Embed Size (px)
Citation preview

Thyroid Ultrasound
for Thyroidologists
Durr-e-Sabih

...Ultrasound allows surgeons and
endocrinologists to better follow nodules, identify
tumors, make decisions about surgery on the
contralateral lobe, map metastatic disease and
recurrence and better follow patients with treated
malignancy. Ultrasound improves our selectivity
of patients eligible for surgery because of
improvements in sensitivity and specificity of
ultrasound guided fine needle aspiration biopsy…
Summary of proceedings of the second world congress on Thyroid Cancer.
July 2013. Canada
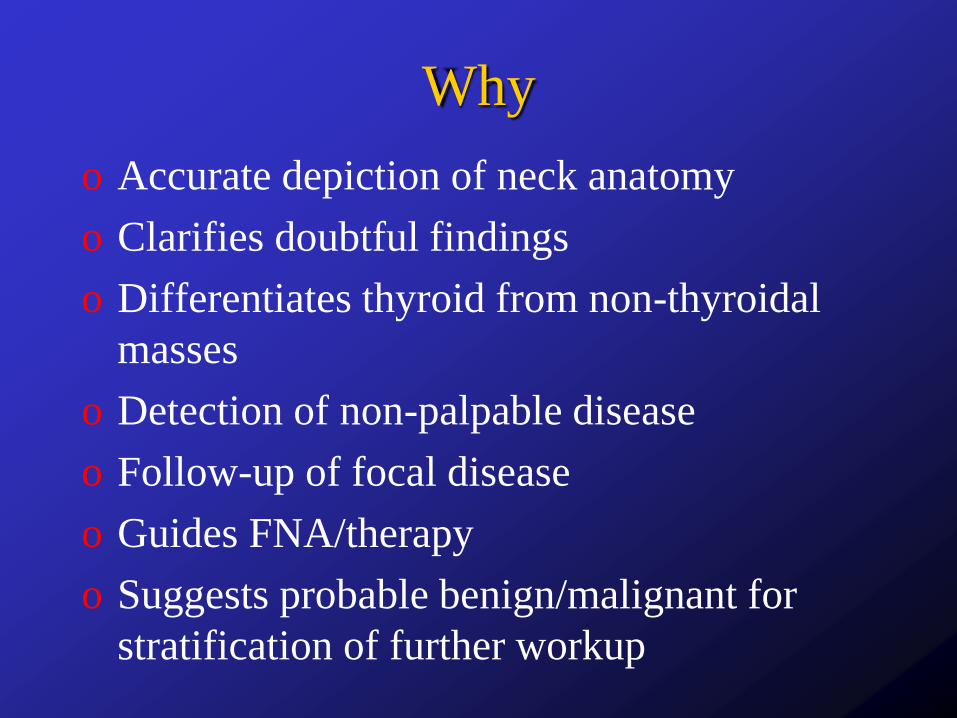
Why
o Accurate depiction of neck anatomy
o Clarifies doubtful findings
o Differentiates thyroid from non-thyroidal
masses
o Detection of non-palpable disease
o Follow-up of focal disease
o Guides FNA/therapy
o Suggests probable benign/malignant for
stratification of further workup

The section
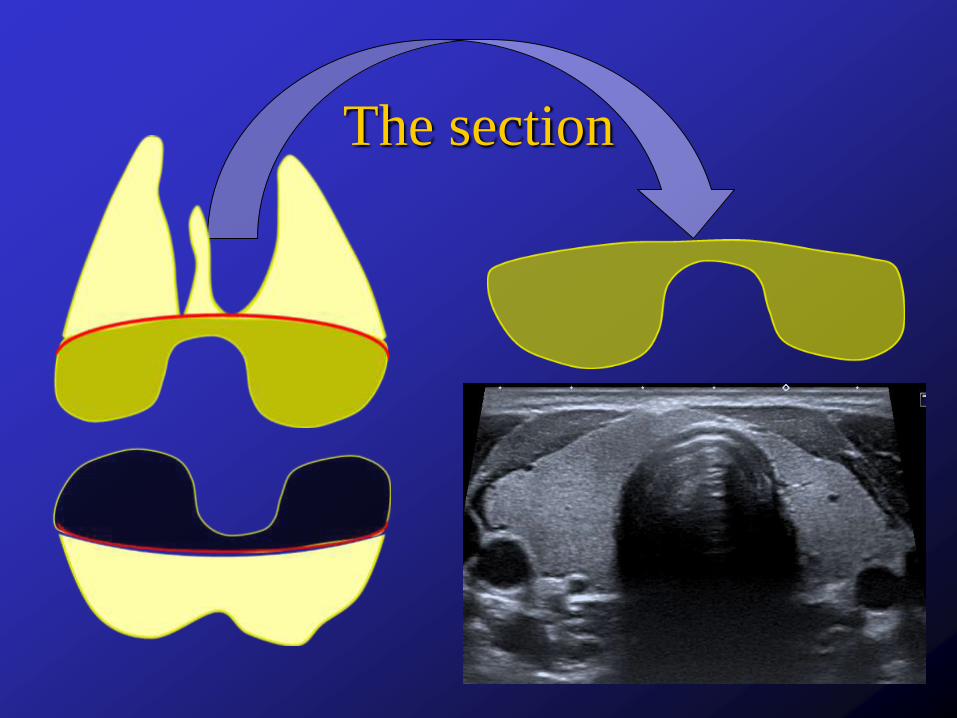
The section

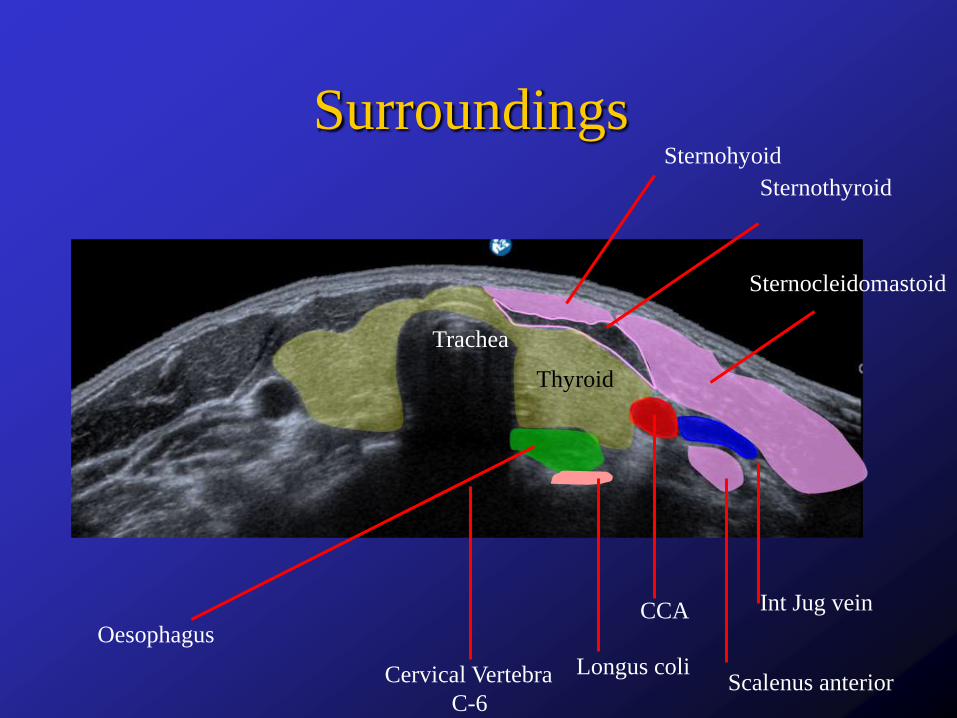
Surroundings
ThyroidTrachea
Oesophagus
Cervical Vertebra
C-6
CCA
Int Jug vein
Sternocleidomastoid
Sternohyoid
Sternothyroid
Longus coli
Scalenus anterior

