Embed Size (px)
Citation preview

By- Dr. Armaan SinghBy- Dr. Armaan Singh
Classification & Detail Info. Classification & Detail Info. {PPT.}{PPT.} of of Bones and JointsBones and Joints

Bone

CORTICAL BONE
• Dense, hard bone found in cortex
• Three quarters of skeletal tissue
• High mineral content
Carter & Hayes, 1976

• Stiffer than cancellous
• Withstands greater stress, less strain
• Fractures when strain exceeds
2% Carter & Hayes, 1976
Cortical Bone

• Low surface area
• Porosity 5-30%
• Slow metabolic rate
• Develops in line of stress
Einhorn,1996
Cortical Bone

TIBIA
• The shaft of the tibia is mainly compact bone
• A central medullary cavity containing mainly fat
• The ends are compact bone
• With an inner core of cancellous bone
• The periosteum is the vascular fibrous connective tissue investing bone

TRABECULAR OR CANCELLOUS BONE
• Found inside cortical shell e.g. Vertebrae
• Consists of horizontal and vertical plates
• Spaces are filled with bone marrow
• Large surface area
• Porosity is between 30-90%

• Greater capacity to store energy
• In vitro fractures at strains >75%
• Metabolically more active
• More sensitive to changes in endocrine hormones
Carter & Hayes,1976; Einhorn, 1996
Trabecular or Cancellous Bone

• Compressive strength is proportional to the square of the apparent density
• Small changes in density
• Large change in strength
Dalen et al., 1976
Cancellous Bone

• Organic matrix
• Type I collagen forms 90% of skeletal weight
• Mineral hydroxyapatite ratio
• Calcium 10
• Phosphate 6
• Carbonate 1
Bone

BONE REMODELLING
• Bone is a living tissue
• Osteoclastic activity i.e. bone resorption takes only few days
• Osteoblastic or bone formation takes several months

Bone Remodelling

Quiescence
Activation
Resorption
Formation
Quiescence
Normal bone turnover
Osteoporotic bone turnover
osteocytes
bone
osteoblastosteoidnew bone
osteoclast
D1202
Phases of Bone Remodelling

A HEALTHY SKELETON DEPENDS ON A BALANCED RANK LIGAND:
OPG RATIO
Prevents Bone Loss
RANK Ligand
OPG
Increases Bone Loss
RANK
Ligand
OPG
RANK Ligand
OPG

A HEALTHY SKELETON REQUIRES A BALANCE OF BONE RESORPTION AND FORMATION
Resting Reversal
Activation
Adapted from Baron, R. General Principles of Bone Biology. In: Primer on the Metabolic Bone Diseases and Disorders of Mineral Metabolism. Favus MJ (Ed.) 5th Edition. American Society for Bone and Mineral Research, Washington DC, 2003: 1–8
When bone turnover is increased, bone loss
dominates
Formation: 3 months
Resorption: 10 days
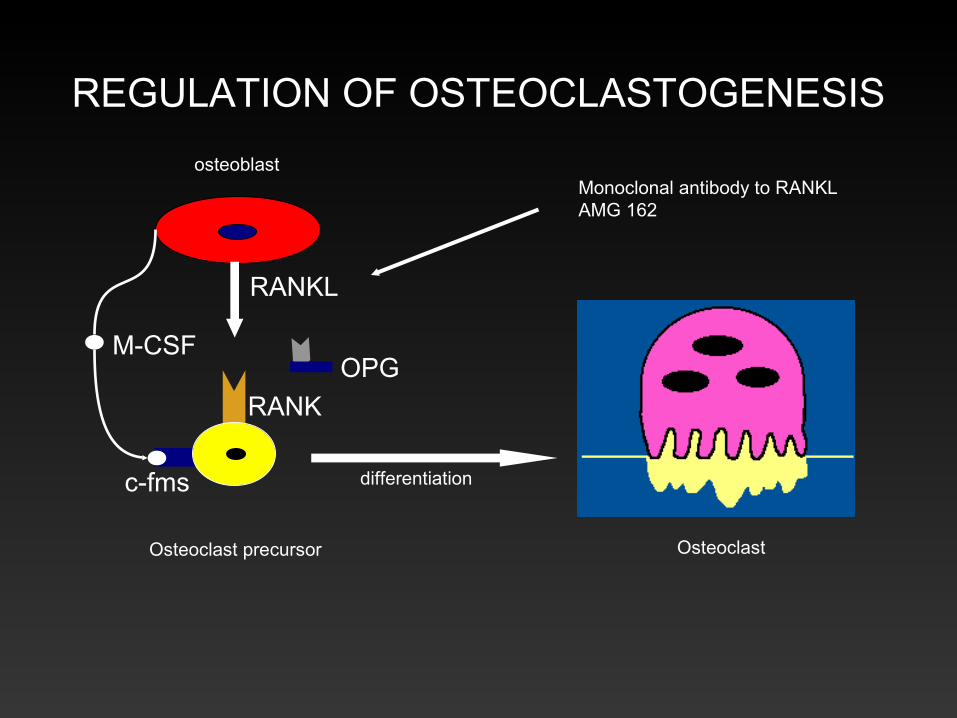
REGULATION OF OSTEOCLASTOGENESIS
Osteoclast precursor
osteoblast
Osteoclast
RANKL
OPG
RANK
c-fms
M-CSF
differentiation
Monoclonal antibody to RANKLAMG 162

Bones Require
• Normal hormones
• Adequate calories
• Particular protein
• Calcium
• Vitamin D
• Regular weight bearing
• Exercise
Bone

