Embed Size (px)
Citation preview

Characteristics and Effectiveness of Fall
Prevention Programs in Nursing
Homes:
A Systematic Review and Meta-
Analysis of
Randomized Controlled Trials
J Am Geriatr Soc 2015; 63:211–221
Falls are an important problem in
RACFs >50% NH residents fall >once a year
Annual hip# rate 4%
12% incur a new fracture within 1 year
after a fall-related hip fracture, and
31% die as a result
Associated with fear and poor QoL

Falls prevention programs*
Single programs – single intervention directed at all residents
Multiple programs – more than one intervention provided to all residents
Multifactorial – more than one intervention targeted to individual risk profile
*Prevention of Falls Network Europe (ProFaNE)

Rationale for the present
review No conclusive evidence on
effectiveness of falls prevention
interventions in RACFs, except
vitamin D supplementation
Heterogeneity
Did not differentiate fallers vs.
recurrent fallers
Vague terminology to define the care
settings
Inclusion criteria
Conducted in a nursing home:“a residential facility that provides 24-hour-a-day
surveillance, personal care, and limited clinical
care for persons who are typically elderly and
infirm”
RCT/ cluster randomised RCT
Duration ≥ 6 months
Single, multiple or multifactorial
programs
Outcome measures: falls, fallers
and recurrent fallers number of falls
◦ RR= number of falls per resident year in
the intervention group/ number of falls per
resident year in the control group
number of fallers and recurrent fallers
◦ RR = proportion of (recurrent) fallers in
intervention group /proportion in control
group

Study Characteristics
13 studies
7 in Europe, 4 in the US, 2 in Australia/NZ
11 were cluster RCTs
22,915 patients (mean age 82-88 yrs)
Follow up 6- 17 months
Intervention type
◦ 6 single
◦ 1 multiple
◦ 6 multifactorial

Positive studies Pooled analysis Components of
intervention
No of Falls 2/12 multifactorial
36-45%
*one study effect
only significant in
cognitively
impaired
residents
10 studies
RR = 0.93, 95%
CI = 0.76–1.13
No effect
Group/ individual
exercise
Medication RV
Hip protectors
Mobility+envior
Ax
Staff training
No of fallers 2/7 multifactorial
25-30%
7 studies
RR = 0.97, 95%
CI = 0.84–1.11
No effect
As above
No of recurrent
fallers
1/4 multifactorial
44%
4 studies
RR = 0.79,
95% CI = 0.65–
0.97
21% reduction in
recurrent fallers
Group exercise
Medication RV
Mobility+envior
Ax Staff training
Pt education
Podiatry
Results

Intervention (number
of studies)
Pooled analysis Effect
Single
Intervention
Staff training &
education (2)
RR = 1.29
95% CI = 1.23–
1.36
more falls in the
intervention
group
Medication
reconciliation (2)
RR= 1.20
95% CI = 0.89–
1.61
trend towards
falls in interven
grp
Vitamin D suppl (1) No effect
Exercise program (1) No effect
Multiple
interventions
Low intensity
exercise+ continence
care (1)
No effect
Multifactorial
interventions
Exercise, Medication,
Orthostatic HypoT,
Environment, Hip
protectors, Vision,
Footwear; and goal
setting, reminders,
and feedback (6)
RR = 0.67,
95% CI = 0.55–
0.82
No of falls by
33%
RR = 0.79
95% CI = 0.65–
0.97
Recurrent
fallers by 21%
Results

Conclusions
Falls are multifactorial; therefore it’s
not surprising that single interventions
failed to show a beneficial effect
Single interventions can even be
harmful in RACF setting
Customized, multifactorial
interventions delivered by MDTs
reduce falls in RACFs

Are the interventions effective in
residents with dementia? There were fewer fallers in intervention
groups that had a greater prevalence of dementia
Each one-point increase in dementia prevalence category corresponded to a RR that was only 0.76 of its former size
No significant associations with dementia prevalence score were found for number of falls (RR = 0.95, 95% CI = 0.72–1.25) or number of recurrent fallers (RR = 1.42, 95% CI = 0.49–4.11).
What should be the composition
of a multifactorial intervention? Small number of studies did not allow
additional moderator analyses to
evaluate which
components/combinations of the
intervention programs were most
effective.

