Embed Size (px)
Citation preview

Image Guided Radiation Therapy
Basic principles, technologies, and future directions
Parminder S. Basran, PhDDept. Medical Physics
BCCA-Vancouver Island Centre

Introduction
• Some definitions and background
• Descriptions of image guided radiation therapy technologies– 2, 2.5, 3 and 4D– Just-it-time vs. Real-time
• Where are we going?

Definitions
IGRT is not:
In a Golden Room of Tools
Idylic Greeks Rummaged Turkey
I’ll Get a Rounda Tequilas
I’m Guessing its Radiation Therapy

Definitions
IGRT is :
- Image Guided Radiation Therapy
- Not new, but now applied with imaging technologies other than portal imaging

Definitions
IGRT• Radiation therapy has evolved from a 2D
technique to 3D, and in some cases 4D
• 3D morphological and functional imaging techniques change targeting
• Refined conformal delivery techniques, ex: IMRT offers the ability to sculpt the dose more closely to the tumour volume.

Definitions
However, with such dose conformity to the tumour volume and the rapid dose fall off outside the tumour volume, the accuracy of daily delivery becomes crucial.
There will be uncertainties introduced in this process and a ‘‘safety” margin should be accounted for.
ICRU-50 + 62 [2,3] create nomenclatures for facilitating the image guidance task by specifying the geometric constructs and margins.

ICRU standard definitions for margins in radiation therapy
GTV
CTV
ITV
PTV

Background
Sources of uncertainties- Systematically defined before treatment
- Potentially largest source is target volume identification*
- Rx to Tx errors
- During treatment- Systematic errors- Daily non-predicted errors (random?)
*Rasch C, Steenbakkers R, van Herk M. Target definition in prostate, head, and neck. Semin Radiat Oncol 2005;15:136–45.

Displacements with Respect to Isocentre
-15
-12.5
-10
-7.5
-5
-2.5
0
2.5
5
7.5
10
12.5
15
-15 -12.5 -10 -7.5 -5 -2.5 0 2.5 5 7.5 10 12.5 15
Left-Right [mm]
Su
p-I
nf
[mm
]Patient 1
Patient 2
Patient 3
Patient 1 AVERAGE
Patient 2 AVERAGE
Patient 3 AVERAGE

Background
During treatment- Systematic errors
- Controllable and correctable
- Daily non-predicted errors (random)- Primarily a function of the “system” itself- Ex: Flipping a balanced coin is unpredictable,
but flipping a weighted coin is somewhat predictable.

Background
Some examples of “weighted” coins in RT- A really bad/good breast-board- A really good/bad couch indexing system- An overzealous/far-sighted Portal Image
analyzer
If you know your coin is weighted, then you will have a better understanding of your margins.

What is IGRT?For purposes here, it is a generalized approach of capturing
and reducing systematic and random errors when delivering radiation therapy.
Involves acquiring data that can capture the position of treatment volumes
Ex: prostate and dose escalation, hypofractionation
avoidance structuresEx: SBRT spinal cord
It doesn’t have to be Image-based (but GRT doesn’t sound sexy). BUT we will assume this data = images

Image Guided RT :Classical approach (Just in Time)
Patient Set-up
Assess Patient Position
AdjustPatient Position
VerifyPatient Position
TreatPatient
Decisions / Processes
On-line
Decisions /
Processes
On-line
Decisions /
Processes
Off-line
Planning CT
TreatmentPlan

Decisions / Processes
Real Time
Image Guided RT :Real-Time (nD +1) approach
Patient Set-up
Assess Patient
Positioning
AdjustPatient Set-up
VerifyPatient Set-up
TreatPatient
Decisions / Processes
On-line Decisions /
Processes
Adaptive
Decisions /
Processes
On-line
Decisions /
Processes
Off-line
Planning CT
TreatmentPlan

Image Guided RT Technologies
Categorized by the
• # of dimensions of
acquisition
• Modality– x-rays: kV / MV– Ultrasound– MRI