• The rate of turnover is determined by hormonal and local factors
Bone

Four Mechanisms of Bone Mass Regulation

• Changes in bone function lead to changes in bone
• Bone is laid down where needed
• Bone is resorbed where it is not needed
Wolff, 1892
Wolff’s Law
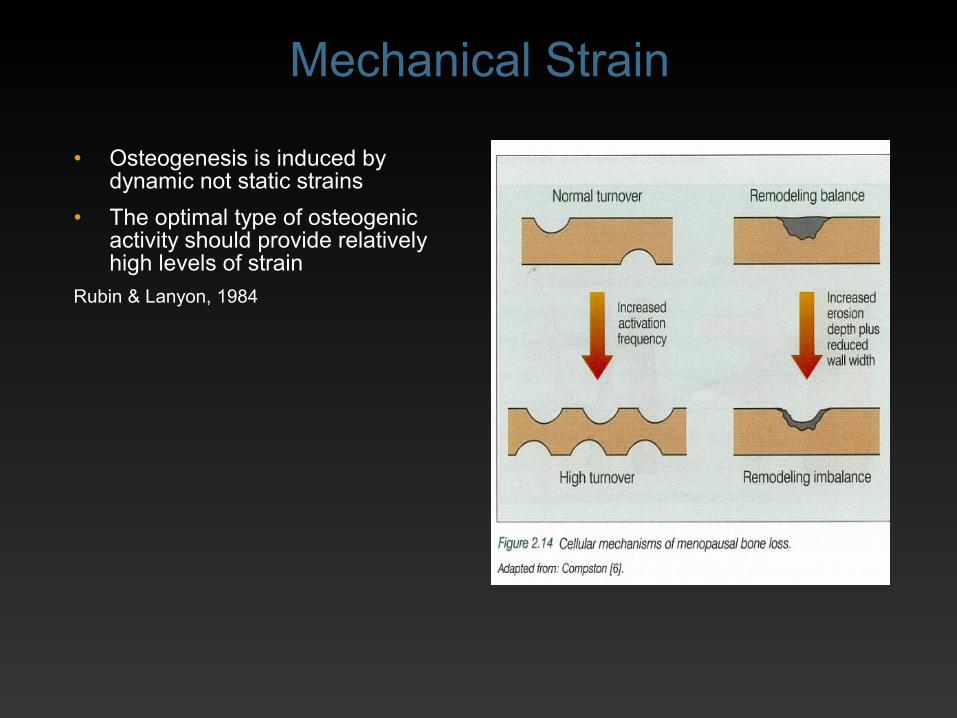
• Osteogenesis is induced by dynamic not static strains
• The optimal type of osteogenic activity should provide relatively high levels of strain
Rubin & Lanyon, 1984
Mechanical Strain

• Tensile forces result in osteoclastic activity
• On the convex side of an angulated bone
• Compressive force results in osteoblastic activity on concave side
Bone

Bones require
• Normal hormones
• Adequate calories
• Particularly protein
• Calcium
• Vitamin D
• Regular weight bearing exercise
Bone
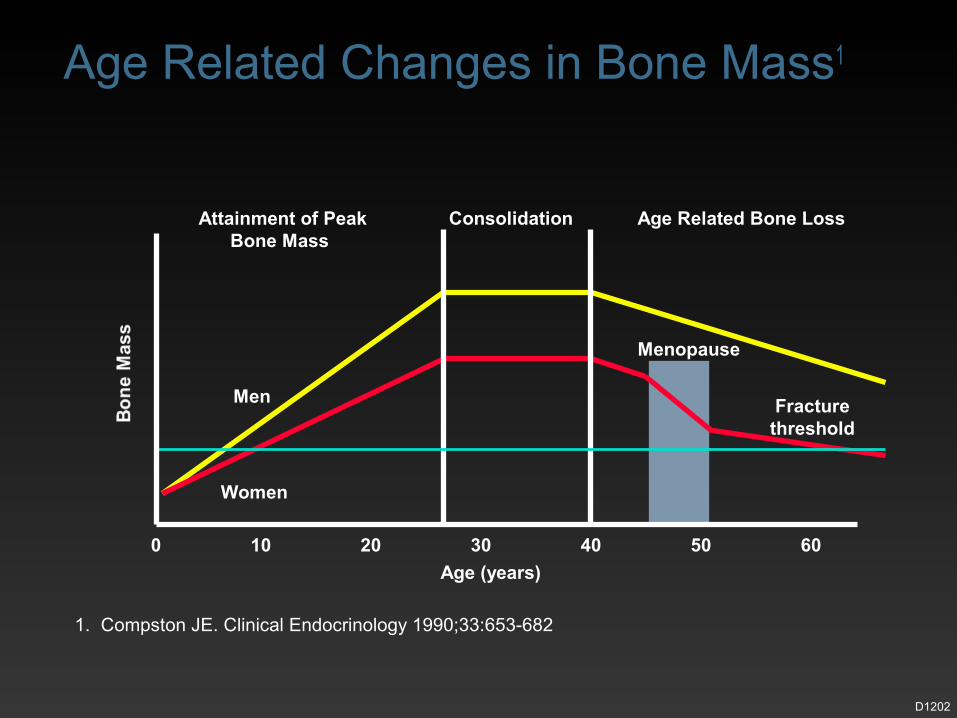
Age (years)
Attainment of Peak Bone Mass
Consolidation Age Related Bone Loss
Men
Women
Menopause
0 10 20 30 40 50 60
Fracturethreshold
1. Compston JE. Clinical Endocrinology 1990;33:653-682
D1202
Age Related Changes in Bone Mass1

PEAK BONE MASS• Genetic
• Environmental factors
• Mechanical strain
• Hormones

PEAK BONE MASS• Weight bearing activity during
adolescence and early adulthood was a far more important predictor of peak bone mass than calcium intake
Welten et al., 1994

LOW PEAK BONE MASS• Growing bone has a greater capacity to
add new bone to skeleton than mature bone
Forwood & Burr, 1993
OSTEOGENESIS• Muscle action is main stimulus for
bone formation
• Mechanical force
• Weight bearing
Birge et al., 1968

