TNF ))
6.6. Reduced red cell productionReduced red cell production
blunting of the erythropoietic responseblunting of the erythropoietic response inhibit RBC production directly by inhibiting boneinhibit RBC production directly by inhibiting bone
marrowmarrow
inhibits differentiation of erythroid progenitor cellsinhibits differentiation of erythroid progenitor cells

8/7/2019 Anemia in Critically Ill Patient1
http://slidepdf.com/reader/full/anemia-in-critically-ill-patient1 17/38
7.7. Iron metabolismIron metabolism
�� acute inflammation decreases the iron available for acute inflammation decreases the iron available for
erythropoiesiserythropoiesis
�� Serum Fe & TIBC ( Serum Fe & TIBC (adequate stores of iron in theadequate stores of iron in thebone marrow which may not be effectively utilizedbone marrow which may not be effectively utilized
i.e. functional Fe def)i.e. functional Fe def)
�� Normal to high serum ferritin concentrationNormal to high serum ferritin concentration
�� no significant increase in circulating reticulocytesno significant increase in circulating reticulocytes�� reticulocyte hb concentration (CHR) and % of reticulocyte hb concentration (CHR) and % of
hypochromic red cells in peripheral bloodhypochromic red cells in peripheral blood

8/7/2019 Anemia in Critically Ill Patient1
http://slidepdf.com/reader/full/anemia-in-critically-ill-patient1 18/38
8.8. B12 and folate metabolismB12 and folate metabolism
�� Rodriguez et al. found evidence in only 2%Rodriguez et al. found evidence in only 2%
of ICU ptsof ICU pts
9.9. Inappropriately low circulatingInappropriately low circulating
erythropoietin levelerythropoietin level
�� from inhibition of the EPO gene byfrom inhibition of the EPO gene byinflammatory cytokinesinflammatory cytokines
10.10. Abnormal red cell maturation Abnormal red cell maturation
Inflammatory cytokines directly inhibit redInflammatory cytokines directly inhibit redcell formation and induce apoptosis of cell formation and induce apoptosis of
erythroid precursor cellserythroid precursor cells

8/7/2019 Anemia in Critically Ill Patient1
http://slidepdf.com/reader/full/anemia-in-critically-ill-patient1 19/38
Schematic diagram showing stages in red blood cell maturation from pluripotential stem cellsand the sites of action of potential inhibitors during critical illness.
Walsh T S , Saleh E Br. J. Anaesth. 2006;97:278-291
© The Board of Management and Trustees of the British Journal of Anaesthesia 2006. All rightsreserved. For Permissions, please e-mail: [email protected]

8/7/2019 Anemia in Critically Ill Patient1
http://slidepdf.com/reader/full/anemia-in-critically-ill-patient1 20/38
InvestigationsInvestigations
FBC/Peripheral blood filmFBC/Peripheral blood film
RBC indices and morphologyRBC indices and morphology
Reticulocyte countReticulocyte count Iron studyIron study
Red cell folate and Vitamin B12 levelRed cell folate and Vitamin B12 level
Bone marrow aspiration and biopsyBone marrow aspiration and biopsy

8/7/2019 Anemia in Critically Ill Patient1
http://slidepdf.com/reader/full/anemia-in-critically-ill-patient1 21/38
Bed side testBed side test-- for occult bloodfor occult blood -- NGNG
aspirate or faecesaspirate or faeces
Upper and lower GI
endoscopyUpper and lower GI
endoscopy Imaging studiesImaging studies

8/7/2019 Anemia in Critically Ill Patient1
http://slidepdf.com/reader/full/anemia-in-critically-ill-patient1 22/38

8/7/2019 Anemia in Critically Ill Patient1
http://slidepdf.com/reader/full/anemia-in-critically-ill-patient1 23/38
Management of anaemia inManagement of anaemia in
critically ill patientscritically ill patients

