Embed Size (px)
Citation preview

Emergency management of Metabolic Crisis Dr. Vidyut Bhatia Pediatric Gastroenterologist Indraprastha Apollo Hospital, New Delhi Editor: Celiac Focus

Inborn Errors of Metabolism
Individually rare, together they are 1:800-5000 incidence
Most difficult task for clinician is to know when to consider IEM and which tests to order for evaluation
Don’t be fooled--other diagnoses like sepsis, ICH, pulm. hem. may accompany IEM
Clues to presence of IEM may often be found in FH

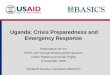
PROTEIN GLYCOGEN FAT
AMINO ACIDS FRUCTOSE
GALACTOSE
FREE FATTY ACIDS
AMMONIA
UREA
UREA CYCLE
ORGANIC ACIDS GLUCOSE
PYRUVATE
ACETYL CoA
KREBS CYCLE
NADH
KETONES
ATP
LACTATE
An integrated view of the metabolic pathways

Metabolic Diseases Which Can Present in Crisis
Defects of glucose homeostasis (20)
Defects of amino acids (10)
Defects of fatty or organic acids (20)
Defects of Lactate/Pyruvate (20)
Defects of Peroxisomes
Others

IEM- Index of Suspicion
Rapid deterioration in an otherwise well infant
Septic appearing infant
Failure to thrive
Regression in milestones
Recurrent emesis or feeding difficulty,
alterations in respirations, lethargy, jaundice, sz, intractable hiccups
Dietary aversion Family history
Severe hyperammonemia, metabolic acidosis abnl urine/body smell

“Waiting until sepsis and other more common causes of illness are ruled out before initiating a specific diagnostic evaluation is inadvisable, as is indiscriminate
study of all ill newborns for metabolic disorders.”

History and Antecedent Events
Catabolic state induction (sepsis, fasting, dehydration)
Protein intake
Change or addition of PO proteins, carbs, etc… in formula
Consanguinity
FHx of SIDS, autism, devl delay

Assessment:
Vitals Level of alertness Abnl activity/mvmts CV- perfusion Dysmorphology, hair, eyes-cornea Abdo- HS megaly Neuro- DTRs, tone, etc Skin- bruise, pigment, color

Recognize that Smell
Musty or Mousy:
PKU
Boiled Cabbage
Tyrosinemia or hypermethioninemia
Maple Syrup
maple syrup urine disease
Sweaty feet:
isovaleric acidemia or glutaric acidemia type II
Cat urine
multiple carboxylase deficiencies (Biotin deficiency)

Laboratory Assessment of Neonates Suspected of Having an Inborn Error of Metabolism Routine Studies Special Studies Blood lactate and pyruvate Complete blood count and differential Plasma amino acids Plasma ammonia Plasma carnitine Plasma glucose Urine amino acids Plasma electrolytes and blood pH Urine organic acids Urine ketones Urine-reducing substances

Emergency Management:
Can be life threatening event requiring rapid assessment and management
Two primary goals
removal of accumulating metabolites
prevention of catabolism

Treatment of the Acutely Sick Child Maintain ABC
Oxygenation Hydration Acid/Base balance
STRIVE TO IDENTIFY PRIMARY METABOLIC DISORDER

Emergency Management
NPO
D5-D10 1-1.5 x maint
Correct hypoglycemia
Correct hypoglycemia IV dextrose bolus, 25%, 0.25-0.5 g/kg/dose (1-2 mL/kg); not to exceed 25 g/dose
Dextrose 10-15% IV @ 8-10 mg/kg/min
Add insulin, 0.2-0.3 IU/kg, as needed

Acidosis and electrolyte abnormalities
The pH and dose at which bicarbonate should be administered are controversial
pH <7.0-7.2, dose 0.35-0.5 mEq/kg/h up to 1-2 mEq/kg/h
For intractable acidosis, consider hemodialysis
Dialysis, lactulose if High/toxic NH4 (nl is <35µmol/L)

Some quick supplements:
Carnitine: IV/PO 100 mg/kg/d
Sodium Benzoate, Phenylacetate for Hyperammonemia
IV: 0.25 g/kg bolus over 24 h, then infusion of 0.25 g/kg over 24 h
Mega-vitamin therapy:
Vitamin B12 (1 mg) should be given im (B12 responsive form of methylmalonic academia)
Biotin (10 mg) should be given orally or by nasogastric tube, (multiple carboxylase deficiency)

Patient is stabilized Now what?
Broad DDx
You can group into KEY features
Can focus on initial labs = Hyperammonia, hypoglycemia, metabolic acidosis.
Can focus on Prominent neurologic features
Can focus on Dysmorphic features
If these don’t exactly fit, resort back to categories of IEMs and Neurodegenerative Disorders.