Surroundings
Surroundings
Thyroid
Trachea
Oesophagus
Cervical Vertebra
C-6
CCA Int Jug vein
Sternocleidomastoid
Sternohyoid
Sternothyroid
Longus coliScalenus anterior

Size
o Each lobe 4-6 cm in cranio-caudal extent
o <1.8 cm in maximum depth, isthmus <6mm
in thickness
o Volume 7-14ml, calculated for each lobe
and add
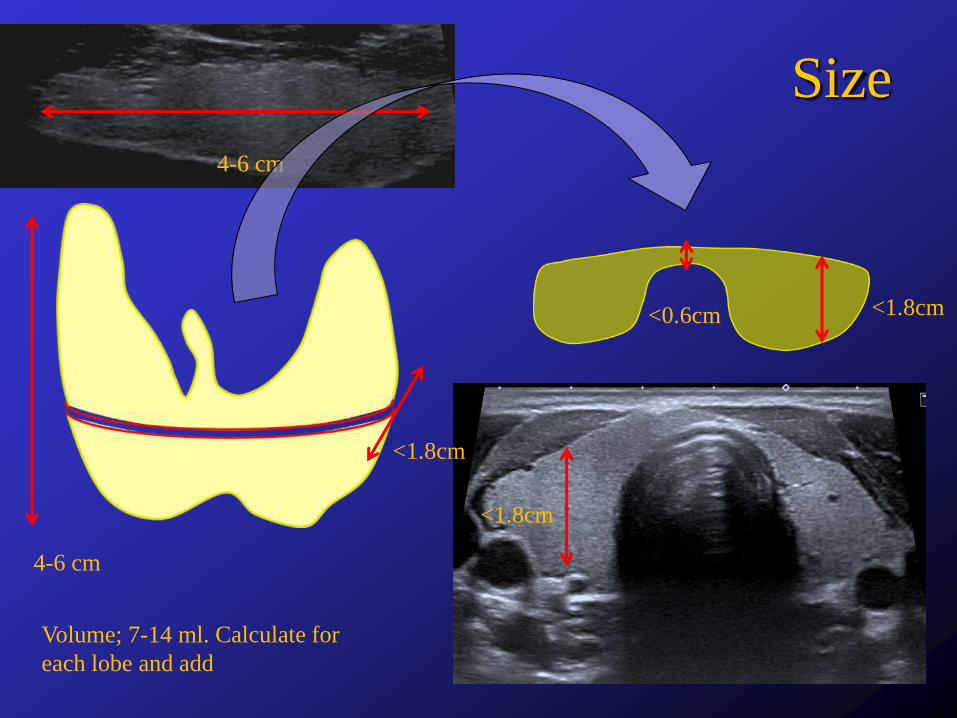
4-6 cm
<1.8cm
<1.8cm
<1.8cm
<0.6cm
Size
4-6 cm
Volume; 7-14 ml. Calculate for
each lobe and add
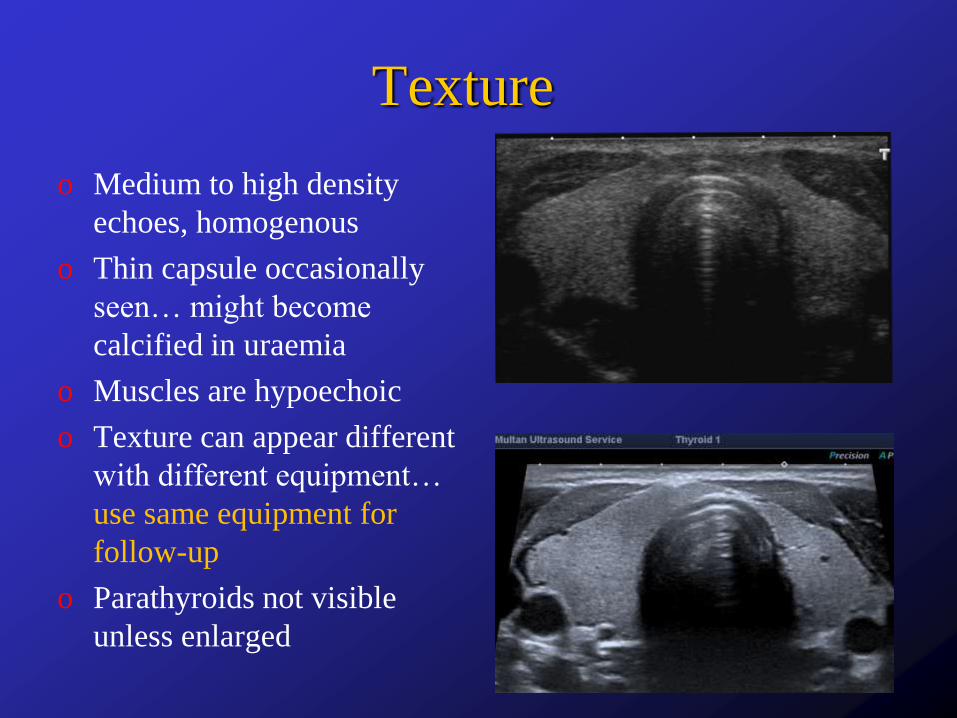
Texture
o Medium to high density
echoes, homogenous
o Thin capsule occasionally
seen… might become
calcified in uraemia
o Muscles are hypoechoic
o Texture can appear different
with different equipment…
use same equipment for
follow-up
o Parathyroids not visible
unless enlarged
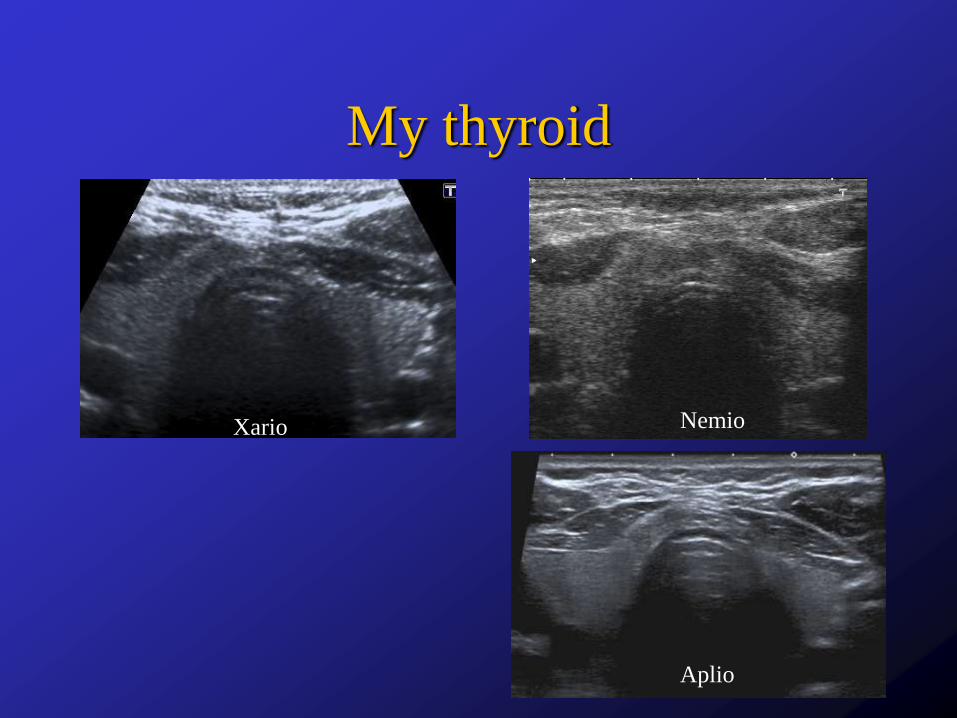
My thyroid
Xario
Aplio
Nemio

