Embed Size (px)
Citation preview

CHEMOTHERAPYHIGHLIGHTS
MOHAMED BAHR; MD, PHD
Antiprotozoal Drugs

Mohamed Bahr; MD, PhD
ANTIPROTOZOAL DRUGS
Mohamed Bahr; MD, PhD
ANTIAMEBIC DRUGS
Mohamed Bahr; MD, PhD
Mohamed Bahr; MD, PhD
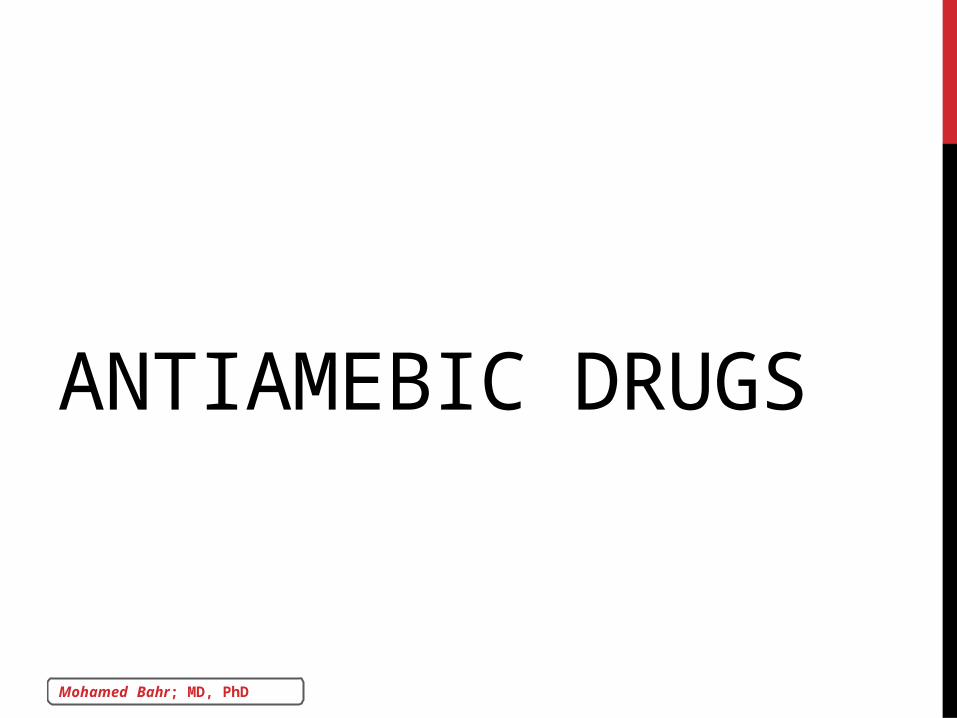
AMEBIASISBowel lumen amebiasis: asymptomatic (carriers or cyst
passers), may become symptomatic if left untreated.
Tissue amebiasis: cysts develop into trophozoites which feed on
intestinal bacteria or invade submucosa of large intestine,
resulting in:
• Intestinal infection: mild to moderate colitis (no dysentery) or
severe (dysentery).
• Amebic granuloma (ameboma) in intestinal wall.
• Extra-intestinal amebiasis: liver abscess, pulmonary amebiasis…
Mohamed Bahr; MD, PhD
1. DILOXANIDE
1st choice luminal amebicide used for:
asymptomatic luminal infections
tissue amebiasis, in combination with tissue amebicides, to
eradicate the source of infection
Side effects: GIT flatulence - nausea - abdominal cramps.
Teratogenic.

Mohamed Bahr; MD, PhD
2. IODOQUINOL
Alternative to diloxanide.
Also used in giardiasis.
Adverse Effects
GIT upset: nausea, vomiting, diarrhea.
SMON.
Thyroid enlargement.

