Embed Size (px)
Citation preview
Drug History and Introduction to Prescribing
Dr Andrew Stein, Consultant Nephrologist, UHCW

Outline of Talk
• Drug History
• Introduction to Prescribing
• Learning Objectives (LO): British National Formulary (BNF) and Formularies
• Quiz
Drug History
Why is it important?
• Make patients better
• Prevent (or reverse) harm to patients
• Prescribing errors very common
• They are the single most preventable cause of patient injury
• Junior doctors: most serious errors occur in prescribing and communication (esp handover)
• Good idea of PMH

Prescribing Errors
• 18,820 patients admitted to hospital over a six-month period
• 1,225 related to an adverse drug reaction (ADR; prevalence 6.5%)
• ADR led directly to admission in 80% cases
• Majority (72%) of these admissions were avoidable
• Bed stay was eight days (4% hospital bed capacity)
• Annual cost to NHS was £466 million pa
Pirmohamed M, BMJ 2004

If do one thing well, whilst clerking as F1-2 ..
• Take a good drug history
• No one else will, ie doctors that follow you
• Or state that you are not doing it (unable to, and why)

Information Sources
• Patient
• Family or carer
• GP (recent referral letters)
• Recent discharge letters
• Tablets themselves (weekly packs)
• Medication list (actual)
• Pharmacy (local)
• Ask pharmacist (reconciliation)
Interviewing the Patient
• Introduce yourself
• “My name is Dr Stein and I am your doctor”
• (Ps insert your name above)
• I would like to know about your tablets (start with open questions)
Drug History
• “Are you taking any tablets at the moment?”
• “What do you take that for?”
• “How many times a day do you take that tablet?
• “How many do you take? Do you know the strength of the tablets?”
• “Do you buy any other medication from the chemist (OTC) or internet?”
• “Do you take any other drugs (herbal or recreational)?”
Drug History (Repeat)
• It is so important, start again
• So you are on ‘x statin’ and ‘y pril’ .. anything else?
• Anything else?
• Are you sure?
Drug History (Specific)
• Oral contraceptive (OC) .. “are you on the Pill?”
• Warfarin (ask if, AF, CCF)
• Injections (INSULIN, EPO)
• Inhalers
• Eye drops (TIMOLOL)
• Patches (contraceptive implants, analgesia)
Drug History (Recent)
• Often cause of admission, so very, very important
• “Any changes to your tablets recently?”
• “New ones?”
• “One stopped? By whom? When? Why?”
• “Doses changed?”
• (Repeat) “Any other changes?”
Barriers to full Drug History (LO) • Patient
– Belief – physician has information (and we are all linked)
– Unfamiliar with medications and names
– Memory/Confusion (acute or chronic, or both)
– Language barrier
– Visual or hearing impairment
– Child/Elderly
– Old information
• Different locations (specialist units, different hospitals, psychiatry)
• Carer gives or sets up medication
• Bottles, blister packs or list unavailable
• ‘Difficult historian (you)’
Drug History Top Tips
• Balance open-ended questions (“tell me about your tablets”) with closed questions (eg requiring yes/no answers, eg “are you on the pill”?)
• Ask non-biased questions
• Avoid leading questions
• Explore vague responses (non-compliance)
• Avoid medical jargon (“ACE inhibitors”) – Keep it Simple
• Avoid judgmental comments, or colluding

Allergies
• “Are you allergic to any drugs?”
• “When and what happened when you took this medication?” (anaphylaxis)
• “Have you taken that medication since, and what happened?”
• “Are you allergic to anything else?” (repetition)
NB: Patients assume GPs + hospitals have agreed accessible place for allergy lists
Additional Questions to Explore Effectiveness/Compliance
• “Are any of your tablets causing side effects?”
• “Have you changed the dose or stopped any medication because of unwanted effects?”
• “Do you sometimes stop taking your medicine whenever you feel better?”
• “Do you sometimes stop taking your medicine if it makes you feel worse?”

