Embed Size (px)
DESCRIPTION
Sudhakar Kundapur Venkatesh ∗, John Mun Chin Wan. European Journal of Radiology 67 (2008) 311–320. Articulo de Revisión para fines docentes
Citation preview

European Journal of Radiology 67 (2008) 311–320
Review
CT of blunt pancreatic trauma—A pictorial essay�
Sudhakar Kundapur Venkatesh ∗, John Mun Chin WanDiagnostic Radiology, National University Hospital, Yong Loo Lin School of Medicine, National University of Singapore, Singapore 119074, Singapore
Received 19 March 2007; received in revised form 6 June 2007; accepted 12 July 2007
Abstract
Blunt trauma to pancreas is uncommon and clinical features are often non-specific and unreliable leading to possible delays in diagnosis andtherefore increased morbidity. CT has been established as the imaging modality of choice for the diagnosis of abdominal solid-organ injury inthe blunt trauma patient. The introduction of multidetector-row CT allows for high resolution scans and multiplanar reformations that improvediagnosis. Detection of pancreatic injuries on CT requires knowledge of the subtle changes produced by pancreatic injury. The CT appearanceof pancreatic injury ranges from a normal initial appearance of the pancreas to active pancreatic bleeding. Knowledge of CT signs of pancreatic
trauma and a high index of suspicion is required in diagnosing pancreatic injury.© 2007 Elsevier Ireland Ltd. All rights reserved.K
C
1
f
R
0d
eywords: Blunt trauma; Pancreas; CT
ontents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3111.1. Mechanism of blunt pancreatic injury . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3121.2. Associated injuries . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3121.3. Clinical features . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3121.4. Laboratory findings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3121.5. Diagnosis of blunt pancreatic trauma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3121.6. CT in blunt pancreatic trauma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 313
1.6.1. Parenchymal injury . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3131.6.2. Ductal injury . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 315
1.7. Grading of pancreatic injuries . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3151.8. Complications of pancreatic trauma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3151.9. Clinical course . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 317
1.10. Follow up CT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3192. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. Introduction
Blunt traumatic injury to pancreas is uncommon accountingor less than 2% of all cases of abdominal injuries [1]. Diag-
� This work was presented as educational exhibit at European Congress ofadiology, Vienna, Austria, 2006.∗ Corresponding author. Tel.: +65 6772 2248; fax: +65 6773 0190.
E-mail address: [email protected] (S.K. Venkatesh).
naissulapm
720-048X/$ – see front matter © 2007 Elsevier Ireland Ltd. All rights reserved.oi:10.1016/j.ejrad.2007.07.003
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 319
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 319
osis and accurate grading of pancreatic injury is essential,s the presence of pancreatic ductal injury mandates operativentervention, and missed injuries to the pancreas can result inignificant morbidity [2]. The clinical features are non-specific;erum amylase levels and diagnostic peritoneal lavage may benreliable, due in part to the retroperitoneal location of the organ
eading to possible delays in diagnosis. Delays in diagnosisre associated with an increase in complications especially inatients with higher grade pancreatic injuries [3,4]. CT is theost widely used imaging modality in assessment of major
3 n Jou
acavboCrdei
1
mtbsctsh[isBaf
btttmpv
stw
1
eiaoialtdpip
1
atempnhowesoawohda
1
ta[ia[
tiaecPmeai
1
tcaapop
12 S.K. Venkatesh, J.M.C. Wan / Europea
bdominal trauma and therefore emerged as the modality ofhoice in evaluating pancreatic injury. The reported sensitivitynd specificity of CT in detecting pancreatic injury has beenariable, as findings may be absent or subtle and can be missedy even experienced radiologist. The existing literature on CTf pancreatic trauma is mostly from non-helical or incrementalT and introduction of multidetector CT with faster and high
esolution scans and multiplanar reformations may improveiagnosis of pancreatic trauma. We are presenting a pictorialssay of CT appearances of different grades of pancreaticnjuries which a radiologist should be aware of.
.1. Mechanism of blunt pancreatic injury
The pancreas is a retroperitoneal organ and lies across theidline and the upper lumbar vertebral bodies. The retroperi-
oneal location of the pancreas protects it from most instances oflunt abdominal trauma. Pancreatic injury usually results fromevere anterior–posterior force vectors compressing the pan-reas against the spine, and commonly the injury occurs justo the left of the superior mesenteric vessels [1] e.g. against theteering wheel in a motor vehicle accident in adults, from bicycleandlebar injuries in children, and from child abuse in infants1] or a misplaced seat belt [5]. Other less common situationsnclude direct blow to the abdomen [6], falls [7] and rarely asports related injury [8], Karate [9], and stomping injury [10].lunt pancreatic injury is more common in children and youngdults because they have a thinner or absent mantle of protectiveat that surrounds the pancreas in older adults [1].