Image Guided RT Technologies
2D: MV Portal imaging• Just-in-time• Real-time

Image Guided RT Technologies
2D: kV imaging• Real-time

Image Guided RT Technologies
2D: kV imaging• 2D + 1

Image Guided RT Technologies
2D: Ultrasound• Just-in-time• Real-time
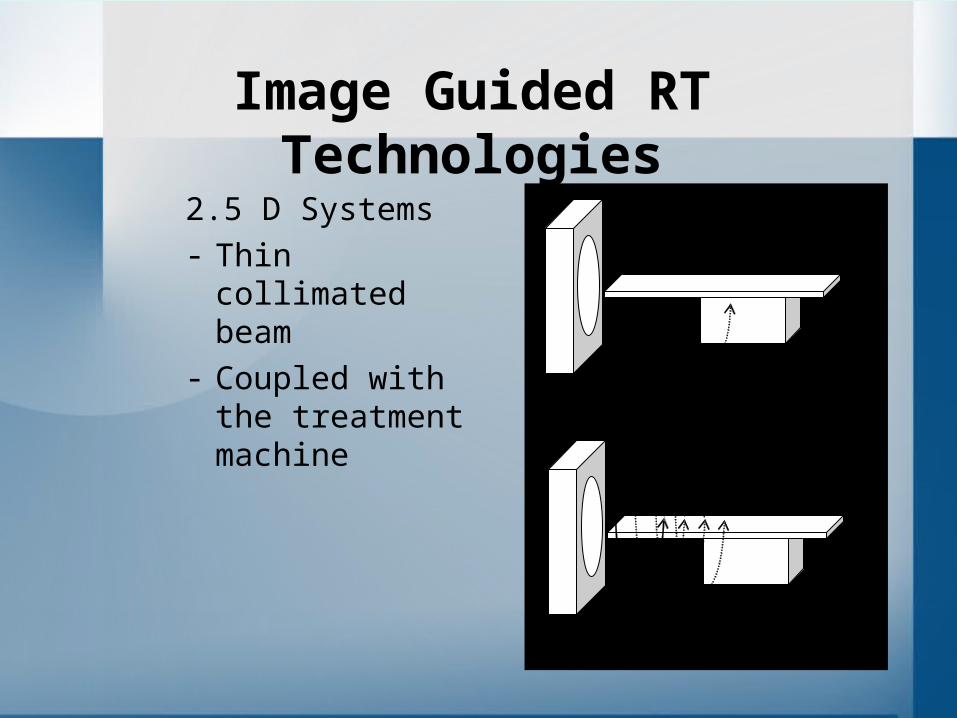
Image Guided RT Technologies
2.5 D Systems- Thin collimated
beam- Coupled with the
treatment machine
T=1 s … 3 s … 5 s … Couch motion
steps in after each gantry rotation
Acquire, translate, and acquire …
Couch motion is constant during continuous gantry rotation
Continuously acquire and translate

Image Guided RT Technologies
2.5 D Systems
Tomotherapy
MV CT
– Just in time
– 2.5D + 1
(research only)

Image Guided RT Technologies
2.5 D Systems
CT on rails
– Just in time
– Real-time
(research)

Image Guided RT Technologies
3D Systems- True acquisition of 3D data, not just
stacking 2D data and calling it 3D- Focus of most clinical research
- Technically challenging- Noise vs. dose vs. accuracy
- Key Modalities- X-ray- MR- Ultrasound

Image Guided RT Technologies
3D kilovoltage X-ray imaging systems

Image Guided RT Technologies
3D X-ray imaging systems

Image Guided RT Technologies
3D MVCT imaging systems

Image Guided RT Technologies
3D Megavoltage imaging systems

Image Guided RT TechnologiesPros / Cons of MV CT (2.5 & 3D)
• the treatment beam is used for imaging, MV-based solutions provide most accurate/direct geometric information concerning alignment of treatment beam and target.
• On the other hand, MV-based solutions will inherently be inferior to kV-based solutions as kV images provide better soft-tissue contrast owing to the prevalence of photoelectric absorption interactions.


Image Guided RT TechnologiesPros / Cons of MV CT (2.5 & 3D)• MV based volumetric imaging features some additional
generic advantages.– The imaging dose can be easily incorporated into the dose
calculation algorithm – Linear relationship between electron density and megavoltage
HUs due to Compton scatter – MV-based CT images can be used to complement or even
replace diagnostic kV CT images when high density objects introduce severe artifacts, due to the fact that these artifacts and beam hardening are less critical for MV sources.
• A potential argument against MV-based solutions could be patient dose, however, it should be noted at this point that extra patient dose due to IGRT is a complex issue (see AAPM TG 75).