8/7/2019 Anemia in Critically Ill Patient1
http://slidepdf.com/reader/full/anemia-in-critically-ill-patient1 24/38
Iron Therapy Iron Therapy
Final decision will depend ultimately on theFinal decision will depend ultimately on theaetiology of anaemia in the critically illaetiology of anaemia in the critically illpatient.patient.
IDA is noted in a small subset of criticallyIDA is noted in a small subset of criticallyill patients and iron supplementation of ill patients and iron supplementation of such patients is appropriate.such patients is appropriate.
If anaemia is multifactorialIf anaemia is multifactorial -- may be usefulmay be useful
as an adjunct with erythropoietin.as an adjunct with erythropoietin. Specific populations of ICU patients maySpecific populations of ICU patients may
not benefit from iron therapynot benefit from iron therapy

8/7/2019 Anemia in Critically Ill Patient1
http://slidepdf.com/reader/full/anemia-in-critically-ill-patient1 25/38
Microbe require iron for growthMicrobe require iron for growth
High ferritinHigh ferritin-- binds to Fe making it lessbinds to Fe making it less
available for bacteriaavailable for bacteria Antibacterial effect of cytokines such as Antibacterial effect of cytokines such as
Interferon, TNF, IL is mediated byInterferon, TNF, IL is mediated by
intracellular depletion of ironintracellular depletion of iron

8/7/2019 Anemia in Critically Ill Patient1
http://slidepdf.com/reader/full/anemia-in-critically-ill-patient1 26/38
Oral formOral form
Ferrous sulphate/gluconate/fumarateFerrous sulphate/gluconate/fumarate
P arental formP arental form
Iron dextran/gluconate/sucroseIron dextran/gluconate/sucrose
Adverse effectAdverse effect
GI irritationGI irritation
Interferes with absorption of other drugs likeInterferes with absorption of other drugs like
phenytoin/tetracyclinephenytoin/tetracycline
Anaphylaxis with iron dextran Anaphylaxis with iron dextran

8/7/2019 Anemia in Critically Ill Patient1
http://slidepdf.com/reader/full/anemia-in-critically-ill-patient1 27/38
Blood transfusionBlood transfusion
At what plasma Hb do the risk of At what plasma Hb do the risk of
anaemia outweighs the potential risk of anaemia outweighs the potential risk of
transfusion in critically ill patients?????transfusion in critically ill patients?????

8/7/2019 Anemia in Critically Ill Patient1
http://slidepdf.com/reader/full/anemia-in-critically-ill-patient1 28/38
At 1982 At 1982-- Allen and colleagues suggested Allen and colleagues suggested
10/30 rule as a clinically useful transfusion10/30 rule as a clinically useful transfusion
trigger trigger-- Never been supported by RCTsNever been supported by RCTs
cost and availability of blood productscost and availability of blood products
along with risk a/w transfusionalong with risk a/w transfusion-- reasons toreasons to
reconsider the trigger for transfusionreconsider the trigger for transfusion

8/7/2019 Anemia in Critically Ill Patient1
http://slidepdf.com/reader/full/anemia-in-critically-ill-patient1 29/38
TRICC trialTRICC trial--
838 pts randomly assigned to liberal transfusion838 pts randomly assigned to liberal transfusiongroup or a restrictive groupgroup or a restrictive group
Restrictive transfusion strategy is at least as effectiveRestrictive transfusion strategy is at least as effective
as and possibly superior to liberal strategyas and possibly superior to liberal strategy
Among pts aged <55yrs, and admission APACHE II Among pts aged <55yrs, and admission APACHE II <20, statistically significantly better 30d mortality<20, statistically significantly better 30d mortality
among pts in restrictive groupamong pts in restrictive group
ABC trial ABC trial
Both ICU and overall mortality were significantlyBoth ICU and overall mortality were significantlyhigher in pts who had vs had not received ahigher in pts who had vs had not received a
transfusiontransfusion