Two-thirds of blunt pancreatic injuries occur in the pancreaticody, and the remainder occurs equally in the head, neck, andail [11]. Complete pancreatic rupture as a result of traumaticransection, usually occurs in the line of the superior mesen-eric vein at the neck of the gland. [5]. The pancreatic duct is
ore rigid than the pancreatic blood vessels, capsule and thearenchyma, therefore injury to the duct can occur without anyisible signs of bleeding or capsule ruptures [12].
In a patient with trauma from an anterior–posterior compres-ion with deceleration and an anterior truncal seat belt mark,he examiner should consider aortic and small bowel injuries asell as pancreatic injury [13].
.2. Associated injuries
Isolated pancreatic injuries are rare, and associated injuries,specially to the liver, stomach, duodenum, and spleen, occurn over 70–90% of cases [1,11,12]. The duodenum, which liesdjacent to the pancreas, is likely to be involved in most casesf pancreatic trauma. Forces to the left side of midline maynjure the distal body or tail of the pancreas and may be associ-ted with injuries to the spleen, stomach, descending colon, andeft kidney. In contrast, blows from the right side may injurehe pancreatic head or uncinate process along with the bile
uct, duodenum, liver, right kidney, and ascending colon. Mostatients with pancreatic injuries will have at least one associatednjury with an average of 3–4.1 associated abdominal injurieser patient [1].s[om
rnal of Radiology 67 (2008) 311–320
.3. Clinical features
The typical clinical triad of pancreatic trauma is upperbdominal pain, leukocytosis, and elevated serum amylase levelhat may, however, be absent in adults during the first 24 h andven for several days [14]. Blunt pancreatic trauma is common inultiple injuries patients and difficult to evaluate because these
atients can have concomitant injuries and are clinically oftenot evaluable. In addition, it may be difficult to obtain reliableistory in the trauma patient [15].The retroperitoneal locationf pancreas also minimizes signs or symptoms of such injuries,hich are often vague and non-specific. It has been reported that
pigastric pain out of proportion to physical findings can be aign of pancreatic trauma [16]. The degree of abdominal painr tenderness cannot be used as a discriminator between mildnd major pancreatic injury. Moreover, major pancreatic injuryith minimal epigastric symptoms may be further masked byther associated injuries including long bone fractures [1]. Aigh degree of suspicion is necessary to pursue and establish aiagnosis of pancreatic injury in patients with history of upperbdomen compression injury regardless of degree of pain.
.4. Laboratory findings
The presence of hyperamylasemia after blunt pancreaticrauma is time dependent and a persistently elevated or a risingmylase level are more reliable indicators of pancreatic injury15]. However hyperamylasemia is not specific for pancreaticnjury and can be found in duodenal trauma, hepatic trauma,nd injuries to head and face [17], and in an intoxicated patient18].
The magnitude of the serum amylase levels does not predicthe severity of the damage. Serum amylase levels may be normaln as many as 40% and even in cases of major injury to pancre-tic duct or complete transection of the duct [1,10,19,20]. Serialnzyme values may be useful to follow the late development ofases of pancreatic contusion or pseudocyst formation [21,22].ersistent elevation may indicate a need for operative manage-ent [19]. Trypsinogen-activating peptide is another pancreatic
nzyme that may be used in evaluation for possible blunt pancre-tic injury, although its use has not been thoroughly evaluatedn clinical trials to date [1].
.5. Diagnosis of blunt pancreatic trauma
Establishment of an accurate and rapid diagnosis of bluntraumatic injury of the pancreas continues to be a challenginglinical problem. Frequently pancreatic injuries are discoveredt laparotomy mandated by other associated abdominal injuriesnd abdominal bleeding [23] and many of these without anyre-operative imaging work up [15]. The increasing trend of non-perative management, especially in blunt trauma and stableatients, and the consequences of delayed or missed diagno-
is makes accurate diagnosis of pancreatic injury important3,15,23]. Associated injuries can potentially divert the attentionf the caring physicians and can make the diagnosis and treat-ent of pancreatic injuries even more complicated and difficult
n Journal of Radiology 67 (2008) 311–320 313
[wtodwtoiCfa
1
itpe[rca
fspgot(3oatamtmacosbbiwvtcdwda
d
Table 1CT signs of pancreatic injury (adapted from Refs. [1,4,34])
Specific signsFracture of the pancreasPancreatic lacerationFocal or diffuse pancreatic enlargement/edemaPancreatic hematomaActive bleeding/extravasation of intravenous contrastFluid separating the splenic vein from posterior aspect of pancreas
Non-specific signsInflammatory changes in peripancreatic fat and mesenteryFluid surrounding the superior mesenteric arteryThickening of the left anterior renal fasciaPancreatic ductal dilatationAcute pseudocyst formation/peripancreatic fluid collectionFluid in the anterior and posterior pararenal spacesFluid in transverse mesocolon and lesser sacHemorrhage into peripancreatic fat, mesocolon and mesentery
tmsiFatdaapteTa
1
ap(otc[iai
aocW
S.K. Venkatesh, J.M.C. Wan / Europea
7]. Mechanism of injury should be the guide for diagnosticorkup. It may be difficult to obtain reliable history in the
rauma patient. There may be possible delays from the timef injury and when a diagnosis of pancreatic trauma is madeue to non-specific clinical features and laboratory findings asell radiological findings. Over time, pancreatic trauma tend
o become more radiologically apparent with the developmentf post-traumatic pancreatitis and/or edema with peripancreaticnflammatory changes which may be demonstrated on follow upT. This may be complemented with the development of clinical
eatures and positive laboratory findings such as elevated serummylase.