Patient Education
• Encourage ownership
• Educate patient to bring medication (or list) from home at each appointment, admission (prescription and OTC)
• Encourage family members/ cares to become involved
• Encourage one pharmacy, one GP etc
Introduction to Prescribing
What is Prescribing?
• Prescribing is part of a logical process, based on comprehensive and objective information
• Key part of Western Medicine
• It is not a knee-jerk reflex, a recipe from a cook-book (swelling ≠ LASIX)
• Ie identify cause of swelling (CCF = furosemide)
• Never a response to commercial pressure
Write legibly (prescribing is not a joke)
P-drugs
• A physician should develop a standard treatment for common disorders, resulting in a set of first-choice drugs, called p(ersonal)-drugs
• You should know these drugs inside out
• Do not deviate, whatever reps tell you

Some of my ‘P-drugs’
Group Name Dose Alternative Monitor
ACEi Ramipril 2.5-10 mg od Lisinopril K, Urea, creat
ARB Losartan 25-100 mg od Candesartan K, urea, creat
B-blocker Bisoprolol 2.5-10 mg od Atenolol Pulse rate
Loop diuretic Furosemide 40-250 mg od Bumetanide Na, K
Thiazide diuretic
Bendroflumeth-azide
2.5-5 mg od Hydrochlorothi-azide
Na, K
HMG-CoA Atorvastatin 10-80 mg od Simvastatin Muscle pain, CK
Basic Rules• All in front of BNF
• CAPITALS
• Generic (‘chocolate’) not trade name (not ‘Cadburys’)
• Black or blue pen
• Date (with year)
• Dose, frequency
• Duration (if necessary)
• ‘Name, rank, number’
• Clear signature (PRINT if necessary)
• Legible
Dose (1)
• Biggest cause of problems
• Know simple doses, ie why I prefer LOSARTAN 25-100 mg, rather
• And .. avoid combination drugs
Dose (2): Problems start
• Grams (g)
• Milligrams (mg) .. easy to confuse with ..
• Micrograms (DIGOXIN 0.25 mcg) vs mcg vs μcg
• Picograms (DIGOXIN 250 pcg)
• Answer (BNF): write ‘micrograms’ below the dose
• Eg ‘6
micrograms’
If you have to break open 40 bottles, “Houston .. We have a problem”
Drugs Written as Units
• Eg insulin, heparin
• Common cause of (sometimes) major problems (hypoglycaemia, bleeding)
• As ‘u’ can be confused as a ‘0’ increasing the dose 10 fold
• Answer (BNF): (like micrograms) write the word ‘unit’ under the dose
• Eg ‘6
units’

Frequency
• OD (1x day)
• BD (2x)
• TDS (3x)
• QDS (4x)
• If cannot remember Latin, keep it simple, eg 1x per day etc
• Beware odd frequencies, eg weekly
Duration
• 5/7 = 5 days (good default short course)
• 2/52 = 2 weeks
• 1/12 = 1 month
• But do patients understand ‘5/7’?

Mode
• PO = oral
• IV = intravenous (not ‘stronger’ than oral)
• IM = intramuscular
• SC = subcutaneous
• Other ..
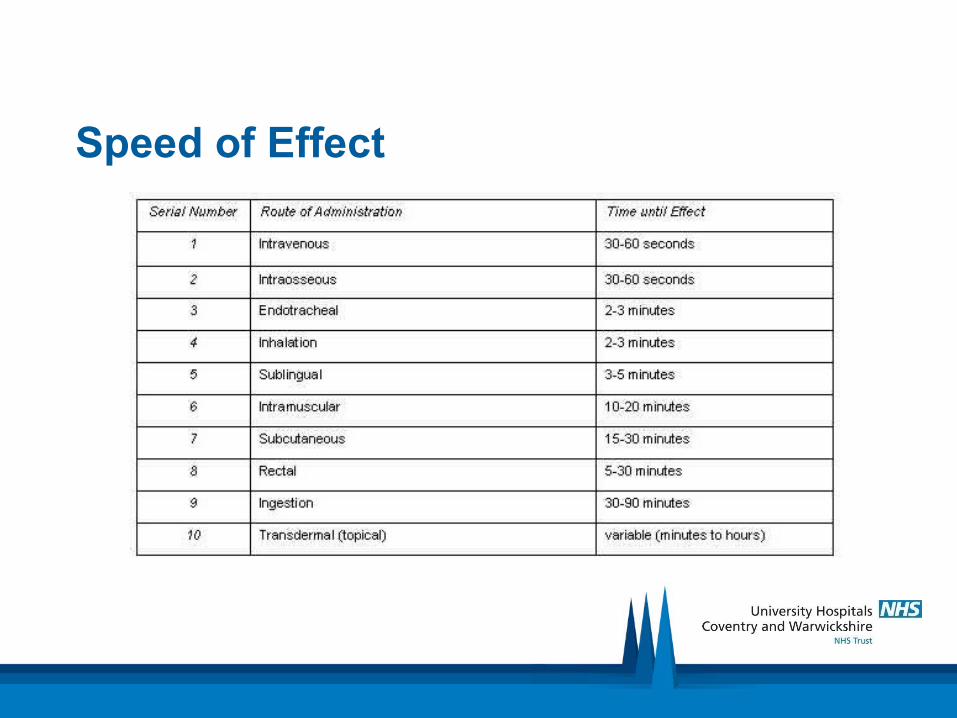
Speed of Effect
Side-effects
• Hard one
• Use BNF
• But .. the big BUT
• Know (and warn patient, preferably in writing) if:
• > 1%
• Serious, or serious to them (eg ciclosporin)