Image Guided RT TechnologieskV-CBCT considerations• Field of View
– Determines the length of scan available and possible solutions if longer scan lengths are required
– What size is the reconstruction circle?– Determines the lateral FOV
• Filters required? – Which filters are available?– Involves time to select and insert, and affects image quality– Are filters interlocked?– If not, then risk of poor quality or unusable scans from incorrect
filters selection
• Can panel be positioned remotely? If so, does this the system come with an anti-collision system?– Will involve time to position if not remotely accessed

Image Guided RT TechniqueskV-CBCT considerations• What are the available rotation speeds?
– Determines the acquisition time– What are the possible angles of rotation?– Affects the flexibility of scanning; e.g. the possibility of performing half-
scans for small regions, rotations through 180 degrees (underneath the patient) and using preset or flexible start and stop angles
• How ergonomic is the operation?– One- or two-button operation, foot- or hand-control, several screens
affects the ease of operation and the risk of aborted scans
• Can the scan be stopped and restarted?– Will result in extra dose if the scan is interrupted inadvertently, and
has to be started from the beginning– Also allows the scan to be acquired with the patient in several breath
holds.

Image Guided RT Technologies
• Other 3D / 4D techniques– ViewRay
• 3 Cobalt sources w/ intensity modulation capabilities
• MR scanner• Real-time imaging

Image Guided RT Technologies
• Other 3D / 4D techniques– MR-Linac projects
• Edmonton
• Germany

Image Guided RT techniques
3D +1– Simultaneously collect 3D images
• Prior to treatment
• During treatment

“Symmetry captures image data during the breathing phase and performs sophisticated computations to provide 4D data. This data helps to visualize the tumor position in each phase of the respiratory cycle to arrive at an average position of the tumor for each treatment”

Where are we going?
New machines slated for install likely around mid March
All will have - 2D MV imaging- 2D kV imaging- 3D kV-CBCT abilities
Some (or maybe just 1) will have- RPM imaging capabilities- 6 Degrees of Freedom couch motion- ?

The factors for consideration in image registration and set-up evaluation and their relevance.
What assessment tools are available?• View several planes, and availability of visual methods to
compare image to reference (spyglass, colourwash, checker board, toggle function)
How many degrees of freedom are available?• Availability of inclusion/exclusion of rotation• Will affect the flexibility of the system, the ability to use
different correction protocols, and the precision of the match results
What functions are available for registration?• entire image or a ROI, choice of intensity levels, and soft
tissue or bony anatomy selection is available

The factors for consideration in image registration and set-up evaluation and their relevance.
Is manual or automatic match available?• Affects time to match, training, decision making, and match
results, ability to check registration
Is rigid- or non-rigid-matching used?
Can the couch correction be applied remotely?• Affects efficiency of on-line verification, correction & patient
safety• If the couch can be moved remotely, is visual monitoring
available and/or collision detection systems? Is the movement mechanically limited?
What is the resolution of couch movement?• Affects accuracy but is also dependent on couch calibration

Where are we going?
IGRT Working Group
Charged with helping lead the integration of IGRT at our clinic– Determine starting point/site for implementing IGRT program
– Identify & Define Training Needs and Establish Training Program
– Establish & implementing site-specific protocols & procedures
– Evaluate, track efficiency and efficacy of IGRT practices

Where are we going with IGRT here?
Likely endpoints• An efficient and clearly defined set of IGRT processes / protocols
– Better patient treatments– More confidence in treatment– Customized treatment– Ability to image daily if needed– Less subjectivity– Better image quality– A program that would allow us participate in trials requiring IGRT– Clearly defined protocols– Automated couch moves
• Programs for– Well defined quality control and assurance for
• Patient specific procedures, protocols, and patient QA: an auditing system• Machine-related QA
– Education and training• Clear indication of the resource implications

Thanks…
and stay tuned..










![PET-guided delineation of radiation therapy treatment ......and many other techniques including CyberKnife, heavy ion therapy [6] and many other radiation therapy devices for dose](https://img.dokumen.tips/doc/110x75/5ec54a2492626b725255921d/pet-guided-delineation-of-radiation-therapy-treatment-and-many-other-techniques.jpg)


