.6. CT in blunt pancreatic trauma
CT is routinely used as first-line imaging in the acute abdom-nal trauma patient and can be helpful in defining injuries tohe pancreas and associated complications. The detection ofancreatic injury with CT depends on the technique used, thexperience of the observer and the timing of the examination24]. Details of scanning technique should be available for theeader. The technique modifications may require bowel opacifi-ation with oral contrast material, decompression of the stomachnd repeat scans if images are not satisfactory.
Currently multidetector-row CT (MDCT) scanners are usedor evaluation of abdominal trauma cases as they are faster tocan which greatly reduces bowel artifacts and resolves manyrevious technical problems. Generally oral contrast is notiven, but may be administered in selected cases. Dependingn the available scanner, the protocol for MDCT for abdominalrauma is 1.2–2.5 mm collimation; 1–1.75 pitch; 100–150 ml300–370 mg I/ml) of contrast agent injected intravenously at–6 ml/s [25,26]. Scanning is performed at 60–70 s from thenset of contrast injection in portal venous phase coveringbdomen and pelvis. Images are reconstructed at 2.5–3 mmhickness and 2–3 mm intervals. Thinner slice reconstructionsnd multiplanar reconstructions in orthogonal or curved planesay be performed as deemed necessary. Modifications of this
echnique are frequently necessary in trauma situations as scansay include whole body, or a CT angiogram of thorax and
bdomen for suspected bleeding may be performed. In suchases, portal venous phase scans of the abdomen must alwaysbtained immediately after obtaining the angiogram. Delayedcans are also performed in cases of suspected intra-abdominalleeding and may be helpful in cases of suspected pancreaticleeding. Suspicion of isolated pancreatic injury is rare, andn such cases a dedicated pancreatic CT may be performedith scans at pancreatic parenchymal phase (35 s) and portalenous phase (60 s) [27]. Bolus administration of contrast andiming is also critical to scan when enhancement of the pan-reatic parenchyma is optimal and minimize missing of ductalisruption. Pancreas may appear normal in 20–40% of patientshen performed within 12 h after trauma and this is probably
ue to obscuration of the fracture plane, hemorrhage, and closepposition of the pancreatic fragments [1].Most of the literature published on accuracy of CT iniagnosis of blunt pancreatic trauma is based on incremen-
te
s
Extraperitoneal fluidIntraperitoneal fluid
al non-helical CT and there are limited reports using modernultidetector CT technique [28]. The reported sensitivity and
pecificity of CT is variable with an overall sensitivity in detect-ng all grades of pancreatic injury around 80% [1,5,12,29–31].urther when CT is inaccurate in grading the degree of pancre-tic injury; usually a lower grade of injury is diagnosed thanhat actually found at laparotomy [1,7,32,33]. The accuracy ofetecting a major ductal injury by CT has been reported to bes low as 43% [1,5,29–31]. The problem of under-recognizednd missed blunt pancreatic injuries is even more apparent inatients with minimal retroperitoneal fat [1]. With the introduc-ion of multidetector-row CT and volumetric scanning, one canxpect the accuracy of detection of ductal injury to improve [28].he CT signs of pancreatic injury reported in literature [1,4,34]re summarized in Table 1.
.6.1. Parenchymal injuryContusion appears as focal or diffuse areas of low attenu-
tion (Figs. 1, 2, 4, 5 and 8) within the normally enhancingarenchyma. Lacerations are seen as low-attenuation lineFigs. 3, 8 and 10–12) oriented perpendicular to the long axisf the pancreas. In some patients a pancreatic cleft can be iden-ified, usually between the neck and body of the pancreas. Thisleft is a normal variant and should not be construed as an injury1]. The diagnosis of a pancreatic parenchymal fracture on CTs based on visualization of a clear separation across the longxis of the pancreas. The most common site for such a fractures the body or neck of the gland [7].