Blood supply
o Superior thyroid artery and vein at the upper
pole of each lobe
o Inferior thyroid vein at the lower pole
o Inferior thyroid artery is posterior to the
lower third of each lobe

Superior thyroid artery
Inferior thyroid artery
Inferior thyroid vein
Sup th.
vein
Mid
th.
vein
Inf th.
vein
Int jug
vein
Thyroida
ima
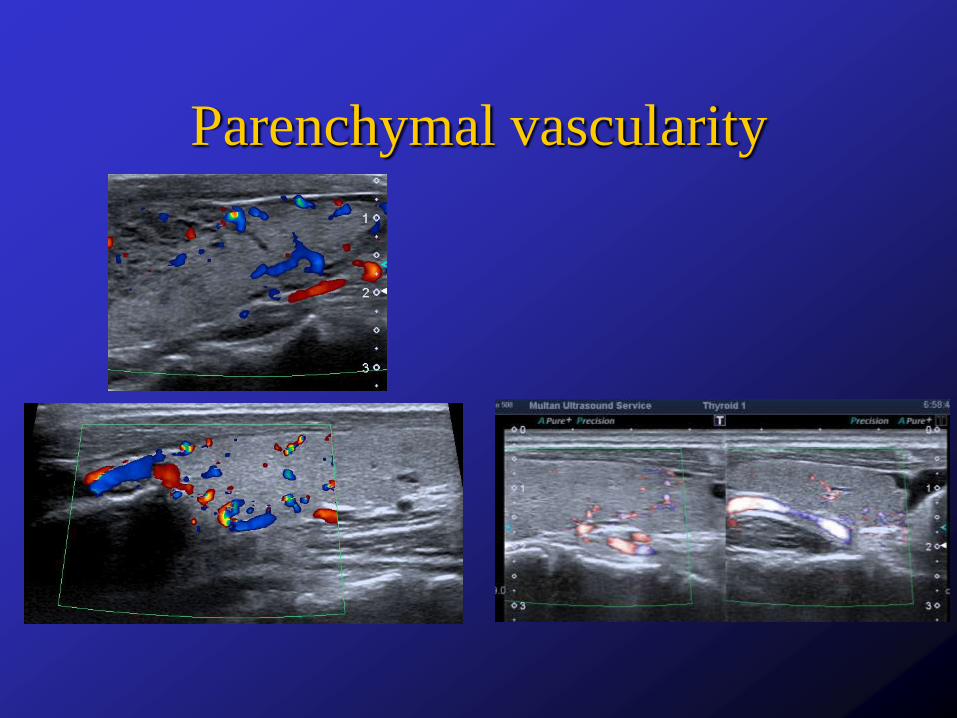
Parenchymal vascularity
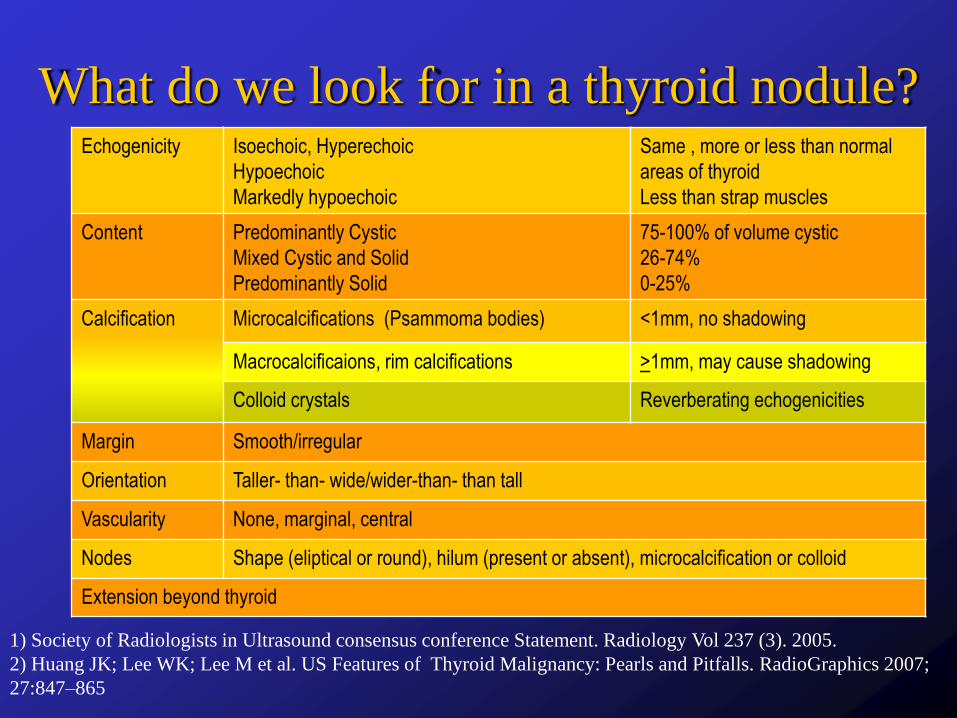
What do we look for in a thyroid nodule?Echogenicity Isoechoic, Hyperechoic
Hypoechoic
Markedly hypoechoic
Same , more or less than normal
areas of thyroid
Less than strap muscles
Content Predominantly Cystic
Mixed Cystic and Solid
Predominantly Solid
75-100% of volume cystic
26-74%
0-25%
Calcification Microcalcifications (Psammoma bodies) <1mm, no shadowing
Macrocalcificaions, rim calcifications >1mm, may cause shadowing
Colloid crystals Reverberating echogenicities
Margin Smooth/irregular
Orientation Taller- than- wide/wider-than- than tall
Vascularity None, marginal, central
Nodes Shape (eliptical or round), hilum (present or absent), microcalcification or colloid
Extension beyond thyroid
1) Society of Radiologists in Ultrasound consensus conference Statement. Radiology Vol 237 (3). 2005.
2) Huang JK; Lee WK; Lee M et al. US Features of Thyroid Malignancy: Pearls and Pitfalls. RadioGraphics 2007;
27:847–865