Diagnostic algorithm
METABOLIC ACIDOSIS
HYPERAMMONEMIA
Ketonuria Ketonuria
Hyperlactatemia
Hypoglycemia
Major hyperlactatemia Maple Syrup Urine Disease (MSUD)
Maple Syrup Urine Disease (MSUD)
Hypoglycemia Organic aciduria
Organic aciduria Pyroglutamic
aciduria
Non-ketonic hyperglycinemia Sulfite oxydase deficiency - XO
Urea Cycle Disorders
Respiratory chain
Fatty acid oxydation Variant hyperinsulinism
(glutamate dehydrogenase)
Fatty acid oxydation Glycogen storage disease Glyconeogenesis defects
Mitochondrial defect
no
no
no no
no
no no
no
yes
yes
yes
yes
yes
yes
yes yes

Quick References:
MA: *metabolic acidosis
NH4:
Glu:
Dz: *Non-ketotic Hyperglycine
*Urea Cycle defects
*Fatty Acid Oxs *OAemia
*OAemia *OAemia
*OAemia *Glycogen Strg dfc *Amino Aciduris
*Carb Metabolism dfc

Organic Acidemias:
*Acidotic with high Gap
*Urine Ketones high
*High to nl Ammonia
Often present first 2-7 days of life after dietary protein introduced.
Drunk appearance in infant.
*May have low WBC and Plts.
Check serum AAs/OAs, Urine AAs/OAs, CSF OAs/AAs.

Organic Acidemias
Isoleucine Valine Methionine Cholesterol Odd chain fatty acids
leucine Isovaleryl CoA HMG CoA Acetyl CoA
Krebs Cycle
Methylmalonyl CoA Propionyl CoA Succinyl CoA biotin B12
Lysine Tryptophan Glutaryl CoA Crotonyl CoA
3MCC
Acetyl CoA
Organic acids are intermediates in the catabolic pathways to break down amino acids, lipids and other compounds to acetyl CoA and succinyl CoA which are entry points into the Kreb cycle
*Urine organic acid analysis will show elevation of organic acids proximal to the enzymatic block; the resulting pattern is interpreted by the metabolic laboratory

Urea Cycle Defects
Symptom free period and then emesis->lethargy-->>COMA
Key features: High Ammonia, low BUN Possible Lactic acidosis *Absence of ketonuria* Nl to mild low Glucose
**Treat high ammonia, infuse glucose, send plasma AAs/OAs, urine orotic acid, and plasma citrulline.
Infusion of 6ml/kg 10% Arginine HCl over 90 min may help

Consequences
Once ammonia >150 µmol/L can lead to permanent neurological damage
Requires prompt & aggressive treatment Withdraw dietary protein
Sodium benzoate/ phenylbutyrate
Haemofiltration/dialysis

Urea cycle disease versus organic acidemias
lethargy/coma
vomiting
hyperammonemia
metabolic ketoacidosis
primary respiratory alkalosis
UCD OA
+ +/-
+
+
+
+ + +
-
-
+

Fatty acids
fasting
ketones
acetyl CoA
Krebs cycle
VLCAD LCHAD MCAD SCAD
CPT1/CPT2
+
Brain
Fatty acid oxidation
Distinguishing feature of FAOD is hypoketotic hypoglycemia MCAD deficiency most common and has a 25% risk of death with first episode LCHAD, VLCAD and carnitine uptake disorder are variably associated with, hepatomegaly, liver disease, hypertrophic cardiomyopathy and potential arrythmias

Liver disease
A metabolic liver disease should be suspected if there is one or more of the following:
persistent unconjugated jaundice
hepatocelluar dysfunction
hypoglycemia without other liver dysfunction

Liver disease
Hepatocellular dysfunction Disorders of amino acid metabolism
Tyrosinemia I Disorders of carbohydrate metabolism
Galactosemia Hereditary Fructose Intolerance Glycogen Storage Disease type IV
Lysosomal storage disorders Niemann Pick Disease

Galactosemia
Galactokinase deficiency--less common
Galactose-1-P uridyl transferase (GALT) deficiency- causes classic galactosemia
Gal-1- P is toxic
Clinical
Presents classically as a sick newborn with vomiting diarrhea, jaundice, progressive liver and renal disease, E.coli sepsis, progressive bilateral cataracts

Galactosemia
Dx assisted by Non-glucose reducing substances in urine
Confirmation by Galactose-1-PO uridyl transferase activity in RBCs

Lastly: Non-ketotic Hyperglycinemia
Unique entity in that Glucose, NH4, pH are all normal
4 types with varying ages of onset, however, classic form is Neonatal with onset in 1st week of life.
Will present just like the other devastating IEMs. Lethargy, emesis, hypotonia, seizures, etc…
Uncontrolled hiccups.
Dx with no urine ketones, and Elevated Glycine.
No effective Rx. Will require diet restriction

The Metabolically ill Child
If you Don’t know you Wont think
If You Don't Think You Wont Look
If You Don't Look You Wont Find
If You Don't Find You Can’t Treat