Fracture or laceration of the pancreas may produce little sep-ration of fragmented tissue or change in density in the regionf interest after administration of intravenous contrast. A pan-reatic fracture often is visualized only on one or two images.
hen the findings of pancreatic fracture are suspicious, addi-
ional thin-slice reconstructions or multiplanar reconstructionspecially in coronal plane may be useful [25].An intrapancreatic hematoma (Fig. 6), when seen, is a verypecific sign of an injured pancreas: the hematoma often is sit-

314 S.K. Venkatesh, J.M.C. Wan / European Journal of Radiology 67 (2008) 311–320
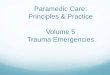
Fig. 1. A 53-year-old male suffered blunt abdomen injury with steering wheel after hitting his car into a tree. Contrast enhanced CT sections (A and B) showingsuperficial contusions (grade I injury) of the head and body of pancreas (arrows).
Fig. 2. Blunt pancreatic trauma. Superficial contusion of the head of pancreas(r(
ufcacc
Ftc
Fig. 4. Blunt pancreatic trauma. Contrast-enhanced CT scan showing fluidbetween posterior pancreas and the splenic vein (arrow heads). Contusions ofthe body and head of pancreas also demonstrated (white arrows). There is freeintraperitoneal fluid (black arrow) due to associated bowel injury (not shown).
black arrow heads). Note the associated duodenal contusion (curved arrow),etropancreatic collection of blood (white arrow) and right pararenal collectionsopen arrow heads).
ated within the fracture, resulting in separation of the fractureragments [35]. Fluid separating the splenic vein and the pan-reas (Figs. 4 and 8) has been suggested as a means of identifying
pancreatic injury and was found in 90% of cases of pan-reatic injury in one study [36]. Normally the splenic vein islosely apposed to the posterior aspect of the pancreas or is sep-
ig. 3. Blunt pancreatic trauma. Contrast-enhanced CT demonstrating a lacera-ion of the body of pancreas (white arrow) with associated retroperitoneal fluidollection (black arrow).
Fig. 5. Blunt pancreatic trauma. Contrast-enhanced CT demonstrating focalhypodensity and swelling of the body of pancreas (white arrows). There is alsofluid in the lesser sac (curved arrow), left anterior pararenal space (open arrow)and hemoperitoneum (arrow heads).

S.K. Venkatesh, J.M.C. Wan / European Jou
Fig. 6. Blunt pancreatic trauma. Contrast-enhanced CT scan at the level of pan-cT(
afloHmtPlmTcipst
t(oa
Fi(t
1
iactn(o
cpwtwCubtuetmchadn
1
mo
reas demonstrating a surgically confirmed hematoma in the head of pancreas.here is also intraperitoneal free fluid (white arrow) secondary to splenic injury
not shown).
rated from the pancreas by a thin layer of fat. In a patient withuid between the splenic vein and the pancreas and a historyf abdominal trauma, a pancreatic injury should be suspected.owever this may be non-specific [37] and rarely the only abnor-al CT finding in patients with blunt pancreatic trauma and
herefore should be viewed with suspicion and followed up.eripancreatic fluid collections (Fig. 8) appear similar to other
ow attenuation fluid collections with associated mass effect andinimal peripancreatic edema and inflammatory changes [37].hickening of the left anterior renal fascia (Fig. 7) is not spe-ific for pancreatic injury and may be related to current or pastnflammatory lesions in this region. Therefore, in traumatizedatients, unexplained thickening of the left anterior renal fasciahould alert the radiologist to possible parenchymal injuries ofhe pancreas (Fig. 9).
Fluid collections in the retroperitoneum, lesser sac,
he transverse mesocolon and mesentery are non-specificFigs. 2–5, 8 and 10–13). Similarly intraperitoneal free fluidr blood (Figs. 4–7) can be found in pancreatic trauma as wells in the other intra abdominal injuries.ig. 7. Peripancreatic inflammatory changes following blunt trauma. There isncreased density of the peripancreatic fat, and left anterior para renal regionwhite arrows). Retroperitoneal free gas pockets (arrow heads) are seen fromraumatic perforation of the second part of the duodenum (not shown).
ppATtmbeAntgspt
1
rmto
rnal of Radiology 67 (2008) 311–320 315
.6.2. Ductal injuryIt is often difficult to determine whether pancreatic duct is
njured or not on the initial CT (Figs. 8, 9, 11). The depth oflaceration has been correlated with the probability of pan-
reatic ductal injury. If the laceration is less than 50% of thehickness of the pancreas, pancreatic ductal injury is usuallyot observed [1,38]. A patient with a post-traumatic pseudocystFig. 8) should be considered to have a ductal leak until proventherwise [1].