Features Feature Benign Malignant
Tall/Wide Wider than tall +++ ++
Taller than wide + ++++
Contents Purely cystic ++++ +
Cystic with thin septa +++ +
Mixed Solid/cystic +++ ++
Purely solid +++ ++
Comet tail reverberations +++ +
Echogenicity Hyperechoic ++++ +
Isoechoic +++ ++
Hypoechoic +++ +++
Markedly hypoechoic + ++++
Halo Thin ++++ ++
Thick + +++
Absent + +++
Margins Well defined +++ ++
Poorly defined ++ +++
Spiculated + ++++
Calcification Eggshell +++ ++
Coarse +++ +
Micro ++ ++++
Doppler Peripheral +++ ++
Internal flow ++ +++
Thyroid nodules

Thyroid Nodules
o Is it in the thyroid or outside it?
Hyperplastic, Adenomatous or
Colloid Nodule
o Cellular hyperplasia, microndule nodule,
macronodule formation
o Liquefactive degeneration with
accumulation of serous fluid, blood and
colloid material
o Calcification, often coarse and peripheral
o Can be hypo functioning, normally
functioning or hyperfunctioning

Colloid cyst and Nodule,
Haemorrhagic cyst
© Dr. Ravi Kadasne. UAE
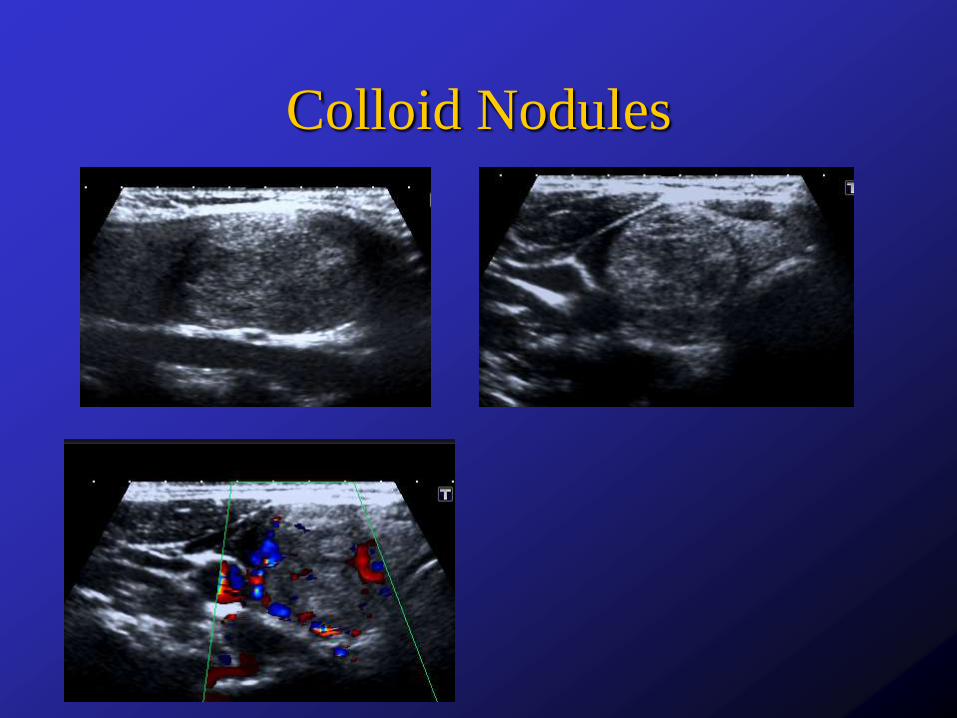
Colloid Nodules
Follicular Neoplasm
o Follicular adenoma is a true neoplasm with
compression of adjacent tissue and fibrous
capsulation
o Capsular/vascular invasion is the hallmark
of follicular carcinoma, that can be seen on
histology and not cytology

Follicular Neoplasm
o FNA does not differentiate between benign
follicular adenoma and carcinoma (capsular
and vascular invasion)
o Usually solid
o Hypo, iso or hyperechoic
o Thin or thick halo
o Peripheral rim of vessels, sometimes extending
inwards in spoke-wheel pattern
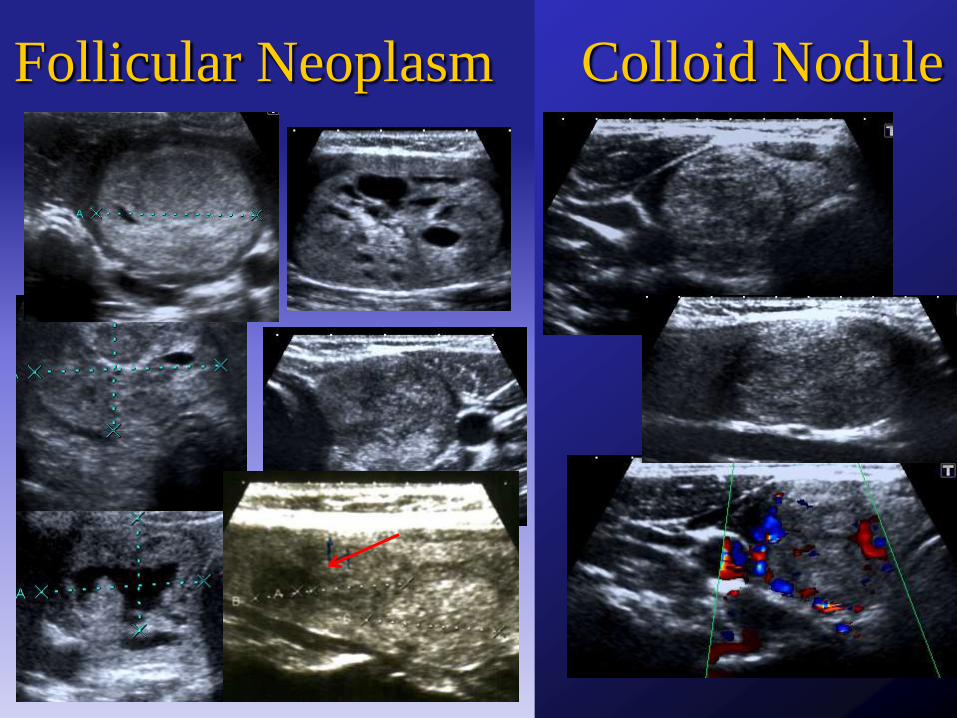
Follicular Neoplasm Colloid Nodule

