Embed Size (px)
Citation preview

1
NORTH OF TYNE GUIDELINES FOR:
PRIMARY MANAGEMENT OF DRUG PRESCRIBING IN
NON-MALIGNANT PAIN
(EXCLUDING DETAILED RECOMMENDATIONS FOR LONG TERM
STRONG OPIATES)
February 2015 (minor update April 2017)

2
CONTENTS
Page Introduction 3
Patient information 3
How to use this guideline 3 Summary of primary management of drug prescribing in non-malignant pain 4 Additional notes 5 Appendices Appendix 1: Examples of drug titration regimens 6 Gabapentin, pregabalin and amitryptyline/duloxetine Appendix 2: Summary of drug costs 11
Appendix 3: Patient agreement form 12 Appendix 4: Summary of on line resources 13 Appendix 5: Membership of the guideline development group 14
Date of guideline and date of review

3
INTRODUCTION This guidance is intended only to inform prescribing of analgesic drugs in chronic non-malignant pain and has been developed as a consensus between representatives from primary and secondary care, with reference to national guidelines, including from NICE. It is intended to guide prescribing, but every patient should be assessed and managed individually. The underlying condition causing the pain should be managed in line with other relevant guidelines, the details of which are beyond the scope of this guideline. However, it was felt noteworthy to state that those with inflammatory joint disease with inflammation, should be considered for referral to a rheumatologist, as these patients may be treated with different NSAIDs, COX2 inhibitors, DMARDs and biologics for example. However, patients with chronic pain syndromes, without inflammation, should not generally be referred to a rheumatologist. The guideline is confined to analgesic drug prescribing, but any prescribing must be part of a clearly set out overall management plan, incorporating all aspects of care and using shared decision making with the patient. Other guidelines should be referred to as appropriate. In particular the local guideline group felt that the pathways in the Map of Medicine developed in collaboration with the British Pain Society should be considered to put this prescribing guideline into a framework of best practice, available at http://app.mapofmedicine.com/mom/58/index.html, and found under the department of medicine, under the specialist area of pain management. These include:
Chronic pelvic pain (for men and women)
Chronic widespread pain, including fibromyalgia
Complex regional pain syndrome
Initial assessment and early management of pain
Low back and radicular pain
Neuropathic pain This local guideline is not intended to inform prescribing in trigeminal neuralgia, in patients with malignant pain or in patients with a history of substance misuse. This guideline is intended for all clinicians in Newcastle, North Tyneside, and Northumberland who prescribe analgesic drugs. PATIENT INFORMATION There are many sources of patient information available, some of which are for individual causes of pain, for example back pain. In some cases a written plan developed with the patient may be helpful. The pain tool kit is available at http://www.paintoolkit.org/, and information about other patient information is included in appendix 4. The guideline group has not specifically endorsed a particular resource. Details for accessing a locally developed patient information leaflet for patients being treated with gabapentin and pregabalin are included in appendix 4. How to use the guideline The guideline includes summary flow chart which can be printed and laminated for easy reference if preferred, with notes for additional information. The BNF, SPCs and the Local Formularies should be referred to as appropriate.