When pancreatic duct injury is suspected magnetic resonanceholangiopancreaticography (MRCP) or endoscopic retrogradeancreatogram (ERP) may be done to establish ductal injuryhich will have an impact on management. ERP can be under-
aken in stable patients and requires experienced endoscopistsho may not be available in an acute trauma setting. ThereforeT findings are of great importance. Pancreatic ductal injury isnlikely if CT scans are normal and ductal disruption is likely toe present if the CT scans showed a deep laceration or transec-ion (Fig. 10) of the pancreas [38]. Some authors suggest a followp non-contrast CT after an inconclusive ERP to demonstratextravasation of contrast. If extravasation is found, an opera-ive management is indicated [18]. Even during laparotomy itight be difficult to clarify the question of whether the pan-
reatic duct is injured or not [39]. Whether during laparotomy aigh probability of pancreatic duct injury is sufficient to performpancreatic resection or whether disruption of the pancreatic
uct should be proven before resection by additional invasive oron-invasive diagnostic methods, is still open to discussion.
.7. Grading of pancreatic injuries
Pancreatic organ injury severity has been graded to help withanagement of the trauma cases and also for comparison of
utcomes. The location of the injury (proximal versus a distalancreas) and the status of the main pancreatic duct are the majoroints of the grading system currently proposed by the Americanssociation for the Surgery of Trauma (AAST) [40] (Table 2).his grading system is widely accepted and may be used to iden-
ify patients who are likely to have prolonged stay and higherorbidity so that an early institution of special trauma care can
e indicated. A CT grading system has been proposed by Wangt al. [38] which compliments the surgical classification: grade, pancreatitis or superficial laceration (<50% pancreatic thick-ess); grade B1, deep laceration (>50% pancreatic thickness) ofhe pancreatic tail; grade B2, transection of the pancreatic tail;rade C1, deep laceration of the pancreatic head; grade C2, tran-ection of the pancreatic head. Ductal injury could be accuratelyredicted with this grading system in their study [38]. However,here are no studies published validating the CT classification.
.8. Complications of pancreatic trauma
Blunt pancreatic injuries without ductal leakage usually
esolve spontaneously without complications, and treatmentay be guided by the clinical course. Pancreas related complica-ions occur in 11–62% of patients with an average morbidity ratef 36% [14]. Pancreas specific complications include pancre-

316 S.K. Venkatesh, J.M.C. Wan / European Journal of Radiology 67 (2008) 311–320
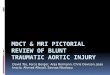
Fig. 8. Contrast enhanced CT of a 23-year-old motorcyclist who had blunt injury to upper abdomen with the handlebar after hit behind by a lorry. Contrast enhancedCT scan (A) done 3 h after trauma shows a heterogeneous appearance of the head of pancreas (white arrow) with a subtle linear hypodensity (black arrow) acrossthe neck of the pancreas. A repeat CT scan (B) done 42 h after initial CT showed a small acute collection at the neck of pancreas (white open arrow). Note thefluid between splenic vein and posterior pancreas (black arrow). There is also perirenal fluid collection (arrow heads). Patient underwent surgical drainage of thec gemeC duct (a
a(stb
Feho
ollection, repair of the associated duodenal perforation and conservative manaT scan (C) demonstrated a pseudocyst (white arrow) with a dilated pancreatict 5 months showed resolution of the cyst.
tic fistula, traumatic pancreatitis (Fig. 14), pancreatic abscess
Fig. 15), and pseudocyst (Fig. 8) formation and major ducttricture (Figs. 8 and 11) [12]. Other less frequent complica-ions include peritonitis, intestinal obstruction, gastrointestinalleeding and acalculus cholecystitis [11].fTtt
ig. 9. Grade III pancreatic injury in a 43-year-old man who had a road traffic accidennhanced CT (A) done 4 h after injury shows laceration of the head of pancreas withead). The grade III injury is highly predictive of pancreatic duct injury which was cff of the main pancreatic duct (arrow).
nt of the associated hepatic laceration. Two months after surgery, a follow uparrow heads). Cystojejunostomy was performed and follow up CT (not shown)
Pancreatic fistula is the commonest complication accounting
or 23% followed by pancreatitis (10%) and pseudocysts (5%).he pseudocysts are most likely to develop in patients with duc-al injury. Patients with acute pseudocysts should be consideredo have a ductal injury unless proven otherwise. Post-traumatic
t and was trapped between the steering wheel and the seat for 15 min. Contrastactive bleeding (black arrow). Note the intact rim of pancreas posterior (arrowonfirmed at surgery with intra-operative pancreatogram (B) demonstrating cut

S.K. Venkatesh, J.M.C. Wan / European Journal of Radiology 67 (2008) 311–320 317
Fig. 10. A 26-year-old male suffered blunt injury to abdomen by bicycle handle bar after hit by a truck. Contrast enhanced CT (A) showing transection of the tail oft h it isa ed tw( t of th
pmrdtol
dd
Fadf
he pancreas (arrow). Ductal injury cannot be assessed at this initial CT, althougnd left renal injury (curved arrow). Endoscopic pancreaticogram (B) performarrow). Patient underwent distal pancreatectomy and conservative managemen
ancreatitis occurs in 6–10% of cases and may lead to significantorbidity and mortality, particularly in patients with hemor-
hagic pancreatitis [5,15]. Pancreatitis may appear as focal or
iffuse enlargement that may progress on serial CT examina-ion, but this may take 24–48 h [5,24]. Infection of a pseudo cystr collection can lead to abscess formation which can potentiallyead to sepsis and distal complications such as acute respiratory1
6
ig. 11. A 10-year-old boy presenting with abdominal pain and vomiting after injurcute fluid collection (arrow) with a laceration in the body of the pancreas (curved arrilated pancreatic duct with stricture at the site of laceration (arrow head) and a pseuollow up CT (C) at 2 months showed residual stricture of the pancreatic duct (arrow
very likely that duct is injured. Note the associated retroperitoneal hematomao days later shows contrast extravasation from the duct at the transection sitee renal injury.