Papillary Thyroid Cancer
o Hypoechoic
o Microcalcification
o Hypervascular
o Cervical nodes with possible
microcalcification or cystic degeneration

Papillary Carcinoma with Nodes
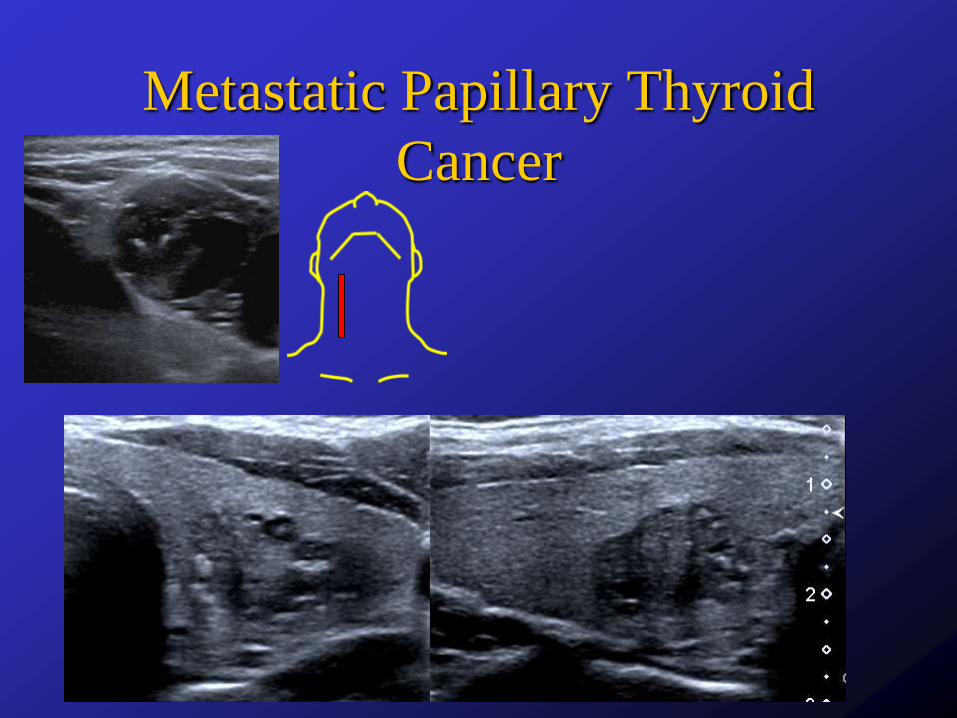
Metastatic Papillary Thyroid
Cancer

Papillary Carcinoma
Follicular Thyroid Carcinoma
o Similar to follicular neoplasm on ultrasound
o Difficult to differentiate from follicular
neoplasm on cytology… so many advocate
surgical removal of all follicular neoplasms
o Some may have very irregular margins,
thick irregular halos and chaotic internal
vascularity
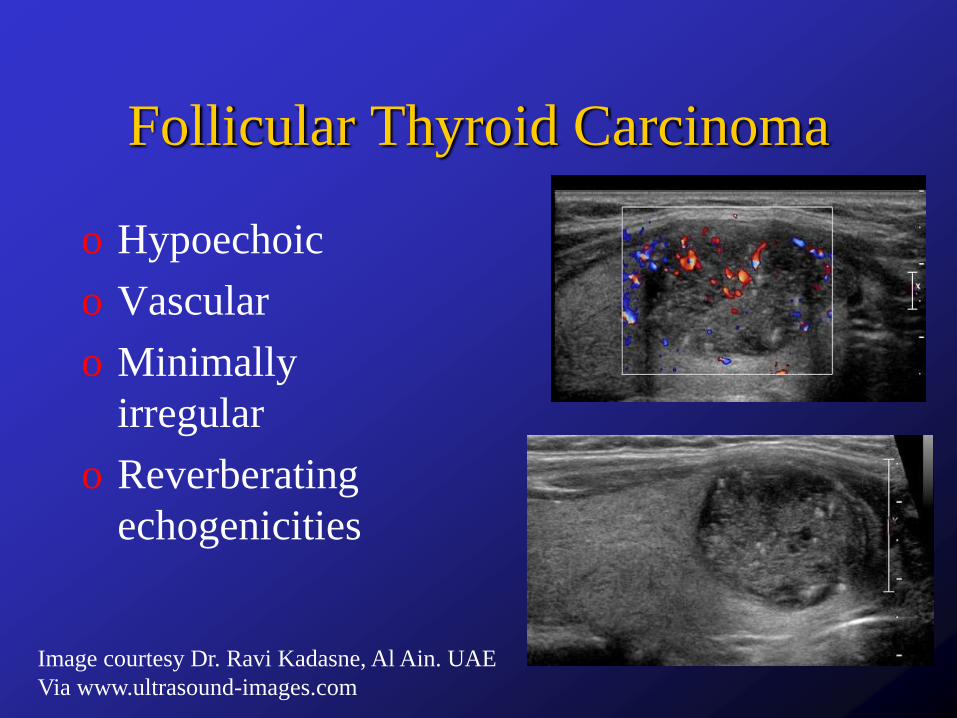
Follicular Thyroid Carcinoma
o Hypoechoic
o Vascular
o Minimally
irregular
o Reverberating
echogenicities
Image courtesy Dr. Ravi Kadasne, Al Ain. UAE
Via www.ultrasound-images.com
Other Carcinomaso Medullary
o Part of the MEN-II syndrome, tends to be multicentric or
bilateral
o Similar to papillary carcinoma on ultrasound
o Calcifications tend to be coarse
o Anaplastic
o Large, hypoechoic, encase or invade blood vessels and muscles
o Lymphoma
o In most there is pre-existing Hashimoto’s and hypothyroidism,
rapidly growing mass
o Extremely hypoechoic, lobulated, areas of cystic necrosis

