Embed Size (px)
Citation preview

IMAGING FEATURES OF GIT AND PANCREATIC
DISEASES

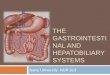
Plain film radiograph
Hepatic angle
Spenic angle
Renal shadow
Psoas muscle
Properitoneal fat strip

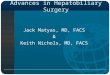
Normal CT anatomy
1.LHV, left hepatic vein
2.MHV, middle hepatic vein;
3.RHV, right hepatic vein;
4.IVC, inferior vena cava
5.Ao,aorta
6.Stomach
12
3 4 5 6

1.LPV, left portal vein
2.Stomach
3.Speen
4.IVC, inferior vena cava
5.Ao,aorta
5
2
3
1
4

1.Gallbladder
2.RPV, right portal vein
3.antrum
4.duodenal bulb
3
4
1
1

1.CA,celiac axis2.Splenic artery3.common hepatic artery4.Duodenum5.Kidney6.Pancreas7.Portal vein8.Adrenal gland
12
34
55
67

SMA:superior mesenteric artery
CBD,common bile duct
Spenic vein
Pancreas

SMV, superior mesenteric vein
SMA, superior mesenteric artery
Uncinate process

CTA
SMA, superior mesenteric artery
CA,celiac axis
Splenic artery
common hepatic artery

main portal trunk; right portal branch; splenic vein; inferior mesenteric
vein; superior mesenteric
vein

RHV, right hepatic vein;
MHV, middle hepatic vein;
LHV, left hepatic vein
IVC, inferior vena cava

pancreatic duct

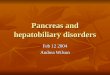
Upper abdominal calcification
may be an important sign of disease Gallstones ,Porcelain gallbladder Urinary Calculi Calcified adrenal glands Pancreatic calcification Tumor calcification ……………

Gallstones 15% -20%of gallstones
contain sufficient calcium to be identified on plain film
right upper quadrant laminated appearance(a dense outer rim and more
radiolucent center)


Porcelain gallbladder
calcification in the wall of the gallbladder
indicative of chronic obstruction of the cystic duct, chronic gallbladder inflammation, and an increased risk of gallbladder carcinoma

diffuse Discontinuous mural calcification

Kidney stones About 85% of urinary calculi
are visible on plain film. Staghorn Calculus a large calculus occupying the
collecting system of the left kidney and assuming its shape

Calcified adrenal glands associated with
adrenal hemorrhage in the newborn, tuberculosis, and Addison disease
either side of the first lumbar vertebra

Pancreatic Calcifications
chronic alcohol-induced pancreatitis
Coarse and punctate calcifications
extend upward across the left upper quadrant


Diffuse Liver Disease Fatty liver
Cirrhosis

Fatty liver(Steatosis) In normal adults, the precontrast attenuation value of the liver is
consistently higher than that of the spleen Milder degrees of diffuse steatosis :the attenuation value of the
liver is less than that of the spleen Marked diffuse steatosis :the liver parenchyma is lower in
attenuation than the hepatic blood vessels

The attenuation value of the liver parenchyma is markedly lower than that of the spleen
The intrahepatic vessels stand out as hyperattenuating structures

Focal fatty infiltration
The same imaging features as diffuse infiltration
Vessels run their normal course through the area of involvement
(lack of mass effect )

Cirrhosis hypertrophy of the caudate lobe and left lobe with shrinkage of
the right lobe
inhomogeneity of hepatic parenchyma,
irregularity (nodularity) of the liver surface,
Extrahepatic signs :evidence of portal hypertension, splenomegaly, and ascites

nodularity of the liver contour
atrophy of the medial segment (M) and enlargement of the lateral segment
prominent notch in the right posterior surface of the liver

Focal Liver diseases
Cyst Hemangioma Hepatocellular
carcinoma metastasis

Cyst:CT appearance
a well-circumscribed, homogeneous mass of near-water-attenuation value (less than 20 HU)
no enhancement after IV contrast medium administration