istress syndrome and multi-organ failure which can lead toeath.
.9. Clinical course
Minor contusions and superficial lacerations comprise8–87% of all cases of pancreatic trauma basically allowing con-
ed by the steering wheel in a bump car 10 days earlier. CT scan (A) shows anow). He was conservatively managed. Follow up CT after I month (B) shows adocyst (arrow). Percutaneous drainage of the pseudocyst was performed and ahead). Patient is asymptomatic and on follow up.

318 S.K. Venkatesh, J.M.C. Wan / European Journal of Radiology 67 (2008) 311–320
Fig. 12. Grade III injury of pancreas. Contrast enhanced CT demonstrating adeep laceration of the head and uncinate process of the pancreas with an intactposterior and medial rim of pancreas (arrow head) consistent with a grade IIIinjury of pancreas. There is extensive mesenteric and retroperitoneal collection.
Table 2American association for the surgery of trauma pancreatic organ injury gradingscalea
Grade Injury Description
I Hematoma Minor contusion without duct injuryLaceration Superficial laceration without duct injury
II Hematoma Major contusion without ductal injuryLaceration Major laceration without ductal injury or
tissue loss
III Laceration Distal transection or parenchymal injurywith duct injury
IV Laceration Proximal transection or parenchymalinjury involving ampulla
V Laceration Massive disruption of pancreatic head
Proximal pancreas is to the right of superior mesenteric vein. Advance onegrade for multiple injuries to same organ. Based on most accurate assessmentat autopsy, laparotomy or radiological study.
a From Ref. [40].
Fig. 14. Peri-pancreatic inflammatory changes consistent with pancreatitis in apatient with grade I injury (not shown) to neck of pancreas.
Fig. 15. Post-pancreatic trauma complication. Contrast enhanced CT scandemonstrating a rim enhancing collection (arrow) in the right hypochondriumconsistent with abscess formation.
Fig. 13. Grade IV injury of pancreas. A 34-year-old male laborer hit by a metal rail swung across by a tractor presented with epigastric pain and shock. Contrastenhanced CT (A) done 8 h after injury shows transection of the head of pancreas (white open arrow). A fluid collection seen in the pancreatico-duodenal groove (arrow)separating the duodenum (d) from pancreas. A caudal CT section (B) showing active extravasation from pancreatico-duodenal vessels. Note large retroperitonealhematoma (curved arrows). Patient underwent surgery and hematoma was evacuated; however, died 4 days later secondary to coma from associated head injury.

n Jou
sreud2lts7t[aamaisdtap[
1
cieussc
2
piaisi
R
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
S.K. Venkatesh, J.M.C. Wan / Europea
ervative treatment in stable patients without concomitant injuryequiring operation [12,41]. In patients with associated injuries,arly mortality within the first 24 h can be as high as 30%, partic-larly if there is concomitant vascular injury, and the mortalityue to pancreatic rupture caused by blunt injury can be up to0% [42,43]. Injuries to the pancreatic head are almost twice asikely to be fatal (28%) than injuries to the tail (16%), likely dueo associated injuries of the portal vein, superior mesenteric ves-els and inferior vena cava [38]. Grades I and II injuries have a% mortality and grade III and IV are associated with 29% mor-ality [44]. Three fourths of all fatalities occur in the first 48–72 h2,14,44,45]. The mortality rates of the blunt pancreatic injurypproximate those for penetrating pancreatic injury which isround 20% [12,46]. The most common causes of morbidity andortality are due to a delay in diagnosis and injury to the pancre-
tic duct. The morbidity rate is 12–30% and can increase to 60%f treatment is delayed [44]. Presence of a ductal injury leads tohift from non-operative management to operative treatment asisruption of duct carry a high risk of pancreas related complica-ions. [12]. Management of pancreatic injuries includes drainagelone, distal pancreatectomy, exploration without drainage,yloric exclusion, ductal ligation and pancreaticojejunostomy11,12].