CLASSIFICATION OF BONESBy Shape
• Long
• Short
• Flat
• Irregular
• Sesamoid
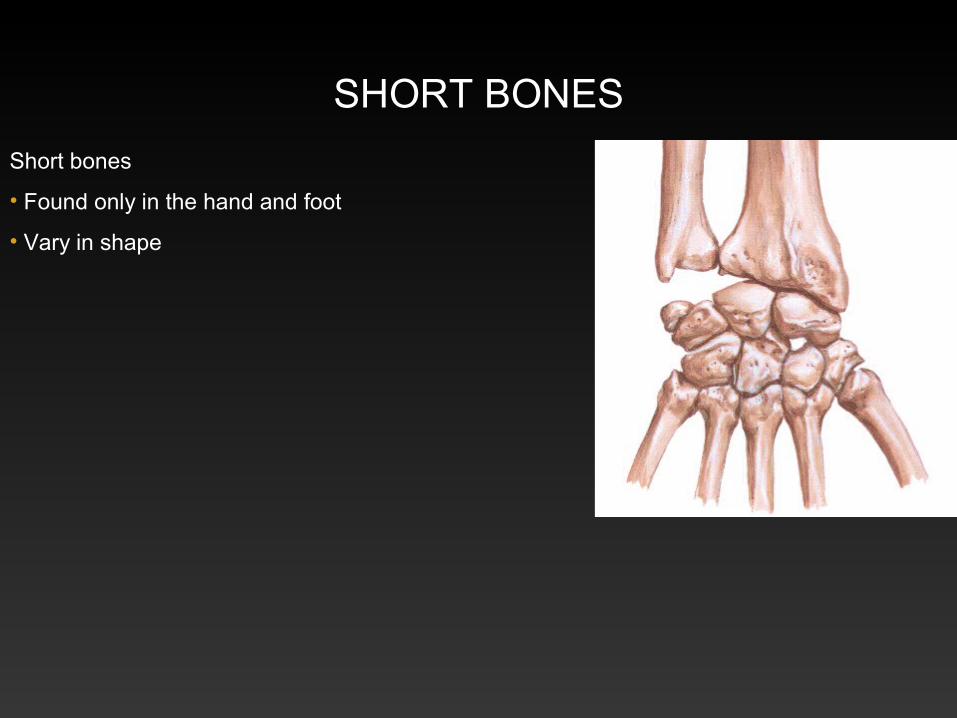
SHORT BONES
Short bones
• Found only in the hand and foot
• Vary in shape
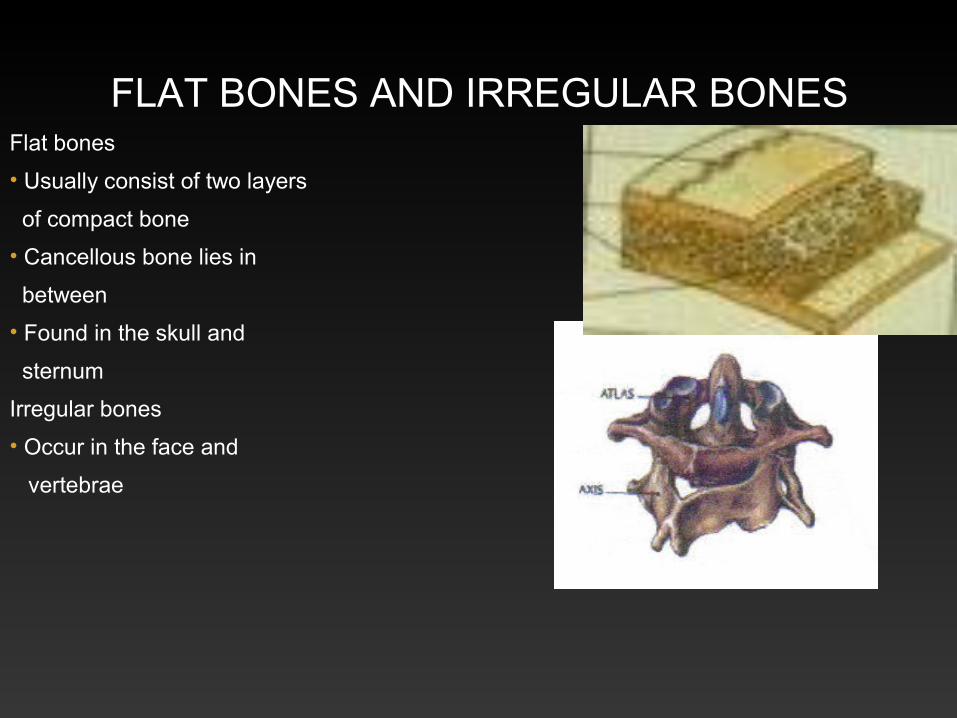
FLAT BONES AND IRREGULAR BONESFlat bones
• Usually consist of two layers
of compact bone
• Cancellous bone lies in
between
• Found in the skull and
sternum
Irregular bones
• Occur in the face and
vertebrae

SESAMOID BONESSesamoid bones
• Develop in tendons where
they cross bone
• Or articular surfaces,
patella
• Sesamoids in relation to
thumb and hallux
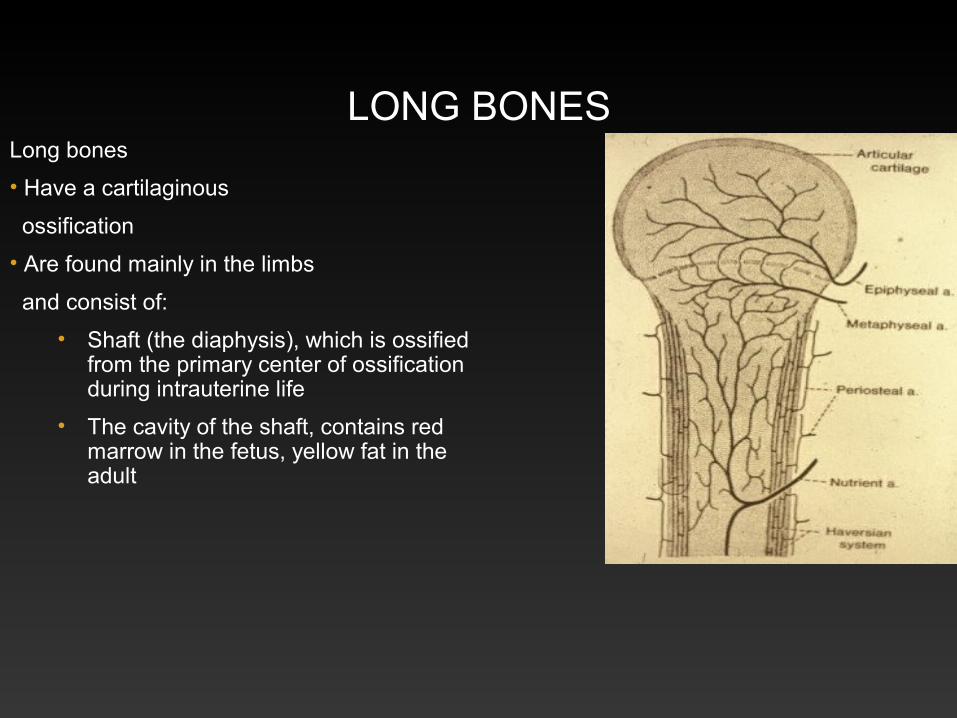
LONG BONESLong bones
• Have a cartilaginous
ossification
• Are found mainly in the limbs
and consist of:
• Shaft (the diaphysis), which is ossified from the primary center of ossification during intrauterine life
• The cavity of the shaft, contains red marrow in the fetus, yellow fat in the adult

BONE GROWTH• Diaphysis: shaft ossified from primary
center of ossification which appears 6-8th week of intrauterine life
• Epiphysis: ossified from secondary center
• Growth plate is cartilage
• Injury of epiphysis affects growth