Mohamed Bahr; MD, PhD
3. PAROMOMYCIN (REMAINS IN GIT LUMEN)
GIT

Mohamed Bahr; MD, PhD
1. METRONIDAZOLE (FLAGYL)
It is a prodrug which is activated by reduction of
its NITRO group → disruption of DNA structure
and function → cell death.
Mohamed Bahr; MD, PhD
USESAnaerobic protozoal infections:
• Amebiasis (all forms except asymptomatic cyst passers).
• Others: Giardiasis - Trichomoniasis (urogenital).
Anaerobic bacterial infections:
• Pseudomembranous colitis due to Clostridium difficile.
• Brain abscess, ulcerative gingivitis and dental infections, leg
ulcers.

Mohamed Bahr; MD, PhD
ADVERSE EFFECTSGIT: unpleasant metallic taste, glossitis, stomatitis, nausea and
vomiting.
CNS (serious): dizziness - vertigo - ataxia - neuropathy -
convulsions.
Dark urine - dysuria.
Neutropenia.
Teratogenic
Enzyme inhibitor: ↑ warfarin level.
Mohamed Bahr; MD, PhD
2. TINIDAZOLE (FASIGYN)Similar to metronidazole but more effective, longer t ½, and
less teratogenic.
Mohamed Bahr; MD, PhD
3. CHLOROQUINE
LIVER
Mohamed Bahr; MD, PhD
4. EMETINE AND DEHYDROEMETINERemember: Amphotericin
Severe
Mohamed Bahr; MD, PhD
5. TETRACYCLINES
Mild
Mohamed Bahr; MD, PhD
Mohamed Bahr; MD, PhD
ANTIMALARIAL DRUGS
Mohamed Bahr; MD, PhD
Mohamed Bahr; MD, PhD
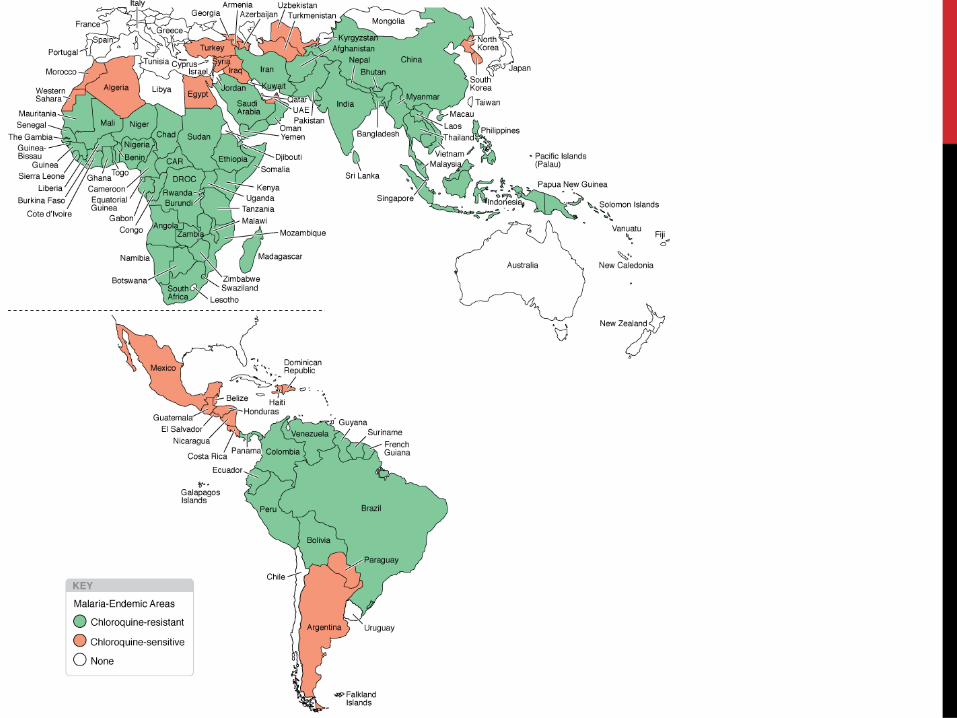
PROBLEMS1. Chloroquine resistance: chloroquine is the mainstay of
antimalarial therapy, but resistance to drug
(geographically distributed) is a major problem especially
with P falciparum (most dangerous → encephalopathy
and renal failure).
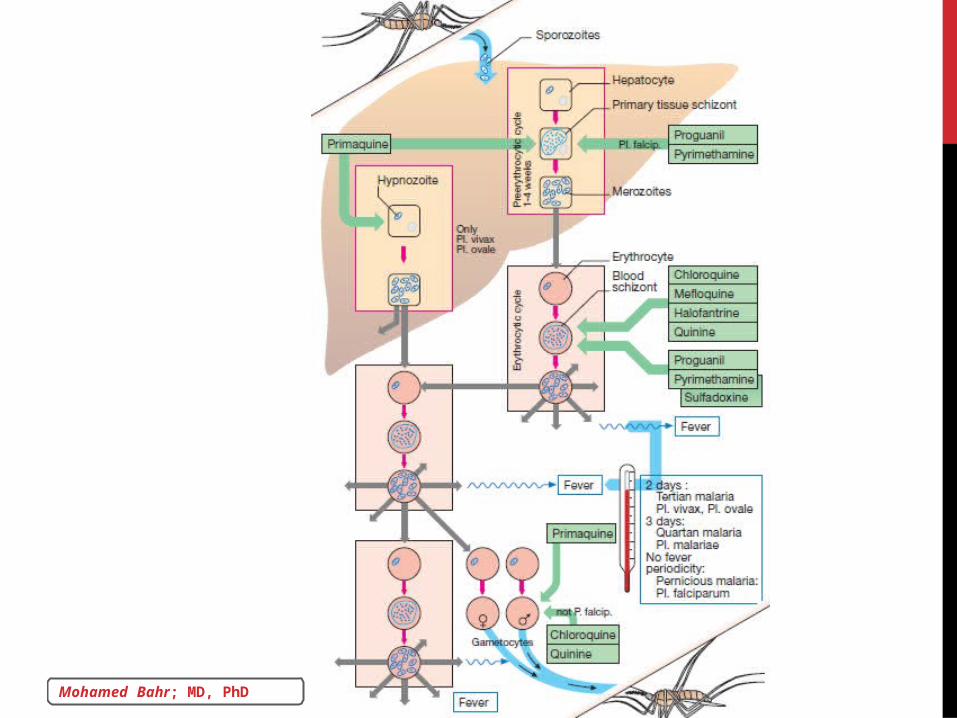
2. Relapse: re-activation of dormant form in hepatic cells →
relapses in P ovale and P vivax, not in P falciparum.
Mohamed Bahr; MD, PhD