4
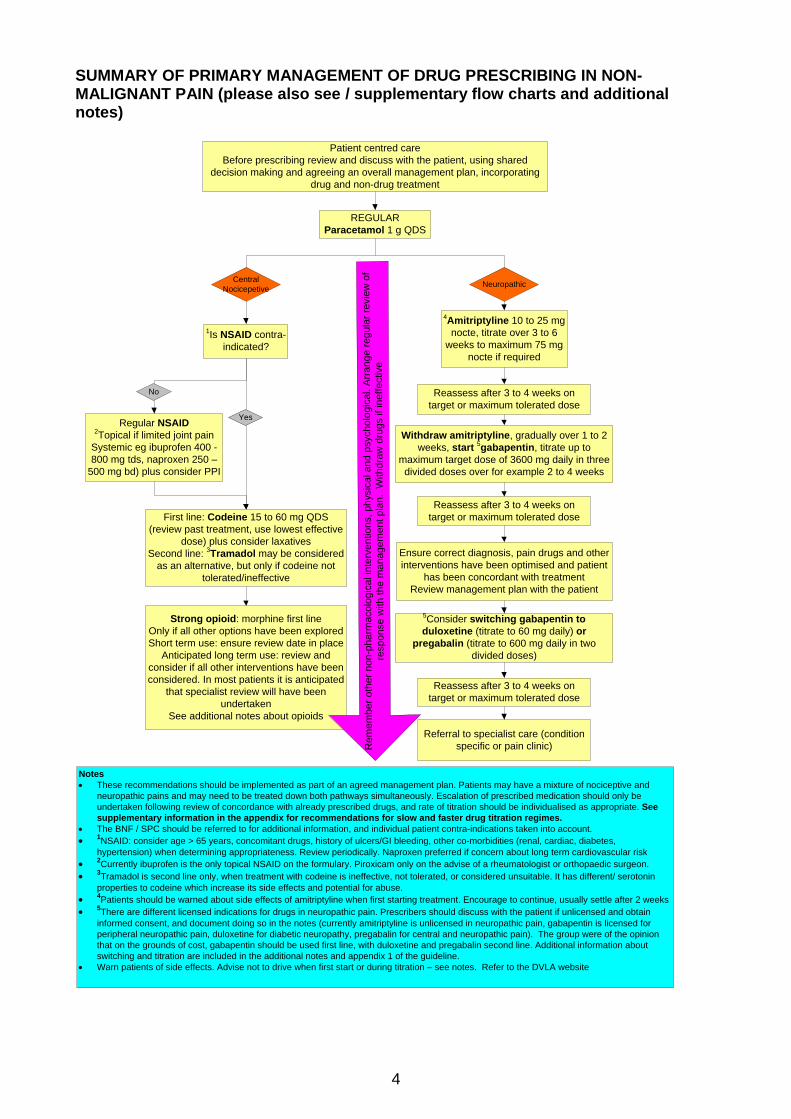
SUMMARY OF PRIMARY MANAGEMENT OF DRUG PRESCRIBING IN NON-MALIGNANT PAIN (please also see / supplementary flow charts and additional notes)
Patient centred care
Before prescribing review and discuss with the patient, using shared
decision making and agreeing an overall management plan, incorporating
drug and non-drug treatment
REGULAR
Paracetamol 1 g QDS
4Amitriptyline 10 to 25 mg
nocte, titrate over 3 to 6
weeks to maximum 75 mg
nocte if required
Regular NSAID2Topical if limited joint pain
Systemic eg ibuprofen 400 -
800 mg tds, naproxen 250 –
500 mg bd) plus consider PPI
First line: Codeine 15 to 60 mg QDS
(review past treatment, use lowest effective
dose) plus consider laxatives
Second line: 3Tramadol may be considered
as an alternative, but only if codeine not
tolerated/ineffective
1Is NSAID contra-
indicated?
Strong opioid: morphine first line
Only if all other options have been explored
Short term use: ensure review date in place
Anticipated long term use: review and
consider if all other interventions have been
considered. In most patients it is anticipated
that specialist review will have been
undertaken
See additional notes about opioids
Withdraw amitriptyline, gradually over 1 to 2
weeks, start 5gabapentin, titrate up to
maximum target dose of 3600 mg daily in three
divided doses over for example 2 to 4 weeks
Reassess after 3 to 4 weeks on
target or maximum tolerated dose
Reassess after 3 to 4 weeks on
target or maximum tolerated dose
Ensure correct diagnosis, pain drugs and other
interventions have been optimised and patient
has been concordant with treatment
Review management plan with the patient
5Consider switching gabapentin to
duloxetine (titrate to 60 mg daily) or
pregabalin (titrate to 600 mg daily in two
divided doses)
Referral to specialist care (condition
specific or pain clinic)Re
me
mb
er
oth
er
no
n-p
ha
rma
co
log
ica
l in
terv
en
tio
ns,
ph
ysic
al a
nd
psych
olo
gic
al. A
rra
ng
e r
eg
ula
r re
vie
w o
f
resp
on
se
with
th
e m
an
ag
em
en
t p
lan
. W
ith
dra
w d
rug
s if in
effe
ctive
Notes
These recommendations should be implemented as part of an agreed management plan. Patients may have a mixture of nociceptive and
neuropathic pains and may need to be treated down both pathways simultaneously. Escalation of prescribed medication should only be
undertaken following review of concordance with already prescribed drugs, and rate of titration should be individualised as appropriate. See
supplementary information in the appendix for recommendations for slow and faster drug titration regimes.