8/7/2019 Anemia in Critically Ill Patient1
http://slidepdf.com/reader/full/anemia-in-critically-ill-patient1 30/38
Complications of blood transfusionComplications of blood transfusion
Immediate reactionsImmediate reactions Febrile nonFebrile non--haemolytic reactionshaemolytic reactions
Allergic reactions Allergic reactions-- mild urticaria to anaphylaxismild urticaria to anaphylaxis
Acute haemolytic reaction Acute haemolytic reaction
Volume overloadVolume overload-- FFP more prone because it isFFP more prone because it isinfusion volume and it being hyper infusion volume and it being hyper--oncoticoncotic
Bacterial contaminationBacterial contamination
HypothermiaHypothermia
CoagulopathyCoagulopathy Citrate toxicityCitrate toxicity-- metabolic alkalosismetabolic alkalosis
plasma calcium and magnesiumplasma calcium and magnesium

8/7/2019 Anemia in Critically Ill Patient1
http://slidepdf.com/reader/full/anemia-in-critically-ill-patient1 31/38
TRALITRALI
DefinitionDefinition-- hypoxia and pulmonary oedema occurringhypoxia and pulmonary oedema occurring
during or within 6 hours of a transfusion in the absenceduring or within 6 hours of a transfusion in the absence
of CCF or volume overloadof CCF or volume overload
diagnosis of TRALI
relies on the exclusion of cardiogenicdiagnosis of TRALI
relies on the exclusion of cardiogenicpulmonary oedema, volume overload and sepsispulmonary oedema, volume overload and sepsis
PathogenesisPathogenesis
controversialcontroversial
thought to occur secondary to lipids and cytokines in thethought to occur secondary to lipids and cytokines in the
transfused product or from interaction between patient white celltransfused product or from interaction between patient white cellantigens and donor antibodies (or vice versa).antigens and donor antibodies (or vice versa).

8/7/2019 Anemia in Critically Ill Patient1
http://slidepdf.com/reader/full/anemia-in-critically-ill-patient1 32/38
Risk factorsRisk factors
emergency cardiac surgeryemergency cardiac surgery hematologic malignancyhematologic malignancy
massive transfusionmassive transfusion
sepsissepsis
mechanical ventilation, andmechanical ventilation, and
high APACHE II scorehigh APACHE II score
9090--day survival of ICU patients developingday survival of ICU patients developingTRALI in this study was only 53 percent.TRALI in this study was only 53 percent.

8/7/2019 Anemia in Critically Ill Patient1
http://slidepdf.com/reader/full/anemia-in-critically-ill-patient1 33/38
TreatmentTreatment
supportive and ventilation is required insupportive and ventilation is required in
most patientsmost patients
most do well with an associated mortalitymost do well with an associated mortalityof 5of 5--10%10%
use of leucoreduced blood componentsuse of leucoreduced blood components
and fresher blood/blood components mayand fresher blood/blood components may
also have a benefitalso have a benefit

8/7/2019 Anemia in Critically Ill Patient1
http://slidepdf.com/reader/full/anemia-in-critically-ill-patient1 34/38
Delayed reactionsDelayed reactions
Delayed HaemolysisDelayed Haemolysis
AlloimmunisationAlloimmunisation
Transfusion associated Graft VersusTransfusion associated Graft Versus--Host Disease (TaHost Disease (Ta--GVHD)GVHD)
occurs when donor lymphocytes in cellular blood products engraft in aoccurs when donor lymphocytes in cellular blood products engraft in asusceptible transfusion recipient, which proliferate and damage target organssusceptible transfusion recipient, which proliferate and damage target organsespecially bone marrow, skin, liver and gastrointestinal tract.especially bone marrow, skin, liver and gastrointestinal tract.
Iron accumulationIron accumulation Predictable consequence of chronic RBCPredictable consequence of chronic RBC
Patients receiving chronic transfusion usually have their iron status monitoredPatients receiving chronic transfusion usually have their iron status monitoredand managed by their physician.and managed by their physician.
Infectious Disease transmissionInfectious Disease transmission Definitive evidence of transmission by transfusion requires demonstration of Definitive evidence of transmission by transfusion requires demonstration of
seroconversion or new infection in the recipient.seroconversion or new infection in the recipient.
Suspected transfusionSuspected transfusion--transmitted bacterial or parasitic infection (malaria) shouldtransmitted bacterial or parasitic infection (malaria) shouldbe reported urgently in order to recall other potentially infectious blood productsbe reported urgently in order to recall other potentially infectious blood productsfrom the same donation.from the same donation.