Mohamed Bahr; MD, PhD
I. 4-AMINOQUINOLINES
Mohamed Bahr; MD, PhD
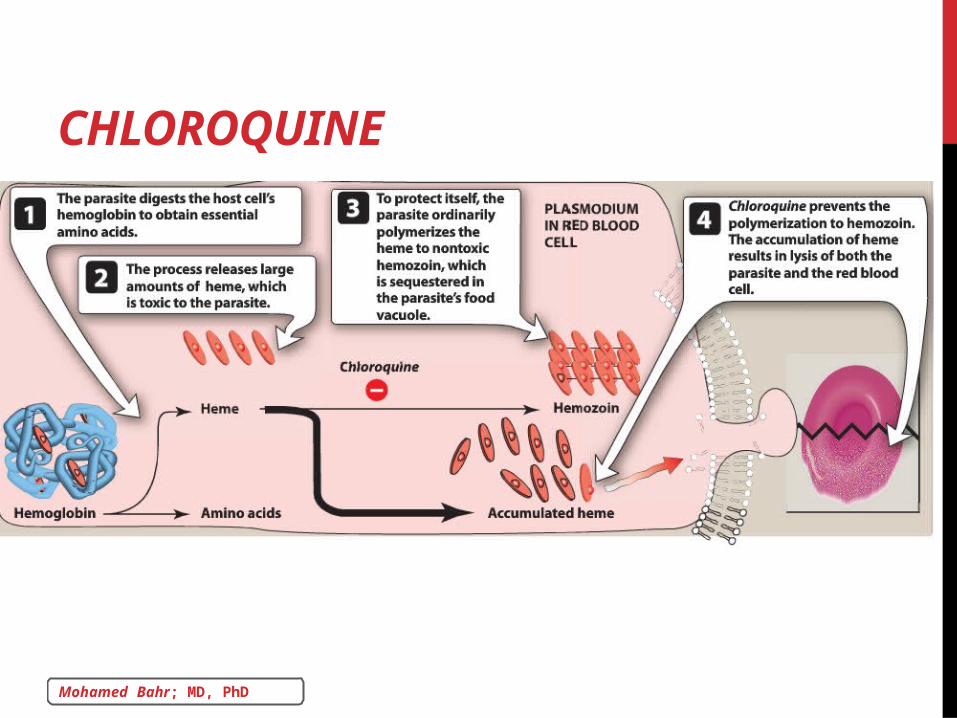
CHLOROQUINE