The BNF / SPC should be referred to for additional information, and individual patient contra-indications taken into account.
1NSAID: consider age > 65 years, concomitant drugs, history of ulcers/GI bleeding, other co-morbidities (renal, cardiac, diabetes,
hypertension) when determining appropriateness. Review periodically. Naproxen preferred if concern about long term cardiovascular risk
2Currently ibuprofen is the only topical NSAID on the formulary. Piroxicam only on the advise of a rheumatologist or orthopaedic surgeon.
3Tramadol is second line only, when treatment with codeine is ineffective, not tolerated, or considered unsuitable. It has different/ serotonin
properties to codeine which increase its side effects and potential for abuse.
4Patients should be warned about side effects of amitriptyline when first starting treatment. Encourage to continue, usually settle after 2 weeks
5There are different licensed indications for drugs in neuropathic pain. Prescribers should discuss with the patient if unlicensed and obtain
informed consent, and document doing so in the notes (currently amitriptyline is unlicensed in neuropathic pain, gabapentin is licensed for
peripheral neuropathic pain, duloxetine for diabetic neuropathy, pregabalin for central and neuropathic pain). The group were of the opinion
that on the grounds of cost, gabapentin should be used first line, with duloxetine and pregabalin second line. Additional information about
switching and titration are included in the additional notes and appendix 1 of the guideline.
Warn patients of side effects. Advise not to drive when first start or during titration – see notes. Refer to the DVLA website
Central
NocicepetiveNeuropathic
No
Yes
Reassess after 3 to 4 weeks on
target or maximum tolerated dose

5
ADDITIONAL NOTES
1. Patients prescribed analgesic drugs should receive appropriate advice about driving. It is an offence for patients to drive or attempt to drive when unfit to do so due to drugs, this includes prescribed medication. Some analgesic drugs can cause drowsiness and impaired judgement and patients should be advised not to drive if they feel unfit to do so. A new offence of driving with certain specified controlled drugs in excess of specified levels in the body is expected to come into force on 2 March 2015. Particular care should be taken when drugs are first initiated and or titrated. For further information refer to the DVLA website https://www.gov.uk/government/publications/at-a-glance. 2. Prescribing should take into account any co-morbidities and need for dose adjustments or if drugs are contra-indicated eg gabapentin and pregabalin dose adjustment required in renal impairment, duloxetine is contra-indicated in hepatic impairment. The BNF and SPC for individual drugs should always be referred to. 3. The rate at which drugs are titrated should be individualised, and particularly in the elderly, slower rates of titration should be considered. In general, drugs should not be overlapped if one is weaned down and another started. Treatment should be individualised, but suggested drug titration regimens are included in the appendix. 4. Co-codamol is not included in the flow chart and its use is discouraged, due inflexibility of dosing, and paracetamol and codeine should be prescribed separately. If cocodamol is used, this should be in tablet form, not the effervescent preparation which has a high salt content. 5. Codeine is preferred to dihydrocodeine, as dihydrocodeine which is on the formulary restricted for use in breast feeding mothers (either alone or when taken in combination with paracetamol as codydramol) has a shorter half life and the effects are more likely to lead to abuse. However, both codeine and dihydrocodeine are associated with the risk of developing physical and psychological dependency and there should be arrangements for review when being prescribed. 6. If amitriptyline is not tolerated, other central antidepressant analgesics may be used, usually on advice from specialist care, but are not recommended routinely. Imipramine is the only other approved alternative on the North of Tyne formulary. 7. Nabilone is included on the local formulary for use as an analgesic drug in chronic pain (unlicensed) which has not responded to other treatments. Treatment should only be initiated by a pain consultant. 8. Initiation of strong opioids should only be considered when all other options have proved ineffective and after a review of concordance with other prescribed treatments. Morphine is first line and other agents such as oxycodone should only be considered in patients intolerant of morphine. If strong opioid use may be anything other than short term patients should have had specialist review, unless there are good reasons not to do so. 9. If there are concerns about the potential misuse of chronic pain drugs, a written and signed agreement with the patient should be considered. An example of such an agreement which practices may wish to adopt is included in the appendix.