Inpatient: are drugs being given?
• Yes, you have to check
• Why, would they not be

Monitor
• Is it working?
• Compliance
.. how can you do that

Admendments to Standard Dosages (LO): Interactions)
• Very complicated
• Eg SIMVASTATIN 40 mg (20 mg if on VERAPAMIL/DILTIAZEM)
• Look them up

Admendments (LO): Elderly and Children
• Be careful
• If in doubt reduce dose and/or frequency
• Ask a senior

Admendments (LO):Renal, liver failure etc
• Many drugs are excreted by the kidney (eg digoxin) or liver so dose (esp maintenance) has to be reduced
• Other drugs are toxic to the kidney (aminoglycosides) or liver, so should be avoided, or used with caution
• Golden rule: if patient has renal or liver failure .. look it up
Admentments (LO):Pregnancy (two people)
• Its complicated
• Do not do it
• Ask someone more senior

Advice re how to look after medication
Stopping or changing dose of drug
• Just as dangerous as starting
• Who you are
• When
• Why stopping or changing
Don’t be afraid. Do something
• With all these ‘do’s and don’t’s, can be frightened to do anything
• If patient is unwell, do something
• Ask a senior, esp in F1/2 years
• Prescribing can be very therapeutic to you (eg furosemide in acute heart failure)
‘Where there is pus, let it out’
• Do you need to consider– Surgical option
– Radiological therapeutic option
• Don’t use prescribing to ‘treat a CRP’
• What is the cause of the raised CRP?
• Appendicectomy story ..
Factors that Influence Prescribing (LO)
• Knowledge
• Experience
• BNF and Local Formulary (next)
• Pharmaceutical industry (no)
• Cost (yes, esp GP)
• P-drugs
BNF and Local Formulary (LO)
• BNF says what can be prescribed in UK
• Licensed uses
• Local formulary (by Trust) will say what is recommended (should link to local guidelines)
• Look at via UHCW intranet (local one is within it)
• SWFT, George Eliot Hospitals, GPs and Psychiatry may have different formulary
• Look at Lothian, Wolverhampton formularies
BNF: Limitations (LO)
• Side-effects (what to mention to patient, first ever)
• Interactions (first ever)
• Cost
• More info: Manufacturer’s Summary Product Characteristics (SPC) via Google
BNF – ‘Yellow Forms’
• Side-effect profiles, interactions
• Would not exist without these .. and you
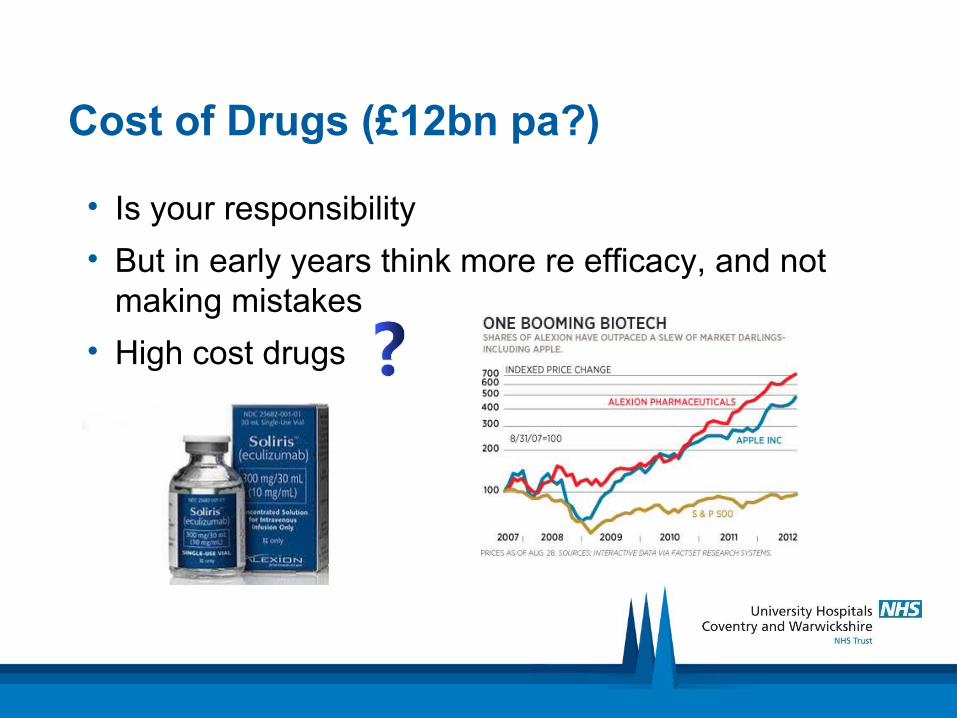
Cost of Drugs (£12bn pa?)
• Is your responsibility
• But in early years think more re efficacy, and not making mistakes
• High cost drugs