EPIPHYSIS• Is ossified from a secondary center of
ossification
• These usually appear shortly after birth
• Except for the lower end of the femur, which appears 9 months intrauterine life, just before birth
• Epiphysis unite with the diaphysis (shaft) from puberty to early twenties depending on the bone involved
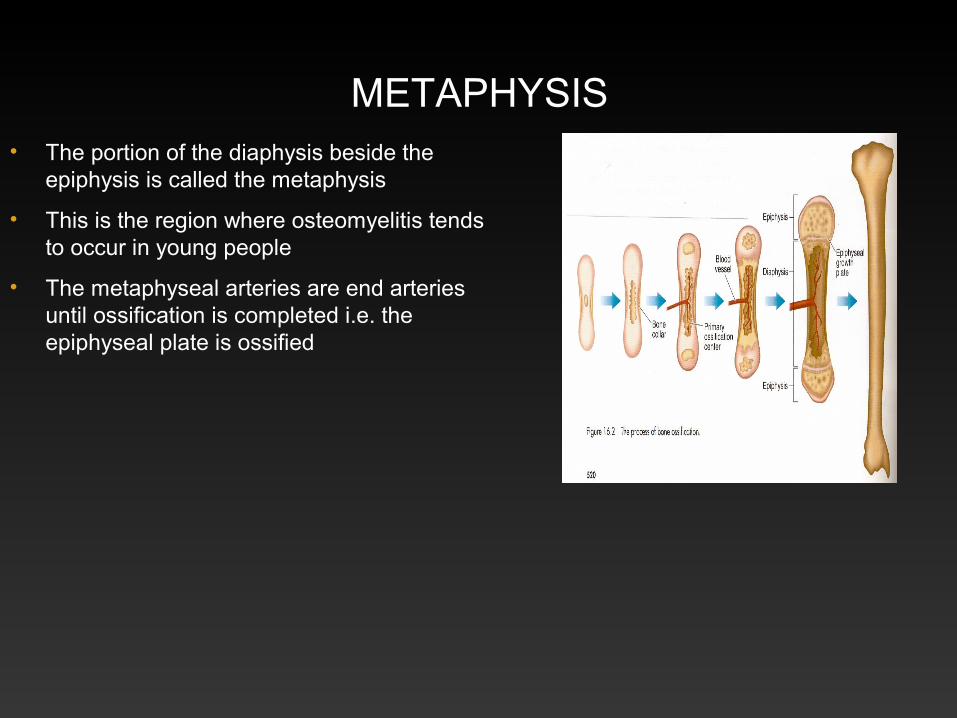
METAPHYSIS• The portion of the diaphysis beside the
epiphysis is called the metaphysis
• This is the region where osteomyelitis tends to occur in young people
• The metaphyseal arteries are end arteries until ossification is completed i.e. the epiphyseal plate is ossified
BONES
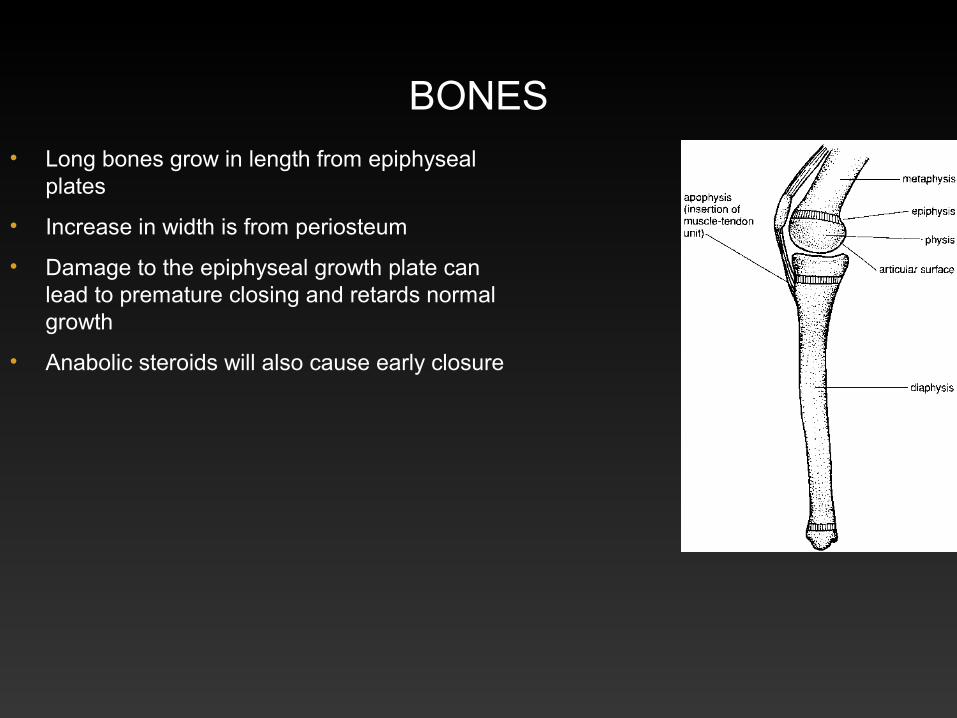
• Long bones grow in length from epiphyseal plates
• Increase in width is from periosteum
• Damage to the epiphyseal growth plate can lead to premature closing and retards normal growth
• Anabolic steroids will also cause early closure

EPIPHYSES
• Traction epiphyses
• The tibial tuberosity
• Osgood-Schlatters
• Medial epicondyle of the humerus, in ‘little league elbow’
• Compression epiphysis
• The distal end of the humerus

MUSCULOSKELETAL PROBLEMS
• Younger athletes
• Suffer many of the same injuries and illnesses as adults
• Differences is the structure of growing bone
Avulsed epiphysis

LESIONS WHICH AFFECT GROWTH PLATEArticular
• Perthes: femoral
• Kienbock: lunate
• Kohler: navicular
• Freiberg: 2nd metatarsal
• Osteochondritis dissecans
• Lateral aspect medial femoral condyle

EPIPHYSEAL INJURIES
• Shearing forces
• Avulsion forces
• Compression fractures
• Metaphyseal
• Growth plate
• Avulsion

GROWTH PLATE FRACTURESSALTER-HARRIS CLASSIFICATION
• Type 1 and type 2 heal well
• Type 3 and type 4 involve joint surface as well as growth plate
• Type 5 compression of growth plate
• Difficult to detect
• Growth ceases

BLOOD SUPPLY OF BONE
• Periosteal arteries enter bone at several points to supply the compact bone
• Nutrient arteries supply spongy bone and bone marrow