.10. Follow up CT
The difficulties involved in initial CT scan grading of pan-reatic injury highlight the need to proceed with great cautionf a nonoperative path is taken. False negative results or under-stimation of initial CT scan grading may be associated withnopacified bowel loops adjacent to the pancreas, motion andtreak artifacts, as well as suboptimal bolus enhancement. Inuch cases, serial CT scans may be helpful to identify the pan-reatic injury [47].
. Conclusions
A pictorial review of the spectrum of CT appearances of bluntancreatic injury is reported. CT detection of blunt pancreaticnjuries is challenging and requires close attention to techniquend awareness of the subtle changes produced by pancreaticnjury. A repeat CT with thin sections should be considered intable patients when there is a strong suspicion of pancreaticnjury following a normal admission CT.
eferences
[1] Cirillo Jr RL, Koniaris LG. Detecting blunt pancreatic injuries. J Gastroin-test Surg 2002;6:587–98.
[2] Kao LS, Bulger EM, Parks DL, Byrd GF, Jurkovich GJ. Predictorsof morbidity after traumatic pancreatic injury. J Trauma 2003;55:898–905.
[3] Leppaniemi AK, Haapiainen RK. Risk factors of delayed diagnosis of
pancreatic trauma. Eur J Surg 1999;165:1134–7.[4] Bigattini D, Boverie JH, Dondelinger RF. CT of blunt trauma of the pan-creas in adults. Eur Radiol 1999;9:244–9.
[5] Wilson RH, Moorehead RJ. Current management of trauma to the pancreas.Br J Surg 1991;78:1196–202.
[
[
rnal of Radiology 67 (2008) 311–320 319
[6] DeRoux SJ, Prendergast NC. Lacerations of the hepatoduodenal ligament,pancreas and duodenum in a child due to blunt impact. J Forensic Sci1998;43:222–4.
[7] Dodds WJ, Taylor AJ, Erickson SJ, Lawson TL. Traumatic fracture of thepancreas: CT characteristics. J Comput Assist Tomogr 1990;14:375–8.
[8] Harrison JD, Branicki FJ, Makin GS. Pancreatic injury in association foot-ball. Injury 1985;16:232.
[9] Nielsen TH, Jensen LS. Pancreatic transection during karate training. Br JSports Med 1986;20:82–3.
10] Higashitani K, Kondo T, Sato Y, Takayasu T, Mori R, Ohshima T. Completetransection of the pancreas due to a single stamping injury: a case report.Int J Legal Med 2001;115:72–5.
11] Madiba TE, Mokoena TR. Favourable prognosis after surgical drainageof gunshot, stab or blunt trauma of the pancreas. Br J Surg 1995;82:1236–9.
12] Bradley EL, Young PR, Chang MC, et al. Diagnosis and initial managementof blunt pancreatic trauma: guidelines from a multi-institutional review.Ann Surg 1998;227:861–9.
13] Rodriguez J, Buechter KJ. Pancreatic trauma. Prob Gen Surg 1998;15:51–8.
14] Meredith JW, Trunkey DD. CT scanning in acute abdominal injuries. SurgClin North Am 1988;68:255–68.
15] Ilahi O, Bochicchio GV, Scalea TM. Efficacy of computed tomography inthe diagnosis of pancreatic injury in adult blunt trauma patients: a single-institutional study. Am Surgeon 2002;68:704–8.
16] Akhrass R, Yaffe M, Brandt CP, Reigle M, Fallon Jr WF, MalangoniMA. Pancreatic trauma: a ten year multi-institutional experience. Am Surg1997;63:598–603.
17] Greenlee T, Murphy K, Ram MD. Amylase isoenzymes in the evaluationof trauma patients. Am Surg 1984;50:637–40.
18] Wright MJ, Stanski C. Blunt pancreatic trauma: a difficult injury. SouthMed J 2000;93:383–5.
19] Canty Sr TG, Weinman D. Management of major pancreatic duct injuriesin children. J Trauma 2001;50:1001–7.
20] White PH, Benfield JR. Amylase in the management of pancreatic trauma.Arch Surg 1972;105:158–63.
21] Rescorla FJ, Plumley DA, Sherman S, Scherer III LR, West KW, GrosfeldJL. The efficacy of early ERCP in pediatric pancreatic trauma. J PediatrSurg 1995;30:336–40.
22] Jobst MA, Canty Sr TG, Lynch FP. Management of pancreatic injury inpediatric blunt abdominal trauma. J Pediatr Surg 1999;34:818–24.
23] Brooks A, Shukla A, Beckingham I. Pancreatic trauma. Trauma2003;5:1–8.
