Embed Size (px)
Citation preview


PANCREATIC INJURY
It is relatively uncommon being encountered in
around 3 % of abdominal trauma, usually caused by
blunt trauma.
FAST has a limit role in acute pancreatic injury.
CT is the most reliable imaging modality.
MRCP is useful in evaluating PD disruption and
associated fluid collection.

CT Findings In Pancreatic Injury
Thickened anterior pancreatic fascia and fluid in the
lesser sac.
Fluid rim between pancreas and splenic vein.
Focal pancreatic contusion and hematoma.

Pancreatic Laceration
PANCREATIC TRAUMA

PANCREATIC TRAUMA

A CT scan performed after abdominal trauma showing diffuse pancreatic
enlargement and was interpreted as suspicious for pancreatic injury. (Grade 1
injury).
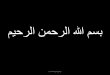
Follow-up CT scan 3 days after abdominal trauma
revealing a tear of the pancreatic body.

A CT scan performed 7 months after surgery showing the
presence of a pseudocyst adjacent to the point of injury

Laceration of the
pancreatic neck without
duct injury

Pancreatic transection (neck)
with duct injury

Subtle pancreatic contusion

Indirect Signs • Edema with global pancreatic enlargement and
loss of lobulation
• Peripancreatic fat infiltration
• Peripancreatic fluid, especially if it is located
around the SMA or the omental bursa
• Hematic fluid between the dorsal surface of the
pancreas and the splenic vein
• Thickening of the left anterior pararenal fascia or
fluid in the anterior pararenal space
• Concomitant duodenal injury

Serum amylase, hematocrit and hemoglobin values during
the initial three days after abdominal trauma.

THANK YOU