BLOOD SUPPLY OF BONE
• Periosteal arteries enter the bone at several points to supply the compact bone
• Nutrient arteries supply the spongy bone and bone marrow
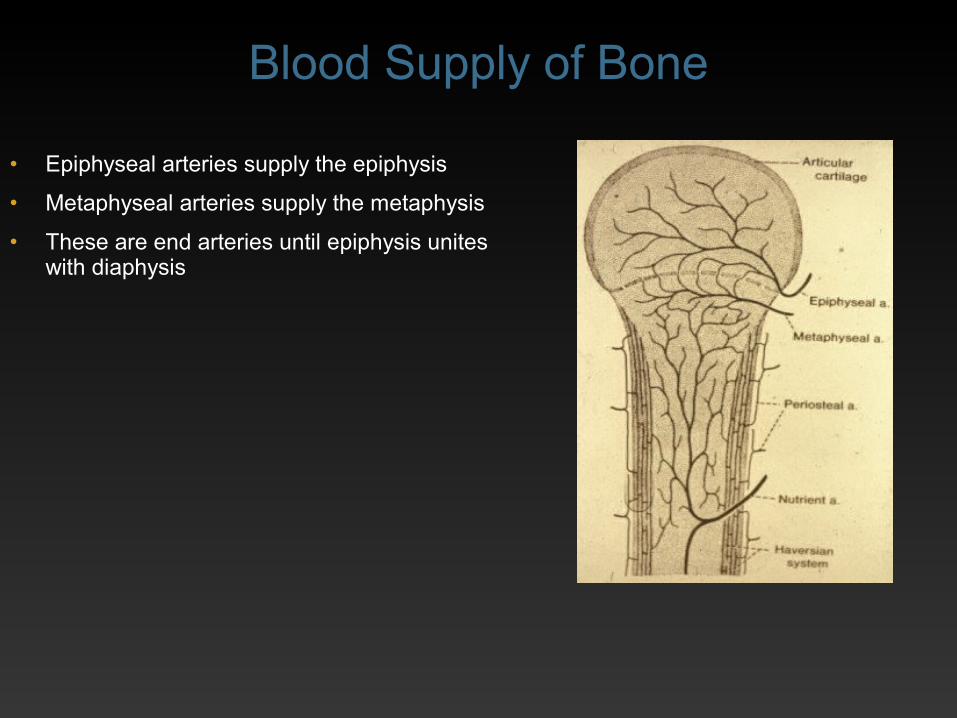
• Epiphyseal arteries supply the epiphysis
• Metaphyseal arteries supply the metaphysis

BLOOD SUPPLY OF BONE• Periosteal arteries occur particularly at the sites of
attachments of muscles and tendons
• If a group of muscles inserted into a bone is paralysed before puberty
• That bone will be shorter than the equivalent bone on the other side
• Due to reduced blood supply from the muscles involved
• The lack of stimulus to bone from lack of muscle contractions
• After puberty only muscle bulk is reduced
• Epiphyseal arteries supply the epiphysis
• Metaphyseal arteries supply the metaphysis
• These are end arteries until epiphysis unites with diaphysis
Blood Supply of Bone
AVASCULAR NECROSIS• Bones that have a large surface area covered
with articular cartilage tend to have a poorer blood supply
• Avascular necrosis occurs if blood supply is cut off due to fracture
• e.g. head of femur, due to fracture of neck of femur
• Proximal portion of the scaphoid
• Body of talus or dislocation e.g. lunate

APOPHYSIS• Tendon attachment to growth plate
• Traction injuries may occur
• Medial epicondylitis
• Limit numbers of pitches in baseball
• Osgood-Schlatters lesion of tibial tuberosity
• 12-16 year olds

AVULSION FRACTURES
Medial epicondyle
BONES IN CHILDREN
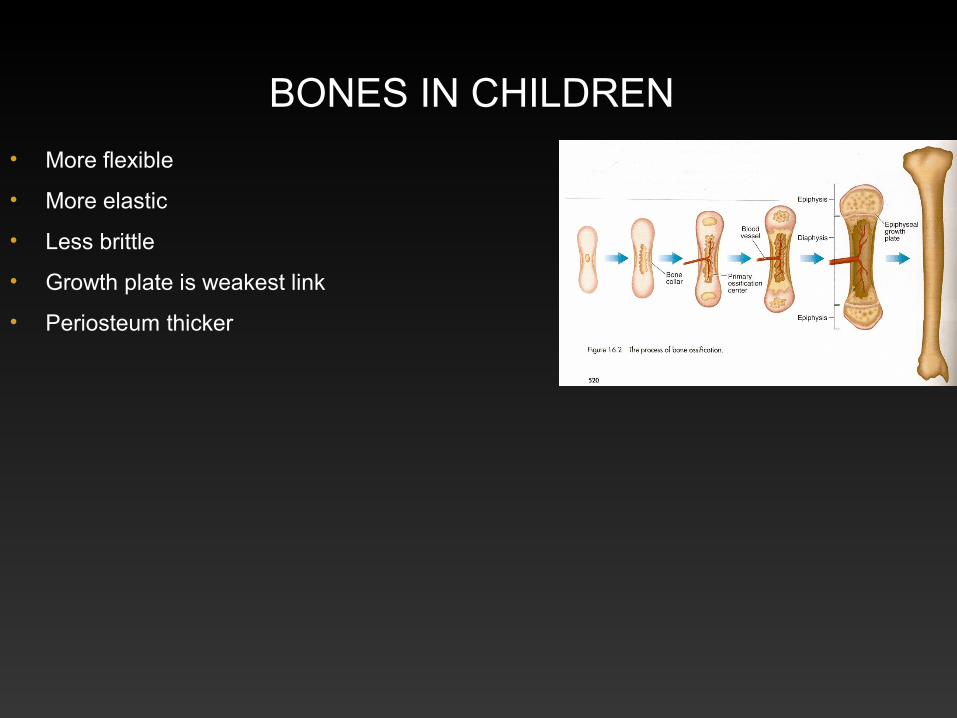
• More flexible
• More elastic
• Less brittle
• Growth plate is weakest link
• Periosteum thicker

• Articular cartilage thicker
• Junction between
• Metaphysis and epiphysis vulnerable
• Shearing forces
• Tendon attachment to apophysis weak
Bones in Children

EATING DISORDERSMay result in
• Delayed bone growth
• Delayed menarche
• Low peak bone mass
• Osteopenia or osteoporosis
• Increased musculo-skeletal problems