6
Appendix 1
What dose of gabapentin should be used, and how should it be titrated?
Various dose titrations may be used for gabapentin, depending on the person taking it and how well they tolerate it. The speed of titration will vary among individuals and should be tailored to the individual. For example, elderly or frail people are more likely to experience adverse effects and will require slower titration [[NICE CKS 2014].
Examples of a fast dosing schedule and a slow dosing schedule are shown below, however the how to titrate the dose depends on the individual response to treatment
Fast titration (usually suitable for otherwise healthy younger adults)
Start with 300 mg once a day on day 1, then 300 mg twice a day on day 2, then 300 mg three times a day on day 3.
Alternatively, start with 300 mg three times a day on day 1, then increased according to response in steps of 300 mg (in 3 divided doses) every 2–3 days up to maximum of 3600 mg a day (1200 mg three times a day). [NICE CKS 2014]
The minimum time to reach a dose of 1800 mg/day is one week, to reach 2400 mg/day is a total of 2 weeks, and to reach 3600 mg/day is a total of 3 weeks. [Summary of Product Characteristics [Gabapentin SPC]
An example of a fast dosing schedule for otherwise healthy younger adults is shown below:
Example Fast Dosing Schedule for Gabapentin
Morning Midday Night Total daily
dose
Day 1 300mg 300mg
Day 2 300mg 300mg 600mg
Day3 300mg 300mg 300mg 900mg
Dose can be increased in 300mg increments every 2- 3 days until sufficient pain relief is
achieved or the maximum daily dose of 3600mg is reached e.g.
Day 6 300mg 300mg 600mg 1200mg
Day 9 600mg 300mg 600mg 1500mg
Day 12 600mg 600mg 600mg 1800mg
Day 15 600mg 600mg 900mg 2100mg
Day 18 900mg 600mg 900mg 2400mg
Day 21 900mg 900mg 900mg 2700mg
Day 24 900mg 900mg 1200mg 3000mg
Day 27 1200mg 900mg 1200mg 3300mg
Day 30 1200mg 1200mg 1200mg 3600mg
Maximum
dose
Slow dose titration (suitable if patient is elderly, frail or has experienced adverse effects with higher doses)
Start with 100 mg at night, increasing by 100 mg a day until pain is significantly reduced, intolerable adverse effects occur, or a maximum daily dosage of 3600 mg (1200 mg three times a day) is reached
If the person experiences adverse effects during daily titration, a slower titration (for example increasing the dose every 3–7 days) may help. (NICE CKS 2014)

7
Recommended dosage adjustment for gabapentin in people with renal impairment. Adjust the dose for people with renal impairment (see below) Consult the manufacturer's Summary of Product Characteristics if the person is undergoing haemodialysis
Dosage of Gabapentin in Adults Based on Renal Function
Creatinine Clearance
(ml/min)
Total Daily Dose (mg/day)
≥80 900-3600
50-79 600-1800
30-49 300-900
15-29 150b-600
<15c 150b-300
Data from NICE CKS
How long should a trial of treatment last? Consider trialling gabapentin for 3–8 weeks, with at least 2 weeks at the maximum tolerated
dose, before deciding it is not effective It may take several weeks to reach an effective dosage (usually 1200 mg to 3600 mg a
day). Onset of action may be seen as early as the second week of treatment with rapid titration, but the peak effect usually occurs about 2 weeks after a therapeutic dosage is achieved; therefore, an adequate trial may be 2 months or longer.
If gabapentin is not effective or not tolerated, discontinue treatment gradually over a minimum of 1 week [NICE CKS 2014].