Limitations
Poor methodological quality of studies:
blinding difficult, loss of FU
Small number of studies eligible
“nursing home” definition is far from
satisfactory
Inconsistencies/ vague definitions in
reporting falls related outcomes
Some studies had FU <12 months
Cochrane Database Systematic
Review 2012 1. No evidence overall that exercise reduces falls in care
facilities, but may be more effective in less frail
residents. Of the exercise types, only balance training
using mechanical apparatus in intermediate level care
facilities was effective.
2. Results relating to medication review by pharmacists
are equivocal.
3. The prescription of vitamin D in care facilities is
effective in reducing falls.
4. There is currently no evidence of effect from
interventions targeting staff and the organisation of
care.
5. Some falls prevention programmes that target multiple
individual risk factors (classified as multifactorial
interventions) may be effective.
Cameron et al. Interventions for preventing falls in older people in care facilities and hospitals.
Cochrane Database of Systematic Reviews 2012, Issue 12. Art. No.: CD005465. DOI:10.1002/14651858.CD005465.pub3.
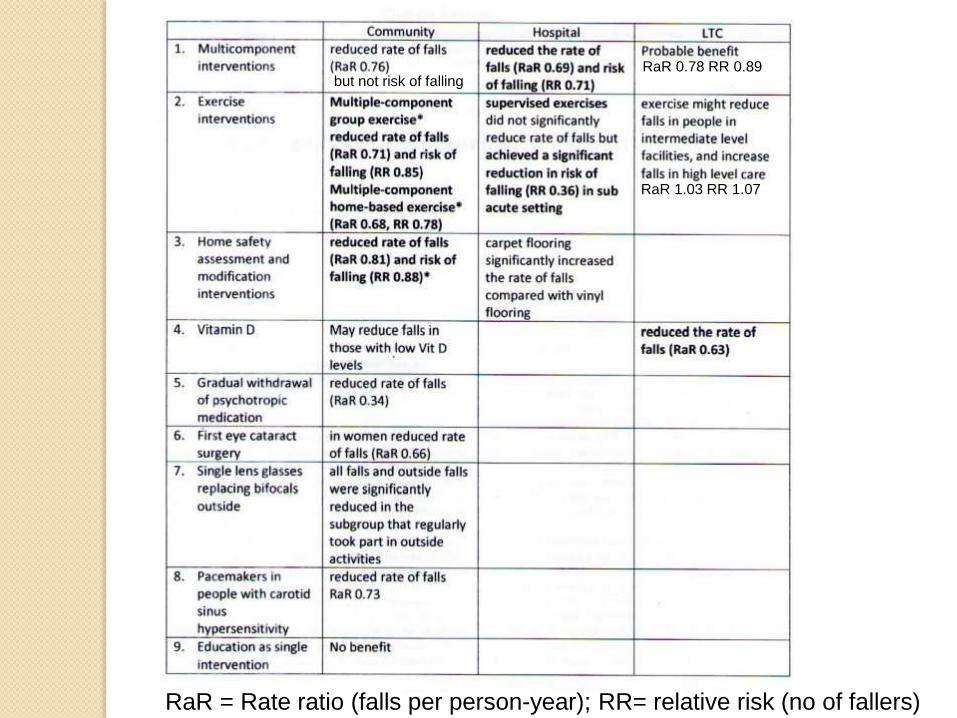
RaR = Rate ratio (falls per person-year); RR= relative risk (no of fallers)
RaR 0.78 RR 0.89
RaR 1.03 RR 1.07
but not risk of falling





