ARTICULAR CARTILAGE• The thickness of the cartilage
depends on the stress to which it is normally subjected
• Varies over the joint surface
• Patella has the thickest articular cartilage
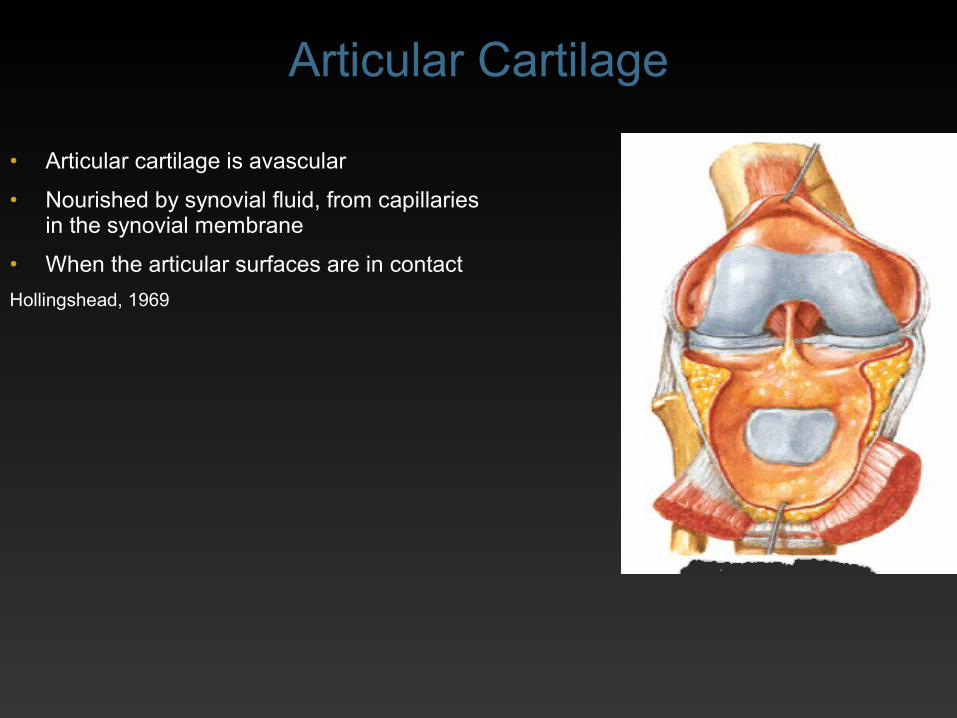
• Articular cartilage is avascular
• Nourished by synovial fluid, from capillaries in the synovial membrane
• When the articular surfaces are in contact
Hollingshead, 1969
Articular Cartilage

MUSCULOSKELETAL INJURIES
Extrinsic factors
• Sport
• Contact sports
• Environment
• Equipment
• Protective
• Overuse
Intrinsic factors
• Physical
• Physiological
• Psychological
• Previous injury

BONE PAIN• Osteomyelitis
• Tumour (night pain)
• Osteochondritis
• Rheumatoid arthritis

STRESS FRACTURESSTRESS FRACTURES• Biomechanical causes
• Training errors
• Athletic triad
• Amenorrhea
• Eating disorders
• Osteoporosisor osteopenia
• X-ray many times negative
• MRI is extremely sensitive
• Stress fracture of the femoral neck is potentially serious and need often surgery
JOINT
• Junction between two bones
• Function and movement depends
• Size and shape of articular surfaces
• Soft tissues surrounding the joint

RANGE OF JOINT MOVEMENT• Shape of articulating surfaces
• Restraint due to ligaments and muscles crossing joint
• Pain, weakness, spasm or contracture of muscles
• Bulk of adjacent soft tissue
• Impingement of bony surfaces
• Scarring of skin due to injury or burns

MUSCLES• Muscle can only act on a joint, if it crosses
the joint
• Muscles that have a common action on the joint tend to have same nerve supply
• Usually nerve of compartment gives an articular branch to joint
• Exception, flexors of the elbow, where median, ulnar and radial all give branches

CLASSIFICATION OF JOINTS• Fibrous
• Cartilaginous
• Primary and secondary
• Synovial

FIBROUS JOINTS
• Fibrous union
• Slight movement
• Gomphosis i.e. tooth and its socket
• Sutures
• Syndesmosis
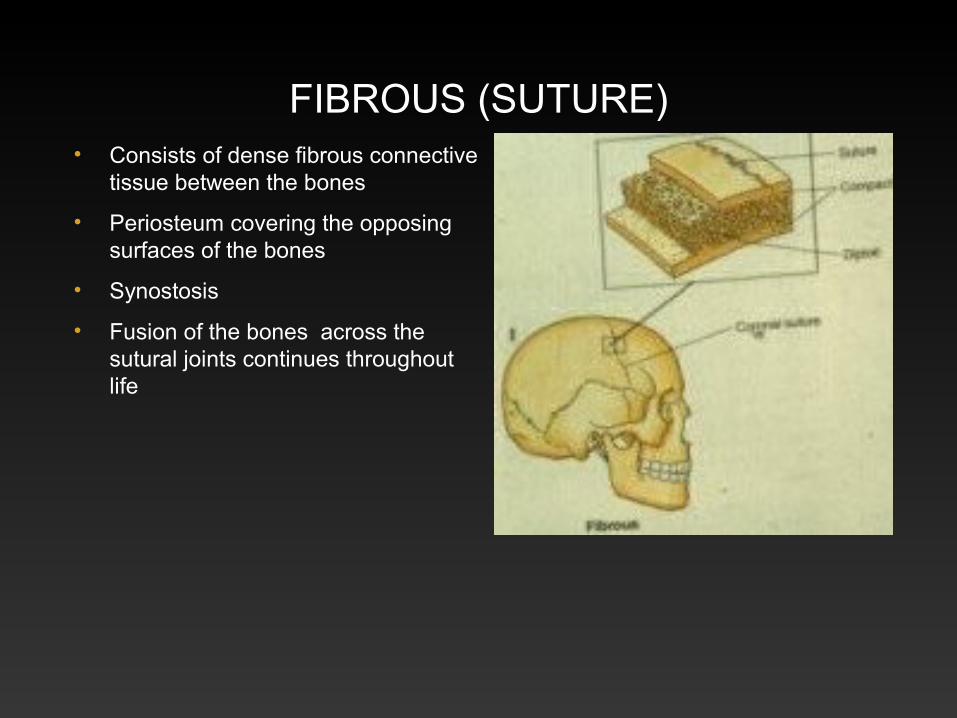
FIBROUS (SUTURE)• Consists of dense fibrous connective
tissue between the bones
• Periosteum covering the opposing surfaces of the bones
• Synostosis
• Fusion of the bones across the sutural joints continues throughout life