8
What dose of pregabalin should be used, and how should it be titrated? NICE CKS suggest starting pregabalin treatment at 150 mg a day (given in two to three divided doses), If necessary, increase the dose after 3 to 7 days to 300 mg a day (given in two to three divided doses). The dose can be increased further if necessary to a maximum dose of 600 mg a day (given in two to three divided doses) after an additional 7-day interval [NICE CKS 2014]. It may be prudent to give the first dose at night:
Example Standard Dosing Schedule for Pregabalin
Morning Night Total daily dose
Day 1 75mg 75mg
Day 2 75mg 75mg 150mg (for 3
days)
Day3 75mg 75mg 150mg
Day 4 75mg 75mg 150mg
Day 5 75mg 150mg 225mg
Day 6 150mg 150mg 300mg
for 7 days
Day 13 150mg 300mg 450mg
Day 14 300mg 300mg 600mg
Maximum dose
A lower starting dose and a more conservative dosing schedule may be appropriate for some people, for example people who cannot initially tolerate 75 or 150 mg a day, or people with reduced renal function:
Example Slow Dosing Schedule for Pregabalin
Morning Night Total daily dose
Day 1 25mg 25mg (for 3 days)
Day 2 25mg
Day 3 25mg
Day 4 25mg 25mg 50mg for 7 days
Day 11 50mg 50mg 100mg for 7 days
Day 18 75mg 75mg 150mg for 7 days
Day 25 150mg 150mg 300mg for 7 days
Day 32 300mg 300mg 600mg
Maximum dose
Manufacturer’s recommended dosage adjustment for pregabalin in people with renal impairment. The manufacturer’s Summary of Product Characteristics recommends the following maximum staring and total daily doses of pregabalin, depending upon renal function:
Dosage of Pregabalin in Adults Based on Renal Function
Creatinine Clearance
(ml/min)
Starting dose (mg/day) Maximum Daily Dose (mg/day)
30-60 75mg (divided doses) 300mg
15-29 25–50 mg (as one daily
dose or divided in two
doses)
300 mg (divided in two or three
doses)
<15 25 mg once a day 75 mg once a day

9
Seek specialist advice and consult the manufacturer's Summary of Product Characteristics for use in people undergoing haemodialysis [SPC Pregabalin] How long should a trial of treatment last?
Consider trialling pregabalin for 4 weeks before deciding it is not effective. If pregabalin is not effective or not tolerated, discontinue treatment gradually over a
minimum of 1 week [NICE CKS 2014].

10
Amitriptyline and Duloxetine
Amitriptyline What dose of amitriptyline should be used, and how should it be titrated? Start with 10 mg a day (taken at night) and gradually titrate up to an effective dose or the person's maximum tolerated dose (no higher than 75 mg a day) [NICE CKS 2014]
Example Dosing Schedule for Amitriptyline
Step 1 10mg at night for 1 week
Step 2 20mg at night for 1 week
Evaluate response
Step 3 30mg at night
Step 4 if dose tolerated and increase required 40mg at night
Step 5 if dose tolerated and increase required 50mg at night
Maximum dose is 75mg at night
How long should a trial of treatment last?
Consider trialling amitriptyline for 6–8 weeks, with at least 2 weeks at the maximum tolerated dose, before deciding it is not effective
If no improvement is seen with 75 mg a day, consider seeking specialist advice or switching to a different drug. Dosages higher than 75 mg a day could be considered in consultation with a specialist pain service.
If amitriptyline is not effective or not tolerated, discontinue treatment gradually over a minimum of 4 weeks to prevent discontinuation symptoms (such as dizziness, nausea, paraesthesiae, anxiety, diarrhoea, flu-like symptoms, and headaches) [NICE CKS 2014]
~~~~~~~~~~~~~~~~~~~~~~~~~~
Duloxetine What dose of duloxetine should be used, and how should it be titrated?
Start duloxetine treatment at 60 mg a day. If necessary, increase the dose up to a maximum of 120 mg a day (in two divided doses).