8/7/2019 Anemia in Critically Ill Patient1
http://slidepdf.com/reader/full/anemia-in-critically-ill-patient1 35/38
Transfusion relatedTransfusion related
Immunomodulation (TRIM)Immunomodulation (TRIM) first demonstrated in the renal transplant setting, when significantlyfirst demonstrated in the renal transplant setting, when significantly
improved renal allograft survival after transplant was seen inimproved renal allograft survival after transplant was seen in
patients who had received transfusion before transplantpatients who had received transfusion before transplant
PathogenesisPathogenesis transfused allogeneic WBCs are responsible for the majority of transfused allogeneic WBCs are responsible for the majority of
TRIM effects.TRIM effects.
impaired natural killer cell function, decreased macrophageimpaired natural killer cell function, decreased macrophage
phagocytic function, suppression of lymphocyte production andphagocytic function, suppression of lymphocyte production and
ineffective antigen presentation.ineffective antigen presentation.
Clinical effects of TRIMClinical effects of TRIM-- risk of cancer recurrence, postoperativerisk of cancer recurrence, postoperative
infection and shortinfection and short--term mortalityterm mortality

8/7/2019 Anemia in Critically Ill Patient1
http://slidepdf.com/reader/full/anemia-in-critically-ill-patient1 36/38
Other risks associated with bloodOther risks associated with blood
transfusiontransfusion
prolong storage may ability to improveprolong storage may ability to improve
oxygenationoxygenation
in animal models blood stored >28d didn¶tin animal models blood stored >28d didn¶t
improve O2 consumption as compared with thatimprove O2 consumption as compared with thatstored <3daysstored <3days
In a trauma registry of 16,824 pts, transfusion of In a trauma registry of 16,824 pts, transfusion of
old blood (storage>15d) was independentold blood (storage>15d) was independent
predictor of mortality, ICU admission/length of predictor of mortality, ICU admission/length of
stay and hospital length of staystay and hospital length of stay

8/7/2019 Anemia in Critically Ill Patient1
http://slidepdf.com/reader/full/anemia-in-critically-ill-patient1 37/38
what happens during prolongwhat happens during prolong
storage??storage??
RBC lose 2,3 DPG stores and ATPRBC lose 2,3 DPG stores and ATP
diminished cellular deformability,diminished cellular deformability,
cytoskeleton oxidation and impairedcytoskeleton oxidation and impaired
oxygen off oxygen off--loadingloading

8/7/2019 Anemia in Critically Ill Patient1
http://slidepdf.com/reader/full/anemia-in-critically-ill-patient1 38/38
Erythropoietin therapyErythropoietin therapy
RCT of 1302 pts from 65 ICUsRCT of 1302 pts from 65 ICUs
EpoetinEpoetin group when compared with placebogroup when compared with placebogroupgroup
had a greater mean increase in Hbhad a greater mean increase in Hb fewer median red blood cell units administered/ptfewer median red blood cell units administered/pt
a 19% reduction in total no of RBC unitsa 19% reduction in total no of RBC unitstransfusedtransfused
no statistical difference in secondary outcomesno statistical difference in secondary outcomes(ventilation free days, start of mechanical(ventilation free days, start of mechanicalventilation, ICU readmission, ICU length of stay or ventilation, ICU readmission, ICU length of stay or mortality)mortality)







![[PPT]PEMERIKSAAN LABORATORIUM PADA ANEMIA … · Web viewPEMERIKSAAN LABORATORIUM PADA ANEMIA HEMOLITIK ELLYZA NASRUL Anemia hemolitik - Klasifikasi anemia berdasarkan morfologi anemia](https://img.dokumen.tips/doc/110x75/5c85338309d3f279718c7183/pptpemeriksaan-laboratorium-pada-anemia-web-viewpemeriksaan-laboratorium-pada.jpg)