Two large well-circumscribed, homogeneous, near-water-density masses
no discernible wall

Hemangioma
the most common benign liver tumor
fed by hepatic artery branches
internal circulation is slow
generally remain stable in size over time

well-defined, hypodense on unenhanced scans Enhancement pattern : nodular enhancement
from the periphery of the lesion and proceeding toward the center gradually

Precontrast CT :an attenuation value similar to that of the blood in the inferior vena cava(IVC)

Arterial phase :multiple areas of globular, peripheral enhancement.
Note that the enhanced portions of the mass have an attenuation value similar to that of the intrahepatic vessels.

Equilibrium phase : near-complete enhancement of the mass with an attenuation value equivalent to that of the blood in the inferior vena cava(IVC) and hepatic veins

T2WI:marked hyperintense

Hepatocellular carcinoma
The most common primary malignancy of the liver Risk factors : cirrhosis, chronic hepatitis Growth patterns: solitary massive, multinodular, and diffuse
infiltrative Serum α-fetoprotein(AFP) levels are often
elevated

Hypervascular :contrast enhancement on arterial phase images, with diminishing enhancement on delayed phase images
Tumor thrombus
Tumor capsule: a sharply marginated rim


Necrosis: central low density
The satellite lesions



T2WI T1WI
AP PP DP

Portal Vein Thrombosis
Multiple hypodense nodules ----HCC
Filling defect with the vein

Metastases
The most common malignant masses in the liver Most commonly originate from the GI tract,
breast, and lung Necrosis, fibrosis, calcification, or hemorrhage
within the mass The most common enhancement
pattern :continuous ring-like enhancement

• Multiple
• Hypoattenuating lesions
with mild continuous rim
enhancement

T2WI:a central area of hyperintensity
rim enhancement

Normal MR Cholangiopancreatography (MRCP).

Biliary Dilatation
Diameter of intrahepatic bile ducts larger than 40% of the diameter of the adjacent portal vein
Dilation of the common duct greater than 6 mm Gallbladder diameter greater than 5 cm


Causes of Biliary Tract Obstruction

Choledocholithiasis approximately 20% of cases of obstructive jaundice in the adult
CT:high-density calcification within the duct
MRCP has shown good sensitivity (86% to 100%) and specificity (85% to 100%) for ductal stones



MRCP
Filling defects

Cholangiocarcinoma
arise from the epithelium of bile ducts and are usually adenocarcinomas
Growth patterns include mass forming, periductal infiltrating, and intraductal polypoid

• Mass forming
• periductal infiltrating
• Intraductal polypoid

Peripheral cholangiocarcinoma
Delayed enhancementbiliary dilatationAtrophy (liver)


Perihilar and extrahepatic cholangiocarcinomas
typically exhibit an infiltrating growth pattern focal, circumferential thickening of the bile duct with proximal
dilatation perihilar lesions may be similar in appearance to the intrahepatic,
mass-forming type of cholangiocarcinoma, or may manifest as an intraluminal polypoid mass





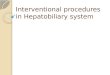
Pancreatic carcinoma a highly lethal tumor CT is recommended for initial imaging assessment CT:a hypodense mass that distorts the contour of the gland obstruction of the common bile duct and pancreatic duct and
atrophy of pancreatic tissue beyond the tumor

A B
C D


Signs of unresectability
tumor involvement of adjacent organs enlarged regional lymph nodes (>15 mm) encasement or obstruction of peripancreatic
arteries or veins metastases in the liver peritoneal carcinomatosis

Pancreatic Carcinoma: Nonresectable
encases and narrows the celiac axis and its branches
partially envelopes the aorta

Plain film radiographs of the abdomen are important for the assessment of the acute abdomen
CT, US, and MR provide comprehensive evaluation of the abdomen, including the peritoneal cavity, retroperitoneal compartments, abdominal and pelvic organs, blood vessels, and lymph nodes

THANK YOU