FIBROUS SYNDESMOSIS
• Interosseous membranes: radius and ulna, similar in lower limb and inferior tibio-fibular joint

PRIMARY CARTILAGINOUS• Cartilage continuous with bone
• No movement
• Rib and costal cartilage: costo-chondral joints
• First costal cartilage and sternum
• Diaphysis and epiphysis
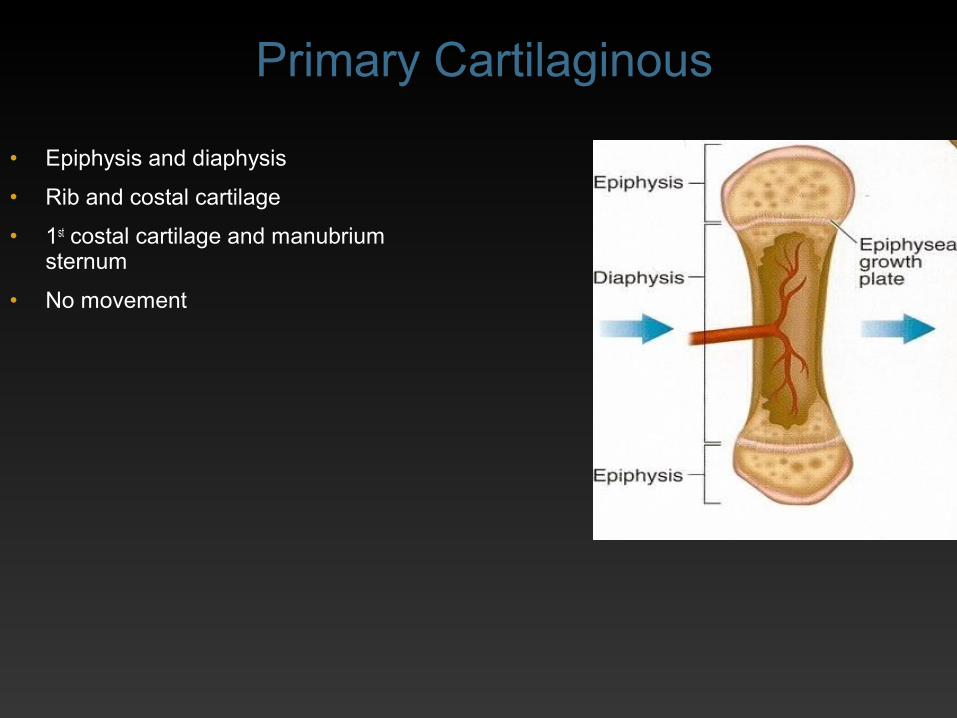
• Epiphysis and diaphysis
• Rib and costal cartilage
• 1st costal cartilage and manubrium sternum
• No movement
Primary Cartilaginous

• Epiphysis and diaphysis
Primary Cartilaginous

SECONDARY CARTILAGINOUS• Hyaline cartilage
• Disc of fibro-cartilage
• Mid line joints
• Very little movement
• Intervertebral discs
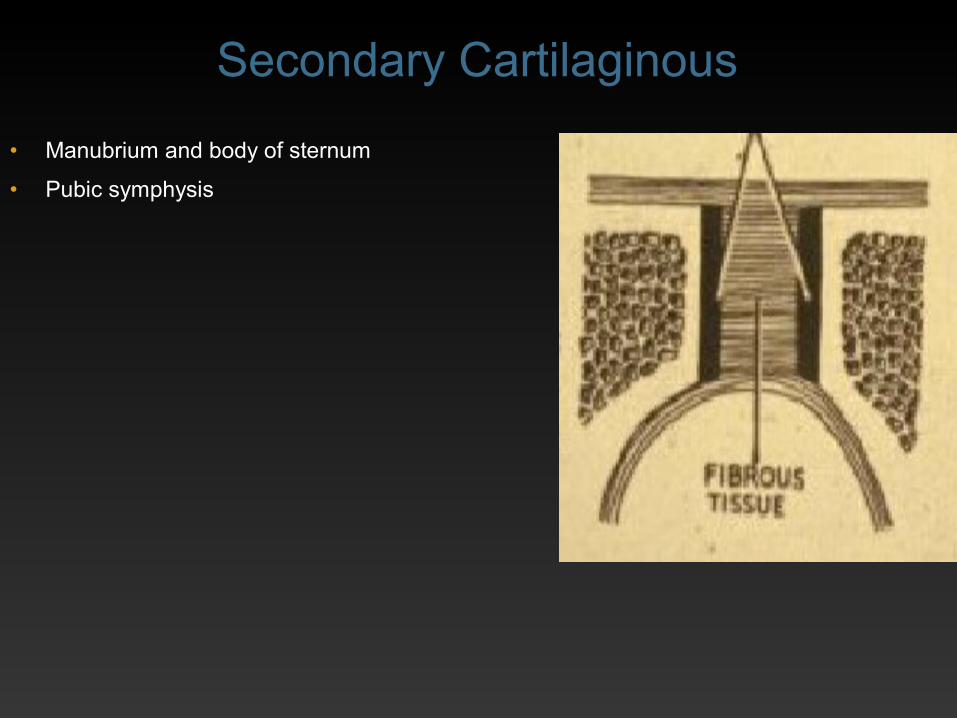
• Manubrium and body of sternum
• Pubic symphysis
Secondary Cartilaginous

SYNOVIAL• Hyaline articular cartilage
• Capsule
• Synovial membrane lines capsule, non articular structures inside joint
• Never lines articular cartilage
• Discs or menisci are fibro cartilage

TYPES OF SYNOVIAL JOINTS
• Shape of articular surface
• Plane
• Hinge
• Condylar
• Pivot
• Saddle
• Ellipsoid
• Ball and socket

TYPES OF SYNOVIAL JOINTSSHAPE OF ARTICULAR SURFACE
• Plane: talo-calcaneal
• Hinge: elbow, interphalangeal joints
• Condylar: knee, metacarpophalangeal
• Pivot: superior radio-ulnar, atlanto-axial
• Saddle: trapezium-base first metacarpal
• Ellipsoid: wrist
• Ball and socket: hip, shoulder, talo-calcaneo-navicular

DESCRIPTION OF A JOINTClassify
• Shape of articular surfaces
• Cartilage covering surface
• Attachments of capsule
• Ligaments, disc
• Haversian pads of fats fill joint spaces
• Synovial membrane
• Movements
• Relations
• Blood and nerve supply
• Clinical significance