Mohamed Bahr; MD, PhD
ADVERSE EFFECTS GIT: nausea, vomiting and diarrhea.
Hypersensitivity: pruritis (most common).
CNS…
Neutropenia.
Cardiotoxic: quinidine-like action (hypotension and arrhythmias).
Eye: corneal opacity, blurred vision and retinopathy.
Ototoxicity
Hemolytic Anemia: in G6PD-deficient subjects.
Mohamed Bahr; MD, PhD
QUININE AND QUINIDINECardiotoxic: Quinidine-like action → hypotension and
arrhythmias.
Eye → blurred vision and blindness.
Cinchonism: tinnitus - headache - dizziness and visual
disturbances.
Black water fever and hemolysis.
Uterus: abortion.
Not in Prophylaxis!
Mohamed Bahr; MD, PhD
QUININE AND QUINIDINE
Alternatives

Mohamed Bahr; MD, PhD
MEFLOQUINE
Excellent Alternative

Mohamed Bahr; MD, PhD
II. HALOFANTRINE
Cardiotoxic
Alternative

Mohamed Bahr; MD, PhD
III. 8-AMINOQUINOLINES: PRIMAQUINE
Radical cure
Terminal
prophylaxis
Gametocidal

Mohamed Bahr; MD, PhD
G6PD
Teratogenic
Mohamed Bahr; MD, PhD
IV. ANTIFOLATE ANTIMALARIAL DRUGS
Blood schizonticides (mainly)
1ry tissue schizonticides
sporontocides

Mohamed Bahr; MD, PhD
Treatment of chloroquine-resistant falciparum (fansidar plus
quinine).
Prophylaxis in all types (proguanil + chloroquine).