24] Jurkovich GJ. The duodenum and pancreas. In: Mattox KL, Feliciano DV,Moore EE, editors. Trauma. 4th ed. McGraw-Hill: New York; 2000. p.735–62.
25] Shanmuganathan K. Multi-detector row CT imaging of blunt abdominaltrauma. Semin Ultrasound CT MR 2004;25:180–204.
26] Mullinix AJ, Foley WD. Multidetector computed tomography and bluntthoracoabdominal trauma. J Comput Assist Tomogr 2004;28:S20–7.
27] McNulty NJ, Francis IR, Platt JF, Cohan RH, Korobkin M, Gebremariam A.Multi-detector row helical CT of the pancreas; effect of contrast-enhancedmulti-phasic imaging on enhancement of the pancreas, peripancreatic vas-culature, and pancreatic adenocarcinoma. Radiology 2001;220:97–102.
28] Teh SH, Sheppard BC, Mullins RJ, Schreiber MA, Mayberry JC. Diag-nosis and management of blunt pancreatic ductal injury in the era ofhigh-resolution computed axial tomography. Am J Surg 2007;193:641–3.
29] Jeffrey Jr RB, Federle MP, Crass RA. Computed tomography of pancreatictrauma. Radiology 1983;147:491–4.
30] Leppaniemi A, Haapiainen R, Kiviluoto T, Lempinen M. Pancreatic trauma:acute and late manifestations. Br J Surg 1988;75:165–7.
31] West OC, Jarolinek AM. Abdomen: traumatic emergencies. In: Harris JrJH, Harris WH, editors. The radiology of emergency medicine. 2nd ed.
Philadelphia: Lippioncott-Williams & Wilkins; 2000. p. 708–10.32] Akhrass R, Kim K, Brandt C. Computed tomography: an unreliable indi-cator of pancreatic trauma. Am Surg 1996;62:647–51.
33] Wyatt SH, Fishman EK. Spiral CT of the pancreas. Semin Ultrasound CTMR 1994;15:122–32.

3 n Jou
[
[
[
[
[
[
[
[
[
[
[
[
[ical factors in the treatment of pancreatic trauma. Surgery 1976;80:
20 S.K. Venkatesh, J.M.C. Wan / Europea
34] Gupta A, Stuhlfaut JW, Fleming KW, Lucey BC, Soto JA. Blunt traumaof the pancreas and biliary tract: a multimodality imaging approach todiagnosis. Radiographics 2004;24:1381–95.
35] Lane MJ, Mindelzun RE, Jeffrey RB. Diagnosis of pancreatic Injury afterblunt abdominal trauma. Semin Ultrasound CT MRI 1996;117:177–82.
36] Lane MJ, Mindelzun RE, Sandhu JS, McCormick VD, Jeffrey RB. CTdiagnosis of blunt pancreatic trauma: Importance of detecting fluid betweenthe pancreas and the splenic vein. AJR Am J Roentgenol 1994;163:833–5.
37] Sivit CJ, Eichelberger MR. CT diagnosis of pancreatic injury in children:significance of fluid separating the splenic vein and the pancreas. AJR AmJ Roentgenol 1995;165:921–4.
38] Wong YC, Wang LJ, Lin BC, Chen CJ, Lim KE, Chen RJ. CT gradingof blunt pancreatic injuries: prediction of ductal disruption and surgicalcorrelation. J Comput Assist Tomogr 1997;21:246–50.
39] Patton JH, Lyden SP, Croce MA, et al. Pancreatic trauma. A simplifiedmanagement guideline. J Trauma 1997;43:234–41.
40] Moore EE, Cogbill TH, Malangoni MA, et al. Organ injury scaling.II. Pancreas, duodenum, small bowel, colon, and rectum. J Trauma1990;30:1427–9.
[
rnal of Radiology 67 (2008) 311–320
41] Timberlake GA. Blunt pancreatic trauma: experience at a rural referralcenter. Am Surg 1997;63:282–6.
42] Graham GM, Mattox KL, Jordan GL. Traumatic injuries of the pancreas.Am J Surg 1978;136:744–8.
43] Jones RC. Management of pancreatic trauma. Am J Surg1985;150:698–704.
44] Wolf A, Bernhardt J, Patrzyk M, Heidecke CD. The value of endoscopicdiagnosis and the treatment of pancreas injuries following blunt abdominaltrauma. Surg Endosc 2005;19:665–9.
45] Arsenio JA, Demetriades D, Hanpeter DE, Gambaro E, Chahwan S.Management of pancreatic injuries. Curr Probl Surg 1999;36:325–419.
46] Heitsch RC, Knutson CO, Fulton RL, Jones CE. Delineation of crit-
523–9.47] Brestas PS, Karakyklas D, Gardelis J, Tsouroulas M, Drossos C. Sequen-
tial CT evaluation of isolated non-penetrating pancreatic trauma. JOP2006;7:51–5.