CAPSULE• Collagen
• Expanded tendon
• Sesamoid bone
• Thickened to form ligaments
• Haversian pads of fats fill joint spaces

PLANE JOINT
• Surface is flat
• Only allows gliding movement
• Non-axial e.g. facet joints of vertebrae
• Talo-calcaneal joint
Talo-calcaneal

HINGE JOINT
• Movement in one plane (uniaxial) e.g. elbow
• Interphalangeal joints in hand and foot
• Strong ligaments on sides, weaker anterior and posterior
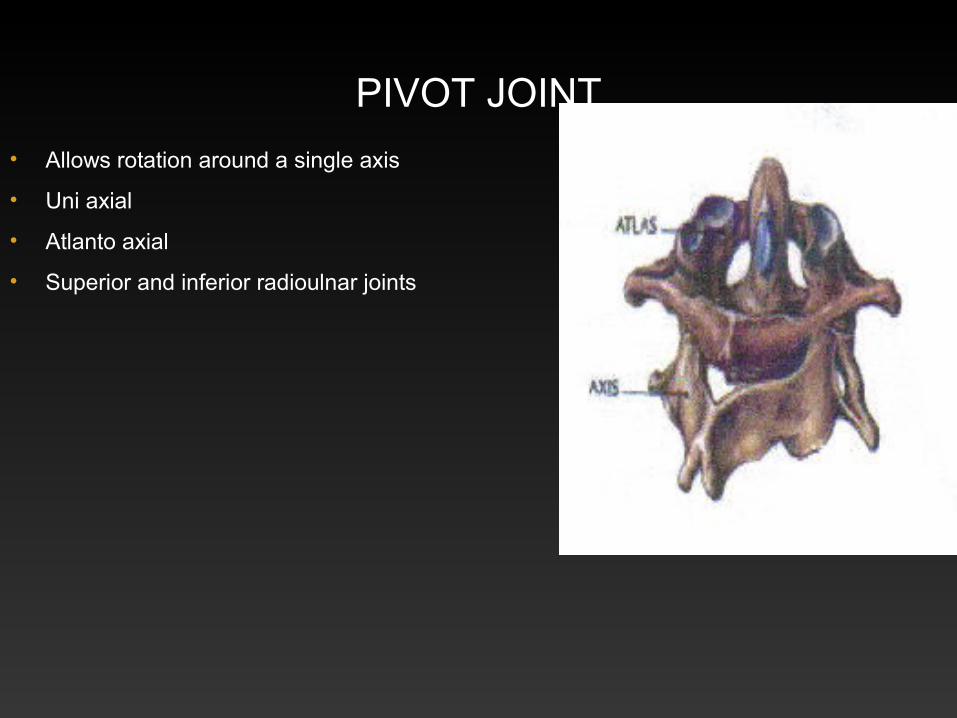
PIVOT JOINT
• Allows rotation around a single axis
• Uni axial
• Atlanto axial
• Superior and inferior radioulnar joints

SADDLE JOINT
• Saddle-shaped concavo-convex surfaces
• Movement in two planes (biaxial) e.g. carpo-metacarpal of the thumb (trapezium and base of first metacarpal)

CONDYLARJOINT
• Two axes at right angles to each other
• Movement in two planes (biaxial)
• Meta-carpophalangeal
• Sternoclavicular
• Atlanto-occipital joints

BALL AND SOCKET JOINT• Allows movement in three axes
• Multiaxial
• Hip
• Shoulder
• Talocalcaneo-navicular joints

SYNOVIAL JOINTS• Discs of fibro cartilage or menisci in some joints
• Blood supply at periphery
• Increase the depth and mobility of the joint
• Synovial folds in joints
• Synovial membrane
• Nerve endings also in fat
• Infrapatellar fat pad
• Facet joints of lumbar vertebrae
• Elbow

CAPSULE• Consists of collagen (type I)
• Thickened to form ligaments
• Expanded quadriceps tendon
• Sesamoid bone in quadriceps tendon
• Synovial membrane lines the inner surface of the capsule and non articular structures inside capsule

FIBROCARTILAGENOUS DISCS
Infrapatellar fat pad
Lateralmeniscus

HAVERSIAN PADS OF FAT• Fat pads are semi-liquid at body
temperature
• They fill the changing spaces that occur during movement
• These pads help to reduce friction between moving tissues

SENSORY SUPPLY• Sensory nerves in fibrous capsule and
ligaments and synovial membrane
• Information about pain
• The position of the joint (proprioception)
• Poor proprioception predisposes to injury
Isakov & Mizrahi, 1997

SYNOVIAL JOINT
• The epiphyses of many long bones are intracapsular
• Injury to a joint, before the cessation of growth, may damage the epiphyseal cartilage
• The articular surfaces are covered by hyaline or articular cartilage

HYALINE CARTILAGE• Hyaline cartilage is avascular
• Nutrition is by diffusion from the synovial fluid
• Must be in contact with the opposing articular surface

OPEN AND CLOSED KINETIC CHAIN
• Open kinetic chain
• The distal segment is free in space
• Raising the hand in the air
• Closed kinetic chain
• The distal segment is fixed

THE DEGREES OF FREEDOM
• Joints can also be classified by degrees of freedom
• Reflects the axis of movement
• If a joint has only one axis
• It has only one degree of freedom

• Nonaxial: no axis of rotation
• Uniaxial: move in one axis
• Have one degree of freedom
• Acromioclavicular 1
• Elbow 1, radioulnar 1
• Proximal and distal interphalangeal 1
• Biaxial: move in two axes
• Have two degrees of freedom
• Metacarpophalangeal 2 +
• Wrist 2 +
• Multiaxial: move in three axes
• Have three degrees of freedom
• Maximum any joint can possess
• Shoulder 3
• Sternoclavicular 3
• Hip 3
• Talocalcaneonavicular 3
The Degrees of Freedom

CLOSE-PACKED
• Stable position
• Surfaces fit together
• Ligaments taut
• Spiral twist
• Screw home articular surface
• Stable position

LEAST-PACKED
• Joint more likely to be injured in least-packed position
• Capsule slackest
• Joint held in this
• Position when injured
• Fluid in knee held in 20° flexion

• Shape of articulating surfaces
• Restraint due to ligaments and muscles crossing joint
• Pain, weakness, spasm or contracture of muscles
• Bulk of adjacent soft tissue
• Impingement of bony surfaces
• Scarring of skin due to injury or burns
RANGE OF JOINT MOVEMENT





