No dosage adjustment is necessary for people with mild or moderate renal dysfunction (creatinine clearance 30 to 80 mL/minute [NICE CKS 2014]
A lower starting dose of 30mg may be appropriate as nausea may occur on initiation If insomnia is an issue, it would be prudent to avoid night-time dosing
How long should a trial of treatment last? Consider trialling duloxetine for up to 8 weeks before deciding it is not effective. Additional response after 8 weeks is unlikely Reassess treatment at least every three months If duloxetine is not effective or not tolerated, discontinue treatment gradually over a
minimum of 1 to 2 weeks in order to reduce the risk of withdrawal reactions [NICE CKS 2014]

11
Appendix 2 Summary of drug costs – April 2017 Drug Tariff
Gabapentin caps 100mg 100 = £1.79 Gabapentin caps 300mg 100 = £2.60 Gabapentin caps 400mg 100 = £3.01 Gabapentin tabs 600mg 100 = £7.45 Gabapentin tabs 800mg 100 = £29.39 Pregabalin 25mg 100 = £115.00 Pregabalin 50mg 100 = £115.00 Pregabalin 75 mg 100 = £115.00 Pregabalin 100 mg 100 = £115.00 Pregabalin 150 mg 100 = £115.00 Pregabalin 200 mg 100 = £115.00 Pregabalin 225 mg 100 = £115.00 Pregabalin 300 mg 100 = £115.00 Amitryptyline 10mg 100 = £3.32 Amitriptyline 25mg 100 = £3.21 Amitryptyline 50mg 100 = £10.71 Duloxetine 30mg 100 = £7.07 Duloxetine 60mg 100 = £7.57
12
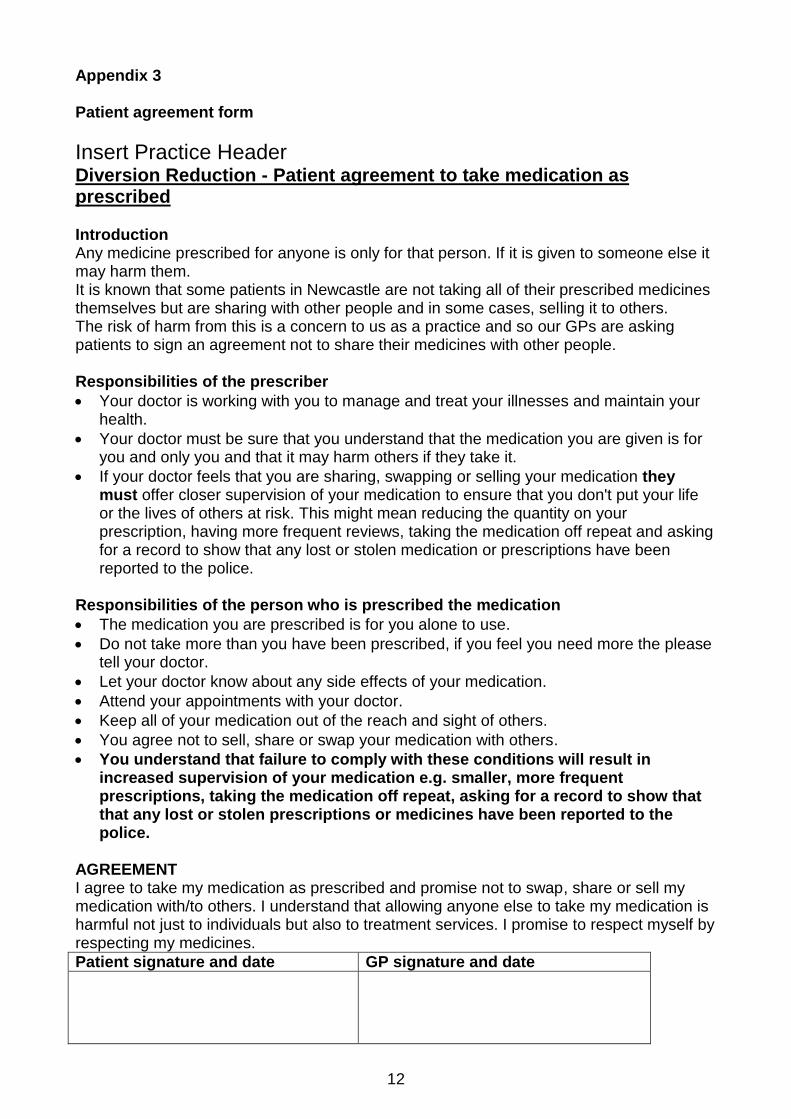
Appendix 3
Patient agreement form
Insert Practice Header Diversion Reduction - Patient agreement to take medication as prescribed Introduction Any medicine prescribed for anyone is only for that person. If it is given to someone else it may harm them. It is known that some patients in Newcastle are not taking all of their prescribed medicines themselves but are sharing with other people and in some cases, selling it to others. The risk of harm from this is a concern to us as a practice and so our GPs are asking patients to sign an agreement not to share their medicines with other people. Responsibilities of the prescriber
Your doctor is working with you to manage and treat your illnesses and maintain your health.