How specific is ultrasound?
o Ji-Zhen Zhang, Bing Hu. Sonographic features of
thyroid follicular carcinoma in comparison with
thyroid follicular adenoma. J Ultrasound Med
2014; 33:221-227
o Ji Hyun Lee, Jung Hee Shin et al. Sonographic and
cytopathologic correlation of papillary carcinoma
variants. J Ultrasound Med 2015; 34:1-15
How specific is ultrasound?
o Ji-Zhen Zhang, Bing Hu. Sonographic features of
thyroid follicular carcinoma in comparison with
Thyroid follicular adenoma. J Ultrasound Med
2014; 33:221-227
o Ji Hyun Lee, Jung Hee Shin et al. Sonographic
and cytopathologic correlation of papillary
carcinoma variants. J Ultrasound Med 2015; 34:1-
15
Features, Scores and Patterns…
Organizing the Data
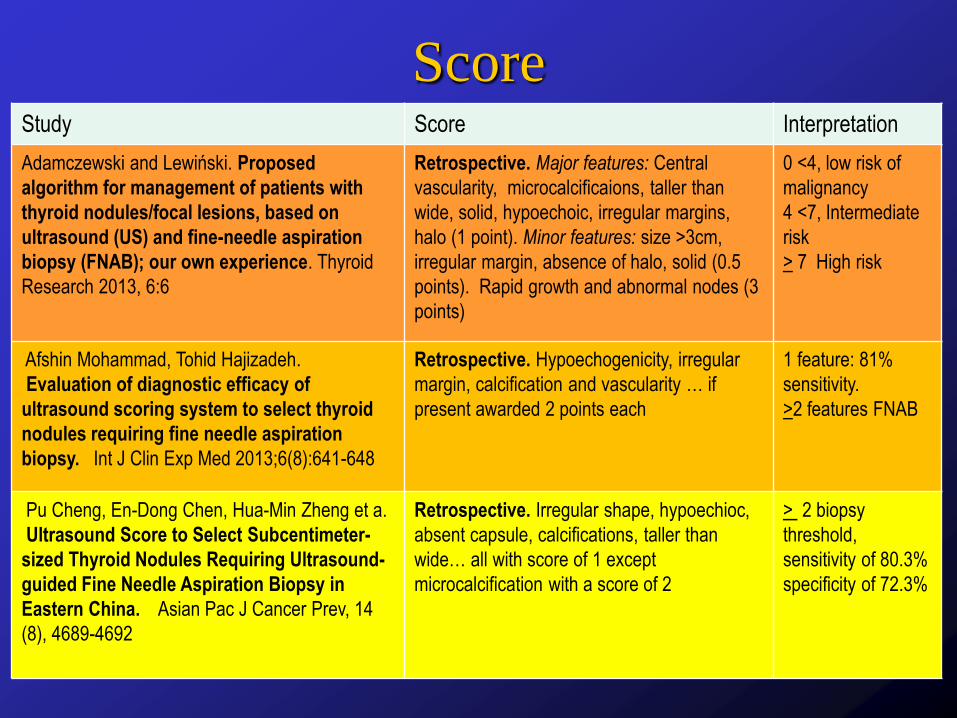
ScoreStudy Score Interpretation
Adamczewski and Lewiński. Proposed
algorithm for management of patients with
thyroid nodules/focal lesions, based on
ultrasound (US) and fine-needle aspiration
biopsy (FNAB); our own experience. Thyroid
Research 2013, 6:6
Retrospective. Major features: Central
vascularity, microcalcificaions, taller than
wide, solid, hypoechoic, irregular margins,
halo (1 point). Minor features: size >3cm,
irregular margin, absence of halo, solid (0.5
points). Rapid growth and abnormal nodes (3
points)
0 <4, low risk of
malignancy
4 <7, Intermediate
risk
> 7 High risk
Afshin Mohammad, Tohid Hajizadeh.
Evaluation of diagnostic efficacy of
ultrasound scoring system to select thyroid
nodules requiring fine needle aspiration
biopsy. Int J Clin Exp Med 2013;6(8):641-648
Retrospective. Hypoechogenicity, irregular
margin, calcification and vascularity … if
present awarded 2 points each
1 feature: 81%
sensitivity.
>2 features FNAB
Pu Cheng, En-Dong Chen, Hua-Min Zheng et a.
Ultrasound Score to Select Subcentimeter-
sized Thyroid Nodules Requiring Ultrasound-
guided Fine Needle Aspiration Biopsy in
Eastern China. Asian Pac J Cancer Prev, 14
(8), 4689-4692
Retrospective. Irregular shape, hypoechioc,
absent capsule, calcifications, taller than
wide… all with score of 1 except
microcalcification with a score of 2
> 2 biopsy
threshold,
sensitivity of 80.3%
specificity of 72.3%
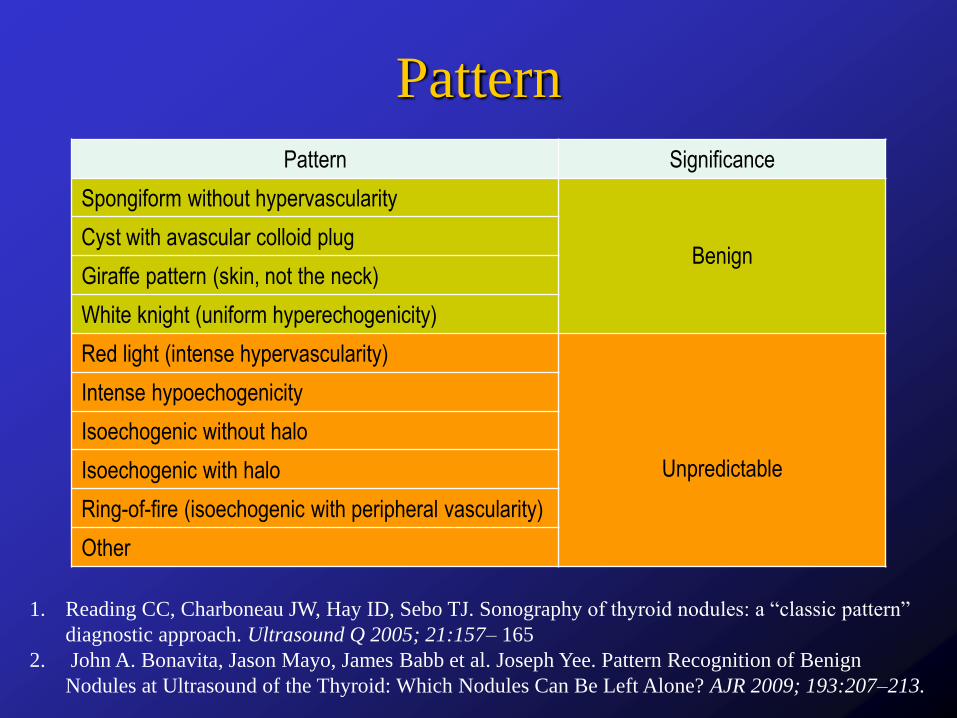
Pattern
Pattern Significance
Spongiform without hypervascularity
Benign Cyst with avascular colloid plug
Giraffe pattern (skin, not the neck)
White knight (uniform hyperechogenicity)
Red light (intense hypervascularity)
Unpredictable
Intense hypoechogenicity
Isoechogenic without halo
Isoechogenic with halo
Ring-of-fire (isoechogenic with peripheral vascularity)
Other
1. Reading CC, Charboneau JW, Hay ID, Sebo TJ. Sonography of thyroid nodules: a “classic pattern”
diagnostic approach. Ultrasound Q 2005; 21:157– 165
2. John A. Bonavita, Jason Mayo, James Babb et al. Joseph Yee. Pattern Recognition of Benign
Nodules at Ultrasound of the Thyroid: Which Nodules Can Be Left Alone? AJR 2009; 193:207–213.
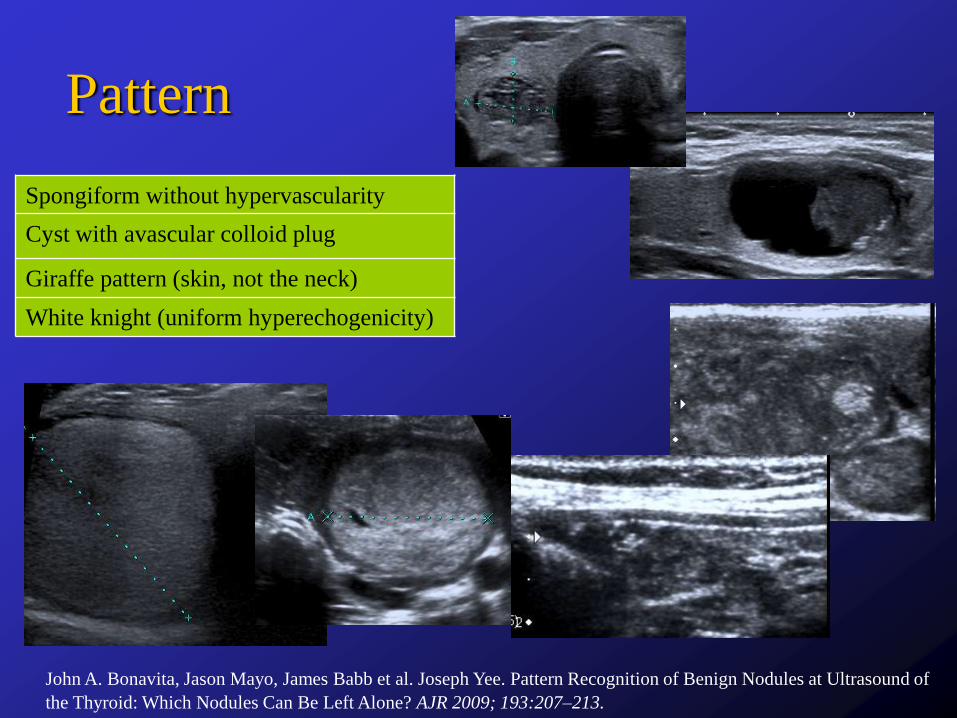
Pattern
Spongiform without hypervascularity
Cyst with avascular colloid plug
Giraffe pattern (skin, not the neck)
White knight (uniform hyperechogenicity)
John A. Bonavita, Jason Mayo, James Babb et al. Joseph Yee. Pattern Recognition of Benign Nodules at Ultrasound of
the Thyroid: Which Nodules Can Be Left Alone? AJR 2009; 193:207–213.