Cost of NHS

Cost of NHS Per Person Per Year
BNF - Demonstration
Quiz
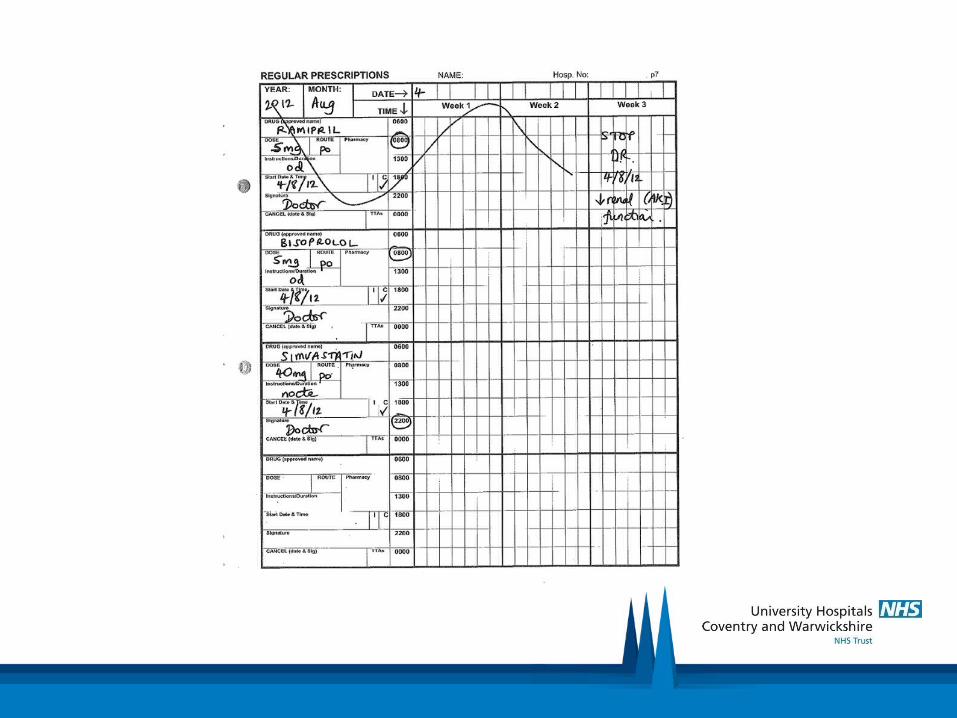
Quiz
• First drug chart: list ‘good’ things (and a couple less good)
• Second drug chart: list ‘poor’ things

Buy a Book
Use the Internet
• http://www.uhs.nhs.uk/Media/suhtideal/Doctors/SaferPrescribingWorkbook/Section1-Prescriptionwriting.pdf
Summary
• Drug history is a very important skill
• Prescribing is a central tenet of Western Medicine
• BNF and local formulary should be part of your daily life as a doctor
• “A good doctor (physician, surgeon, GP, psychiatrist etc) is a good pharmacologist (and more importantly) clinical prescriber”