Your doctor must be sure that you understand that the medication you are given is for you and only you and that it may harm others if they take it.
If your doctor feels that you are sharing, swapping or selling your medication they must offer closer supervision of your medication to ensure that you don't put your life or the lives of others at risk. This might mean reducing the quantity on your prescription, having more frequent reviews, taking the medication off repeat and asking for a record to show that any lost or stolen medication or prescriptions have been reported to the police.
Responsibilities of the person who is prescribed the medication
The medication you are prescribed is for you alone to use.
Do not take more than you have been prescribed, if you feel you need more the please tell your doctor.
Let your doctor know about any side effects of your medication.
Attend your appointments with your doctor.
Keep all of your medication out of the reach and sight of others.
You agree not to sell, share or swap your medication with others.
You understand that failure to comply with these conditions will result in increased supervision of your medication e.g. smaller, more frequent prescriptions, taking the medication off repeat, asking for a record to show that that any lost or stolen prescriptions or medicines have been reported to the police.
AGREEMENT I agree to take my medication as prescribed and promise not to swap, share or sell my medication with/to others. I understand that allowing anyone else to take my medication is harmful not just to individuals but also to treatment services. I promise to respect myself by respecting my medicines.
Patient signature and date GP signature and date
13
Appendix 4
Summary of some on line resources which may be of interest Map of medicine: http://app.mapofmedicine.com/mom/58/index.html Pain tool kit: http://www.paintoolkit.org/ Local patient information leaflet for gabapentin and pregabalin: link on local website to be added Faculty of Pain Medicine patient information leaflets for amitryptyline, duloxetine, gabapentin, pregabalin available at http://www.rcoa.ac.uk/faculty-of-pain-medicine/patient-information and https://www.britishpainsociety.org/british-pain-society-publications/patient-publications/ DVLA information: https://www.gov.uk/government/publications/at-a-glance. Drugs and driving: Guidance from the Department of Transport and Patient Information Leaflet http://www.mhra.gov.uk/Safetyinformation/DrugSafetyUpdate/CON462303 Pregabalin and gabapentin: advice for prescribers on the risk of misuse https://www.gov.uk/government/publications/pregabalin-and-gabapentin-advice-for-prescribers-on-the-risk-of-misuse NHSE advice about generic / branded pregabalin available at http://www.england.nhs.uk/wp-content/uploads/2015/03/pregabalin-guidance.pdf

14
Appendix 5 Membership of the guideline development group Dr J Skinner, Consultant Community Cardiologist / Clinical Director for Community Services (guideline co-ordinator), The Newcastle upon Tyne Hospitals NHS Foundation Trust Dr C Coe, Consultant in Pain Management, Northumbria Healthcare NHS Foundation Trust Dr H Coundon, GP, North Tyneside CCG Mr Neil Frankland, Medicines Optimisation Pharmacist, NECS Ms Anne Henry, Medicines Optimisation Pharmacist, NECS Dr C Hodgkinson, GP, Newcastle North and East CCG Mr M Lowery, Formulary Pharmacist, The Newcastle upon Tyne Hospitals NHS Foundation Trust Ms C Miller, Pharmacist, Northumbria Healthcare NHS Foundation Trust (represented partly by Ms C Copeland) Dr J Warrington, GP, Northumberland CCG Dr N Weaver, GP, Newcastle West CCG Dr Paul Wilkinson, Consultant in Pain Management, The Newcastle upon Tyne Hospitals NHS Foundation Trust And circulated for comments to: Dr S Bennett, Consultant Diabetologist, Northumbria Healthcare NHS Foundation Trust Dr M Groves, Consultant Rheumatologist, Northumbria Healthcare NHS Foundation Trust Dr L Kay, Consultant Rhematologist, The Newcastle upon Tyne Hospitals NHS Foundation Trust Dr N Leech, Consultant Diabetologist, The Newcastle upon Tyne Hospitals NHS Foundation Trust Conflicts of interest PW has in the past given talks for GPs and judged the Grunenthal Innovation awards for which he has received honoraria from Pfizer and Grunenthal. Date and date of review February 2015, review February 2018

15





