Pattern
Red light (intense hypervascularity)
Intense hypoechogenicity
Isoechogenic without halo
Isoechogenic with halo
isoechogenic with peripheral vascularity
(Ring-of-fire )
Other
John A. Bonavita, Jason Mayo, James Babb et al. Joseph Yee. Pattern Recognition of Benign Nodules at Ultrasound of
the Thyroid: Which Nodules Can Be Left Alone? AJR 2009; 193:207–213.
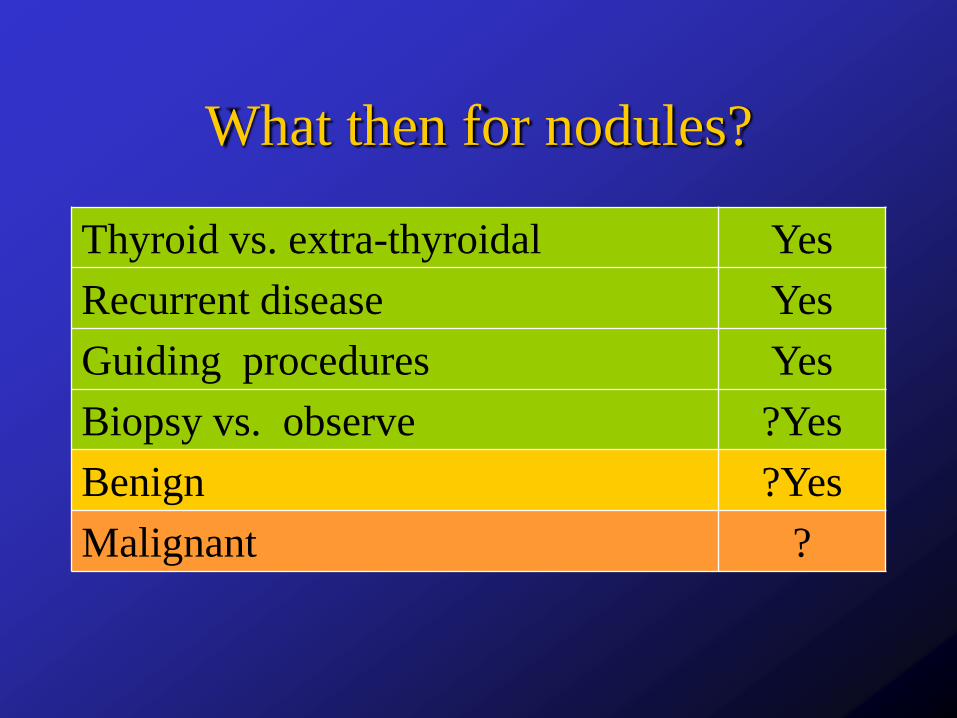
What then for nodules?
Thyroid vs. extra-thyroidal Yes
Recurrent disease Yes
Guiding procedures Yes
Biopsy vs. observe ?Yes
Benign ?Yes
Malignant ?
Diffuse Thyroid Disease
o Hyperplasia
o Thyroiditis
o Graves disease
o Colloid goitre