Mohamed Bahr; MD, PhD
ADVERSE EFFECTS
GIT
G6PD
Remember: TMP
Mohamed Bahr; MD, PhD
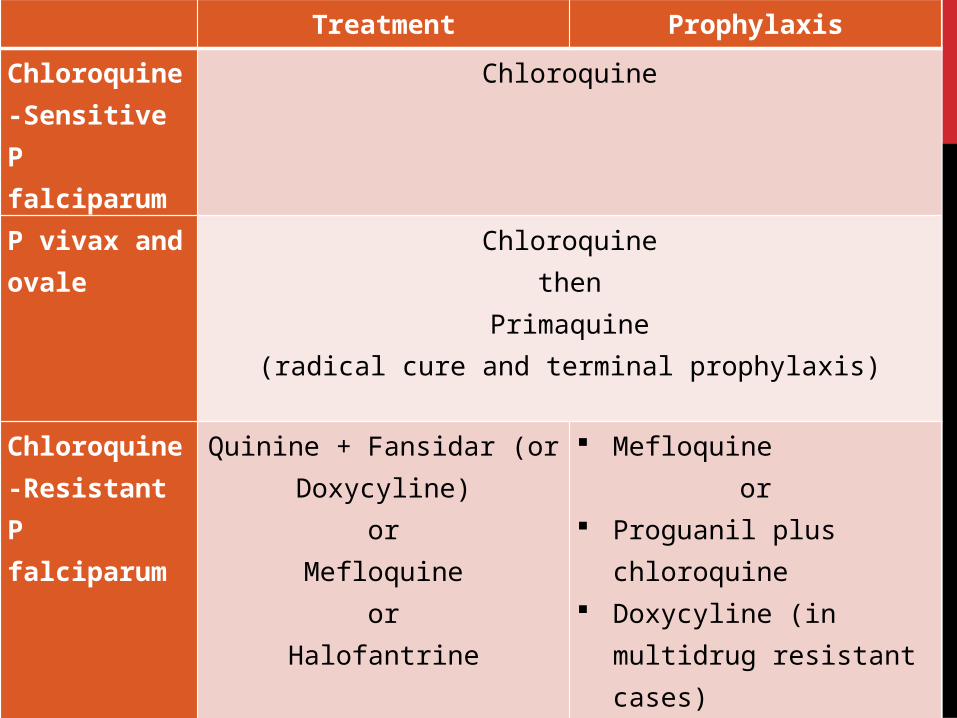
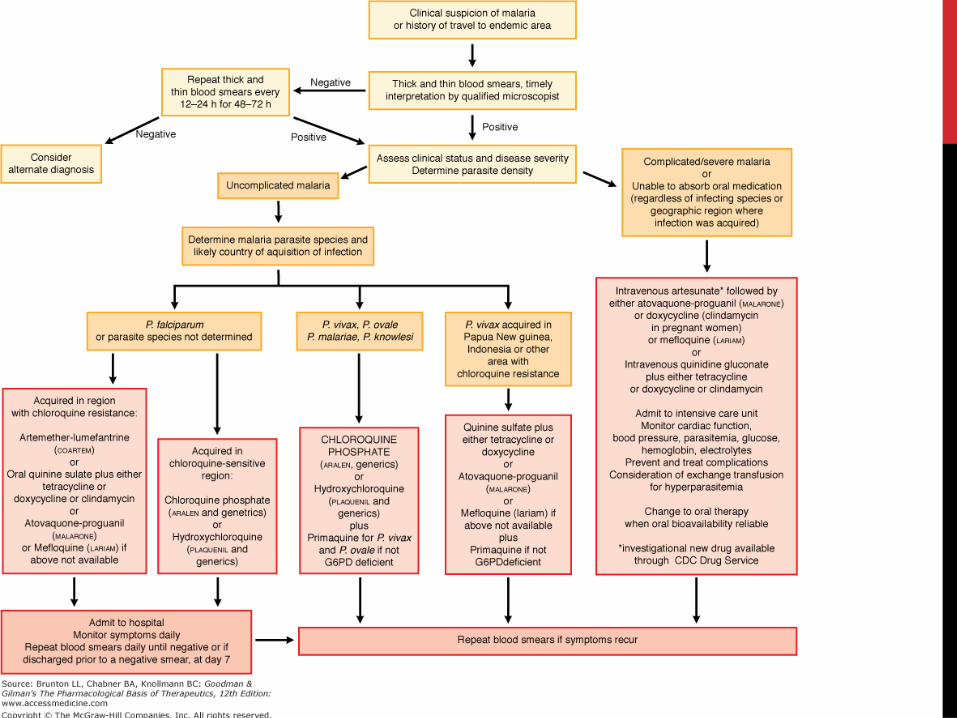
Treatment Prophylaxis
Chloroquine-Sensitive P falciparum
Chloroquine
P vivax and ovale
Chloroquinethen
Primaquine(radical cure and terminal prophylaxis)
Chloroquine-Resistant P falciparum
Quinine + Fansidar (or Doxycyline)
orMefloquine
orHalofantrine
Mefloquine or
Proguanil plus chloroquine Doxycyline (in multidrug
resistant cases)
Mohamed Bahr; MD, PhD
DRUGS FOR CHEMOPROPHYLAXIS ARE GIVEN:
for 2 wks (chloroquine, mefloquine) or for 2 days
(proguanil or doxycyline) before travel
AND
for 4 wks after leaving endemic area.
Mohamed Bahr; MD, PhD
Mohamed Bahr; MD, PhD
ANTITRYPANOSOMAL DRUGS

Mohamed Bahr; MD, PhD

Mohamed Bahr; MD, PhD
Mohamed Bahr; MD, PhD
REFERENCESLippincott’s Illustrated Reviews, 5th ed.
Color Atlas of Pharmacology, 2nd ed.
Goodman and Gilman's The Pharmacological Basis of
Therapeutics, 12th ed.