Thyroid Hyperplasia
o Hyperplasia of cells or acini, followed by
micro and then macronodule formation
o Hyperplastic nodules can undergo
liquefaction with accumulation of serous
fluid, blood and colloid

Suppurative and Subacute
Thryoiditis
o Suppurative thyroiditis is very rare and a
typical abscess is seen.
o Subacute granulomatous thyroiditis (De
Quervain’s disease)
o Hypoechoic, diffusely or focally
o Decreased flow in involved area, normal flow
in uninvolved areas
http://www.thyroidmanager.org/chapter/ultrasonography-of-the-thyroid/#
toc-sonography-in-the-patient-with-an-enlarged-thyroid-gland-goiter

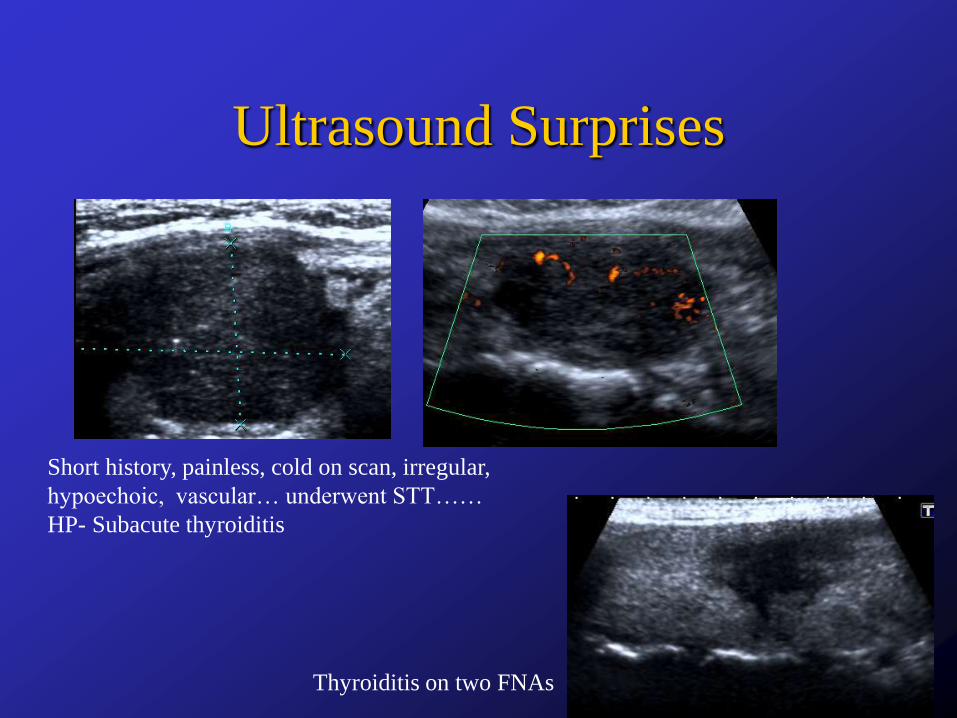
Ultrasound Surprises
Short history, painless, cold on scan, irregular,
hypoechoic, vascular… underwent STT……
HP- Subacute thyroiditis
Thyroiditis on two FNAs
Hashimoto’s Thyroiditis
o Enlarged, hypoechoic, hypervascular,
coarse
o Micronodular, nodules are hypoechoic,
intervening bands can be echogenic.
o Very high flow to very low flow
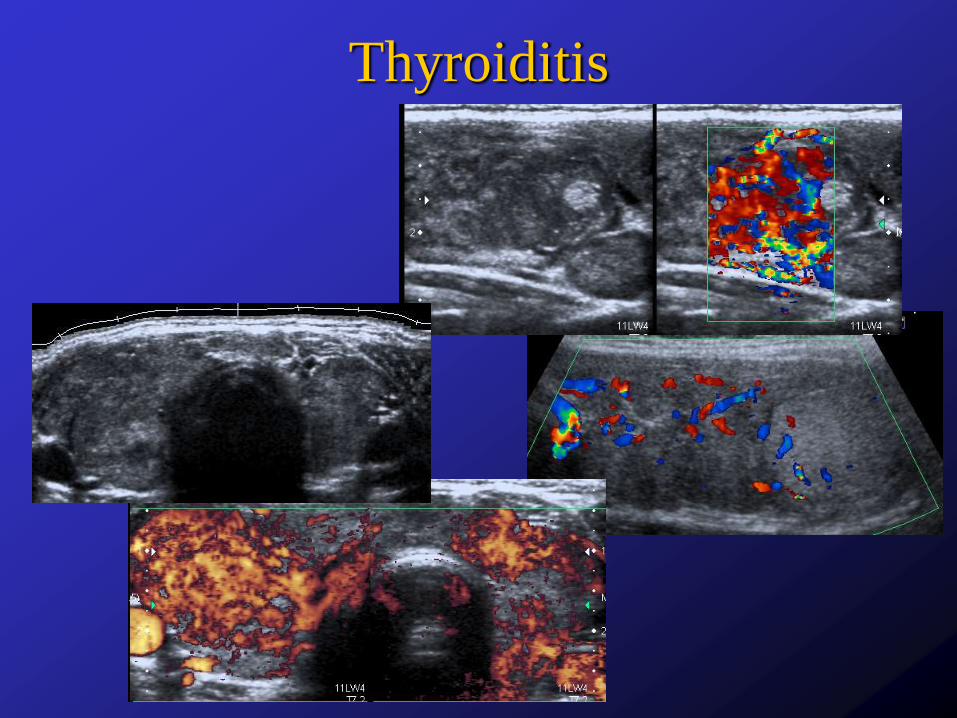
Thyroiditis

Thyrotoxicosis

Thank you
![Welcome [] · Introduction to Musculoskeletal Ultrasound: Getting Started Michael Cartwright, MD | Neuromuscular Ultrasound Francis O. Walker, MD | Neuromuscular Ultrasound Vern Juel,](https://img.dokumen.tips/doc/110x75/5eddc8a7ad6a402d6668f9ab/welcome-introduction-to-musculoskeletal-ultrasound-getting-started-michael.jpg)